E UROPEAN UROLOGY XXX (2017) XXX–XXX · not notably different between PNL types. Study designs...
16
Platinum Priority – Stone Disease Editorial by XXX on pp. x–y of this issue Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A Systematic Review from the European Association of Urology Urolithiasis Guidelines Panel Yasir Ruhayel a , Abdulkadir Tepeler b , Saeed Dabestani a , Steven MacLennan c , Alesˇ Petrˇı´k d,e , Kemal Sarica f , Christian Seitz g , Andreas Skolarikos h , Michael Straub i , Christian Tu ¨rk j , Yuhong Yuan k , Thomas Knoll l, * a Department of Urology, Ska ˚ne University Hospital, Malmo ¨, Sweden; b Department of Urology, Sen Jorj Austria Hospital, Istanbul, Turkey; c Academic Urology Unit, University of Aberdeen, Aberdeen, UK; d Department of Urology, Region Hospital, C ˇ eske ´ Budeˇjovice, Czech Republic; e Department of Urology, First Faculty of Medicine, Charles University in Prague, Prague, Czech Republic; f Department of Urology, Dr. Lutfi Kirdar Kartal Research and Training Hospital, Istanbul, Turkey; g Department of Urology, Medical University Vienna, Vienna, Austria; h Second Department of Urology, Sismanoglio Hospital, Athens Medical School, Athens, Greece; i Department of Urology, Technical University Munich, Munich, Germany; j Department of Urology, Hospital of the Sisters of Charity, Vienna, Austria; k Department of Medicine, McMaster University, Hamilton, Canada; l Department of Urology, Sindelfingen-Boeblingen Medical Center, University of Tu ¨bingen, Sindelfingen, Germany E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X ava ilable at www.sciencedirect.com journa l homepage: www.europea nurology.com Article info Article history: Accepted January 30, 2017 Associate Editor: Giacomo Novara Keywords: Mini-perc Percutaneous nephrolithotomy Residual fragments Stone surgery Stenting Systematic review Urinary calculi Abstract Context: Miniaturized instruments for percutaneous nephrolithotomy (PNL), utilizing tracts sized 22 Fr, have been developed in an effort to reduce the morbidity and increase the efficiency of stone removal compared with standard PNL (>22 Fr). Objective: We systematically reviewed all available evidence on the efficacy and safety of miniaturized PNL for removing renal calculi. Evidence acquisition: The review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement. Since it was not possible to perform a meta-analysis, the data were summarized in a narrative synthesis. Evidence synthesis: After screening 2945 abstracts, 18 studies were included (two randomized controlled trials [RCTs], six nonrandomized comparative studies, and 10 case series). Thirteen studies were full-text articles and five were only available as congress abstracts. The size of tracts used in miniaturized procedures ranged from 22 Fr to 4.8 Fr. The largest mean stone size treated using small instruments was 980 mm 2 . Stone-free rates were comparable in miniaturized and standard PNL procedures. Procedures per- formed with small instruments tended to be associated with significantly lower blood loss, while the procedure duration tended to be significantly longer. Other complications were not notably different between PNL types. Study designs and populations were heterogeneous. Study limitations included selection and outcome reporting bias, as well as a lack of information on relevant confounding factors. Conclusions: The studies suggest that miniaturized PNL is at least as efficacious and safe as standard PNL for the removal of renal calculi. However, the quality of the evidence was poor, drawn mainly from small studies, the majority of which were * Corresponding author. Department of Urology, Klinikum Sindelfingen-Bo ¨ blingen, University of Tu ¨ bingen, Arthur-Gruber-Strasse 70, 71065 Sindelfingen, Germany. Tel. +49 7031 9812501; Fax: +49 703 9812354. E-mail address: [email protected] (T. Knoll). EURURO-7240; No. of Pages 16 Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A Systematic Review from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/ j.eururo.2017.01.046 http://dx.doi.org/10.1016/j.eururo.2017.01.046 0302-2838/# 2017 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Transcript of E UROPEAN UROLOGY XXX (2017) XXX–XXX · not notably different between PNL types. Study designs...

EURURO-7240; No. of Pages 16
Platinum Priority – Stone DiseaseEditorial by XXX on pp. x–y of this issue
Tract Sizes in Miniaturized Percutaneous Nephrolithotomy:
A Systematic Review from the European Association of Urology
Urolithiasis Guidelines Panel
Yasir Ruhayel a, Abdulkadir Tepeler b, Saeed Dabestani a, Steven MacLennan c, Ales Petrık d,e,Kemal Sarica f, Christian Seitz g, Andreas Skolarikos h, Michael Straub i, Christian Turk j,Yuhong Yuan k, Thomas Knoll l,*
a Department of Urology, Skane University Hospital, Malmo, Sweden; b Department of Urology, Sen Jorj Austria Hospital, Istanbul, Turkey; c Academic Urology
Unit, University of Aberdeen, Aberdeen, UK; d Department of Urology, Region Hospital, Ceske Budejovice, Czech Republic; e Department of Urology, First
Faculty of Medicine, Charles University in Prague, Prague, Czech Republic; f Department of Urology, Dr. Lutfi Kirdar Kartal Research and Training Hospital,
Istanbul, Turkey; g Department of Urology, Medical University Vienna, Vienna, Austria; h Second Department of Urology, Sismanoglio Hospital, Athens
Medical School, Athens, Greece; i Department of Urology, Technical University Munich, Munich, Germany; j Department of Urology, Hospital of the Sisters of
Charity, Vienna, Austria; k Department of Medicine, McMaster University, Hamilton, Canada; l Department of Urology, Sindelfingen-Boeblingen Medical
Center, University of Tubingen, Sindelfingen, Germany
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X
ava i lable at www.sc iencedirect .com
journa l homepage: www.europea nurology.com
Article info
Article history:
Accepted January 30, 2017
Associate Editor:
Giacomo Novara
Keywords:
Mini-perc
Percutaneous nephrolithotomy
Residual fragments
Stone surgery
Stenting
Systematic review
Urinary calculi
Abstract
Context: Miniaturized instruments for percutaneous nephrolithotomy (PNL), utilizingtracts sized �22 Fr, have been developed in an effort to reduce the morbidity andincrease the efficiency of stone removal compared with standard PNL (>22 Fr).Objective: We systematically reviewed all available evidence on the efficacy and safetyof miniaturized PNL for removing renal calculi.Evidence acquisition: The review was performed according to the Preferred ReportingItems for Systematic Reviews and Meta-analyses statement. Since it was not possible toperform a meta-analysis, the data were summarized in a narrative synthesis.Evidence synthesis: After screening 2945 abstracts, 18 studies were included (tworandomized controlled trials [RCTs], six nonrandomized comparative studies, and 10 caseseries). Thirteen studies were full-text articles and five were only available as congressabstracts. The size of tracts used in miniaturized procedures ranged from 22 Fr to 4.8 Fr.The largest mean stone size treated using small instruments was 980 mm2. Stone-freerates were comparable in miniaturized and standard PNL procedures. Procedures per-formed with small instruments tended to be associated with significantly lower bloodloss, while the procedure duration tended to be significantly longer. Other complicationswere not notably different between PNL types. Study designs and populations wereheterogeneous. Study limitations included selection and outcome reporting bias, as wellas a lack of information on relevant confounding factors.Conclusions: The studies suggest that miniaturized PNL is at least as efficacious andsafe as standard PNL for the removal of renal calculi. However, the quality of theevidence was poor, drawn mainly from small studies, the majority of which were
* Corresponding author. Department of Urology, Klinikum Sindelfingen-Boblingen, University ofTubingen, Arthur-Gruber-Strasse 70, 71065 Sindelfingen, Germany. Tel. +49 7031 9812501;Fax: +49 703 9812354.E-mail address: [email protected] (T. Knoll).
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046
http://dx.doi.org/10.1016/j.eururo.2017.01.0460302-2838/# 2017 European Association of Urology. Published by Elsevier B.V. All rights reserved.

EURURO-7240; No. of Pages 16
single-arm case series, and only two of which were RCTs. Furthermore, the tract sizes usedand types of stones treated were heterogeneous. Hence, the risks of bias and confoundingwere high, highlighting the need for more reliable data from RCTs.Patient summary: Removing kidney stones via percutaneous nephrolithotomy (PNL) usingsmaller sized instruments (mini-PNL) appears to be as effective and safe as using larger(traditional) instruments, but more clinical research is needed.
# 2017 European Association of Urology. Published by Elsevier B.V. All rights reserved.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X2
1. Introduction
Kidney stone disease is considered to be an important
health issue; its incidence has increased over the years to
almost 9% [1]. Despite efforts in prevention and advances in
management methods, urolithiasis is still an important
cause of morbidity in all age groups and carries a significant
economic burden because of associated direct and indirect
costs [2,3].
Percutaneous nephrolithotomy (PNL) has gained accep-
tance as the gold standard for the treatment of large renal
calculi [4,5]. During the past 20 yr, the instruments used
have been miniaturized in an effort to decrease morbidity
associated with standard PNL and increase the efficiency of
stone removal. Jackman et al [6] and Helal et al [7] initially
used smaller instruments in 1997 for pediatric cases with
the proposed advantage of lower morbidity. Today, the term
mini-perc, or mini-PNL (mPNL), usually describes tract sizes
between 14 Fr and 22 Fr, although a clear definition does not
exist [4]. Recently, even smaller systems—ultramini-PNL
(umPNL) using tracts sized 11–13 Fr and microperc (mPNL)
using tracts sized 4.8–10 Fr—have been introduced as
alternative modalities to reduce procedure-related morbid-
ity [8,9].
The primary goal of PNL is to achieve stone-free status
while minimizing morbidity and complications. It has been
reported that tract size is one of the main parameters
affecting the complication rate [10]. However, reducing the
tract size may adversely affect some procedure-related
factors such as operation time [11]. We performed a
systematic review to assess the relative benefits and harms
of different PNL tract sizes for the treatment of renal stones.
2. Evidence acquisition
2.1. Search strategy
This systematic review was performed according to the
Preferred Reporting Items for Systematic Reviews and
Meta-analyses (PRISMA) statement [12] and the Cochrane
Handbook for Systematic Reviews of Interventions
[13]. Studies on PNL (from January 1, 2000 to October 30,
2014) were identified by highly sensitive searches of
electronic databases (Embase, Medline, the Cochrane
Central Register of Controlled Trials, and the Health
Technology Assessment Database). Studies in languages
other than English were excluded. The protocol for the
review is available on PROSPERO (CRD42015023766; www.
crd.york.ac.uk/PROSPERO).
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
The articles identified were independently screened by
two reviewers (Y.R. and A.T.). Full-text articles of potentially
relevant studies were subsequently independently scruti-
nized for eligibility. Disagreements were resolved by a third
party (T.K.).
2.2. Selection of studies
We included randomized controlled trials (RCTs), nonran-
domized comparative studies (NRCSs), and single-arm
studies with at least one study arm reporting efficacy or
safety data on PNL procedures using tracts sized �22 Fr
(mPNL, umPNL, or mPNL) for treatment of renal stones in
adults (age �18 yr). Studies published as full-text articles or
as congress abstracts were included. The exclusion criteria
were: case series (single arm) of <20 patients; pediatric
studies (age <18 yr); patients with pre-existing nephros-
tomy before PNL; anatomic abnormalities (eg, horse-shoe
kidney, transplanted kidney, malrotated kidney); use of
electrohydraulic lithotripsy for stone fragmentation; and
multitract punctures (ie, more than one tract used during
procedure). However, studies fulfilling any exclusion
criterion were included if groups of patients of interest to
this review were reported separately, or if the fraction of
procedures or patients with criteria meriting exclusion
constituted <10% of the total study population.
The primary benefit outcomes were the immediate
stone-free rate (ISFR) and the stone-free rate (SFR) at a later
date (after auxiliary procedures for a period of up to 3 mo).
For this review, ‘‘stone-free’’ was defined as there being no
detectable stone fragments on radiology; if an alternative
definition was used by the trialist (eg, residual fragments
sized <4 mm), the data were reclassified accordingly. The
imaging modality used to assess stone-free status was not
considered.
The primary harm outcomes were intraoperative and
postoperative complications. These were recorded as the
incidence of grouped complications according to severity,
such as Clavien grade, or as the incidence of ad hoc
individual complications such as blood loss (as defined by
the trialist; eg, ml of blood or change in hemoglobin
concentration), the need for blood transfusions, visceral
injury, urosepsis, pneumothorax, or death.
The secondary benefits and harms outcomes were:
duration of the procedure; quality of life (QOL; as defined by
the trialist); pain (as defined by the trialist; eg, analgesic
requirement, pain scores quantified on a visual analog scale
[VAS], etc); need for a secondary procedure (procedure to
clear the stone beyond the primary procedure, including
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 3
EURURO-7240; No. of Pages 16
retreatment using the same modality [ie, more than one
PNL session] or other modality such as shockwave
lithotripsy [SWL] or transurethral endoscopic lithotripsy);
need for adjunctive procedure (a procedure to deal with a
complication [eg, nephrostomy or double-J stent insertion
for obstruction] and procedures incidental to the stone
removal process such as stent insertion and/or removal);
duration of hospital stay; hospital readmission; and
emergency department visit.
