
Dyslipidemia Drug Update and Guidelines Review ACPE … drug... · circulating atherogenic...
13
22 Palmetto Pharmacist • Volume 56 Number 3 Objective: After completing this activity, participants should be able to: 1) Define dyslipidemia and atherosclerotic cardiovascular disease. 2) Identify the four statin benefit groups according to the 2013 ACC/AHA guideline. 3) Compare and contrast the National Lipid Association Guideline and the ACC/AHA guideline. 40 Categorize statins and doses according to intensity of therapy 50 Determine statin treatment intensity based on patient risks. 6) Provide counseling pearls for individual statins. 7) Examine the proprotein convertase subtilisin kexin type 9 inhibitors as an alternative or add-on to statin therapy. Conflict of interest statement: The authors have no conflict of interest for their work on this article or topic. Abstract: Dyslipidemia is a major risk factor for the development of atherosclerotic cardiovascular disease (ASCVD). In the past, guidelines specifically targeted low-density lipoprotein cholesterol (LDL-C) concentrations as the main bio-marker for assessing risk and determining management strategy. Released in 2001, the National Cholesterol Education Program (NCEP) Adult Treatment Panel III highlighted additional risk factors other than LDL-C yet still set LDL-C “therapeutic” goal concentrations. The 2013 American College of Cardiology and the American Heart Association (ACC/AHA) Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults identify four patient groups with the most extensive evidence of benefit for ASCVD prevention. Lifestyle and drug therapy remain recommended for these patient groups. The ACC/AHA guideline highlights statins, at specific doses or intensity, as the preferred treatment goal. In contrast, the National Lipid Association (NLA) specifies that treatment intensity should still be decided based on Dyslipidemia Drug Update and Guidelines Review ACPE UAN: 0171-9999-16-018-H01-P James Sterrett, PharmD, BCPS, CDE, Assistant Professor, SC College of Pharmacy Michael Corvino, PharmD, Pharmacy Manager, Walgreens Pharmacy Austin Avrett, PharmD, Pharmacist Consultant, Americare Pharmacy Jason Haney, PharmD, BCPS, Assistant Professor, SC College of Pharmacy circulating atherogenic cholesterol and, of these, non- high density lipoprotein cholesterol (non-HDL-C) is the best surrogate marker to assess pathogenic lipid levels. This continuing education activity overviews diagnostic criteria for dyslipidemia, summarizes current clinical practice guidelines, and discusses available treatment options for dyslipidemia management. Keywords: American College of Cardiology, American Heart Association, Atherosclerosis Biomarker, Atherosclerotic Cardiovascular Disease, Dyslipidemia, Statins, Lipid Management, National Cholesterol Education Program, National Lipid Association. INTRODUCTION Introduction: Dyslipidemia is a prevalent condition affecting over 100 million Americans. Patients with dyslipidemia have an increased risk for developing coronary heart disease (CHD) and stroke. CHD is the most common cause of death in the United States in both women and men. According to Heart Disease and Stroke Statistics 2015 Update, approximately 1 out of every 7 deaths is related to underlying CHD. 1- 2 Pharmacists are well positioned to impact these statistics. Because they are often the most easily accessible health care professionals, pharmacists can identify and refer patients at risk for dyslipidemia and cardiovascular disease. Because of their medication expertise, they can offer evidence-based recommendations to primary care providers to improve cardiovascular outcomes. 3 In fact, pharmacists’ interventions have been shown to significantly improve quality when involved in the interprofessional care of dyslipidemia. 4 This continuing education activity overviews diagnostic criteria for dyslipidemia, summarizes current clinical practice guidelines, and discusses available treatment options for dyslipidemia management. Although there are several dyslipidemia guidelines internationally, this paper will focus on the 2013 American College of Cardiology/American Heart Association Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular JOURNAL CE
Transcript of Dyslipidemia Drug Update and Guidelines Review ACPE … drug... · circulating atherogenic...

22 Palmetto Pharmacist • Volume 56 Number 3
Objective: After completing this activity, participants should be able to:1) Define dyslipidemia and atherosclerotic cardiovascular disease.2) Identify the four statin benefit groups according to the 2013 ACC/AHA guideline.3) Compare and contrast the National Lipid Association Guideline and the ACC/AHA guideline.40 Categorize statins and doses according to intensity of therapy50 Determine statin treatment intensity based on patient risks.6) Provide counseling pearls for individual statins.7) Examine the proprotein convertase subtilisin kexin type 9 inhibitors as an alternative or add-on to statin therapy.
Conflict of interest statement: The authors have no conflict of interest for their work on this article or topic.
Abstract: Dyslipidemia is a major risk factor for the development of atherosclerotic cardiovascular disease (ASCVD). In the past, guidelines specifically targeted low-density lipoprotein cholesterol (LDL-C) concentrations as the main bio-marker for assessing risk and determining management strategy. Released in 2001, the National Cholesterol Education Program (NCEP) Adult Treatment Panel III highlighted additional risk factors other than LDL-C yet still set LDL-C “therapeutic” goal concentrations. The 2013 American College of Cardiology and the American Heart Association (ACC/AHA) Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults identify four patient groups with the most extensive evidence of benefit for ASCVD prevention. Lifestyle and drug therapy remain recommended for these patient groups. The ACC/AHA guideline highlights statins, at specific doses or intensity, as the preferred treatment goal. In contrast, the National Lipid Association (NLA) specifies that treatment intensity should still be decided based on
Dyslipidemia Drug Update and Guidelines ReviewACPE UAN: 0171-9999-16-018-H01-P James Sterrett, PharmD, BCPS, CDE, Assistant Professor, SC College of PharmacyMichael Corvino, PharmD, Pharmacy Manager, Walgreens PharmacyAustin Avrett, PharmD, Pharmacist Consultant, Americare PharmacyJason Haney, PharmD, BCPS, Assistant Professor, SC College of Pharmacy
circulating atherogenic cholesterol and, of these, non-high density lipoprotein cholesterol (non-HDL-C) is the best surrogate marker to assess pathogenic lipid levels. This continuing education activity overviews diagnostic criteria for dyslipidemia, summarizes current clinical practice guidelines, and discusses available treatment options for dyslipidemia management.
Keywords: American College of Cardiology, American Heart Association, Atherosclerosis Biomarker, Atherosclerotic Cardiovascular Disease, Dyslipidemia, Statins, Lipid Management, National Cholesterol Education Program, National Lipid Association.
