

DSRIP Meeting Agenda...Dec 07, 2016 · DSRIP Meeting Agenda PAGE 1 Date and Time December 7, 2016,...
49
DSRIP Meeting Agenda PAGE 1 Date and Time December 7, 2016, 3-5pm Meeting Title NYP PPS Project Advisory Committee Location MSCHONY, 3959 Broadway, Tower 103 (1st floor) Facilitator Anne Sperling Go to Meeting https://global.gotomeeting.com/join /237782405 Conference Line United States +1 (872) 240-3412 Access Code: 237-782-405 Attendees Project Advisory Committee Membership Meeting Topic: How to End the AIDS Epidemic Time 1. Welcome (Anne Sperling) 2. NYS and NYP PPS Updates (Isaac Kastenbaum) 3. Election Overview and Potential Impact on Healthcare (Ross Frommer and Kate Spaziani) 4. Community Health Worker Presentation (Patricia Peretz, Marielena Chacon- Travis, Maura Frank) 5. Presentation by Isabella (Laura Hernandez, Vonni Pina, Yaffa Ungar) 6. 2017 Meeting Schedule (Lauren Alexander) 7. Identify Action Items 5 mins 15 mins 30 mins 20 mins 20 mins 5 mins 2 mins
Transcript of DSRIP Meeting Agenda...Dec 07, 2016 · DSRIP Meeting Agenda PAGE 1 Date and Time December 7, 2016,...

DSRIP Meeting Agenda
PAGE 1
Date and Time December 7, 2016, 3-5pm
Meeting Title NYP PPS Project Advisory Committee
Location MSCHONY, 3959 Broadway, Tower 103 (1st floor)
Facilitator Anne Sperling
Go to Meeting https://global.gotomeeting.com/join/237782405
Conference Line United States +1 (872) 240-3412 Access Code: 237-782-405
Attendees
Project Advisory Committee Membership
Meeting Topic: How to End the AIDS Epidemic Time
1. Welcome (Anne Sperling)
2. NYS and NYP PPS Updates (Isaac Kastenbaum)
3. Election Overview and Potential Impact on Healthcare (Ross Frommer and Kate Spaziani)
4. Community Health Worker Presentation (Patricia Peretz, Marielena Chacon-Travis, Maura Frank)
5. Presentation by Isabella (Laura Hernandez, Vonni Pina, Yaffa Ungar)
6. 2017 Meeting Schedule (Lauren Alexander)
7. Identify Action Items
5 mins
15 mins
30 mins
20 mins
20 mins
5 mins
2 mins

DSRIP Meeting Agenda
PAGE 1
Date and Time December 7, 2016, 3-5pm
Meeting Title NYP PPS Project Advisory Committee
Location MSCHONY, 3959 Broadway, Tower 103 (1st floor)
Facilitator Anne Sperling
Go to Meeting https://global.gotomeeting.com/join/237782405
Conference Line United States +1 (872) 240-3412 Access Code: 237-782-405
Attendees
Beverly Ader (Visiting Nurse Service of New York) Lauren Alexander (NYP)
David Alge (NYP) Ross Fromer (CUMC)
Ana Garcia (NYP) Vonni Pina (Isabella)
Laura Hernandez (Isabella) Yaffa Ungar (Isabella)
Faith Wiggins (1199 SIEU) Lucia Capitelli (NYSPI)
Chris Duffy (St. Mary’s Hospital for Children) Jean-Marie Bradford (NYSPI)
Anthony Ercolano (NYP) Isaac Kastenbaum (NYP)
Anne Sperling (NYP) Patricia Peretz (NYP)
Kate Spaziani (NYP) Maura Frank (NYP)
Marielena Chacon-Travis (NYP) Evelyn Espana (NYP)
Henley Vargas (NYP) Sandy Merlino (VNSNY)
Carlos Molina (Hostos) Andy Nieto (NYP)
Alessia Daniele (WCMC) Emma Conroy (NYCDOHMH)
David Baily (Office of Congressman-Elect Espaillat) Anthony Notaro (Community Board 1)
Amy Shah (NYCDOHMH) Marcy Thompson (ASCNYC)
Ed Perez (Argus) Theo Figurasin (NYSNA)
Meeting Topic: How to End the AIDS Epidemic Time
1. Welcome (Anne Sperling)
2. NYS and NYP PPS Updates (Isaac Kastenbaum)
3. Election Overview and Potential Impact on Healthcare (Ross Frommer and Kate Spaziani)
4. Community Health Worker Presentation (Patricia Peretz, Marielena Chacon-Travis, Maura Frank)
5. Presentation by Isabella (Laura Hernandez, Vonni Pina, Yaffa Ungar)
6. 2017 Meeting Schedule (Lauren Alexander)
7. Identify Action Items
5 mins
15 mins
30 mins
20 mins
20 mins
5 mins
2 mins
Action Items
Description Owner Start Date Due Date Status
Share 2017 PAC meeting schedule with members / send Outlook invites
L. Alexander 12/7/2016 12/30/2016 In progress
Explore ideas generated for future PAC meeting agendas
L. Alexander 12/7/2016 Ongoing In progress
1
Presentation to New York Presbyterian
PPS Project Advisory Committee (PAC) Meeting, December 7, 2016