2.3. Data extraction
A data extraction form was developed a priori to collect
information on study design, characteristics of participants
and interventions, and primary and secondary outcome
measures (benefits and harms).
2.4. Risk-of-bias assessment
Two reviewers (Y.R. and A.T.) independently assessed the
risk of bias (RoB) for individual studies. Any disagreements
were resolved by discussion or by consulting a third author
(T.K.). The RoB in RCTs was assessed using the recom-
mended tool in the Cochrane Handbook for Systematic
Reviews of Interventions [13]. This included assessment of
random sequence generation, allocation concealment,
blinding of participants and personnel, blinding of outcome
assessment, incomplete outcome data, selective reporting,
and other sources of bias.
RoB in NRCSs was assessed using all seven domains
above and an extra item to assess the risk of findings being
explained by confounding. This is a pragmatic approach
informed by methodological literature pertaining to asses-
sing RoB in NRCSs [14,15]. A list of the most important
potential confounders for harm and benefit outcomes was
developed a priori with clinical content experts (European
Association of Urology Urolithiasis Guidelines Panel). The
potential confounding factors were stone size, stone
location, obesity, previous open surgery on a kidney (eg,
open nephrolithotomy), subcostal versus intercostal punc-
ture, and calyceal access (upper vs middle vs lower calyx).
For each study, an algorithmic approach was used to
assess the risk of confounding bias. The following were
considered in sequence. (1) Was the prognostic confounder
considered? If ‘‘no’’, the study was deemed to be at ‘‘high’’
RoB for this confounder. If ‘‘yes’’, go to the next question. (2)
Was the confounder balanced between the intervention(s)
and control group (s)? If ‘‘yes’’, the study was at ‘‘low’’ RoB. If
‘‘no’’, go to the next questions. (3) Was the confounder
controlled for in the analysis, for example via statistical
adjustment such as univariate or multivariate analysis or
propensity score matching? If ‘‘yes’’, the study was at ‘‘low’’
RoB. If ‘‘no’’, the study was at ‘‘high’’ RoB.
The approach described above cannot be used to assess
RoB in NRCSs. To address the external validity (ie,
applicability of the results to different people, places, or
time) of the NRCSs, we assessed whether study participants
were selected consecutively or representative of a wider
patient population, and whether the specified confounding
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
factors were comparable across studies reporting on the
same intervention. This too was a pragmatic approach
informed by the methodological literature [16,17]. Further
details on the approach outlined above are available on
PROSPERO (CRD42015023766; www.crd.york.ac.uk/
PROSPERO).
The key RoB and confounder assessments from the tools
described above were summarized and presented graphi-
cally (Fig. 2).
2.5. Data analysis
For the purposes of this review, we refer to all procedures
using smaller tract sizes (�22 Fr) as mPNL when compared
with procedures using larger instruments (unless otherwise
specified). A meta-analysis for the two RCTs was not feasible
because of heterogeneity in study design. Forest plots were
created for the RCTs and NRCSs reporting SFRs to show the
direction and magnitude of effects.
3. Evidence synthesis
3.1. Search results
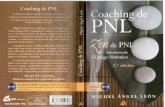
The search returned 2945 abstracts (Fig. 1), of which
240 were scrutinized for eligibility. Four articles in
languages other than English were excluded, as were an
additional 218 studies that did not meet the remaining
inclusion criteria. A total of 18 studies were eligible for final
inclusion, of which 13 were full-text articles [8,11,18–28]
and five were conference abstracts [29–33].
3.2. Study and patient characteristics
Of the 18 studies included, two were RCTs [19,28], six were
NRCSs [11,21,22,24,26,27], and ten were single-arm case
series on mPNL only [8,18,20,23,25,29–33]. There was one
study on PNL using tract size 22 Fr [21] and one on tract
sizes <20 Fr [29]. Three studies evaluated tract size 18 Fr
[18,22,23], two studies 16 Fr [19,26], and two 14 Fr
[11,25]. One study reported on tracts sized 14–18 Fr [24],
and another on tracts �18 Fr [27]. There were three studies
on tract sizes 11–13 Fr [8,20,30] and one on 4.8 Fr [28]. Three
studies presented as conference abstracts did not explicitly
state the tract size, but the procedures were termed mPNL
[31–33]. No studies reported QOL outcomes. The baseline
characteristics of the participants in the studies included
are outlined in Table 1 and the findings are summarized in
Table 2.
3.3. RCTs
Two RCTs were identified, both of which were full-text
articles. Only one study investigated the benefits and harms
of mPNL using ‘‘regular’’ (16 Fr) compared to standard PNL
(24 Fr) [19]. Both blood loss and the need for blood
transfusion were significantly lower in the mPNL group
(both p < 0.05), although the types of stone were not fully
comparable. The SFR was only significantly different for
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

Records identified through database searching(n = 2945 )
Abstr acts screened (n = 2945 )
Excluded
(n = 222)(n = 99)(n = 123)
Abstracts assessed for eligibilit y
Tota l (n = 240)Full-text articles (n = 112)
Conference abstracts (n = 128)
Full-text articles included (n = 13)
Scr
een
ing
Incl
ud
edE
ligib
ility
Iden
tifi
cati
on
Conference abstracts included (n = 5)
Records exclude dn = 2705
Reasons for exclusio n
• Language other than Englis h• Interventio n no t relevant• Popula tio n unclea r• Ba sic scien ce studie s• Participant s in cas e serie s with n <2 0• Case s <1 8 yr of ag e >10%• Cases wi th ana tomica l anomalie s >10 %• Case s treate d bilaterall y >10%• Multipl e tract s use d in >10 % of cases• Dat a not in useabl e format• Imagin g studies• Duplicat e studie s or duplicat e data
Studies included in systema tic reviewTota l (n = 18)• 2 RC Ts• 6 NRCS s• 10 case serie s
Fig. 1 – Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram showing the screening process for inclusion ofstudies. RCT = randomized controlled trial; NRCS = non-randomized comparative study.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X4
EURURO-7240; No. of Pages 16
multiple calyceal stones (85% for mPNL vs 70% for standard
PNL, p < 0.05). The duration of the procedure was longer in
the mPNL group for all stone types (all p < 0.05; Table 1).
The other RCT was a comparison of mPNL (4.8 Fr) and
standard PNL (30 Fr) [28]. No benefit was found with respect
to ISFR (p = 1), although blood loss and procedure duration
were lower (p = 0.004 and 0.034, respectively) and hospital
stay was shorter (p = 0.001). Intrarenal pelvic pressure was
higher in the mPNL group (p < 0.0001; Table 1).
3.4. NRCSs
Six NRCSs were included, all of which were full-text articles.
One study compared five groups with successively increas-
ing PNL tract size (22, 24, 26, 28, and 30 Fr) [21]. Blood loss
increased with the tract size (p < 0.05) but the procedure
duration did not significantly differ between the groups
(Table 2). Another study using the PNL Global Study database
of The Clinical Research Office of the Endourological Society
(CROES) reported data for four groups (�18, 24–26, 27–30,
and �32 Fr) [27]. The only relevant outcomes were blood
loss and blood transfusion rates, which significantly
increased with the tract size (p = 0.00016 and <0.0001).
Four comparative studies comprised two main comparator
groups (mPNL vs standard PNL). In one of the studies [11],
the control arm (30 Fr) was further divided into two groups:
patients who received a nephrostomy tube and patients who
did not (tubeless). SFR was lower in the mPNL group (14 Fr)
than in either of the standard PNL groups (tube p = 0.016 and
tubeless p = 0.009). Blood loss was lower than in the tube
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
standard PNL group (p = 0.021) but not the tubeless standard
PNL group (p = 0.041). Tubeless standard PNL was also
superior in terms of analgesic requirement, pain (VAS), and
duration of procedure and hospital stay (Table 2). Xu et al
[26] compared 16 Fr mPNL with 24 Fr PNL, and observed
lower blood loss in the mPNL group (p = 0.015), although the
stones treated were also smaller. ISFR, complication rates,
procedure duration, and hospital stay did not differ (Table 2).
Mishra et al [24] compared mPNL (14–18 Fr) with standard
PNL (24–28 Fr), but interpretation of the results is obscured
by the use of different energy sources for stone fragmenta-
tion: laser in the mPNL group and pneumatic in the standard
PNL group [24]. The study reported similar SFR (p = 0.49) and
analgesic requirement (p = 0.28), but lower blood loss
(p = 0.0098) and procedure duration (p = 0.0008), and
shorter hospital stay (p <0.00001) in the mPNL group. A
greater proportion of procedures were tubeless in the mPNL
(78%) than in the standard PNL group (14%; p < 0.001). Knoll
et al [22] compared mPNL (18 Fr) and standard PNL (26 Fr)
and found similar ISFR in both groups (p = 1.00). However,
stones were significantly larger in the standard PNL group
(p = 0.042). The study also revealed similar blood loss,
complication rates, procedure duration, and analgesic
requirements for both groups (all p > 0.05). However pain
scores (VAS) were lower (p = 0.048) and hospital stay was
shorter (p = 0.021) among mPNL patients. All mPNL proce-
dures were tubeless if uncomplicated and the patient was
rendered stone-free, otherwise a nephrostomy tube was
placed. All patients undergoing standard PNL received a
nephrostomy tube.
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

Karaköse2014 [21]
Xu 2014 [26]
Knoll 2010 [22]
Yamaguchi 2011 [27]
Mishra 2011 [24]
Gius�2007 [11]
+
+
–
?
–?
–
?
?
–
–
–
–
–
–
–
–
– –
–
+
+
+
+
+
?
?
?
?
+
+
+ –
–
–
+
+
+
–
–
–
–
–
–
–
–
–
–
–
–
+
–
+ –
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
+
?
Low risk
High risk
Unclear risk
Tepeler2014 [28]
Cheng 2010 [19] ?
+
+?
–
??
+
+
– + –
–
+
?
Low risk
(A)
(B)
(C)
High risk
Unc lear risk
–
+
?
Low risk
High risk
Unclear risk
Miller 2014 [32]
?
Karatag2014 [31]
Desai 2013 [30]
Desai 2013 [8]
Desai 2013 [20]
Abdelhafez2013 [18]
Bha�u2014 [29]
Zimmermans2012 [33]
Lu 2013 [23]
Sung 2006 [25]
?
?
?
?
?
?
?
?
?
?
–
–
?
?
?
?
+
? +
?
? ?
+ +
+ +
? +
+ ? ?
??? ?
? +
? ?
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
?