INTRODUCTIONIntroduction: Dyslipidemia is a prevalent condition affecting over 100 million Americans. Patients with dyslipidemia have an increased risk for developing coronary heart disease (CHD) and stroke. CHD is the most common cause of death in the United States in both women and men. According to Heart Disease and Stroke Statistics 2015 Update, approximately 1 out of every 7 deaths is related to underlying CHD.1-
2 Pharmacists are well positioned to impact these statistics. Because they are often the most easily accessible health care professionals, pharmacists can identify and refer patients at risk for dyslipidemia and cardiovascular disease. Because of their medication expertise, they can offer evidence-based recommendations to primary care providers to improve cardiovascular outcomes.3 In fact, pharmacists’ interventions have been shown to significantly improve quality when involved in the interprofessional care of dyslipidemia.4 This continuing education activity overviews diagnostic criteria for dyslipidemia, summarizes current clinical practice guidelines, and discusses available treatment options for dyslipidemia management. Although there are several dyslipidemia guidelines internationally, this paper will focus on the 2013 American College of Cardiology/American Heart Association Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
JOURNAL CE

Palmetto Pharmacist • Volume 56, Number 3 23
JOURNAL CERisk in Adults (ACC/AHA Guideline) and the National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia (NLA guideline).
Pathophysiology and Pathogenesis: Lipoproteins are complex molecules responsible for transporting lipid molecules around the body. Triglycerides, phospholipids and cholesterol are plasma fats fundamental to cell membrane function and hormone synthesis; however, abnormal levels of these fats can lead to CHD and stroke, especially in the elderly.5 Dyslipidemia results from high serum concentrations of total cholesterol, LDL-C, or triglycerides or from low serum concentrations of HDL-C.
Atherosclerosis is a multifactorial disease impacted by genetic as well as environmental factors. Clinical atherosclerosis occurs over the course of five key events: damage to the endothelium, cholesterol invasion, inflammatory response, plaque formation, and plaque rupture. The delicate endothelial lining of the blood vessel may be damaged by high blood pressure, diabetes, smoking, and dyslipidemia. Plasma LDL-C crosses the damaged endothelium to the extracellular matrix of the artery wall. Once in the artery, LDL-C is oxidized, a process that recruits macrophages. The resulting inflammatory response leads to unstable arterial plaque formation on the inner portion of the artery. Unstable atherosclerotic plaques may rupture, triggering clot formation and negative clinical outcomes, such as heart attack and stroke. Plaques that cause less than 50% stenosis of the luminal diameter are prone to rupture, while those that exceed 70% stenosis typically cause predictable symptoms of ischemia, such as angina pectoris.6
Elevated triglycerides also pose an increased risk for CHD, potentially through the fact that an increased concentration of circulating triglycerides corresponds to a more atherogenic LDL-C particle size.7 A 2007 Veterans Administration study of 14,000 patients, aged 26 to 45 years, with a mean follow up of 10.5 years, found that high triglyceride concentrations on first measurement were strongly and independently associated with CHD risk in the highest versus the lowest triglyceride quintile group (hazard ratio 4.9 [95% CI, 1.01 to 24.55]).8
HDL-C particles, on the other hand, are thought to protect against heart disease. In particular, HDL-C’s role is to transport cholesterol and triglycerides away from the artery wall, and return the cholesterol to the liver for excretion or re-utilization. This process decreases macrophage accumulation, plaque formation and, ultimately, cardiovascular events. Higher HDL-C levels, in fact, have been associated with better cardiovascular outcomes.9
There are two common subsets of dyslipidemia: familial and acquired. Familial hypercholesterolemia is an inherited disorder that causes severe elevations in total cholesterol and LDL-C. Patients diagnosed with familial hypercholesterolemia have a high rate of cardiovascular disease.10 Acquired hypercholesterolemia can result from a poor diet or from a metabolic disturbance caused by a medical condition or pharmacologic therapy.
Global Assessment: The 2001 National Cholesterol Education Program (NCEP) Adult Treatment Panel III utilized the Framingham-Risk calculator to estimate the possibility of a CVD event within 10 years. Although it paved the way for successful patient care, this points-based calculator did not include race or diabetes status. Furthermore, it did not put enough emphasis on age, which is now considered the biggest predictor of a CVD event. The new updated global assessment, referred to in the ACC/AHA guideline as the “Pooled Cohort Equation,” predicts a patient’s 10-year and lifetime risk of having an atherosclerotic cardiovascular disease (ASCVD) event (coronary death, nonfatal myocardial infarction, or stroke).11 The pooled cohort equation, also known as the ASCVD risk estimator, provides the basis for a discussion between the patient and provider regarding the impact of early intervention to lower risks. This pooled cohort equation includes the following variables:
• Age• Gender• Race• Total cholesterol• HDL-C• Systolic blood pressure• Blood pressure lowering medication use• Diabetes status• Smoking status
24 Palmetto Pharmacist • Volume 56 Number 3
This estimator is based on data from non-Hispanic whites and African Americans in the United States, which limits its applicability to some populations. Other factors omitted from this estimator are a family history of premature cardiovascular disease, LDL-C ≥160 mg/dL, and genetic dyslipidemias. Additionally, diabetes is only distinguished as being present without regard the type, or duration of diabetes, or degree of control.
The online link to pooled cohort equation is http://my.americanheart.org/cvriskcalculator. At this site, one can also find applications for a smartphone to quickly assess risk percentage and a step-by-step approach to treatment based on AHA/ACC guidelines.
