DUI SERVICE PROVIDER ORIENTATION · 10/20/2016 1 2016 idhs dui orientation‐‐assessments...
61
Transcript of DUI SERVICE PROVIDER ORIENTATION · 10/20/2016 1 2016 idhs dui orientation‐‐assessments...

DUI SERVICE PROVIDER ORIENTATION
Illinois Department of Human ServicesDivision of Alcoholism and Substance Abuse
Provided by the Institute for Legal, Legislative & Policy Studies Center for State Policy and Leadership University of Illinois Springfield

DUI SERVICE PROVIDER ORIENTATION
DAY 2 AFTERNOON:
DUI ASSESSMENT TOOLS

10/20/2016
1
2016 IDHS DUI ORIENTATION‐‐ASSESSMENTS
[email protected] OR [email protected] UPDATED 10/2016
My Training Room Rules
[email protected] OR [email protected] updated 10/2016

10/20/2016
2
30 second introduction
•Who I am…
•Where I work…•What I do…•How long I’ve been in the field…
[email protected] OR [email protected] updated 10/2016
Assessment Tools
Driver’s Risk Inventory (DRI‐2) Mortimer‐FilkinsAdult Substance Use & Driving Survey ‐ Revised Illinois (ASUDS‐RI)
•Who uses the DRI?•Who uses the M/F?•Who uses the ASUDS?•Who’s thinking about changing tools?
[email protected] OR [email protected] updated 10/2016

10/20/2016
3
Driver’s Risk InventoryDRI‐2BEHAVIOR DATA SYSTEMS
1.800.231.2401
[email protected] OR [email protected] UPDATED 10/2016
DRI‐2 Features
Normed on all (BDS‐recorded) DUI offenders
BDS reviews data collected on an annual basis and updates test as needed (+ yearly summary)
Includes gender specific norms
Identifies attempts to fake or under report problems/concerns
Measures DUI involvement and risk to public safety
It is a valid instrument
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
4
Administering the DRI‐2
113 Questions◦ Three sections of true/false and multiple choice
Computer◦ On‐line testing or flash drives
Paper and pencil
Interview
IMPORTANT: A few minutes of oral instructions can put the client at ease while providing structure and clarifying expectations.
[email protected] OR [email protected] UPDATED 10/2016
Six Empirically‐Based Measures (Scales)
Truthfulness Scale
Alcohol Scale
Drug Scale
Driver Risk Scale
Stress/Coping Abilities Scale
Substance Use Disorder Scale (DSM‐5)
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
5
DRI‐2 Scales
Truthfulness Scale—measures how truthful the client was and identifies self‐protective, recalcitrant and guarded people who minimize or even conceal information.
Alcohol Scale—measures client’s alcohol use and proneness to alcohol‐related problems.
Drug Scale—measures client’s drug use and proneness to drug‐related problems.
[email protected] OR [email protected] UPDATED 10/2016
DRI‐2 Scales (cont’d)
Driver Risk Scale—measures the client’s driving risk, independent from their involvement with alcohol/drugs. Helps identify the irresponsible/aggressive driver.
Stress/Coping Scale—measures the client’s ability to handle or cope with stress. Severely impaired coping abilities are indicative of other identifiable emotional/mental health problems.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