Fig. 2 – Risk of bias and confounding assessment summary. (A) Risk of bias assessment for randomized controlled trials. (B) Risk of bias andconfounding assessment for non-randomized comparative studies. (C) Risk of bias assessment for case series. Green circle = low risk of bias orconfounding; red circle = high risk of bias or confounding; yellow circle = unclear risk of bias or confounding.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 5
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046

Ta
ble
1–
Ba
seli
ne
cha
ract
eri
stic
sin
all
the
stu
die
sin
clu
de
d
Stu
dy
ID,
de
sig
n,
cou
ntr
y,
recr
uit
me
nt
pe
rio
d
Inte
rve
nti
on
NFU
(mo
),
me
an�
SD,
med
ian
[ran
ge]
Ag
e(y
r),
me
an�
SD,
med
ian
[ran
ge]
Ge
nd
er
M/F
BM
I(k
g/m
2),
me
an�
SD,
med
ian
[ran
ge]
Incl
usi
on
crit
eri
aE
xcl
usi
on
crit
eri
aS
ton
esi
ze
inm
mo
rm
m2,
me
an�
SD
[ran
ge
+IQ
R]
Sto
ne
loca
tio
n
inU
C,
MC
,
LC,
Po
rU
PJ
if
av
ail
ab
le
Sto
ne
late
rali
ty
R/L
Ou
tco
me
sm
ea
sure
d
Te
pe
ler
20
14
,R
CT
,T
urk
ey
,
20
12
–2
01
3[2
8]
mP
NL
4.8
Fr1
00
47
.2�
15
.1[2
8–
66
]4
/62
7.5�
3.6
(21
.8–
33
.5)
NR
Ag
e<
18
yr,
na
rro
w
infu
nd
ibu
lum
,im
pa
cte
dU
PJ
sto
ne
,u
rete
ral
ob
stru
ctio
n
pre
ve
nti
ng
inse
rtio
no
fst
en
t
toC
S,
mu
ltip
lere
na
la
cce
sse
s
19
.9�
5.0
(12
–3
0)
mm
Re
na
lN
RB
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Oth
er:
pe
lvic
pre
ssu
re
PN
L3
0Fr
10
44
.3�
10
.1[2
7–
62
]2
7.8�
2.8
(23
.7–
33
.1)
21
.9�
4.8
(15
–3
0)
mm
Re
na
l
Ch
en
g2
01
0,
RC
T,
Ch
ina
,
20
04
–2
00
7[1
9]
mP
NL
16
Fr7
2N
R3
7.2
(24
–6
7)
1.2
NR
Sin
gle
tra
ct
Sin
gle
tech
niq
ue
Pa
tie
nts
req
uir
ing
mu
ltip
le
tra
cts
an
db
oth
tech
niq
ue
s
(min
ia
nd
sta
nd
ard
)
98
0m
m2
18
(25
%)
Sta
gh
orn
27
(38
%)
P
27
(38
%)
mu
ltip
leC
Ra
tio
1.5
Be
ne
fits
:IS
FR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DH
S,
DP
,
an
alg
esi
cre
qu
ire
me
nt
PN
L2
4Fr
11
53
9.6
(27
–7
2)
1.2
10
10
mm
22
9(2
5%
)S
tag
ho
rn
46
(40
%)
P
40
(35
%)
Mu
ltip
leC
Ra
tio
1.4
Ka
rak
ose
20
14
,co
mp
ara
tiv
e
stu
dy
,T
urk
ey
,2
01
1–
20
12
[21
]
mP
NL
22
Fr1
50
45
.6�
12
.52
[26
–7
1]
9/6
NE
‘‘Un
ev
en
tfu
lP
CN
L’’
‘‘Co
mp
lica
ted
pro
ced
ure
s’’,
mu
ltip
letr
act
s,a
bn
orm
al
pre
op
era
tiv
ere
na
lfu
nct
ion
,
pre
vio
us
ren
al
surg
ery
on
ipsi
late
ral
uri
na
rytr
act
,
py
on
ep
hro
sis,
ex
tre
me
blo
od
loss
,p
erf
ora
tio
n
34
.36�
10
.41
[10
–4
5]
mm
NR
8/7
Ha
rms:
CG
,B
L,B
T,
AP
,S
P
Se
con
da
ryo
utc
om
es:
DP
PN
L2
4Fr
19
45
.94�
14
.69
[24
–7
2]1
1/8
37
.47�
10
.35
[17
–5
3]
mm
10
/9
PN
L2
6Fr
26
46
.19�
12
.24
[25
–7
1]1
7/9
37
.88�
14
.14
[10
–5
5]
mm
18
/8
PN
L2
8Fr
18
41
.88�
16
.53
[22
–6
9]8
/10
36
.49�
11
.33
[25
–5
0]
mm
9/9
PN
L3
0Fr
32
45
.37�
13
.80
[24
–7
2]2
1/1
13
7.5
3�
12
.23
[30
–5
5]
mm
15
/17
Xu
20
14
,co
mp
ara
tiv
est
ud
y,
Ch
ina
,2
01
1–
20
13
[26
]
mP
NL
16
Fr3
70
50
.3�
14
.81
3/2
42
2.7�
1.4
Re
na
lst
on
e>
20
mm
,ag
e>
18
an
d<
60
yr,
AS
AI
or
II
Kid
ne
ya
no
ma
lie
s,
un
con
tro
lle
dco
ag
ulo
pa
thy
,
pre
gn
an
cy,
imm
un
od
efi
cie
ncy
,
hy
pe
rte
nsi
on
,D
M,
he
art
dis
ea
se,
ren
al
insu
ffici
en
cy,
‘‘an
ym
ed
ica
lth
era
py
wh
ich
cou
lda
ffe
cth
em
od
yn
am
ic,
ele
ctro
lyte
,a
nd
me
tab
oli
c
cha
ng
es’
’,a
ny
pa
tie
nt
wh
ose
intr
ao
pe
rati
ve
irri
ga
tio
nti
me
wa
s<
60
or>
12
0m
in,
mu
ltip
letr
act
pro
ced
ure
s,
pa
tie
nts
wh
oh
ad
rece
ive
da
blo
od
tra
nsf
usi
on
33
.4�
10
.3m
mN
R2
2/1
5B
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Oth
er
ou
tco
me
s:v
olu
me
of
flu
id
ab
sorb
ed
PN
L2
4Fr
34
45
.3�
13
.51
3/2
12
2.8�
1.5
41
.4�
10
.9m
m1
8/1
6
Ya
ma
gu
chi
20
11
,co
mp
ara
tiv
e
stu
dy
,g
lob
al,
20
07
–2
00
9[2
7]�
18
Fr2
71
NR
NR
NR
NR
NR
Inco
mp
lete
info
rma
tio
n
(n=
26
6)
NR
NR
NR
Ha
rms:
BL,
BT
24
–2
6Fr
10
39
27
–3
0Fr
35
33
�3
2Fr
37
1
Mis
hra
20
11
,co
mp
ara
tiv
e
stu
dy
,In
dia
,2
00
9–
20
10
[24
]
mP
NL
14
–1
8Fr
26
NR
42
.2�
19
.81
8/8
23
.8�
2.6
Re
na
lst
on
es
10
–2
0m
m
Pe
dia
tric
pa
tie
nts
UT
I
Mo
rbid
ob
esi
ty
Un
corr
ect
ed
coa
gu
lop
ath
ies
14
7�
30
mm
22
(8%
)U
C
1(4
%)
MC
15
(58
%)
LC
9(3
5%
)P
8/1
9B
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DH
S,
DP
,
an
alg
esi
cre
qu
ire
me
nt
PN
L2
4–
28
Fr2
6N
R4
8.2�
16
.81
8/8
22
.6�
2.7
14
9�
60
mm
23
(12
%)
UC
2(8
%)
MC
10
(38
%)
LC
13
(50
%)
P
10
/18
Kn
oll
20
10
,co
mp
ara
tiv
est
ud
y,
Ge
rma
ny
,2
00
7–
20
09
[22
]
mP
NL
18
Fr2
5N
R5
2�
11
.6[2
7–
77
]2
.1:1
(17
/8
)27�
3.5
[19
–3
6]
Pa
tie
nts
wit
hso
lita
ryre
na
l
sto
ne
loca
ted
inlo
we
rp
ole
or
ren
al
pe
lvis
NR
18�
3.3
[10
–2
1]
mm
NR
NR
Be
ne
fits
:IS
FR
Ha
rms:
BL,
fev
er,
VI
Se
con
da
ryo
utc
om
es:
DP
,P
ain
:
VA
S,
AR
,D
HS
PN
L2
6Fr
25
48�
15
.5[2
3–
73
]1
.8:1
(16
/9
)29�
5.6
[19
–4
2]
22�
4.2
5[1
4–
29
]m
m
Giu
sti
20
07
,co
mp
ara
tiv
est
ud
y,
Ita
ly,
19
99
–2
00
4[1
1]
mP
NL
14
Fr4
00
an
d1
48
.0[2
9–
70
]2
0/
20
26
.0K
idn
ey
sto
ne<
20
mm
.
Incl
usi
on
crit
eri
afo
rT
LP
NL:
sin
gle
tra
ct,
ab
sen
ceo
f
coll
ect
ing
syst
em
pe
rfo
rati
on
an
db
lee
din
g,
com
ple
test
on
e
cle
ara
nce
NR
28
0m
m2
20
(50
%)
LC
20
(50
%)
P
21
/1
9B
en
efi
ts:
SFR
Ha
rms:
BL,
BT
Se
con
da
ryo
utc
om
es:
DP
,p
ain
:
VA
S,
AR
,D
HS
Oth
er
ou
tco
me
s:T
RN
A
PN
L3
0Fr
67
51
.3[1
9–
78
]3
6/
31
24
.63
10
mm
2N
R3
0/
37
TL
PN
L3
0Fr
27
48
.5[2
2–
77
]1
4/
13
23
.83
20
mm
2N
R1
2/
15
Mil
ler
20
14
,ca
sese
rie
s,U
K,
20
09
–2
01
3,
ab
stra
ct[3
2]
mP
NL
16
.5Fr
11
60
63
.2
(re
po
rte
da
s
‘‘av
era
ge
ag
e’’)
60
/5
6N
RN
RN
RN
RN
RN
RB
en
efi
ts:
ISFR
,IC
IRFR
,
Ha
rms:
CG
,B
T,
US
,S
P
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Bh
att
u2
01
4,
case
seri
es,
Ind
ia,
20
09
–2
01
3,
ab
stra
ct[2
9]
mP
NL
(�2
0Fr
)3
01
NR
42
NR
NR
NR
Act
ive
ble
ed
ing
dis
ord
er,
UT
I,
pre
gn
an
cy
14
.7�
4.3
mm
NR
NR
Be
ne
fits
:S
FR
Ha
rms:
CG
,B
L,S
P
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Ka
rata
g2
01
4,
case
seri
es,
Tu
rke
y,
20
13
,a
bst
ract
[31
]
mP
NL
68
NR
41
.4N
R2
6.3
NR
NR
12
2m
m2
NR
NR
Be
ne
fits
:S
FR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Oth
er
ou
tco
me
s:D
F
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X6
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046

Desai 2013, case series, India,
recruitment period NR,
abstract [30]
umPNL 12 Fr 74 1 NR
4 (5%) pediatric cases
NR NR umPNL NR 16.6 mm NR NR Benefits: SFR
Harms: CG, BL,
Secondary outcomes:
DHS
Other outcomes: conversion to
mPNL due to bleeding
Desai 2013, case series, India,
recruitment period NR [8]
umPNL 13 Fr 62 1 NR
4 (7%) pediatric cases
NR NR
2 (3%) obese
Renal stones
umPNL
NR 16.8 mm NR NR Benefits: SFR
Harms: CG, BL,
Secondary outcomes:
DHS
Other outcomes: conversion to
mPNL due to bleeding
Desai 2013, case series,
China, 2012 [20]
umPNL 11–13 Fr 36 1 48.2 � 15.7 [2–79]
No. pediatric cases NR
23 / 13 24.63
[18.1–33.2]
Renal stone
<20 mm
NR 14.9 � 4.1 [6–20] mm
Area:
160.6 � 82.7 [30–380] mm2
7 (19%) UC
8 (22%) MC
10 (28%) LC
3 (7%) Multiple C
5 (14%) P
3 (8%) UUr
21 / 15 Benefits: ISFR, SFR,
Harms: CG, BL, US
Secondary outcomes: DP, SP,
DHS
Other outcomes:
Puncture locations
Abdelhafez 2013, case series,
Germany, 2007–2011 [18]
mPNL 18 Fr
Stone size <20 mm
Stone size �20 mm 98
93
1
1
49.6 � 15.9
48.8 � 17.6
NR
NR
25.8 � 5.2
26.5 � 5.9
Consecutive patients with
stones >15 mm or lower calyx
stones >8 mm, or any
previously failed SWL and URS
NR
13.6 � 3.4 mm
37.5 � 22.9 mm
NR NR Benefits: ISFR, SFR,
Harms: CG, BL, BT
Secondary outcomes: DP, SP,
DHS
Zimmermans 2012, case series,
recruitment period NR,
Germany, abstract [33]
mPNL, 18 Fr
All patients, all stone sizes
Stones �500 mm2 652
183
NR 54.1 � 15.7 NR NR mPNL Access not possible
410 mm2
950 mm2
NR NR Benefits: ISFR
Harms: CG, BL, BT, VI
Secondary outcomes: DP, SP
Lu 2012, case series, China,
2009–2010 [23]
Tubeless mPNL
Standard mPNL
(with 16 Fr nephrostomy tube)
16
16
0.5 43.81 � 18.89
46 � 22.37
6/10
7/9
NR Pelvic stone <40 mm Urinary tract obstruction
(BPH, UPJ stenosis), UTI,
Coagulopathies
32.9 � 6.2 mm
31.1 � 6.2 mm
NR
NR
NR Benefits: ISFR
Harms: CG, BL,
Secondary outcomes: DHS, DP,
pain
Sung 2006, case series, Korea,
1999–2002 [25]
mPNL 14 Fr 72 7.2 � 8.3
[0.5–37]
49.5 � 14.7 [1.4–73] 45/27 NR Failed SWL and/or URS
(n = 19), large stone burden
(>600 mm2) (n = 25), P and/or
LC stones, (n = 62), UC stones
(n = 2), calyceal diverticulum
stone (n = 1)
1 pediatric case
31/72 patients had >2
indications
NR 34.2 � 19.9 [6–102] mm 62 (86%) P and/or LC
2 (2%) UC
1 (1%) calyceal
diverticulum
31/41 Benefits: ISFR, SFR
Harms: fever, BL
Secondary outcomes: SP, DHS
AP = adjunctive procedure; BL = blood loss; BT = blood transfusion; C = calyx; CG = Clavien grade; CIRFR = clinically insignificant residual fragment rate; DB = database; DHS = duration of hospital stay; DP = duration of
procedure; EDV = emergency department visit; FU = follow-up (here meaning time point for delayed assessment of stone status, if applicable); HR = hospital readmission; ISFR = immediate SFR; ICIRFR = immediate CIRFR;
LC = lower calyceal; MC = middle calyceal; mPNL = mini-PNL; NR = not reported; P = pelvis; PNL = percutaneous nephrolithectomy; QOL = quality of life; RCT = randomized controlled trial; SFR = stone-free rate;
SP = secondary procedure; UC = upper calycal; umPNL = ultra-mini-PNL; UPJ = ureteropelvic junction; URS = ureteroscopy; US = urosepsis; UUr = upper ureteral; VI = visceral injury.
