Dysfunctional management
10
Transcript of Dysfunctional management


Up to 8 Directorates at each Blood CentreNo single person in charge of all at one site – they work
independently, in consultation only
• DS 2,868• PTI 1,244• DDR 649
• Estates 485• Finance 133• IT 133
• HR 94• Clinical 70• PCS 51
• CCA 38• Strategy Management
10
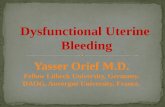
A typical Blood Centre
DS PTI DDR EST FIN IT HR CLIN

Staff Staff
Session ManagerTesting Manager
ADSM
Head of Collections
DS Director
PTI Manager
Head of PTI Ops
PTI Director
Managing Director NBS
SDSM
Collection N or S
Problems – IT, clerical, technical, quality
Directorate management impedes quality and efficiency
Problems – IT, clerical, quality
Problems generated at the bottom cannot be resolved except by agreement. No one is in charge of both collection and lab staff until the Managing Director NBS, who may be 6 tiers up the chain. Many problems therefore are not resolved.

The Directorates are very uneven in size
• DS 2,868• PTI 1,244• DDR 649
• Estates 485• Finance 133• IT 104
• HR 94• Clinical 70• PCS 51
• CCA 38• Strategy Management
10

Directorates are asymmetric: this affects the work
• How is it sensible to have one Director in charge of nearly 3,000 staff while 4 Directors have less than 100?
• We think none of them is paid less than £80,000
• All the support services have a Director. Therefore the Exec and NHSBT Board are dominated by the support service concerns.
• Core work (collecting, testing and transporting blood to hospitals) is relegated to ‘other business’ – the tail ends up wagging the dog
• The support services should have one director looking after hospital liaison (PCS), communications, strategy, HR and finance.
• A Director of Support Services would have 430 staff.

Independent directorates have certain effects
• Each Directorate has its own priorities.
• Each Directorate tends to employ managers to look after its own finance, IT, HR and strategy needs – and yet NHSBT has whole Directorates doing this as well
• This leads to a proliferation of managers, competing priorities, pressure on our department managers

NBS department managers
• In many ways the hardest job in the organisation• Caught between alienated staff and harsh reality
and strategic and theoretical plans• Support Directorates have devolved more and
more work to line managers – HR, finance, admin.
• They rarely have clerical support or a deputy• Deputies are frowned on – except for Directors!• Little input to policy, just execute policy set by
others

Staff
• Are staff alienated? Staff survey says yes.• Baffled by many national initiatives• Some initiatives are not well-grounded in real
world• Difficult or impossible to modify national policy,
even on simple operational matters• But still motivated to provide service to patients
and donors• But this is despite senior management• Senior management is supposed to assist and
facilitate daily work

Not attacking senior managers
• They are good hard-working people
• But the structure they work in does not enable them top do a good job
• Many spend huge amounts of time travelling
• Unproductive time up to 25%
• Long hours – travel, work, travel home – often 12 hour days

Not whinging - We have good positive suggestions
• End directorate management
• Merge support services into one directorate
• Each Centre to have a Director with authority over all departments
• Leave department managers to run their departments – HR and finance to take back their work