Current Guidelines and Recommendations: According to the ACC/AHA guideline, the recommended approach to management of dyslipidemia is to analyze patients based on ASCVD presence and risk. The ACC/AHA guidelines promote 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (“statins”) as the drugs of choice because of positive evidence based research. Instead of having LDL-C or non-HDL-C as performance measures, the ACC/AHA guidelines focus on intensity of statin therapy as the measure of treatment. While LDL-C and Non-HDL-C are surrogate markers that often point clinicians in the right direction, it is important that treatment decisions are based on data involving hard outcomes, also known as patient oriented evidence that matters (POEMs), when available.12 In fact, they specifically state, “No evidence was found that titration or combination drug therapy to achieve specific LDL-C or non-HDL-C levels or percent reduction improved ASCVD outcomes.” Instead, they specifically highlight four patient groups with the best evidence of benefiting from statin therapy by reducing ASCVD events (primary and secondary). The guidelines provide guidance regarding best statin intensity for each of the four groups of patients (along with National Heart, Lung, and Blood Institute (NHLBI) grade for level of evidence).11 Appreciating the level of evidence allows the provider to emphasize areas with high level of evidence versus items that only are based on expert opinion. It provides a great opportunity for putting evidence into perspective, discussing shared decision making between the provider and the patient and placing focus on patient quality of life. The four statin benefit groups and NHLBI recommendation grading methodology (see table 1) are as follows:
1. Patients with clinical ASCVD a. Age ≤75 years old and no safety issues: high intensity statin (IA) b. Age >75 years old or has safety concerns: moderate intensity statin (IA)
2. Patients with LDL-C ≥190 mg/dL (who meet criteria for heterozygous hypercholesterolemia) a. Age ≥21 years old: high intensity statin (IB)
b. Goal is to achieve a 50% reduction in LDL-C. (IIaB) Non-statin therapy may be added to reduce LDL-C if 50% is not achieved with statin monotherapy. (IIbC)
3. Patients with diabetes, between the ages of 40-75 years old, and LDL-C between 70-189 mg/dLa. If patient has an estimated 10-year ASCVD risk < 7.5%, consider moderate intensity statin (IA)b. If patient has an estimated 10-year ASCVD risk ≥ 7.5%, consider high intensity statin (IIaB)
4. Patients without diabetes or clinical ASCVD, between the ages of 40-75 years, with LDL-C between 70-189 mg/dL a. Consider high intensity statin if estimated 10-year ASCVD risk ≥7.5% (IA)
b. Consider a moderate intensity statin if patient cannot tolerate high intensity or if estimated 10-year ASCVD risk is 5 to <7.5% (IIaB)
JOURNAL CE
Palmetto Pharmacist • Volume 56, Number 3 25
Table 1: NHLBI Recommendation Grading MethodologySize of Treatment EffectClass I • Benefit >>> Risk
• Procedure/treatment SHOULD be performed/administeredClass IIa • Benefit >> Risk
• Additional studies with focused objectives needed• IT IS REASONABLE to perform procedure/administer treatment
Class IIb • Benefit ≥ Risk• Additional studies with broad objectives needed; additional registry
data would be helpful• Procedure/treatment MAY BE CONSIDERED
Class III No Benefit orClass III Harm
• Procedure/test not helpful or treatment has no proven benefit• Procedure/test has excess cost without benefit or is harmful to pa-
tientsEstimate of Certainty of Treatment EffectLevel A • Multiple populations evaluated
• Data derived from multiple randomized clinical trials or meta-analy-ses
Level B • Limited populations evaluated• Data derived from a single randomized trial or nonrandomized stud-
iesLevel C • Very limited populations evaluated
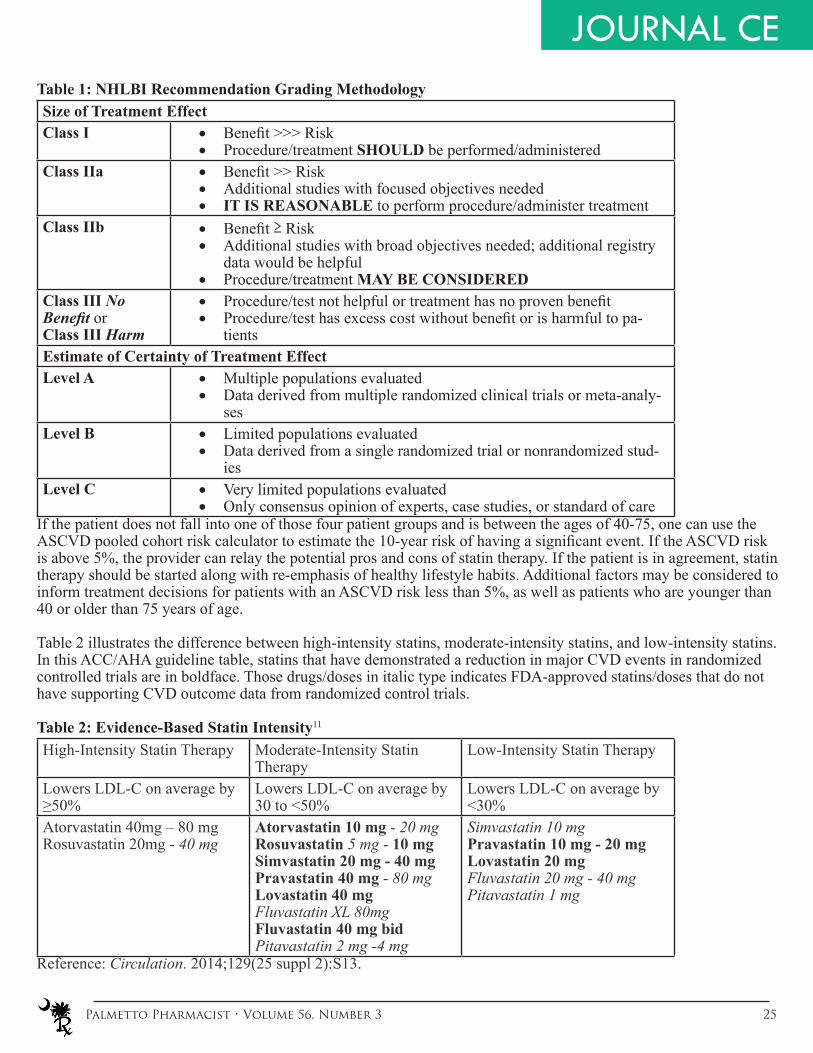
• Only consensus opinion of experts, case studies, or standard of careIf the patient does not fall into one of those four patient groups and is between the ages of 40-75, one can use the ASCVD pooled cohort risk calculator to estimate the 10-year risk of having a significant event. If the ASCVD risk is above 5%, the provider can relay the potential pros and cons of statin therapy. If the patient is in agreement, statin therapy should be started along with re-emphasis of healthy lifestyle habits. Additional factors may be considered to inform treatment decisions for patients with an ASCVD risk less than 5%, as well as patients who are younger than 40 or older than 75 years of age.
Table 2 illustrates the difference between high-intensity statins, moderate-intensity statins, and low-intensity statins. In this ACC/AHA guideline table, statins that have demonstrated a reduction in major CVD events in randomized controlled trials are in boldface. Those drugs/doses in italic type indicates FDA-approved statins/doses that do not have supporting CVD outcome data from randomized control trials.
Table 2: Evidence-Based Statin Intensity11
High-Intensity Statin Therapy Moderate-Intensity Statin Therapy
Low-Intensity Statin Therapy
Lowers LDL-C on average by ≥50%
Lowers LDL-C on average by 30 to <50%
Lowers LDL-C on average by <30%
Atorvastatin 40mg – 80 mgRosuvastatin 20mg - 40 mg
Atorvastatin 10 mg - 20 mgRosuvastatin 5 mg - 10 mgSimvastatin 20 mg - 40 mgPravastatin 40 mg - 80 mgLovastatin 40 mgFluvastatin XL 80mgFluvastatin 40 mg bidPitavastatin 2 mg -4 mg
Simvastatin 10 mgPravastatin 10 mg - 20 mgLovastatin 20 mgFluvastatin 20 mg - 40 mg Pitavastatin 1 mg
Reference: Circulation. 2014;129(25 suppl 2):S13.