E U
R O
P E
A N
U
R O
L O
G Y
X
X X
(
2 0
1 7
)
X X
X –
X X
X
7
EU
RU
RO
-72
40
; N
o.
of
Pa
ge
s 1
6
Ple
ase
cite th
is a
rticle in
pre
ss a
s: R
uh
ay
el
Y,
et
al.
Tra
ct S
izes
in M
inia
turize
d P
ercu
tan
eo
us
Ne
ph
rolith
oto
my
: A
Sy
stem
atic
Re
vie
w fro
m th
e E
uro
pe
an
Asso
ciatio
n o
f U
rolo
gy
Uro
lithia
sis G
uid
elin
es
Pa
ne
l. E
ur
Uro
l (2
01
7),
http
://dx
.do
i.org
/10
.10
16
/j.e
uru
ro.2
01
7.0
1.0
46

Ta
ble
2–
Ou
tco
me
sfo
ra
llth
est
ud
ies
incl
ud
ed
Stu
dy
ID,
de
sig
n,
cou
ntr
y,
recr
uit
me
nt
pe
rio
d
Su
bg
rou
ps
(of
mP
NL
gro
up
)
Inte
rve
nti
on
Co
mp
ara
tor
Ou
tco
me
s
me
asu
red
na
tb
ase
lin
eO
utc
om
es
Re
po
rte
d
pv
alu
es
No
tes
Su
mm
ary
Int
Co
mIn
tC
om
Te
pe
ler
20
14
,R
CT
,
Tu
rke
y,
20
12
–2
01
3[2
8]
NA
mP
NL
4.8
FrP
NL
30
FrB
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L
Se
con
da
ry
ou
tco
me
s:D
P,
DH
S
Oth
er:
intr
are
na
l
pe
lvic
pre
ssu
re
10
10
ISFR
:8
(80
%)
CG
1:
1(1
0%
)
BL:
1.8
%�
0.8
%(0
.9–
3.2
%)
DP
:3
6.5�
14
.2(2
0–
60
)m
in
DH
S:1
.1�
0.3
(1–
2)
d
IPP
:3
0.3�
3.9
mm
Hg
ISFR
:9
(90
%)
CG
3a
:1
(10
%)
BL:
3.5
%�
1.5
%(1
.2–
6.1
%)
DP
:4
9�
9.8
(32
–6
5)
min
DH
S:2�
0.5
(1–
3)
d
IPP
:2
0.1�
3.1
mm
Hg
1 0.0
04
0.0
34
0.0
01
<0
.00
01
BL
rep
ort
ed
as
pe
rce
nt
dro
pin
he
ma
tocr
it
mP
NL
vs
PN
Lsh
ow
ed
no
ISFR
be
ne
fit,
alt
ho
ug
hB
La
nd
DP
we
relo
we
r.IP
Pw
as
hig
he
rin
the
mP
NL
gro
up
Ch
en
g2
01
0,
RC
T,
Ch
ina
,2
00
4–
20
07
[19
]
To
tal
Sta
gh
orn
sto
ne
s(S
S)
Sim
ple
ren
al
pe
lvic
sto
ne
s(S
RP
S)
Mu
ltip
leca
lyce
al
sto
ne
s(M
CS
)
mP
NL
16
FrP
NL
24
FrB
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L
Se
con
da
ry
ou
tco
me
s:D
HS
,
DP
,a
na
lge
sic
req
uir
em
en
t
72
18
27
27
11
5
29
46
40
BL:
0.5
3�
0.7
9g
/dL
BT
:1
(1.4
%)
Pn
eum
oth
ora
x:
1(1
.4%
)
Uri
ne
leak
age:
0(0
%)
DH
S:7
.3(6
–1
2)
d
AR
(pet
hid
ine)
:8
8.7�
40
.6m
g
VA
S(1
–2
d)
SFR
for:
SS:
13
/18
(72
.2%
)
SRP
S:2
5/2
7(9
2.6
%)
MC
S:2
3/2
7(8
5.2
%)
DP
for:
SS:
13
4.4�
19
.7m
in
SRP
S:8
9.4�
21
.5m
in
MC
S:1
13
.9�
20
.3m
in
BL:
0.9
7�
1.4
2g
/dL
BT
:1
2(1
0.4
%)
Pn
eum
oth
ora
x:
0
Uri
ne
leak
age:
2(1
.7%
)
DH
S:7
.5(6
–1
5)
d
AR
(pet
hid
ine)
:9
4.3�
37
.2m
g
VA
S(1
–2
d)
SFR
for:
SS:
22
/29
(75
.9%
)
SRP
S:4
0/4
6(9
1.3
%)
MC
S:2
8/4
0(7
0.0
%)
DP
for:
SS:
11
8.9�
21
.5m
in
SRP
S:7
7�
17
.6m
in
MC
S:1
01
.2�
19
.1m
in
<0
.05
<0
.05
>0
.05
>0
.05
>0
.05
>0
.05
>0
.05
>0
.05
>0
.05
<0
.05
<0
.05
<0
.05
<0
.05
BL
an
dn
ee
dfo
rB
Tw
ere
low
er
inm
PN
Lg
rou
p,
ho
we
ve
rst
on
es
we
ren
ot
full
y
com
pa
rab
le.
mP
NL
resu
lts
mo
stfa
vo
rab
lefo
rm
ult
iple
caly
cea
lst
on
es.
DP
wa
slo
ng
er
inm
PN
Lg
rou
p.
Ka
rak
ose
20
14
,
com
pa
rati
ve
stu
dy
,
Tu
rke
y,
20
11
–2
01
2[2
1]
NA
mP
NL
22
FrU
ncl
ea
r–
chi–
squ
are
test
use
d
Ha
rms:
CG
,B
L,B
T,
AP
,S
P
Se
con
da
ry
ou
tco
me
s:D
P
Oth
er
ou
tco
me
s:
pre
op
vs
po
sto
p
cre
ati
nin
e
15
NA
CG
1:
1,
CG
2:
0
Pre
op
Hb
:1
4.3�
1.5
[11
.6–
17
]g
/dl
Po
sto
pH
b:
13
.7�
1.7
[10
.2–
16
.1]
g/d
l
BT
(n):
0
AP
(n):
4
SP(n
):0
DP
:1
02
.8�
30
.0[5
5–
12
6]
min
Re
fere
nce
gro
up
for
sta
tist
ica
l
an
aly
sis
no
tst
ate
d
PN
L2
4Fr
19
CG
1:
2,
CG
2:
0
Pre
op
Hb
:1
3.9�
1.8
[9.1
0–
17
]g
/dl
Po
sto
pH
b:
12
.9�
1.7
[9.6
–1
5.3
]g
/dl
BT
(n):
0
AP
(n):
2
SP(n
):0
DP
:1
05
.5�
39
.5[7
5–
21
0]
min
PN
L2
6Fr
26
CG
1:
1,
CG
2:
2
Pre
op
Hb
:1
4.7�
1.4
[11
.7–
17
]g
/dl
Po
sto
pH
b:
12
.3�
2.1
[7.9
–1
4.7
]g
/dl
BT
(n):
2
AP
(n):
0
SP(n
):0
DP
:1
03
.7�
40
.5[4
0–
11
5]
min
PN
L2
8Fr
18
CG
1:
0,
CG
2:
4
Pre
op
Hb
:1
4.4�
1.4
[11
.6–
16
.9]
g/d
l
Po
sto
pH
b:
11
.7�
1.8
[8.5
–1
4.1
]g
/dl
BT
(n):
4
AP
(n):
0
SP(n
):0
DP
:1
10
.6�
45
.3[7
0–
24
0]
min
PN
L3
0Fr
32
CG
1:
3,
CG
2:
7
Pre
op
Hb
:1
4.2�
1.6
[9.1
0–
17
]g
/dl
Po
sto
pH
b:
10
.4�
1.8
[8.3
–1
2.3
]g
/dl
BT
(n):
7
AP
(n):
2
SP(n
):0
DP
:1
08
.1�
48
.6[6
5–
22
0]
min
>0
.05
<0
.05
>0
.05
Xu
20
14
,co
mp
ara
tiv
e
stu
dy
,C
hin
a,
20
11
–2
01
3[2
6]
NA
mP
NL
16
FrP
NL
24
FrB
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L
Se
con
da
ry
ou
tco
me
s:D
P,
DH
S
Oth
er
ou
tco
me
s:
vo
lum
eo
ffl
uid
ab
sorb
ed
37
34
ISFR
:2
9/3
7(7
8%
)
CG
2:
5(1
3.3
%)
BL:
7.4�
3.5
g/l
DP
:1
15
.4�
13
.5m
in
DH
S:9
.8�
3.4
d
ISFR
:2
7/3
4(7
9%
)
CG
:5
(14
.7%
)
BL:
9.6�
4.0
g/l
DP
:1
10
.6�
17
.0m
in
DH
S:9
.3�
3.0
d
0.9
15
1.0
00
0.0
15
0.1
88
0.5
73
No
tra
nd
om
ize
d:
sele
ctio
no
f
tech
niq
ue
ba
sed
on
join
t
de
cisi
on
by
surg
eo
ns
an
d
pa
tie
nts
.S
ton
es
inP
NL
gro
up
sig
nifi
can
tly
larg
er
BL
wa
ssi
gn
ifica
ntl
ylo
we
rin
mP
NL
gro
up
,h
ow
ev
er
sto
ne
s
tre
ate
dw
ere
sma
lle
r.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X8
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046

Ya
ma
gu
chi
20
11
,
com
pa
rati
ve
stu
dy
,
Glo
ba
l,2
00
7–
20
09
[27
]
NA
�1
8Fr
NA
Ha
rms:
BL,
BT
27
1N
AB
L:1
1(4
.1%
)
BT
:3
(1.1
%)
NA
NR
CR
OE
Sd
ata
ba
se
BT
rate
sd
iffe
rsl
igh
tly
be
twe
en
Ta
ble
s5
an
d8
(aft
er
sum
min
g
dil
ata
tio
nm
eth
od
s).
Da
tafo
rB
L
calc
ula
ted
fro
mT
ab
le8
(to
tal
of
bo
thd
ila
tati
on
me
tho
ds)
.D
ata
for
BT
are
as
sta
ted
inT
ab
le5
.
Fact
ors
pre
dic
tiv
eo
fb
lee
din
g
com
pli
cati
on
sin
clu
de
she
ath
size
24
–2
6Fr
10
39
BL:
53
(5.1
%)
BT
:5
0(4
.8%
)
27
–3
0Fr
35
33
BL:
30
6(8
.7%
)
BT
:2
08
(5.9
%)
�3
2Fr
37
1B
L:3
3(8
.9%
)
BT
:4
5(1
2.1
%)
Mis
hra
20
11
,
com
pa
rati
ve
stu
dy
,
Ind
ia,
20
09
–2
01
0[2
4]
NA
mP
NL
14
–1
8Fr
PN
L2
4–
28
FrB
en
efi
ts:
SFR
(at
1m
o)
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DH
S,
DP
,a
na
lge
sic
req
uir
em
en
t
27
28
SFR
:2
6/2
7(9
6)%
BL:
0.8�
0.9
%
Pel
vic
per
fora
tio
n:
1
Ble
edin
g0
Fev
er:
2
DP
:4
5.2�
12
.6m
in
DH
S:3
.2�
0.8
d
AR
(tra
mad
ol)
:5
5.4�
50
mg
TL:
21
(78
%)
SFR
:2
8/2
8(1
00
%)
BL:
1.3�
0.4
%
Pel
vic
per
fora
tio
n:
2
Ble
edin
g4
Fev
er4
DP
:3
1�
16
.6m
in
DH
S:4
.8�
0.6
d
AR
(tra
mad
ol)
:7
0.2�
52
mg
TL:
4(1
4%
)
0.4
9
0.0
09
8
1 0.1
1
0.6
6
0.0
00
8
<0
.00
00
1
0.2
8
<0
.00
1
BL
rep
ort
ed
as
pe
rce
nt
dro
pin
he
ma
tocr
it.