6
Risk RangesPercentile Rank: Risk Range:
0 to 39th percentile Low Risk
40th to 69th percentile Medium Risk
70th to 89th percentile Problem Risk
90th to 100th percentile Severe Risk
> These Risk ranges are calculated individually for five of the six.
> The Substance Use Disorder Scale is not scored as the others.
[email protected] OR [email protected] UPDATED 10/2016
Substance Use Disorder Scale
Substance Use Disorder Scale—a separate scale from the other five, and based on how many of the 11 DSM‐5 criteria are endorsed.
◦ None or one = DNM or “Low”◦ Two or three = “Moderate”
◦ Four or five = “Problem”
◦ Six or more = “Severe”
** DRI Risk Ranges vs. DASA Risk vs. DSM‐5 severity scale **
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
7
Special Scores
When the Truthfulness Scale is at or above the 95th percentile, all other scale scores (alcohol, drug, driver risk, and stress/coping) automatically go to the 99th percentile. This is to alert the evaluator to a very high Truthfulness Scale score, which means the test results are inaccurate.
What should you do?
[email protected] OR [email protected] UPDATED 10/2016
Retest
If client’s invalidate their DRI‐2, it is recommended that they be given the opportunity to be retested.
Review oral instructions before testing.
Other option?
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
8
Driver’s Risk Inventory
QUESTIONS ?
[email protected] OR [email protected] UPDATED 10/2016
Mortimer‐Filkins Assessment Tool
RUDOLF G. MORTIMER, PHD.
LYLE FILKINS (1973)
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
9
Mortimer‐FilkinsInitially devised to identify problem drinkers from among dui offenders
Initially validated against a general population
Demonstrates high degrees reliability & validity
Shown to be predictive of dui recidivism
Information from the British Journal of Addiction, Vol. 85, Issue #11, November 1990
[email protected] OR [email protected] UPDATED 10/2016
Mortimer‐FilkinsTwo parts: Interview and Test
Pencil/paper only
58 Questions on Test
188 Questions in Interview
Hand scored (using 3 scoring keys)
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
10
Questionnaire and Interview Summary Sheet
Name: _______________________ Number:______ Date:________
Questionnaire
Score Key 1Key 2
Page Page KEY
1 2 3 TOTAL TOTAL
8 10 10 28 Key 1 X 2 =56
0 4 5 9 Key 2 X 1= 9
(Subtract Key 2 from Key 1) Q = Questionnaire Score = 47
Interview Score
1 2 3 4 5 6 7 8 9 10 11 12 13 14 Page Key
0 0 0 0 Total Total
I – Interview Score: Plus Questionnaire Score: 47
Final Total Score Q + I =
Key 3X4=
[email protected] OR [email protected] UPDATED 10/2016
TABLE 1Revised (1973) Recommended Score Cut-Offs for DUI Client
Classification
Scale
Classification
Social Drinker Presumptive Problem Drinker
Problem Drinker
Questionnaire Only
11 or less 12-15 16 or greater
Interview Only 24 or less 15-39 40 or greater
Questionnaire and Interview Combined
39 or less 40 – 49 50 or greater
[email protected] OR [email protected] UPDATED 10/2016