JOURNAL CE

26 Palmetto Pharmacist • Volume 56 Number 3
Even if high-intensity is indicated, some patients may not tolerate higher statin dosages and warrant dosage reductions. Characteristics predisposing patients to statin adverse effects are the following: age over 75 years, drug-drug interactions, a history of statin myopathy or muscle disorders, has unexplained alanine transaminase (ALT) levels ≥3 times the upper limit of normal, or has multiple or serious comorbidities. Having a statin on board at a lower dose currently preferred to switching to another class of lipid lowering drugs. Once the intensity of the statin is assigned, no dose titration is recommended. The main reason to monitor LDL-C is to assess compliance and response to therapy.
Example case using pooled cohort equation:
59 year-old Caucasian male. His total cholesterol is 180 mg/dL, HDL-C is 40 mg/dL, and systolic blood pressure is 150 mmHg. He has diabetes and hypertension and is being treated for both diseases. He smokes a pack of cigarettes a day.
His 10-year and lifetime ASCVD risks are 36.1% and 69%, respectively. If all of his risk factors were optimized, his 10-year ASCVD risk could be reduced to 5.2%. Although this patient is a good candidate for a high-intensity statin, providing this information can help him make sense of a multi-factorial treatment plan and really shows the impact of smoking cessation, blood pressure reduction, and appropriate statin therapy.
National Lipid Association Dyslipidemia Guidelines: Although guidelines for dyslipidemia changed dramatically from the NCEP’s recommendations to those of the ACC/AHA, setting cholesterol goals for prevention of heart attacks and strokes is still being debated. For example, in 2014 the National Lipid Association (NLA) offered a third installment of its dyslipidemia management guidelines that reaffirmed the use of surrogate markers, especially non-HDL-C, when treating patients with dyslipidemia.13 It should be noted the reason the NLA provides for these surrogate marker goals is based on cohort data associating non-HDL-C levels with risk of CHD. The NLA authors maintain that atherogenic cholesterol, in particular, non-HDL-C, is the main cause of atherosclerosis. Epidemiological studies have shown that non-HDL-C is a stronger predictor of ASCVD than LDL-C alone.14-16 The 2013 International Atherosclerosis Society,17 the 2012 Canadian Cardiovascular Society,18 and the European Atherosclerosis Society19 guidelines also support non-HDL-C as the best surrogate marker threshold and target.
Non-HDL-C includes all cholesterol that contains atherogenic particles, such as LDL-C, very low-density lipoproteins (VLDL), intermediate density lipoproteins, chylomicrons, and lipoprotein (a).14-16 The target non-HDL-C is <130 mg/dL in patients with ASCVD risk factors and <100 mg/dL in patients who already have ASCVD or diabetes with ≥2 major ASCVD risk factors, as indicated in Table 3.13
Table 3: Setting Non-HDL-C Goals13
Risk Category Criteria Non-HDL-C Goal(mg/dl)
Low 0-1 major ASCVD risk factors < 130Moderate 2 major ASCVD risk factors < 130High ≥ 3 major ASCVD risk factors
-Diabetes (type 1 or 2) with 0-1 major ASCVD risk factors-Chronic kidney disease (stage 3 or 4)-LDL-C ≥ 190 mg/dL
< 130
Very High -ASCVD-Diabetes (type 1 or 2) with ≥ 2 major ASCVD risk factors-Evidence of end-organ damage
< 100
ASCVD, atherosclerotic cardiovascular disease
JOURNAL CE

Palmetto Pharmacist • Volume 56, Number 3 27
JOURNAL CEAdapted from Journal of Clinical Lipidology. 2014;8(5):477.
While non-HDL-C is hypothesized to be the best surrogate marker, and recommended as a target by the NLA and other international guidelines, there is insufficient data from randomized controlled trials indicating that adding or titrating lipid-lowering medications to achieve specific non-HDL-C goals significantly reduces ASCVD events.
No matter what approach the clinician takes, all the guidelines for the management of dyslipidemia emphasize a “patient-centered approach” where the patient should take an active role and participate in making decisions for his or her management of dyslipidemia.11,13 The patient-centered theme is an increasingly popular approach because transferring some of the decision-making responsibility over to the patient can lead to improved adherence and outcomes.
Treatment Options for Dyslipidemia:
The first-line therapy in dyslipidemia is statins, which inhibit the enzyme that is the rate-limiting step in cholesterol synthesis. The particular statin and dose should be chosen based on the patient’s ASCVD risk. It is important to educate a patient on potential adverse effects and to explain the long-term benefits of taking a statin. If a patient has side effects from a statin, he or she should be switched to a different statin or have the dosage decreased or changed to an intermittent dosing schedule such as every other day.
Before initiation of a statin, a patient’s baseline liver function tests (ALT) should be established. Routine monitoring is not recommended at this time, but should be considered if patients develop symptoms of hepatotoxicity. In the United States, about 33 million people are taking a statin, and up to 25% of them will experience some type of musculoskeletal pain induced by the statin therapy.20 Therefore, every patient should be informed of the possibility of myalgias and rhabdomyolysis while on statin therapy, and report any signs of muscle weakness, jaundice, pain, or dark, red or cola-colored urine. Combined use of a statin with gemfibrozil or niacin potentially increases the risk of myopathies. Simvastatin, lovastatin, and atorvastatin are major substrates of cytochrome P450 3A4 with simvastatin and lovastain undergoing extensive first-pass metabolism. All three of these statins are at considerable risk of drug interactions due to their CYP 3A4 metabolism. Table 4 lists specific counseling points adapted from Lexicomp Online® that are important when speaking with a patient about a particular statin.