En
erg
yso
urc
efo
rst
on
e
fra
gm
en
tati
on
:
Lase
rfo
rm
PN
L(1
9/1
)
Pn
eu
ma
tic
for
sta
nd
ard
(22
/0)
mP
NL
ha
dsi
mil
ar
SFR
for
1–
2-c
mk
idn
ey
sto
ne
s.
De
spit
elo
ng
er
op
era
tio
n
tim
e,
mP
NL
ha
dsh
ort
er
DH
S
an
dh
igh
er
tub
ele
ssra
te
rela
ted
tole
ssb
lee
din
g
Kn
oll
20
10
,co
mp
ara
tiv
e
stu
dy
,G
erm
an
y,
20
07
–2
00
9[2
2]
NA
mP
NL
18
FrP
NL
26
FrB
en
efi
ts:
ISFR
Ha
rms:
BL,
fev
er,
VI
Se
con
da
ryo
utc
om
es:
DP
,
Pa
in:
VA
S,
AR
,D
HS
25
25
ISFR
:2
4/2
5(9
6%
)
BL:
1/2
5(4
%)
Fev
er:
3/2
5(1
2%
)
VI
(pe
rfo
rati
on
):0
(0%
)
DP
:5
9�
29
.1[3
4–
82
]m
in
Pai
n,
VA
S:3�
3[0
–5
]
AR
(pir
itra
mid
e):
25�
12
mg
DH
S:3
.8�
2.1
d
ISFR
:2
3/2
5(9
2%
)
BL:
2/2
5(8
%)
Fev
er:
5/2
5(2
0%
)
VI
(pe
rfo
rati
on
):1
(4%
)
DP
:4
9�
21
.7[2
6–
73
]m
in
Pai
n,
VA
S:4�
3[1
–7
]
AR
(pir
itra
mid
e):
37�
10
mg
DH
S:6
.9�
2.9
d
NR
NS
0.0
48
NS
0.0
21
Sto
ne
ssi
gn
ifica
ntl
yla
rge
r
(p=
0.0
42
)in
PN
Lg
rou
p.
mP
NL
wa
sT
Lw
ith
thro
mb
in-
ma
trix
tra
ctcl
osu
reif
un
com
pli
cate
da
nd
sto
ne
-fre
e.
Oth
erw
ise
16
Frtu
be
wa
s
pla
ced
.
All
PN
Lh
ad
22
Frtu
be
.B
L
rep
ort
ed
as
‘‘pro
lon
ge
d
po
sto
pe
rati
ve
ble
ed
ing
’’,
alt
ho
ug
hn
op
ati
en
tsre
qu
ire
d
BT
Sh
ort
er
ho
spit
al
sta
ya
nd
less
po
sto
pe
rati
ve
pa
inm
ay
sup
po
rtu
seo
fm
PN
Lfo
r
sma
lle
ra
nd
inte
rme
dia
te
sto
ne
s.Lo
we
rst
on
eb
urd
en
an
dT
Lfa
shio
no
fm
PN
L,m
ay
ha
ve
infl
ue
nce
dre
sult
s
Giu
sti
20
07
,
com
pa
rati
ve
stu
dy
,
Ita
ly,
19
99
–2
00
4[1
1]
NA
mP
NL
14
FrP
NL
30
FrB
en
efi
ts:
SFR
Ha
rms:
BL,
BT
Se
con
da
ryo
utc
om
es:
DP
,
pa
in:
VA
S,
AR
,D
HS
Oth
er
ou
tco
me
s:T
RN
A
40
67
mP
NL
14
Fr
SFR
:3
1/4
0(7
7.5
%)
BL:
4.4
9�
3.1
%
BT
:0
/40
(0%
)
DP
:1
55
.5�
32
.9m
in
Pai
nV
AS:
5.5
3�
1.1
4
AR
(su
bst
ance
NR
):7
3.8�
50
mg
DH
S:3
.05�
1.6
9d
TR
NA
:1
2.3
1�
4.6
5d
PN
L3
0Fr
SFR
:6
3/6
7(9
4%
)
BL:
6.3
1�
4.2
9%
BT
:2
/67
(2.9
%)
DP
:1
06
.6�
24
.4m
in
Pai
nV
AS:
6.3
6�
1.6
7
AR
:8
8.1�
78
.5m
g
DH
S:5
.07�
2.1
5d
TR
NA
:1
7.6
7�
4.7
d
NR
NR
BL
rep
ort
ed
as
pe
rce
nt
dro
pin
he
ma
tocr
it.
An
alg
esi
csu
bst
an
ce
NR
.SD
for
ag
es
NR
.La
cko
f
sta
tist
ica
lca
lcu
lati
on
sfo
re
ve
n
imp
ort
an
to
utc
om
es
such
as
SFR
,d
esp
ite
con
clu
sio
ns
be
ing
dra
wn
for
this
ou
tco
me
mP
NL
SFR
an
dB
Lw
ere
low
er
tha
nfo
rsP
NL.
TL
sPN
Lw
as
sup
eri
or
inte
rms
of
red
uce
d
pa
in,
sho
rte
rh
osp
ita
lst
ay
,
an
dh
igh
er
SFR
,w
hil
e
sho
win
gsi
mil
ar
com
pli
cati
on
rate
s
Tu
be
less
PN
L3
0Fr
27
TL
PN
L3
0FR
SFR
:2
7/2
7(1
00
%)
BL:
5.1
8�
3.6
3
BT
:1
/27
(3.7
%)
DP
:9
5.9�
45
.5m
in
Pai
nV
AS:
3.4
5�
0.6
5
AR
:4
1.1�
30
.2m
g
DH
S:2
.18�
2.1
3d
TR
NA
:1
0.9
3�
4.8
7d
Mil
ler
20
14
,ca
sese
rie
s,
UK
,2
00
9–
20
13
,
ab
stra
ct[3
2]
NA
mP
NL
16
.5Fr
NA
Be
ne
fits
:IS
FR,
ICIR
FR,
Ha
rms:
CG
,B
T,
US
,S
P
Se
con
da
ryo
utc
om
es:
DP
,D
HS
11
6N
AIS
FR:
54
(46
.5%
)
ICIR
FR:
79
.4%
CG
:2
[BT
]3
(2.6
%)
+2
[IN
F]1
8(1
6%
)
BT
:3
(2.6
%)
US
:1
5(1
2.9
%)
DP
:1
74
min
SP
:2
4(2
0.7
%):
SW
L1
0(8
.6%
),U
RS
9
(7.8
%),
PN
L5
(4.3
%)
DH
S:
3.9
d
NA
NR
Co
mp
ari
son
of
retr
osp
ect
ive
ly
rev
iew
ed
case
so
fm
PN
La
nd
PN
L
fro
mC
RO
ES
da
tab
ase
,b
ut
no
com
pa
riso
nd
ata
or
pv
alu
es
incl
ud
ed
inth
ea
bst
ract
Bh
att
u2
01
4,
case
seri
es,
Ind
ia,
20
09
–2
01
3,
ab
stra
ct[2
9]
NA
mP
NL�
20
FrN
AB
en
efi
ts:
SFR
Ha
rms:
BL,
CG
Se
con
da
ryo
utc
om
es:
DP
,D
HS
,A
R
30
1N
AS
FR:
29
7(9
9%
)
BL:
1.0
1g
/dl
CG
1:
2%
,C
G2
:5
%
DP
:5
9m
in
DH
S:
2.9
d
AR
(tra
ma
do
l):
54
mg
NA
NR
Ure
teri
cca
the
ter:
98
Ure
teri
cca
the
ter
+
ne
ph
rost
om
y:
26
DJ
ste
nt:
11
0
DJ
ste
nt
+n
ep
hro
sto
my
:2
8
Ne
ph
rost
om
y:
39
mP
NL
isa
lte
rna
tiv
eto
sta
nd
ard
PN
Lfo
rm
ed
ium
ren
al
sto
ne
s,w
ith
be
tte
r
mo
rbid
ity
pro
file
.H
ow
ev
er
the
reis
no
com
pa
riso
ng
rou
p.
Tu
be
less
mP
NL
ass
oci
ate
d
wit
hb
ett
er
mo
rbid
ity
pro
file
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 9
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046

Ta
ble
2(C
on
tin
ued
)
Stu
dy
ID,
de
sig
n,
cou
ntr
y,
recr
uit
me
nt
pe
rio
d
Su
bg
rou
ps
(of
mP
NL
gro
up
)
Inte
rve
nti
on
Co
mp
ara
tor
Ou
tco
me
s
me
asu
red
na
tb
ase
lin
eO
utc
om
es
Re
po
rte
d
pv
alu
es
No
tes
Su
mm
ary
Int
Co
mIn
tC
om
Ka
rata
g2
01
4,
case
seri
es,
Tu
rke
y,
20
13
,a
bst
ract
[31
]
NA
mP
NL
4.8
FrN
AB
en
efi
ts:
SFR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DP
,D
HS
Oth
er
ou
tco
me
s:D
F
68
NA
SFR
:9
8.5
%
BL:
0.9
5g
/dl
CG
1:
1.4
%+
3a
:4
.2%
DP
:4
0m
in
DH
S:
27
.5h
DF:
10
8s
NA
NR
NA
mP
NL
reco
mm
en
de
da
s
alt
ern
ati
ve
for
me
diu
mre
na
l
sto
ne
sre
sist
an
tto
SW
L
De
sai
20
13
,ca
sese
rie
s,
Ind
ia,
recr
uit
me
nt
pe
rio
dN
R,
ab
stra
ct[3
0]
NA
um
PN
L1
2Fr
NA
Be
ne
fits
:S
FR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DH
S
Oth
er
ou
tco
me
s:
con
ve
rsio
nto
mP
NL
du
eto
ble
ed
ing
74
NA
SFR
:9
2.4
%
CG
1:
1(1
.4%
)
BL:
1.6�
1.0
g/d
l
DH
S:1
.2�
0.8
d
Co
nv
ersi
on
tom
PN
L:2
(2.7
%)
NA
NR
FU:
1m
ou
mP
NL
ve
rysa
fea
nd
effi
caci
ou
sfo
rre
mo
va
lo
f
ren
al
calc
uli
up
to1
8m
m.U
se
of
dis
po
sab
les
ism
inim
al
an
d
pa
tie
nt
reco
ve
ryfa
st
De
sai
20
13
,ca
sese
rie
s,
Ind
ia,
recr
uit
me
nt
pe
rio
dN
R[8
]
NA
um
PN
L1
3Fr
NA
Be
ne
fits
:S
FR
Ha
rms:
CG
,B
L,
Se
con
da
ryo
utc
om
es:
DH
S
Oth
er
ou
tco
me
s:
con
ve
rsio
nto
mP
NL
du
eto
ble
ed
ing
62
NA
SFR
:8
6.6
6%
CG
1(1
.6%
)
BL:
1.4�
1.0
g/d
l
DH
S:1
.2�
0.8
d
Co
nv
ersi
on
tom
PN
L:2
(3.2
%)
NA
NR
FU:
1m
ou
mP
NL
issa
fea
nd
ea
syto
lea
rnb
ut
sho
uld
be
rest
rict
ed
tom
ed
ium
sto
ne
s(<
2.0
cm)
De
sai
20
13
,ca
sese
rie
s,
Ch
ina
,2
01
2[2
0]
NA
um
PN
L1
1–
13
FrN
AB
en
efi
ts:
ISFR
,S
FR,
Ha
rms:
CG
,B
L,U
S
Se
con
da
ryo
utc
om
es:
DP
,S
P,
DH
S
Oth
er
ou
tco
me
s:
Pu
nct
ure
loca
tio
ns
36
NA
ISFR
:8
8.9
0%
SFR
:9
7.2
0%
CG
1:
3(8
.3%
),C
G2
:2
(5.6
%)
BL:
5.4�
7.8
[0–
21
]g
/dl
US:
2(5
.6%
)
DP
:5
9.8�
15
.9[3
0–
90
]m
in
SP:
1(2
.8%
)
DH
S:3
.0�
0.9
[2–
5]
d
NA
NR
FU:
1m
o
Pu
nct
ure
loca
tio
ns:
Up
pe
rca
lyx
:7
(19
.4%
)
Mid
dle
caly
x:
15
(41
.7%
)
Low
er
caly
x:
14
(38
.9%
)
um
PN
Lsa
fea
nd
effi
caci
ou
s
alt
ern
ati
ve
for
sma
ll-v
olu
me
dis
ea
sew
ith
ad
va
nta
ge
of
hig
hIS
FRa
nd
fin
al
SFR
an
d
low
er
com
pli
cati
on
rate
s.