Questionnaire and Interview Summary Sheet
Name: _______________________ Number:______ Date:________
Questionnaire
Score Key 1Key 2
Page Page KEY
1 2 3 TOTAL TOTAL
8 10 10 28 Key 1 X 2 =56
0 4 5 9 Key 2 X 1= 9
(Subtract Key 2 from Key 1) Q = Questionnaire Score = 47
Interview Score
1 2 3 4 5 6 7 8 9 10 11 12 13 14 Page Key
0 0 0 0 Total Total
I – Interview Score: Plus Questionnaire Score: 47
Final Total Score Q + I =
Key 3X4=
[email protected] OR [email protected] UPDATED 10/2016

TABLE 1Revised (1973) Recommended Score Cut-Offs for DUI Client
Classification
Scale
Classification
Social Drinker Presumptive Problem Drinker
Problem Drinker
Questionnaire Only
11 or less 12-15 16 or greater
Interview Only 24 or less 15-39 40 or greater
Questionnaire and Interview Combined
39 or less 40 – 49 50 or greater
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
11
Mortimer‐Filkins
Yes, it’s an acceptable tool per DHS/DASA, but…
1) Only assesses Alcohol
2) Only validated on males, ages 35‐45
3) Has not been updated since 1973
[email protected] OR [email protected] UPDATED 10/2016
Mortimer‐Filkins
QUESTIONS?
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
12
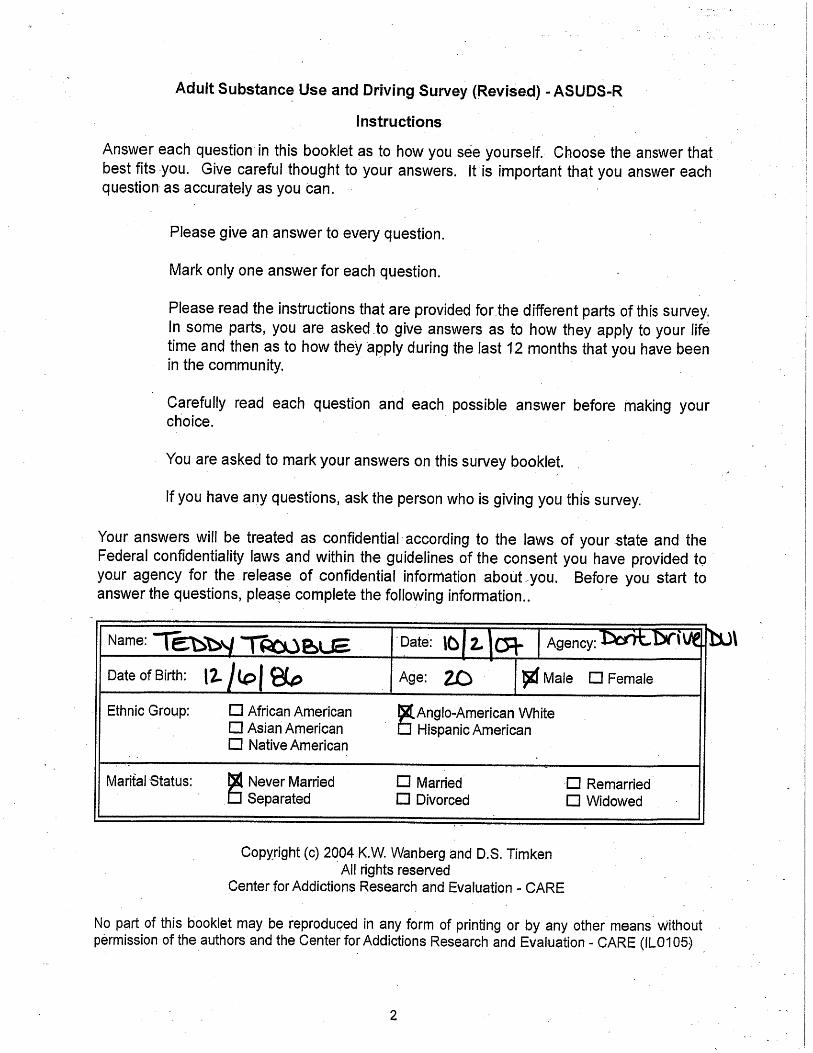
THE ADULT SUBSTANCE USE AND DRIVING SURVEY REVISED (ILLINOIS) ASUDS‐RI
Assessment of the Impaired Driving Offender
DEVELOPED BY DR. KENNETH WANBERG AND DR. DAVID TIMKEN, OF THE CENTER FOR ADDICTION RESEARCH
AND EVALUATION
[email protected] OR [email protected] UPDATED 10/2016
OVERALL GOALS OF TRAINING
To provide an introduction in the use of the
ASUDS‐RI in Differential Screening andassessment of impaired driving offenders
within the framework of the Convergent
Validation Model.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
13
Definitions
Differential Screening:
Multidimensional (AOD) screening that measures the extent to which individuals are involved in various kinds of drugs and the extent of negative consequences or symptoms resulting from this involvement.
[email protected] OR [email protected] UPDATED 10/2016
Definitions (continued)
Convergent Validation Model:
Uses self‐report and other‐reports as valid representations of where the client is at the time of assessment.
[email protected] OR [email protected] UPDATED 10/2016
Self‐report Other reports