Table 4: Counseling Pearls For Individual StatinsSimvastatin • Take at bedtime
• Do not exceed 10 mg with diltiazem, verapamil or dronedarone • Do not exceed 20 mg with amiodarone, amlodipine, or ranolazine • Use with caution when patient is taking a CYP450 3A4 inhibitor• The 80 mg dose is limited to patients that have been taking that dose for
>12 consecutive months without myopathy and without interacting medi-cations
Lovastatin • Take with evening meal• Do not exceed 20 mg per day with danazol, diltiazem, dronedarone or
verapamil• Use with caution when patient is taking a CYP450 3A4 inhibitor• Do not exceed 40 mg with amiodarone
Atorvastatin • Can be taken at any point in the day • Use with caution when patient is taking a potent CYP450 3A4 inhibitor• Do not exceed 20 mg with clarithromycin, itraconazole, and several HIV
treatment regimens• Do not exceed 40 mg with boceprevir or nelfinavir
28 Palmetto Pharmacist • Volume 56 Number 3
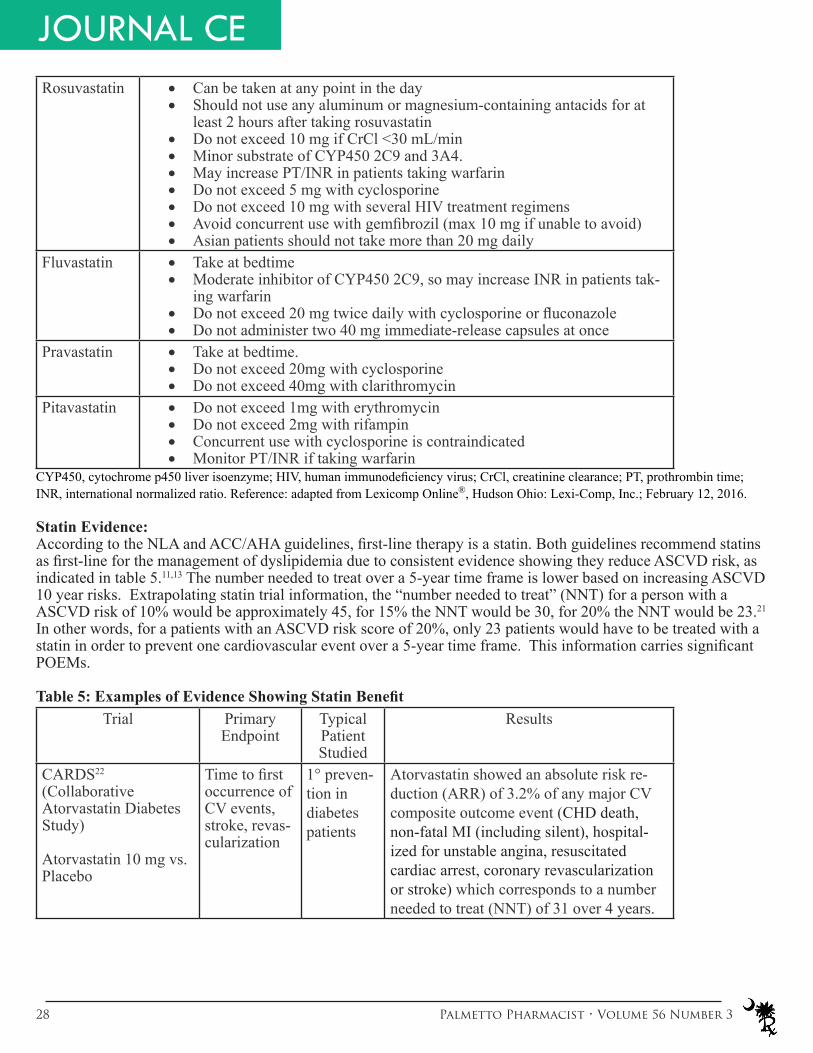
JOURNAL CERosuvastatin • Can be taken at any point in the day
• Should not use any aluminum or magnesium-containing antacids for at least 2 hours after taking rosuvastatin
• Do not exceed 10 mg if CrCl <30 mL/min• Minor substrate of CYP450 2C9 and 3A4.• May increase PT/INR in patients taking warfarin• Do not exceed 5 mg with cyclosporine• Do not exceed 10 mg with several HIV treatment regimens• Avoid concurrent use with gemfibrozil (max 10 mg if unable to avoid)• Asian patients should not take more than 20 mg daily
Fluvastatin • Take at bedtime• Moderate inhibitor of CYP450 2C9, so may increase INR in patients tak-
ing warfarin• Do not exceed 20 mg twice daily with cyclosporine or fluconazole• Do not administer two 40 mg immediate-release capsules at once
Pravastatin • Take at bedtime.• Do not exceed 20mg with cyclosporine• Do not exceed 40mg with clarithromycin
Pitavastatin • Do not exceed 1mg with erythromycin• Do not exceed 2mg with rifampin• Concurrent use with cyclosporine is contraindicated• Monitor PT/INR if taking warfarin
CYP450, cytochrome p450 liver isoenzyme; HIV, human immunodeficiency virus; CrCl, creatinine clearance; PT, prothrombin time; INR, international normalized ratio. Reference: adapted from Lexicomp Online®, Hudson Ohio: Lexi-Comp, Inc.; February 12, 2016.
Statin Evidence:According to the NLA and ACC/AHA guidelines, first-line therapy is a statin. Both guidelines recommend statins as first-line for the management of dyslipidemia due to consistent evidence showing they reduce ASCVD risk, as indicated in table 5.11,13 The number needed to treat over a 5-year time frame is lower based on increasing ASCVD 10 year risks. Extrapolating statin trial information, the “number needed to treat” (NNT) for a person with a ASCVD risk of 10% would be approximately 45, for 15% the NNT would be 30, for 20% the NNT would be 23.21
In other words, for a patients with an ASCVD risk score of 20%, only 23 patients would have to be treated with a statin in order to prevent one cardiovascular event over a 5-year time frame. This information carries significant POEMs.
Table 5: Examples of Evidence Showing Statin BenefitTrial Primary
EndpointTypical Patient Studied
Results
CARDS22 (Collaborative Atorvastatin Diabetes Study)
Atorvastatin 10 mg vs. Placebo
Time to first occurrence of CV events, stroke, revas-cularization
1° preven-tion in diabetes patients
Atorvastatin showed an absolute risk re-duction (ARR) of 3.2% of any major CV composite outcome event (CHD death, non-fatal MI (including silent), hospital-ized for unstable angina, resuscitated cardiac arrest, coronary revascularization or stroke) which corresponds to a number needed to treat (NNT) of 31 over 4 years.

Palmetto Pharmacist • Volume 56, Number 3 29
JOURNAL CEHPS (Heart Protection Study)23
Simvastatin 40 mg vs. Placebo
First major coronary event and first major vascular event
High risk patients with secondary prevention or DM
Simvastatin 40 mg is beneficial for reducing the risk of MI, stroke, and revascularization in people with DM, even without the presence of CHD or high cholesterol over 5 years. Simvastatin provided a 1.8% ARR in all-cause mortality and a 5.4% reduction in major vascular events over a 5-year treatment period corresponding to NNTs of 23 to prevent one death and 19 to prevent a major vascular event.
TNT (Treating to New Targets)24
Atorvastatin 80 mg vs. Atorvastatin 10 mg
Occurrence of major CV event (death from CHD, MI, resuscitation, stroke)
Secondary prevention
Use of an 80-mg dose of atorvastatin to reduce LDL-C levels to 77mg/dL provides additional benefit in patients with stable CHD that is perceived to be well controlled at an LDL-C level of approximately 100 mg/dL. NNT to prevent a major cardiovascular event over 5 years is 24.
IDEAL- (Incremental decreases in endpoints through aggressive lipid lowering) 25 Atorvastatin (40-80mg/day) vs. Simvastatin (20-40mg/day)
Composite: coronary death, non-fatal MI, or cardiac arrest with resuscitation
Secondaryprevention
The IDEAL trial focuses on a comparison of intensive vs low-moderate dose statins. While composite endpoint was not statistically significant, individual endpoints were. NNT to prevent any cardiovascular event over 4.8 years is 23.