Ind
ica
tio
ns
for
um
PN
La
re
mo
de
rate
-siz
ed
sto
ne
sa
s
alt
ern
ati
ve
toE
SW
Lo
rR
IRS
,
low
po
lest
on
es
no
ta
me
na
ble
toR
IRS
,d
ive
rtic
ula
rre
na
l
sto
ne
s,a
nd
sto
ne
sre
fra
cto
ry
toE
SW
L
Ab
de
lha
fez
20
13
,
case
seri
es,
Ge
rma
ny
,
20
07
–2
01
1[1
8]
Sto
ne
size
<2
cmm
PN
L1
8Fr
NA
Be
ne
fits
:IS
FR,
SFR
,
Ha
rms:
CG
,B
L,B
T
Se
con
da
ryo
utc
om
es:
DP
,S
P,
DH
S
98
NA
Sto
ne
size
<2
0m
m
ISFR
:9
0.8
%
SFR
:9
8.9
%
CG
1:
9(9
.2%
),C
G2
(2.0
%):
5(5
.1%
),C
G
3:
5(5
.1%
)
BL:
1.3�
0.9
g/d
l
BT
:0
(0%
)
DP
:6
9.2�
34
.8m
in
SP:
8(8
.16
%)
DH
S:3
.7�
1.2
d
Sto
ne
size�
20
mm
ISFR
:7
6.7
%
SFR
:9
4.6
%
CG
1:
14
(15
%),
CG
2:
6(6
.5%
),C
G3
:5
(5.4
%)
BL:
1.7�
1.2
g/d
l
BT
:1
(1.1
%)
DP
:9
7.4�
48
.7m
in
SP:
17
(18
.3%
)
DH
S:4
.3�
1.5
d
0.0
07
0.1
0.2
0.0
15
NR
<0
.00
1
0.0
02
FU:
1m
oT
ota
lS
FRg
rea
ter
for
sma
ll
sto
ne
s.M
ost
pa
tie
nts
cou
ldb
e
ren
de
red
sto
ne
-fre
ew
ith
1a
ux
ilia
ryp
roce
du
re.
Th
e
hig
hsu
cce
ssra
tea
nd
low
rate
of
hig
he
rg
rad
eco
mp
lica
tio
ns
just
ify
mP
NL
for
larg
est
on
es
Sto
ne
size�
2cm
93
Zim
me
rma
ns
20
12
,
case
seri
es,
Ge
rma
ny
,
recr
uit
me
nt
pe
rio
dN
R,
ab
stra
ct[3
3]
All
pa
tie
nts
,a
llst
on
esi
zes
mP
NL
18
FrN
AB
en
efi
ts:
ISFR
Ha
rms:
CG
,B
L,B
T,
VI
Se
con
da
ryo
utc
om
es:
DP
,S
P
65
2N
AA
llst
on
esi
zes
ISFR
:9
3.6
%
CG
2[P
N]:
49
(7.5
%),
CG
3
[BL]
:2
(0.3
%)
CG
4[C
I]:
1(0
.15
%)
BL:
1(0
.15
%)
AV
F,2
(0.3
%)
recu
rre
nt
ble
ed
ing
s
BT
:9
(1.4
%)
VI:
1(0
.15
%)
cere
bra
lis
che
mia
DP
:6
5�
31
min
SP:
17
2(2
6.4
%)
Su
bg
rou
p:
sto
ne
s�
50
0m
m2
ISFR
:9
1.8
%
CG
2[P
N]:
16
(8.7
%)
BL:
NR
BT
:2
(1.1
%)
VI:
NR
DP
:7
7�
34
min
SP:
65
(35
.5%
)
NR
2/3
pa
tie
nts
wit
hre
curr
en
t
ble
ed
ing
or
AV
Fre
qu
ire
d
rad
iolo
gic
al
inte
rve
nti
on
mP
NL
isre
lia
ble
an
de
ffe
ctiv
e
tech
niq
ue
for
pe
rcu
tan
eo
us
surg
ery
.mP
NL
ise
ffe
ctiv
ea
nd
eq
ua
lly
safe
for
larg
er
sto
ne
bu
rde
ns
Su
bg
rou
po
fst
on
es�
5cm
21
83
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X10
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A SystematicReview from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/j.eururo.2017.01.046

Lu2
01
2,
case
seri
es,
Ch
ina
,2
00
9–
20
10
[23
]
NA
mP
NL
18
Fr
(wit
h1
6Fr
ne
ph
rost
om
ytu
be
)
NA
Be
ne
fits
:IS
FR
Ha
rms:
CG
,B
L
Se
con
da
ryo
utc
om
es:
DH
S,
DP
,p
ain
16
NA
Tu
be
dm
PN
L
ISFR
:1
3(8
1.3
%)
CG
:1
:2
(12
.5%
)
BL:
2.1
4�
0.5
1
TL
mP
NL
ISFR
:1
4(8
7.5
%)
CG
:1
:3
(18
.8%
)
BL:
1.9
1�
0.6
2
1 1 0.2
6
0.4
3
0.0
03
0.0
32
TL
mP
NL
ha
sth
ea
dv
an
tag
es
of
sho
rte
rh
osp
ita
lst
ay
an
d
less
ba
ckp
ain
com
pa
red
to
tub
ed
mP
NL
Tu
be
less
mP
NL
18
Fr1
6D
P:
65
.19�
21
.5
Pai
n:
14
(87
.5%
)
DH
S:4
(3–
12
)d
Oth
er:
uri
nar
yex
trav
asat
ion
:0
DP
:5
9.6
9�
17
.95
Pai
n:
5(3
1.3
%)
DH
S:3
(2–
7)
d
Oth
er:
uri
nar
yex
trav
asat
ion
:1
Su
ng
20
06
,ca
sese
rie
s,
Ko
rea
,1
99
9–
20
02
[25
]
NA
mP
NL
14
FrN
AB
en
efi
ts:
ISFR
,S
FR
Ha
rms:
fev
er,
BL
Se
con
da
ryo
utc
om
es:
SP
,D
HS
72
NA
ISFR
:5
8/7
2(8
0.6
%)
SFR
:6
3/7
2(8
7.5
%)
CG
1[f
ev
er]
:7
(9.7
%),
CG
3[e
mb
oli
zed
he
mo
rrh
ag
e]:
1(1
.4%
)
BL:
1/7
2(1
.4%
)
SP
:1
1/7
2(1
5.3
%)
DH
S:
7.6
8�
3.2
1[4
–2
2]
d
NA
NR
FU:
7m
oH
igh
ISFR
infl
ue
nce
db
yst
on
e
dia
me
ter
an
db
urd
en
.Lo
w
com
pli
cati
on
rate
an
dsh
ort
ho
spit
al
sta
y
AP
=a
dju
nct
ive
pro
ced
ure
;A
R=
an
alg
esi
cre
qu
ire
me
nt;
BL
=b
loo
dlo
ss;
BT
=b
loo
dtr
an
sfu
sio
n;
CG
=C
lav
ien
gra
de
;C
IRFR
=cl
inic
all
yin
sig
nifi
can
tre
sid
ua
lfr
ag
me
nt
rate
;C
RO
ES
=C
lin
ica
lR
ese
arc
hO
ffice
of
the
En
do
uro
log
ica
lS
oci
ety
;D
B=
da
tab
ase
;D
HS
=d
ura
tio
no
fh
osp
ita
lst
ay
;D
P=
du
rati
on
of
pro
ced
ure
;E
DV
=e
me
rge
ncy
de
pa
rtm
en
tv
isit
;FU
=fo
llo
w-u
p(h
ere
me
an
ing
tim
ep
oin
tfo
rd
ela
ye
da
sse
ssm
en
to
fst
on
est
atu
s,if
ap
pli
cab
le);
HR
=h
osp
ita
lre
ad
mis
sio
n;
IPP
=in
tra
ren
al
pe
lvic
pre
ssu
re;
ISFR
=im
me
dia
teS
FR;
ICIR
FR=
imm
ed
iate
CIR
FR;
LC=
low
er
caly
ces;
MC
=m
idd
leca
lyce
s;m
PN
L=
min
i-P
NL;
NR
=n
ot
rep
ort
ed
;P
=p
elv
is;
PN
L=
pe
rcu
tan
eo
us
ne
ph
roli
the
cto
my
;Q
OL
=q
ua
lity
of
life
;R
CT
=ra
nd
om
ize
dco
ntr
oll
ed
tria
l;S
FR=
sto
ne
-fre
era
te;
SP
=se
con
da
ryp
roce
du
re;
sPN
L=
sta
nd
ard
PN
L;T
L=
tub
ele
ss;
TR
NA
=ti
me
tore
turn
ton
orm
al
act
ivit
ies;
UC
=u
pp
er
caly
ces;
um
PN
L=
ult
ra-m
ini-
PN
L;U
PJ
=u
rete
rop
elv
icju
nct
ion
;U
S=
uro
sep
sis;
VI
=v
isce
ral
inju
ry.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 11
EURURO-7240; No. of Pages 16
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
3.5. Case series
Ten case series were included, five of which were full-text
articles [8,18,20,23,25] and five congress abstracts [29–
33]. The smallest tract size studied was 4.8 Fr (mPNL) in a
case series of 68 patients (70 renal units) [31]. SFR was high
(98.5%), while blood loss, complication rates, procedure
duration, and hospital stay were low (Table 2). Three
studies [8,20,30] involved case series in which patients
(n = 74, 62, and 26, respectively) were treated using tract
sizes of 11–13 Fr. SFRs were high (92.4%, 86.7%, and 97.2%,
respectively), while blood loss, complication rates, proce-
dure duration, and hospital stay were low (Table 2).
Conversion to mPNL occurred in approximately 3% of the
procedures. One study of 72 patients treated with 14 Fr
mPNL [25] had SFR of 87.5% and an extended hospital stay
of 7.7 � 3.2 d (range 4–22). Two studies reported on a tract
size of 18 Fr. Lu et al [23] compared procedures with and
without placement of a final nephrostomy tube (both n = 16)
[23], and Abdelhafez et al [18] compared stones measuring in
<20 mm (n = 98) to stones measuring �20 mm (n = 93) in
maximal diameter. Lu et al [23] found that ISFRs were
comparable, but that tubeless procedures were associated
with fewer patients reporting back pain (p = 0.003) and
shorter hospital stay (3 vs 4 d; p = 0.032; Table 2). Abdelhafez
et al [18] found that the ISFR was higher for patients with
smaller stones (90.8% vs 76.7%; p = 0.007), while the SFRs at
1 mo after auxiliary procedures were comparable (98.9% vs
94.6%; p = 0.1). Complication rates were comparable (p = 0.2),
while blood loss was lower (p = 0.015) and the procedure
duration (p < 0.001) and hospital stay were shorter
(p = 0.002) in patients with smaller stones. One abstract
reported on 301 procedures utilizing tracts sized �20 Fr (the
smallest tract size used was not stated) [29]. The SFR was high
at 99%, while blood loss, analgesic requirements, and
complication rates were low, and procedure duration and
hospital stay short. Two abstracts reporting on mPNL did not
explicitly state the size of the sheaths used [32,33], so this
information was obtained via e-mail correspondence with
the authors: Miller et al [32] used 16.5 Fr and Zimmermanns
et al [33] used 18 Fr. Using data from the CROES PNL Global
Study, Miller et al [32] reported a comparatively low ISFR
(46.5%) with a fair rate for immediate clinically insignificant
residual fragments (79.4%). Complication rates were com-
paratively high (eg, urosepsis in 12.9% of patients) and the
procedure duration was 174 min (Table 2). Zimmermanns
et al [33] presented results for two groups: the complete
cohort of 652 patients (all stone sizes) and a subgroup of
183 patients with stones measuring �500 mm2 in area. No p
values were reported, although the ISFR was comparable in
both groups (93.6% vs 91.8%).
3.6. RoB and confounding assessment
Figure 2 summarizes the key RoB and confounding
assessments. Only two studies were RCTs; the remaining
16 were either NRCSs or case series resulting in high RoB
associated with no randomization, incomplete outcome
data (attrition bias), and selective outcome data reporting.
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

Fig. 3 – Forest plot showing the stone-free rates reported in the randomized controlled trial (RCTs) and nonrandomized comparative studies (NRCSs).Reference numbers for studies are given in Table 1. PCNL = percutaneous nephrolithotomy; M-H = Mantel-Haenszel; CI = confidence interval.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X12
EURURO-7240; No. of Pages 16
Most studies reported stone sizes but did not report
stone location. Fewer than half of the studies contained
information on obesity (or body mass index). The risk of
confounding was moderate to high for previous open
surgery, access site, and access location, since only one or
two studies reported on these factors (Fig. 2). The tract size
used and the stone types and locations (when reported)
were heterogeneous.
3.7. Discussion
3.7.1. Principal findings
SFRs were comparable in patients with renal stones treated
with mPNL and standard PNL (Fig. 3). Smaller tracts tended
to be associated with significantly lower blood loss (Fig. 4)
or need for blood transfusion [11,19,21,24,26–28] at the
cost of a significantly longer procedure [11,19,24,28]
Fig. 4 – Forest plot showing the postoperative hemoglobin decrease in (A) g/dlnonrandomized comparative studies (NRCSs). Reference numbers for studies adeviation; CI = confidence interval; IV = inverse variance.