10/20/2016
14
What are the Objectives of Screening and Assessment?
1. To provide an opportunity for clients to disclose their AOD use history, or “tell their story”;
2. To give an opportunity to other sources to tell the story of how they interpret the client’s AOD history;
[email protected] OR [email protected] UPDATED 10/2016
What are the Objectives of Screening and Assessment? (CONTINUED)
3. To determine the level of defensiveness based on the discrepancy between the self report and other reports
4. Estimate the true or valid condition of the client relative to past and recent AOD use, level of mental health problems and motivation for change and treatment
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
15
Sources of Data
1) Self‐report
2) Other‐report data – law enforcement, probation officer, family members, laboratory results, etc.
* Both kinds of data are subjective
[email protected] OR [email protected] UPDATED 10/2016
To achieve the above stated goals, the evaluator has two sources of data:
Other‐report Data is:
Double‐subjective, meaning…
Subject to different interpretations.
Can be controlled if there is an established criteria for decision making which improves the evaluators’ reliability.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
16
Self‐report Data is Essential
It is a valid representation of client at assessment
Client’s willingness to self‐disclose
View distortions as perceptual defensiveness
A change in that view or increase in self‐disclosure means treatment is working
[email protected] OR [email protected] UPDATED 10/2016
…reality is as client perceives it. We approach the world through the process of interpretation. We construct our own realities and form views of ourselves.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
17
Self‐report data can be made more objective if:
Collected in a standardized format
Uses multiple variable measures to cancel out errors.
The evaluator establishes rapport with client –motivational interviewing
[email protected] OR [email protected] UPDATED 10/2016
From The Convergent Validation Perspective Self‐report is the baseline measure of the client’s willingness to self‐disclose at the time of assessment
Self‐report should not be reported as invalid, but rather indicative of the discrepancy between sources of data
Reframe the view of lying, minimizing or denial as perceptual defensiveness.
Getting valid and reliable data depends on building trust and rapport with the client, being up‐front as to how the data will be used, and communicating a positive regard for the client’s self‐disclosure
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
18
Group Activity
[email protected] OR [email protected] UPDATED 10/2016
ASUDS‐RI General Overview and Description
Self‐Report, differential screening instrument for impaired driving offenders ages 16 and older
Self‐administered or interview administered
Appropriate for individuals who are being processed through the judicial system for impaired driving
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
19
General Overview And Description
Comprised of 113 self‐report items◦13 Basic scales, and six (6) Supplemental scales
Basic Scales #1‐11 are normed on impaired IL driving offenders.
Basic Scales #12‐13 are normed on a clinical sample of AOD clients in IOP or Residential treatment.
Supplemental Scales A,B,C are normed on the clinical sample.
Supplemental Scales D,E,F are normed on the Illinois DUI offender.
[email protected] OR [email protected] UPDATED 10/2016
Guidelines For Using Self‐reportPsychometric Tests
Methods of test administration should be standardized
Reading level of client should be checked
Screening instrument should not be used for comprehensive assessment –It is not ASAM. It is not a SUD diagnosis.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
20
Guidelines (Continued)
When using computerized scoring, evaluator should have knowledge of the test itself and not just rely on the computerized interpretation
Clients should receive feedback from their assessment results compared to the normative group.
[email protected] OR [email protected] UPDATED 10/2016
ASUDS‐RI
SCALES AND MEASUREMENTS
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
21
Teddy’s Test
[email protected] OR [email protected] UPDATED 10/2016
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
22
Teddy Trouble 20
25
[email protected] OR [email protected] UPDATED 10/2016
1. Alcohol Involvement (Items 1‐13)
• Measures the extent of involvement in alcohol use.• Measures low level of alcohol use patterns and problems, and many can be endorsed by the average drinker with no alcohol use problems.
• Is a reliable and valid measure of involvement in alcohol use, and, to some extent, abuse.
• Average drinkers will have raw scores in range of one to 10, as it is hard for clients to not provide low‐range affirmative responses.
Teddy’s score is 25
[email protected] OR [email protected] UPDATED 10/2016