CV, cardiovascular; CHD, coronary heart disease; MI, myocardial infarction; NNT, number needed to treat; DM, diabetes mellitus
Second-line treatment options:While statins have consistently demonstrated reduced risk of cardiovascular events, non-statin cholesterol lowering drugs have mixed results in randomized control trials and various interpretations. In patients who are candidates for statins but are statin intolerant, non-statin medication with evidence from randomized control trials can be considered according to current guidelines. Table 6 shows alternative dyslipidemia treatment options. Other than the recent data regarding ezetimibe plus simvastatin from the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) in patients with recent acute coronary syndrome, there is no data supporting the use of non-statin drugs combined with statins to further reduce cardiovascular events.
Table 6: Second-line treatment optionsMedication Class Evidence
• Gemfibrozil• Fenofibrate
• Fibric acid de-rivative
VA-HIT26 trial showed benefit for gemfibrozil compared to placebo in men with a history of heart disease (NNT to prevent a nonfatal MI and CHD death over 5.1 years is 23).
• Niacin • Nicotinic acid CDP27 trial conducted in the 1960s with immediate release niacin compared to placebo showed a non-significant trend toward decreased total mortality (Secondary endpoint: NNT to prevent recurrent nonfatal MI event over 6.2 years is 23).

30 Palmetto Pharmacist • Volume 56 Number 3
JOURNAL CE• Cholestyramine• Colesevelam
• Bile acid se-questrant
LRC-CPPT28 trial showed benefit for cholestyramine compared to placebo for primary prevention (NNT to prevent a nonfatal MI and CHD death over 7.4 years is 59).
• Ezetimibe • Selective cholesterol absorption in-hibitor
IMPROVE-IT29 trial showed benefit of ezetimibe 10mg combined with simvastatin 40mg compared to simvastatin alone in patients who had acute coronary syndrome in the last 10 days (NNT to prevent a composite cardiovascular event over 7 years is 50).
• Mediterranean Diet
• Diet PREDIMED30 trial showed benefit of a Mediterranean diet supplemented by extra virgin olive oil or nuts for primary prevention (NNT to prevent a stroke, MI or death over 4.8 years is 61).
CHD, coronary heart disease; MI, myocardial infarction; NNT, number needed to treat
Proprotein Convertase Subtilisin Kexin Type 9 (PCSK9) Inhibitors:A new drug class, referred to as PCSK9 inhibitors is creating considerable interest in lipid management.31 PCSK9 inhibitors get their name from their mechanism of action; they work by inhibiting a protein known as proprotein convertase subtilisin kexin type 9 (PCSK9).
There are two metabolic processes important to understanding the mechanism of these drugs. The first is that LDL-C particles bind to LDL receptors (LDL-R) on the cell surface and then are taken into the cell to be metabolized. When the LDL-C/LDL-R complex is metabolized, LDL-C is degraded and LDL-R is recycled to the cell surface to remove more circulating LDL-C. This process has a net effect of reducing circulating LDL-C. A different process occurs when endogenous PCSK9 binds to the LDL-C along with the LDL-R complex. All three are taken into the cell as a complex. Along with the LDL-C, the LDL-R is completely degraded, which prevents the LDL-R from being recycled. Fewer receptors on the cell surface allows LDL-C to accumulate.32 If PCSK9 is inhibited, the first process above dominates; LDL-R is constantly recycled to the cell surface substantially decreasing circulating LDL-C. Mutations in PCSK9 has been shown to affect LDL-C levels and also to impact the risk of CHD; if inhibited it lowers LDL-C and decreases the risk of CHD and if promoted, it increases LDL-C and the risk of CHD. A retrospective study of the etiology of atherosclerosis over a 15 year interval was undertaken to determine whether a relationship existed between PCSK9 function, LDL-C levels, and CHD. People who have a mutation in PCSK9 leading to improper protein function had, on average, a 15-22% reduction in LDL-C and a 47-88% reduction in CHD.33 Studies have shown that inhibiting PCSK9 activity with monoclonal antibodies results in a significant reduction in LDL-C and non-HDL cholesterol levels. Alirocumab, developed by Sanofi and Regeneron Pharmaceuticals and marketed as the brand name Praluent, was the first PCSK9 inhibitor approved by the FDA.34 It is indicated as ad-junct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hyper-cholesterolemia or clinical atherosclerotic cardiovascular disease, who require additional lowering of LDL-C. The ODDYSSEY LONG TERM trial demonstrated alirocumab’s ability to lower LDL-C when added to a max tolerated statin therapy. The study lasted 78 weeks and involved 2341 patients. At 24 weeks the treatment group had a 62% decrease in LDL-C when compared to placebo (p<0.0001).35 The starting dose is 75mg injected subcutaneously every 2 weeks as this dose is effective in a majority of patients. If LDL-C response is inadequate, the dose may be increased to 150mg. A post-hoc analysis suggested a 1.6% absolute risk reduction of major cardiovascular events. Verified outcomes are still pending as the The ODDYSSEY OUTCOMES trial is currently prospectively evaluating the long-term effects of alirocumab on cardiovascular events.36
Evolocumab is another PCSK9 inhibitor recently approved by the FDA and marketed by Amgen as Repatha.37 The package insert states that Repatha is indicated as an adjunct to diet and maximally tolerated statin therapy for treat-

Palmetto Pharmacist • Volume 56, Number 3 31
ment of adults with heterozygous familial hypercholesterolemia or clinical atherosclerotic disease who require ad-ditional lowering of LDL-C. It is also indicated as an adjunct to other LDL-C lowering therapies in patients with homozygous familial hypercholesterolemia who require additional lowering of LDL-C. Dosing is either 140mg in-jected subcutaneously every 2 weeks or 420 mg monthly. Data from a phase three trial has shown that evolocumab, when given as monotherapy, can reduce LDL-C levels by 58%.38 Data also indicates that evolocumab can pro-vide an additional 68% reduction in LDL-C when the agent is administered with statin therapy. The OSLER trials showed similar LDL-C lower results as well as demonstrated preliminary cardiovascular risk reduction benefits.39 The FOURIER trial is currently evaluating long-term CV risk reduction.40
While further outcome studies are pending, it is predicted PCSK9 inhibitors hold promise in certain patients who cannot tolerate statins or those with familial hypercholesterolemia who do not achieve favorable reductions in atherogenic cholesterol and event reductions on a statin. These agents are, however, expensive at approximately $10,000 a year (per patient) and this could impact the financial feasibility for some patients.