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
(Fig. 5). Hospital stay length was mostly shorter for mPNL
[11,22,24,34] (Fig. 6). The studies were heterogeneous with
respect to tract and stone sizes, and the RoB and
confounding risk were generally high.
The terms used to describe tract sizes, such as ‘‘mini-
PNL’’, ‘‘ultra-mini-PNL’’, and ‘‘micro-PNL’’, have not been
well defined and partly overlap. In general, tracts sized �18
Fr are used for miniaturized techniques [28,35]. Urologists
need to be aware that such terms describe not only the size
of the access sheath but also of specific instruments,
dilators, and operative concepts [36–40]. This systematic
review indicates that mPNL is a safe and effective evolution
of the PNL technique, and thus warrants further investiga-
tion. RCTs are necessary to better assess the benefits and
harms in relation to both disease-related parameters (stone
size, quantity and location) and interventional parameters
(tract size, puncture locations, and intrapelvic pressure).
and (B) percent reported in randomized controlled trials (RCTs) andre given in Table 1. PCNL = percutaneous nephrolithotomy; SD = standard
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

Fig. 6 – Forest plot showing the length of hospital stay (d) reported in randomized controlled trials (RCTs) and nonrandomized comparative studies(NRCS). Reference numbers for studies are given in Table 1. PCNL = percutaneous nephrolithotomy; SD = standard deviation; CI = confidence interval;IV = inverse variance.
Fig. 5 – Forest plot showing the duration of the procedure (min) reported in randomized controlled trials (RCTs) and nonrandomized comparativestudies (NRCS). Reference numbers for studies are given in Table 1. PCNL = percutaneous nephrolithotomy; SD = standard deviation; CI = confidenceinterval; IV = inverse variance.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 13
EURURO-7240; No. of Pages 16
3.7.2. Implications for practice
Our systematic review demonstrates that the use of
miniaturized PNL systems is effective. This was demon-
strated in most studies, including the first series published
by Jackman et al [6]. The authors reported SFR of 85% in
children and 85% in adults for stones sized 12–15 mm. One
of the few studies showing inferiority for smaller instru-
ments was the series described by Giusti et al [11]. However,
this study demonstrates the confusion caused by non-
standardized terminology, as the instruments used were
not dedicated for PNL but rigid ureteroscopes of small
diameters. The major disadvantage of small instruments is
that it is necessary to fragment stones into smaller pieces
that fit through the narrower sheaths, leading to longer
operating times compared to standard PNL, which allows
removal of large stone fragments with forceps and baskets.
Conversely, extraction of stone fragments seems to be
facilitated by modified Amplatz sheaths, as fragments can
be removed via vacuum suction, an effect that works best
for tracts sized 13–18 Fr [41–43].
The idea behind downsizing PNL is based on the
assumption of lower morbidity than for conventional
PNL. However, there is still controversy regarding whether
miniaturization leads to such a benefit. Li et al [44]
investigated systemic responses to both standard and
mPNL by measuring acute-phase proteins, and found no
significant differences between the groups. In another
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
experimental approach, Traxer et al [45] measured the
extent of damage to the renal parenchyma in pigs
undergoing placement of 11 Fr or 30 Fr nephrostomy tubes.
There were no detectable differences in fibrotic scar
volumes. The hypothesis of lower blood loss with minia-
turized tracts has only been confirmed in a few studies.
Mishra et al [24] reported a slight but clinically significant
advantage for 18 Fr compared to 26 Fr access. However,
others could not confirm such a benefit [22]. The observa-
tion in many series that the rate of tubeless procedures is
much higher than in conventional PNL series may support
the idea of lower intraoperative bleeding, if it is assumed
that a tubeless procedure is performed after uncomplicated
access and stone removal [22,24]. In addition, a meta-
analysis of tubeless versus standard PNL procedures [46]
indicated that tubeless procedures led to shorter hospital
stay, less postoperative pain, and possible quicker recovery,
and may therefore contribute to lower morbidity in
miniaturized PNL. However, most patients with so-called
tubeless procedures received a double-J stent instead of a
nephrostomy tube. As stent-related discomfort is common,
this has to be taken into account and evaluated in future
studies. Sealants are used in tubeless procedures, but their
potential benefit remains controversial [47,48]. Complica-
tion rates for mPNL according to the Clavien-Dindo
classification range from 11.9% to 37.7% [49,50]. Most
complications in published series were of low grade, with
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X14
EURURO-7240; No. of Pages 16
higher rates of blood transfusion and arterial embolization
in complex stone situations [51].
Identifying the right indications remains key in estab-
lishing the optimal use of miniaturized systems, but
published outcomes are heterogeneous in terms of SFR
and complication rates reported. Miniaturized PNL seems to
be more effective for smaller rather than larger renal stones
>20 mm [18,52]. The question arises whether miniaturized
PNL may compete more with SWL and ureteroscopy (URS)
than with conventional PNL. While most published series so
far reported an advantage for percutaneous techniques over
URS [53,54], De et al recently published a meta-analysis
comparing percutaneous stone removal with URS [51]. Al-
though the overall SFR was in favor of PNL, subgroup
analysis indicated that URS provided a significantly higher
SFR rate than miniaturized systems. However, the same
limitations as for the present analysis apply to their
systematic review, with one of the major weaknesses being
the inclusion of different tract sizes. De et al concluded that
URS should be recommended over minimally invasive PNL
for stones sized <20 mm because of the generally lower
morbidity of retrograde access. When compared to SWL,
miniaturized PNL demonstrates higher SFR and a lower rate
of auxiliary measures, although most data come from
pediatric series that were not included in this systematic
review [55–58]. On the basis of the current literature and
experiences, downsized instruments may be used for stones
in all locations accessible for standard PNL. The best
indications seem to be medium stones of up to 20 mm,
although there are no data to support an upper limit. In
general, instruments should be adapted to the anatomy.
Patients with tiny collecting systems may especially benefit
from the use of smaller systems. Another potential
indication might be stones located within calyceal divertic-
ula. Future research should evaluate such issues.
Hemodynamic, electrolyte, and metabolic changes have
been prospectively evaluated when comparing miniaturized
with standard PNL [26]. Interestingly, a trend towards
metabolic acidosis was observed in the mPNL group, possibly
associated with prolonged operating time and higher
intrarenal irrigation pressure. Tepeler et al [28] measured
intrarenal pelvic pressure during PNL procedures using 4.8 Fr
nephroscopes in comparison to conventional PNL. Intrarenal
pressure was significantly lower in the conventional group
during all steps of the procedure. Even though there was no
difference in outcome in their series, surgeons should be
aware of higher pressure for downsized systems [36]. Place-
ment of a ureteral catheter may be helpful for irrigation
outflow to allow intermittent flushing [59].
It is sobering that even the simplest parameter, SFR, is
generally difficult to compare because of different defini-
tions of SFR with regard to the time until stone-free status is
achieved and whether or not residual fragments are
accepted, as well as the maximum fragment size allowable
to justify classification as ‘‘clinically insignificant’’. Further-
more, the imaging modality used to assess stone-free status
varies, with most series using ultrasound or kidney/ureter/
bladder X-ray (KUB), although CT is more sensitive for small
residual fragments [60,61].
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
3.7.3. Implications for research
The concept of reducing the morbidity of PNL by downsizing
the access tract seems convincing. The findings that success
rates are high with miniaturized instruments demonstrate
that the concept does not negatively impact the outcome.
However, well-designed studies are missing and no conclu-
sion can be drawn in terms of potentially lower morbidity.
3.7.4. Limitations
This review has several limitations. Many of the studies
included may be affected by selection bias, outcome-
reporting bias, and the use of different tract sizes. More
than half of the studies were single-arm case series. For five of
the studies, only abstracts were published, severely limiting
the information available and its quality. Furthermore, the
studies were heterogeneous in design, with differences in the
size of tracts used in both the interventional and control arms
(when available) and in the size and location of stones
treated.
Many of the studies included also suffered from other
important methodological limitations. Importantly, most of
the studies on mPNL used single-step dilatation, whereas
conventional PNL procedures were performed with step or
balloon dilatation, entailing different complication rates for
bleeding, for example [62]. Moreover, most mPNL proce-
dures were performed with low intrapelvic pressure, while
standard PNL operations were much more frequently
performed at high pressure, with implications for postop-
erative fever and sepsis, for example [63,64]. In addition,
assessment of the postoperative SFR was obfuscated by the
use of both less sensitive standard radiology (KUB) and
significantly more sensitive CT [65]. Finally, many studies
did not report statistical calculations of differences between
interventional groups for the main outcome measures.
4. Conclusions
The available evidence indicates that mPNL is at least as
efficacious and safe as standard PNL for the removal of renal
calculi, with a limited risk of significant (Clavien grade �2)
complications. However, the quality of the evidence was
poor and drawn mainly from small studies, the majority of
which were single-arm case series and NRCSs, and only two
of which were RCTs. Hence, the risks of bias and
confounding were high. Furthermore, the tract sizes used
and the types of stones treated were heterogeneous. Thus,
more reliable data from well-designed and adequately
sampled and powered RCTs are warranted.
Author contributions: Thomas Knoll had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Knoll, Turk, Ruhayel, Tepeler.
Acquisition of data: Knoll, Ruhayel, Tepeler, Yuan.
Analysis and interpretation of data: Knoll, Turk, Ruhayel, Tepeler.
Drafting of the manuscript: Knoll, Ruhayel, Tepeler, MacLennan, Yuan.
Critical revision of the manuscript for important intellectual content: Knoll,
Turk, Ruhayel, Tepeler, Dabestani, MacLennan, Petrık, Skolarikos, Seitz,
Straub, Yuan.
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X 15
EURURO-7240; No. of Pages 16
Statistical analysis: None.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Knoll, Turk, Ruhayel, Dabestani.
Other: None.
Financial disclosures: Thomas Knoll certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: Ales Petrık has received speaker
honoraria from GSK and fellowship and travel grants from Astellas and
Olympus. Christian Seitz has received consultant fees from Astellas and
speaker honoraria from Rowa Wagner. Michael Straub has received
consultant fees from Richard Wolf Endoskope and Sanochemia
Pharmazeutika. Thomas Knoll has received consultant fees from
Schoelly, Boston Scientific, Olympus, and Storz Medical, and speaker
honoraria from Karl Storz, Richard Wolf, Olympus, Boston Scientific, and
Ibsen; and has participated in trials by Cook and Coloplast. The
remaining authors have nothing to disclose.
Funding/Support and role of the sponsor: None.
Acknowledgments: We are grateful for the valuable help of Karin Plass,
European Association of Urology Guidelines Office, Arnhem, The
Netherlands, for providing administrative support. We also thank
Richard Sylvester and Thomas Lam, of the EAU Guidelines Office, for
providing methodological supervision and support.
References
[1] Hesse A, Brandle E, Wilbert D, Kohrmann KU, Alken P. Study on the
prevalence and incidence of urolithiasis in Germany comparing the
years 1979 vs. 2000. Eur Urol 2003;44:709–13.
[2] Lotan Y, Buendia Jimenez I, Lenoir-Wijnkoop I, et al. Primary
prevention of nephrolithiasis is cost-effective for a national health-
care system. BJU Int 2012;110:E1060–7.
[3] Scales Jr CD, Smith AC, Hanley JM, et al. Prevalence of kidney stones
in the United States. Eur Urol 2012;62:160–5.
[4] Turk C, Knoll T, Petrık A, et al. EAU guidelines on urolithiasis 2014.
Arnhem, The Netherlands: European Association of Urology; 2014.
[5] Preminger GM, Assimos DG, Lingeman JE, et al. Chapter 1: AUA
guideline on management of staghorn calculi: diagnosis and treat-
ment recommendations. J Urol 2005;173:1991–2000.
[6] Jackman SV, Docimo SG, Cadeddu JA, Bishoff JT, Kavoussi LR, Jarrett
TW. The ‘‘mini-perc’’ technique: a less invasive alternative to
percutaneous nephrolithotomy. World J Urol 1998;16:371–4.
[7] Helal M, Black T, Lockhart J, Figueroa TE. The Hickman peel-away
sheath: alternative for pediatric percutaneous nephrolithotomy. J
Endourol 1997;11:171–2.
[8] Desai J, Solanki R. Ultra-mini percutaneous nephrolithotomy
(UMP): one more armamentarium. BJU Int 2013;112:1046–9.
[9] Desai MR, Sharma R, Mishra S, Sabnis RB, Stief C, Bader M. Single-
step percutaneous nephrolithotomy (microperc): the initial clinical
report. J Urol 2011;186:140–5.
[10] Kukreja R, Desai M, Patel S, Bapat S, Desai M. Factors affecting blood
loss during percutaneous nephrolithotomy: prospective study. J
Endourol 2004;18:715–22.