[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
23
2. Driving Risk (Items 14 – 25)
• General everyday driving situations…
• Most DUI clients are reluctant to endorse these items because of perceived threat to loss of license
• Their scores increase on retesting when their responses are perceived to no longer be a threat to loss of license
• Those with a raw score of 10 or higher are being open about their driving habits and attitudes, but also represent a risk
Teddy’s score is 9
[email protected] OR [email protected] UPDATED 10/2016
3. AOD Involvement (Items 26‐35)
• Provides a measure of life time involvement in the 10 major drug categories
• Many multiple drug users may have not used some of the drugs recently, thus age of last use is an important variable
Teddy’s score is 9
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
24
4. AOD Use Benefits (1‐3, 8, 13, 37‐44)
• Measures the degree to which client reports using alcohol or other drugs for social and psychological benefits
• Good indication whether client is using alcohol or other drugs to manage depression, anxiety, feel good, be more sociable
• Moderate to high score suggests AOD psychosocial dependence
Teddy’s score is 17
[email protected] OR [email protected] UPDATED 10/2016
5. AOD Disruption1 (45‐64)
• Broad measure of problems and negative consequences due to AOD use
• Focus is on disruptive signs and symptoms in relationship to drug use in general, not to any specific drug or drug category.
• High scores indicate AOD related loss of behavioral control, disruption of psychosocial functions, and disruption of social role expectations
Teddy’s score is 34
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
25
6. AOD Involvement 12 Months Before Arrest(26‐35, 45‐64)
Same as Scale 3 (lifetime), but…
Broad measure of problems and negative consequences due to AOD use in 12 months prior to last DUI arrest
Focus is on disruptive signs and symptoms in relationship to drug use in general in those 12 months BEFORE arrest…
After arrest, many clients go into a shape‐up mode and stop use.
Teddy’s score is 22
[email protected] OR [email protected] UPDATED 10/2016
7. Mood Adjustment – Psychological Problems(65‐73)
A single dimension of psychological and emotional disruption
High scores indicate depression, worry, anxiety, irritability, anger, feelings of not wanting to live, unable to control emotions
About 20 percent DUI clients will score in range that indicates need for further evaluation for mood/psych problems
Teddy’s score is 10
Would Teddy benefit from a psychological evaluation?
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
26
8. Social‐legal Non‐conforming(81‐106)
• Represents antisocial pattern, but should not be construed as measuring antisocial personality disorder (DSM‐5)
• Has both static and dynamic items. The dynamic items measuring aggressive behavior and rebellious attitudes, and association with antisocial peers.
• Moderate to high scores indicate anti‐social patterns and character pathology, but also indicates openness to self‐disclosure and low defensiveness.
• Item 84 (“..has been charged with DUI’) is good check for overall ASUDS‐RI response validity
Teddy’s score is 14
Look at criminal history?
[email protected] OR [email protected] UPDATED 10/2016
9. Global AOD ‐ Psychosocial Disruption(Sum Scales 3, 5, 7, 8)
• Comprised of the sum of the four scales: AOD Involvement, Disruption1, Mood Adjustment, and Social‐Legal Non‐Conformity.
• Provides a global and overall measure of the degree to which client is indicating life‐functioning problems in the areas of substance use, mood adjustment and community compliance.
• This is the scale that represents the suggested risk classification.
Teddy’s score is 67
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
27
10. Defensive (9, 74 – 80, 84)
• Measures degree to which client is able to self‐disclose
• Comprised of statements to which almost all individuals can give a yes answer, even though it may be at a “hardly at all” level of response.
• It is a measure of social desirability; want raw scores between five and 19
Teddy’s score is 15
[email protected] OR [email protected] UPDATED 10/2016
11. Motivation For Services And Change(107‐113)
• Reliable measure of degree to which client is motivated to seek help, to make changes, and to stop or to continue not to use alcohol or other drugs
• Low score on Motivation, Defensiveness, and Disruption could indicate client’s AOD and other problems are truly in low range and that high level of treatment services not needed.
•This kind of profile should be corroborated with collateral data.
Teddy’s score is 13
How does this reflects his attitude or motivation?
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
28
12. And 13: Involvement 2 And Disruption2
• Scale 12 = Scale 3, except...
• Scale 13 = Scale 5, except…
‐ 12 & 13 are normed on clinical samples:
intensive outpatient and inpatient AOD clients
• Allows comparison of client with own peers and vs. clinical sample
Teddy’s scores are 9 Involvement and 34 Disruption
[email protected] OR [email protected] UPDATED 10/2016
[email protected] OR [email protected] UPDATED 10/2016