Conclusion: The evidence regarding the treatment of dyslipidemia has grown over the past few years and dyslipidemia guidelines have evolved to reflect the body of evidence. Pharmacists can use the guidelines to benefit patients. Efforts can be made to target patients who meet the criteria for one of four statin benefit groups. The new pooled-cohort equation calculator, also referred to as the ASCVD risk estimator, is a useful tool to help guide both providers to appropriate intensity of therapy and for patients to understand the importance of statin therapy and the management of modifiable risk factors. If goals are desired, there are observational studies and guideline support for targeting non-HDL-C although there is a lack of randomized trials verifying outcomes of such an approach. Without contraindications, statins are the preferred first-line class of medications in the current guidelines and should be dosed at appropriate intensity determined by overall risk of an event. Pharmacists should be knowledgeable about the differences between the statins and capable of providing relevant counseling to patients. Pharmacists should also be up-to-date on knowledge of new medications, such as PCSK9 inhibitors, for the management of dyslipidemia and place in therapy.
References1. Mozaffarian D, Benjamin EJ, Go AS, et al.; on behalf of the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322.2. Kochanek KD, Murphy SL, Xu J, Arias E. Mortality in the United States, 2013. NCHS data brief, no 178. Hyattsville, MD: National Center for Health Statistics. 2014.3. Giberson S, Yoder S, Lee MP. Improving patient and health system outcomes through advanced pharmacy practice. A report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service. Dec 2011. 4. Machado M, Nassor N, Bajcar JM, Guzzo GC, Einarson TR. Sensitivity of Patient Outcomes to Pharmacist Interventions. Part III: Sys-tematic Review and Meta-Analysis in HyperlipidemiaManagement. Ann Pharmacother. 2008;42:1195-207.5. Brunzell JD, Davidson MH, Furberg CD, et al. Lipoprotein management in patients with cardio-metabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31:811-22.6. Faxon DP, Fuster V, Libby P, et al. Atherosclerotic Vascular Disease Conference: Writing Group III: pathophysiology. Circulation. 2004;109:2617-25.7. McNamara JR, Jenner JL, et al. Change in LDL particle size is associated with change in plasma triglyceride concentration. Arterio-sclerosis and Thrombosis. 1992;12:1284-90.8. Tirosh A, Rudich A, Shochat T, et al. Changes in triglyceride levels and risk for coronary heart disease in young men. Ann Intern Med. 2007;147(6):377-85.9. Sirtori CR. HDL and the progression of atherosclerosis: new insights. Eur Heart J Suppl. 2006;8(suppl F):F4-9.10. National Human Genome Research Institute. “Familial Hypercholesterolemia.” www.genome.gov/25520184. Accessed May 15, 2015.11. Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guide-lines. Circulation. 2014;129(25 suppl 2):S1–45.12. Shaughnessy AF, Slawson DC, Bennett JH. Becoming an information master: a guidebook to the medical information jungle. J Fam Pract 1994; 39:489-99.13. Jacobson, Terry A., Matthew K. Ito, Kevin C. Maki, Carl E. Orringer, Harold E. Bays, Peter H. Jones, James M. Mckenney, Scott M. Grundy, Edward A. Gill, Robert A. Wild, Don P. Wilson, and W. Virgil Brown. "National Lipid Association Recommendations for Patient-centered Management of Dyslipidemia: Part 1 – Executive Summary." Journal of Clinical Lipidology. 2014;8(5):473-88.14. Kastelein, J.J., van der Steeg, W.A., Holme, I., and TNT Study Group; IDEAL Study Group. Lipids, apolipoproteins, and their ratios in relation to cardiovascular events with statin treatment. Circulation. 2008;117:3002–9.15. Boekholdt, S.M., Arsenault, B.J., Mora, S. et al. Association of LDL cholesterol, non-HDL cholesterol, and apolipoprotein B levels with risk of cardiovascular events among patients treated with statins: a meta-analysis. JAMA. 2012;307:1302–9.
JOURNAL CE

32 Palmetto Pharmacist • Volume 56 Number 3
References Continued 16. Liu J. Sempos CT. Donahue RP. Dorn J, Trevisan M, Grundy SM. Non-high-density lipoprotein and very-low-density lipoprotein cho-lesterol and their risk predictive values in coronary heart disease. Am J Cardiol. 2006;98:1363-8.17. An International Atherosclerosis Society Position Paper: Global Recommendations for the Management of Dyslipidemia (2013). Web. (http://www.athero.org/download/IASPPGuidelines_FullReport_20131011.pdf> Accessed May 9, 2015.18. Anderson, Todd J. et al. 2012 Update of the Canadian Cardiovascular Society Guidelines for the Diagnosis and Treatment of Dyslipid-emia for the Prevention of Cardiovascular Disease in the Adult. Can J Cardiol. 2013;29(2):151–67.19. Catapano AL, Reiner Z, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the man-agement of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Atherosclerosis. 2011;217(1):3-46.20. Spatz ES, Canavan ME, Desai MM. From here to JUPITER: identifying new patients for statin therapy using data from the 1999–2004 National Health and Nutrition Examination Survey. Circ Cardiovasc Qual Outcomes. 2009;2(1):41-8.21. Bandolier Evidence Based Thinking About Healthcare. University of Oxford. http://www.medicine.ox.ac.uk/bandolier/booth/cardiac/statcalc.html. Accessed October 23, 2015.22. Colhoun HM et al, Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364(9435):685-96.23. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7-22.24. LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425-35.25. Pedersen TR, Faergeman O, Kastelein JJP, et al; the Incremental Decrease in Events through Aggressive Lipid Lowering (IDEAL) Study Group. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction. The IDEAL study: a randomized controlled trial. JAMA. 205;294:2437-2445.26. Robins SJ, Collins D, Wittes JT, et al. Relation of gemfibrozil treatment and lipid levels with major coronary events: VA-HIT: a ran-domized controlled trial. JAMA. 2001;285(12):1585-91.27. Berge KG, Canner PL. Coronary drug project: experience with niacin. Coronary Drug Project Research Group. Eur J Clin Pharmacol. 1991;40(Suppl 1):S49-51.28. The Lipid Research Clinics Coronary Primary Prevention Trial results. Reduction in incidence of coronary heart disease. JAMA. 1984;251(3):351-64.29. Cannon CP, et al. "Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes". The New England Journal of Medicine. 2015. 375(25):2387-2397.30. Estruch R, Ros E, Salas-Salvado J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med. 2013;368:1279-90.31. Brendan M. Everett, M.D., M.P.H., Robert J. Smith, M.D., and William R. Hiatt, M.D. Reducing LDL with PCSK9 Inhibitors - The Clinical Benefit of Lipid Drugs. N Engl J Med 2015; 373:1588-1591.32. Peterson A, Fong L, Young S. PCSK9 function and physiology. J Lipid Res. 2008 Jun: 49(6): 1152-1156.33. Cohen, Jonathan C., Eric Boerwinkle, Thomas H. Mosley, and Helen H. Hobbs. "Sequence Variations In Low LDL, and Protection against Coronary Heart Disease." N Engl J Med. 2006;354:1264-72.34. Praluent [Package Insert]. Bridgewater, NJ: Sanofi Aventis. Revised 7/201535. Robinson J, Farnier M, Krempf M, et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N Engl J Med. 2015;372:1489-99. 36. Schwartz GG, Bessac L, Berdan LG, et. Effect of alirocumab, a monoclonal antibody to PCSK9, on long-term cardiovascular outcomes following acute coronary syndromes: rationale and design of the ODYSSEY outcomes trial. Am Heart J. 2014 Nov;168(5):682-9.37. Rapatha [Package Insert]. Thousand Oaks, CA: Amgen Pharmaceuticals. Revised 09/15.38. Koren MJ, Lundqvist P, Bolognese M, et al. Anti-PCSK9 Monotherapy for Hypercholesterolemia: The MENDEL-2 Randomized, Con-trolled Phase III Clinical Trial of Evolocumab. J Am Coll Cardiol. 2014;63(23):2531-40.39. Sabitine M, Guigliano R, Wiviott S, et al. Efficacy and Safety of Evolocumab in Reducing Lipids and Cardiovascular Events. N Eng J Med. 2015;372:1500-9.40. Amgen. Further Cardiovascular Outcomes Research With PCSK9 inhibition in Subjects With Elevated Risk (FOURIER). In: Clinical-Trials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000- [Cited 2014 Aug 18]. Available from: http://clinicaltrials.gov/ct2/show/study/NCT01764633 NLM Identifier: NCT01764633.