[11] Giusti G, Piccinelli A, Taverna G, et al. Miniperc? No, thank you! Eur
Urol 2007;51:810–4.
[12] Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for
systematic reviews and meta-analyses: the PRISMA statement. Ann
Intern Med 2009;151:264–9.
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
[13] Higgins JP, Green S. Cochrane handbook for systematic reviews of
interventions. The Cochrane Collaboration; 2011.
[14] Deeks JJ, Dinnes J, D’Amico R, et al. Evaluating non-randomised
intervention studies. Health Technol Assess 2003;7:1–173.
[15] Reeves BC, Deeks JJ, Higgins JP, Wells GA. Including non-random-
ised studies. In: Higgins JP, Green S, editors. Cochrane handbook for
systematic reviews of interventions. The Cochrane Collaboration;
2011. Chapter 13.
[16] Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L. Do
the findings of case series studies vary significantly according to
methodological characteristics? Health Technol Assess 2005;9:
1–146.
[17] Viswanathan M, Ansari MT, Berkman ND, et al. Assessing the risk of
bias of individual studies in systematic reviews of health care
interventions. Rockville, MD: Agency for Healtcare Research and
Quality; 2008.
[18] Abdelhafez MF, Amend B, Bedke J, et al. Minimally invasive percu-
taneous nephrolithotomy: a comparative study of the management
of small and large renal stones. Urology 2013;81:241–5.
[19] Cheng F, Yu W, Zhang X, Yang S, Xia Y, Ruan Y. Minimally invasive
tract in percutaneous nephrolithotomy for renal stones. J Endourol
2010;24:1579–82.
[20] Desai J, Zeng G, Zhao Z, Zhong W, Chen W, Wu W. A novel technique
of ultra-mini-percutaneous nephrolithotomy: introduction and an
initial experience for treatment of upper urinary calculi less than
2 cm. Biomed Res Int 2013;2013:490793.
[21] Karakose A, Aydogdu O, Atesci YZ. The use of the Amplatz sheath in
percutaneous nephrolithotomy: does Amplatz sheath size matter?
Curr Urol 2013;7:127–31.
[22] Knoll T, Wezel F, Michel MS, Honeck P, Wendt-Nordahl G. Do
patients benefit from miniaturized tubeless percutaneous nephro-
lithotomy?. A comparative prospective study. J Endourol
2010;24:1075–9.
[23] Lu Y, Ping JG, Zhao XJ, Hu LK, Pu JX. Randomized prospective trial of
tubeless versus conventional minimally invasive percutaneous
nephrolithotomy. World J Urol 2013;31:1303–7.
[24] Mishra S, Sharma R, Garg C, Kurien A, Sabnis R, Desai M. Prospective
comparative study of miniperc and standard PNL for treatment of
1 to 2 cm size renal stone. BJU Int 2011;108:896–9.
[25] Sung YM, Chod SW, Jeon SS, Shin SW, Park KB, Do YS. The ‘‘mini-
perc’’ technique of percutaneous nephrolithotomy with a 14-Fr
peel-away sheath: 3-year results in 72 patients. Korean J Radiol
2006;7:103–6.
[26] Xu S, Shi H, Zhu J, et al. A prospective comparative study of
haemodynamic, electrolyte, and metabolic changes during percu-
taneous nephrolithotomy and minimally invasive percutaneous
nephrolithotomy. World J Urol 2014;32:1275–80.
[27] Yamaguchi A, Skolarikos A, Buchholz NPN, et al. Operating times
and bleeding complications in percutaneous nephrolithotomy: a
comparison of tract dilation methods in 5537 patients in the
Clinical Research Office of the Endourological Society percutaneous
nephrolithotomy global study. J Endourol 2011;25:947–54.
[28] Tepeler A, Akman T, Silay MS, et al. Comparison of intrarenal pelvic
pressure during micro-percutaneous nephrolithotomy and conven-
tional percutaneous nephrolithotomy. Urolithiasis 2014;42:275–9.
[29] Bhattu A, Mohan V, Jagtap J, et al. Miniperc: 301 cases single centre
experience and outcome analysis. Indian J Urol 2014;30:S64.
[30] Desai J, Solanki R. Ultra-mini PCNL (UMP). Eur Urol Suppl 2013;12:
eV40.
[31] Karatag T, Buldu I, Inan R, Istanbulluoglu MO. The treatment of
moderate size renal calculi with micro-percutaneous nephrolithot-
omy technique: our clinical experiences. Eur Urol Suppl 2014;13:
e614.
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 7 ) X X X – X X X16
EURURO-7240; No. of Pages 16
[32] Miller S, Taylor A, Ahmad R, et al. Mini-percutaneous nephrolithot-
omy in the treatment of adult renal nephrolithiasis: a single
institution experience. BJU Int 2014;113:S352–3.
[33] Zimmermanns V, Kurzidim S, Liske P, Lahme S. Minimal invasive
PCNL (MPCNL)—proven efficiency and safety after more than
650 consecutive patients. Eur Urol Suppl 2012;11:e1035.
[34] Tepeler A, Sarica K. Standard, mini, ultra-mini, and micro percuta-
neous nephrolithotomy: what is next?. A novel labeling system for
percutaneous nephrolithotomy according to the size of the access
sheath used during procedure. Urolithiasis 2013;41:367–8.
[35] Schilling D, Husch T, Bader M, et al. Nomenclature in PCNL or the
Tower Of Babel: a proposal for a uniform terminology. World J Urol
2015;33:1905–7.
[36] Nagele U, Horstmann M, Sievert KD, et al. A newly designed
Amplatz sheath decreases intrapelvic irrigation pressure during
mini-percutaneous nephrolitholapaxy: an in-vitro pressure-
measurement and microscopic study. J Endourol 2007;21:
1113–6.
[37] Nagele U, Schilling D, Anastasiadis AG, et al. Closing the tract of
mini-percutaneous nephrolithotomy with gelatine matrix hemo-
static sealant can replace nephrostomy tube placement. Urology
2006;68:489–93.
[38] Lahme S, Bichler KH, Strohmaier WL, Gotz T. Minimally invasive
PCNL in patients with renal pelvic and calyceal stones. Eur Urol
2001;40:619.
[39] Desai J, Zeng G, Zhao Z, Zhong W, Chen W, Wu W. A novel technique
of ultra-mini-percutaneous nephrolithotomy: introduction and an
initial experience for treatment of upper urinary calculi less than
2 cm. BioMed Res Int 2013;2013:490793.
[40] Bader MJ, Gratzke C, Seitz M, Sharma R, Stief CG, Desai M. The ‘‘all-
seeing needle’’: initial results of an optical puncture system con-
firming access in percutaneous nephrolithotomy. Eur Urol
2011;59:1054–9.
[41] Nicklas AP, Schilling D, Bader MJ, et al. The vacuum cleaner effect in
minimally invasive percutaneous nephrolitholapaxy. World J Urol
2015;33:1847–53.
[42] Mager R, Balzereit C, Gust K, et al. The hydrodynamic basis of the
vacuum cleaner effect in continuous-flow PCNL instruments: an
empiric approach and mathematical model. World J Urol
2016;34:717–24.
[43] Nagele U, Nicklas A. Vacuum cleaner effect, purging effect, active
and passive wash out: a new terminology in hydrodynamic stone
retrieval is arising—does it affect our endourologic routine? World J
Urol 2016;34:143–4.
[44] Li LY, Gao X, Yang M, et al. Does a smaller tract in percutaneous
nephrolithotomy contribute to less invasiveness?. A prospective
comparative study. Urology 2010;75:56–61.
[45] Traxer O, Smith 3rd TG, Pearle MS, Corwin TS, Saboorian H, Cadeddu
JA. Renal parenchymal injury after standard and mini percutaneous
nephrostolithotomy. J Urol 2001;165:1693–5.
[46] Zhong Q, Zheng C, Mo J, Piao Y, Zhou Y, Jiang Q. Total tubeless versus
standard percutaneous nephrolithotomy: a meta-analysis. J
Endourol 2013;27:420–6.
[47] Borin JF, Sala LG, Eichel L, McDougall EM, Clayman RV. Tubeless
percutaneous nephrolithotomy using hemostatic gelatin matrix. J
Endourol 2005;19:614–7.
[48] Uribe CA, Eichel L, Khonsari S, et al. What happens to hemostatic
agents in contact with urine? An in vitro study. J Endourol
2005;19:312–7.
Please cite this article in press as: Ruhayel Y, et al. Tract Sizes inReview from the European Association of Urology Urolithiasis Gj.eururo.2017.01.046
[49] Abdelhafez MF, Bedke J, Amend B, et al. Minimally invasive percu-
taneous nephrolitholapaxy (PCNL) as an effective and safe proce-
dure for large renal stones. BJU Int 2012;110:E1022–6.
[50] Nagele U, Schilling D, Sievert KD, Stenzl A, Kuczyk M. Management of
lower-pole stones of 0.8 to 1.5 cm maximal diameter by the mini-
mally invasive percutaneous approach. J Endourol 2008;22:1851–3.
[51] De S, Autorino R, Kim FJ, et al. Percutaneous nephrolithotomy
versus retrograde intrarenal surgery: a systematic review and
meta-analysis. Eur Urol 2015;67:125–37.
[52] Fawzi AM, Sakr AMN, Youssef MK, et al. Minimally invasive percu-
taneous nephrolithotomy versus standard PCNL for management of
renal stones in the flank-free modified supine position: single
center experience. Eur Urol Suppl 2015;14:e584.
[53] Knoll T, Jessen JP, Honeck P, Wendt-Nordahl G. Flexible ureteror-
enoscopy versus miniaturized PNL for solitary renal calculi of 10-
30 mm size. World J Urol 2011;29:755–9.
[54] Zhong W, Zhao Z, Wang L, Swami S, Zeng G. Percutaneous-based
management of staghorn calculi in solitary kidney: combined mini
percutaneous nephrolithotomy versus retrograde intrarenal sur-
gery. Urol Int 2015;94:70–3.
[55] Ozturk U, Sener NC, Goktug HNG, Nalbant I, Gucuk A, Imamoglu
MA. Comparison of percutaneous nephrolithotomy, shock wave
lithotripsy, and retrograde intrarenal surgery for lower pole renal
calculi 10-20 mm. Urol Int 2013;91:345–9.
[56] Zeng G, Jia J, Zhao Z, Wu W, Zhao Z, Zhong W. Treatment of renal
stones in infants: comparing extracorporeal shock wave lithotripsy
and mini-percutaneous nephrolithotomy. Urol Res 2012;40:
599–603.
[57] Yan X, Al-Hayek S, Gan W, Zhu W, Li X, Guo H. Minimally invasive
percutaneous nephrolithotomy in preschool age children with
kidney calculi (including stones induced by melamine-contaminat-
ed milk powder). Pediatr Surg Int 2012;28:1021–4.
[58] Kumar A, Kumar N, Vasudeva P, Kumar R, Jha SK, Singh H. A single
center experience comparing miniperc and shockwave lithotripsy for
treatment of radiopaque 1-2 cm lower caliceal renal calculi in chil-
dren: a prospective randomized study. J Endourol 2015;29:805–9.
[59] Nagele U, Walcher U, Bader M, Herrmann T, Kruck S, Schilling D.
Flow matters 2: how to improve irrigation flow in small-calibre
percutaneous procedures—the purging effect. World J Urol
2015;33:1607–11.
[60] Deters LA, Jumper CM, Steinberg PL, Pais Jr VM. Evaluating the
definition of ‘‘stone free status’’ in contemporary urologic litera-
ture. Clin Nephrol 2011;76:354–7.
[61] Ghani K, Alruwaily A, Rogers M, et al. The natural history of
asymptomatic renal stones: a systematic review and meta-analy-
sis. J Urol 2015;1:e1108–9.
[62] Dehong C, Liangren L, Huawei L, Qiang W. A comparison among four
tract dilation methods of percutaneous nephrolithotomy: a sys-
tematic review and meta-analysis. Urolithiasis 2013;41:523–30.
[63] Guo HQ, Shi HL, Li XG, et al. [Relationship between the intrapelvic
perfusion pressure in minimally invasive percutaneous nephro-
lithotomy and postoperative recovery]. Zhonghua Wai Ke Za Zhi
2008;46:52–4.
[64] Zhong W, Zeng G, Wu K, Li X, Chen W, Yang H. Does a smaller tract
in percutaneous nephrolithotomy contribute to high renal pelvic
pressure and postoperative fever? J Endourol 2008;22:2147–51.
[65] Park J, Hong B, Park T, Park HK. Effectiveness of noncontrast
computed tomography in evaluation of residual stones after per-
cutaneous nephrolithotomy. J Endourol 2007;21:684–7.
Miniaturized Percutaneous Nephrolithotomy: A Systematicuidelines Panel. Eur Urol (2017), http://dx.doi.org/10.1016/