[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
29
A. Behavioral Disruption (45‐50)
• Important to remember that this scale was normed on the clinical sample.
• Measures behavioral control loss and disruptions while under influence of drugs.
• High scores (decile ranges 8‐10) may indicate client is at risk of harm to self or others when using, and can get out of control.
Teddy’s score is 11
Do you want to explore loss of control behaviors?
[email protected] OR [email protected] UPDATED 10/2016
B.Psychophysical Disruption (51‐60)
Also normed on the clinical sample.
Measures degree to which client has experienced psychophysical symptoms associated with AOD intoxication or withdrawal.
Can be life threatening, and high scores indicate past AOD dependence.
Teddy’s score is 16.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
30
C. Social Role Disruption (61‐64)
• Final scale in this group normed on the clinical sample.
• Indicates degree to which the individual’s AOD use has disrupted normal and expected social roles, e.g. job, obeying law, family responsibilities
• High scores can be associated with depression and discouragement
• High scores suggest need for life‐management skills and training in areas of employment and family skills
Teddy’s score is 7 which falls in the low‐medium range, but he is only 20 years old.
[email protected] OR [email protected] UPDATED 10/2016
D. Social Non‐conforming (81‐92)
• Within the Community: Measure of past and current rebelliousness and even antisocial behavior and attitudes
• Those with moderate to high scores are open to self‐disclosure
• However, individuals with significant antisocial features and character pathology are often resistant to treatment.
Teddy’s score is 8
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
31
E. Legal Non‐conforming (93‐106)
• Most of these items are static variables.
• Measures degree of involvement in the adult criminal justice system: Hx of arrests, convictions, time on probation/parole, and time spent in jail or prison.
• Most DUI clients will score zero or very low. About 70% will have a low raw score on this scale (4 or less).
• 10th decile range scores on both scales D and E indicate significant problems and history of both antisocial and anti‐legal problems and may suggest a lifestyle pattern of social‐legal non‐conformity
Teddy’s score is 6
[email protected] OR [email protected] UPDATED 10/2016
F. Social‐Legal Non‐Conforming 12 Months(89‐106, last 12 Month Items)
• Measures recent legal problems.
• Over 70% of IL sample of DUI offenders will have a very low raw score (4 or less). Raw scores above 5 suggest client has had noteworthy if not significant involvement in social‐legal non‐conformity in the 12 months prior to their evaluation.
• Only 10 percent of Illinois DUI sample had a raw score of 8 or more.
• Some clients are willing to report recent involvement in the judicial system, but most DUI clients are quite guarded
Teddy’s score is 4.
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
32
ASUDS USER’S GUIDE
THE ASUDS‐RI DISK INCLUDES A COPY OF THE USER’S GUIDE. PLEASE REFER TO THIS GUIDE FOR ADDITIONAL INFORMATION.
[email protected] OR [email protected] UPDATED 10/2016
Make test instructions clear and include the following:
Answer each question as honestly as possible as to how you see yourself
Give only one answer to each question unless otherwise specified
Results will be treated as confidential
Results will be used to develop services most appropriate for you
Results will be shared with you
[email protected] OR [email protected] UPDATED 10/2016

10/20/2016
33
Something to remember….
Offender assessment is client‐centered and society‐centered. The safety and welfare of the client, others and the community are the number one priorities when determining level of service placement.
Although the ASUDS‐RI provides useful guidelines for service placement, final service and treatment referral decisions are never made solely on the results of a self‐report instrument. All sources of data are used in making these decisions.
[email protected] OR [email protected] UPDATED 10/2016
ASUDS‐RI
Questions?
[email protected] OR [email protected] UPDATED 10/2016
10/20/2016
34
THANK YOU FOR PARTICIPATING
Driver’s Risk Inventory (DRI‐2)
Mortimer‐Filkins
Adult Substance Use & Driving Survey ‐ Revised Illinois (ASUDS‐RI)
[email protected] OR [email protected] UPDATED 10/2016

DUI SERVICE PROVIDER ORIENTATION
DAY 2 AFTERNOON: HANDOUTS
DUI ASSESSMENTS