Palmetto Pharmacist • Volume 56, Number 3 33
Dyslipidemia Drug Update and Guidelines ReviewCorresponding Course Program Number: 0171-9999-16-018-H01-P1. Complete and mail entire page. SCPhA members can take journal CE for free; $15 for non-members. Check must accompany test. You may also complete the test and submit payment online at www.scrx.org.2. Mail to: Palmetto Pharmacist CE, 1350 Browning Road, Columbia, SC 29210-6309.3. Continuing Education statements of credit will be issued within six weeks from the date of the quiz, evaluation form and payment are recieved. Noti� cation will be sent via eamil if you have not successfully completed the quiz.4. Participants scoring 70% or greater and completing the program evaluation form will be issued CE credit. Participants recieving a failing grade on any examination will have the examination returned. � e participant will be permitted to retake the examination one time at no extra charge.South Carolina Pharmacy Association is accredited by the Accreditation Council for Pharmacy Education as providers
for continuing education. � is article is approved for 1 contact hour of contiuning education credit (ACPE: UAN: 0171-9999-16-018-H01-P). � is CE credit begins 04/28/2016 and expires 04/28/2019. CE credit will be upload-ed to the CPE Monitor System.
Name _______________________________ License # _________________ Birth Month/Day (MM/DD)___________Address _________________________________________________________________________________________NABP eID ______________ Phone _______________ Email ______________________________________________EVALUATION (circle the appropriate response)1. Did the article achieve the stated objects? (Note at all) 1 2 3 4 5 (Completely)
2. Overall evaluation of the article? (Poor) 1 2 3 4 5 (Excellent)
3. Was the information relevent to your practice? (No) 1 2 3 4 5 (Yes)
4. How long did it take you to read the article and complete the exam? _______________CE credit will ONLY be awarded when a submitted test is accompanied by completing the evaluation above or online at www.scrx.org.
Self-Assessment Questions:
1. Which of the following variables is not built into the pooled cohort equation used to estimate 10-year ASCVD risk?
A. Age B. HDL-CC. GenderD. LDL-C
2. Which of the following patients should receive a moderate-intensity statin instead of high-intensity statin therapy according to ACC/AHA guideline?
A. 30-year old with an LDL-C of 130 and no other co-morbidities with a 10-year ASCVD risk score of 4%B. 68-year old who has a history of 4-vessel heart disease and stent placementC. 45-year old male with diabetes and an LDL-C of 150 and HTN with a 10-year ASCVD risk score of 8%D. 42-year old female with diabetes and an LDL-C of 140, no other comorbidities with an ASCVD risk score of 6.8%
3. What class of cholesterol medications is recommended first-line for the management of dyslipidemia by both the ACC/AHA and NLA guidelines?
A. Omega 3 Fatty AcidsB. Fibric Acid DerivativesC. Bile acid sequestrantsD. HMG CoA-reductase inhibitors (statins)

34 Palmetto Pharmacist • Volume 56 Number 3
Self-Assessment Questions Continued4. According to the NLA guideline, what is the non-HDL-C goal for a patient that has type 2 diabetes and three risk factors for the development of ASCVD?
A. < 100 mg/dLB. < 130 mg/dLC. < 120 mg/dLD. < 70 mg/dL
5. According to ACC/AHA guidelines, what is the best recommendation for a patient who has clinical ASCVD and is 50 years old?
A. Rosuvastatin 10 mg dailyB. Simvastatin 80 mg dailyC. Atorvastatin 80 mg dailyD. Pravastatin 10 mg daily
6. According to ACC/AHA guidelines, what is the best treatment for a patient who is 45 years old, has type-2 diabetes, and has a 10-year ASCVD risk ≥ 7.5%?
A. Atorvastatin 20 mg dailyB. Rosuvastatin 20 mg dailyC. Atorvastatin 10 mg dailyD. Pravastatin 20 mg at bedtime
7. According to the ACC/AHA guideline, what is proper treatment for a patient who is 80 years old has coronary artery disease and had significant muscle pain with high-intensity and is currently taking amlodipine 10mg daily with good blood pressure control?
A. Atorvastatin 40 mg dailyB. Simvastatin 40 mg at bedtimeC. Pravastatin 40 mg at bedtimeD. Rosuvastatin 20 mg daily
8. Which of the following statements is true?
A. Do not exceed 20mg of atorvastatin daily if currently taking itraconazoleB. Rosuvastatin and atorvastatin should only be taken at bedtimeC. Simvastatin, Lovastatin both have interactions related to CYPP450 2C9D. A patient needing to start high intensity statin therapy can start Simvastatin 80mg daily
9. What is the route of administration for the PSCK9 inhibitors?
A. OralB. IntranasalC. IntravenousD. Subcutaneous
10. Which of the following is a true regarding PCSK9 inhibitors?
A. PCSK9 inhibitors cost less than brand name statins.B. A contraindication for PCSK9 inhibitors is a history of statin intolerance.C. Long term cardiovascular data has not been established for PCSK9 inhibitors.D. PCSK9 inhibitors are dosed every 3 months.











![Quantifying atherogenic lipoproteins for lipid-lowering ... · quantification of atherogenic lipoproteins in nonfasting and fasting blood samples [1, 2]. This article summarizes the](https://static.fdocuments.us/doc/165x107/5f1041c77e708231d44836fa/quantifying-atherogenic-lipoproteins-for-lipid-lowering-quantification-of-atherogenic.jpg)