** Nonprofit nonsectarian long term health care center serving the
community since 1875.
* Mission: * Provide quality care through diverse programs designed to
promote health and independence both within and beyond our walls.
* Located in Northern Washington Heights * Service area extends from 110th Street north through the Bronx
* Services Include:
* Skilled Nursing Care Specialty Services include: * Rehabilitation PAC:
* Three short term rehab/PAC units (100 beds) * Expertise in care to persons with cognitive impairment and
multiple comorbidities
2
3
*Ventilator Dependent Care Unit and Step Down services (36+ beds) staffed by board certified intensivists and pulmonologists and full time respiratory therapy
* Intravenous therapies including PICC line insertion *Palliative Care *Dementia Care – 3 dedicated units engaged with
Beatitudes Comfort Matters Accreditation * Community Services:
* Senior Housing * Adult Day Health Care * Home Care – CHHA and LHCSA (wider service area of
NYC and Westchester Counties) * Community Services – Health Homes, NORCS, UMPSI
care management program, MLTC Anchor Care Management Services

4
*Isabella’s Health Home Program
Your Personal Care Managers
*
*DSRIP's purpose is to fundamentally restructure the health care delivery system by reinvesting in the Medicaid program, with the primary goal of reducing avoidable hospital use by 25% over 5 years.
*Health Home is one of the vehicles through which this goal will be
accomplished. * As a result, No two health home CMA programs utilize the same
approach to care management and care coordination
* Isabella’s Health Home Program has modeled its care management services based on DSRIP Goals
5

*
*Health Homes expands on the patient-centered medical homes model's focus of treating the “whole person” using team-based care by emphasizing integrated behavioral health services and linking patients and families to non-medical services.
*Like the PCMH model, Health
Homes seek to reduce costs and improve care quality by reducing emergency department use, hospital admissions and re-admissions, and reliance on long-term care facilities.
Eligibility is based on: • Two chronic health Conditions;
• Serious mental illness,
• One chronic condition (HIV/AIDS) and at risk for developing a second chronic condition
6
The key components of the Health Home model are:
• Comprehensive care management; • Care coordination; • Health promotion; • Comprehensive transitional care
including follow-up from inpatient and other settings;
• Patient and family support; and • Referral to community and support services.

*
* We keep our case loads - 1:40 ratio
* Integrated model where we blend ICM, with health promotion,
* Our Care Managers are Masters level trained in providing social, economic and culturally competent practice– many whom come from the same communities as our members which contributes to enrollment retention.
* Work collaboratively w/providers, community entities, and managed care plan’s care managers - partnering with them in patient education and positive outcome accountability
* We work with the New York Presbyterian Health Home and Mount Sinai Health Home
Isabella’s Health Home Program has modeled its care management services based on DSRIP Goals
7

Care Managers’ Systemic Role

**Make appointments with doctors or specialists and accompany
members to appointments as needed. *Collaborate with providers to make sure needed care is provided *Help patients understand their chronic health conditions *Provide information to help manage problems like diabetes, asthma,
or high blood pressure. Refer patients to community resources *Assist with substance abuse
*Support with weight loss, smoking cessation and/or exercise goals *Assist with housing applications, legal resources, transportation, or
other entitlement issues
9

11
•Obtain and send list of patients from Tableau
NYP ACN/Analytics/Panel
Manager
•Receives list of potentially eligible patients •Labels Health Home Patients •Sends list to PCP/CBO to review prior to IDT
NYP Health Home Admin
•Pt. Discussion during IDT •Confirmation for health home services •RN Care Manager disc. referral w/pt. •Refer to CBO
NYP Primary Care Physician
•Receives referral from NYP PCP •Attends the next patient appt. w/PCP for a warm hand off.
•Brings the pt. into care
Community Based Organization
IDT /HealthHome Work Flow
12
*
*Care manager sits in meetings every other week
*Providers review high risk cases and disc. whether Health Home appropriate of Community Health Worker/RN Care management appropriate
*Updates of on going cases are disc. by care managers *Points of medical collaboration or f/up disc.
*Invaluable relationship b/w providers, Care manager and patient

* Ms. T. 83 year old female living alone on 90 Street.
* Prior to health home referral: * Ms. T. was visiting the ER
every Friday and Saturday * Rent Arrears, losing her rent
money * Missing all of her f/up appt. * Not taking her medications as
prescribed * Family loosely involved * No way to contact her * Did not open the door when
nurses or visitors came to her home
* After Health Home Assessment:
* APS was called for financial management
* Applied for home care services
* Health Home set up daily calls to remind her to take her medication while home care was put in place.
* Weekend pattern of ER visits were I.d. and explored.
* CM advocated w/landlord re:arrears
* CM has provided biweekly updates to IDT and actively collaborated re: transportation, appt. referrals and has kept them abreast of social determinants affecting health
13
*

14
*
*Ms. T is doing well, she has not missed an appointment since we have started working w/her
*She has reduced her ER visits to 99%. She went in once for chest pains
*Has received formal diagnosis of Dementia
*Family involved and made accountable for pt. care
*Reestablished relationship with estranged daughter
*Is now spending time with her grandson whom she has not seen in years.
*No longer feels alone, knowing there is a team who supports her

*
*Referral Sheet *Call: 212-342-9514 *Email: [email protected]
Vonalis Pina, M.S.Ed., LCSW Manager of Isabella’s Health Home
15

*
16

Center for Community Health Navigation at NewYork-Presbyterian Hospital
2005: WIN for Asthma
2008: Patient Navigator
2011: PCMH
2012: WIN for Diabetes
2014: DSRIP
2015: CCHN
CENTER MILESTONES

CENTER MISSION Mission:
– To support the health and wellbeing of patients through the delivery of culturally-sensitive, peer-based support in the Emergency Department, inpatient, outpatient and community settings
Goals: – Improve patient access to NewYork-Presbyterian
– Deepen connection between Hospital and community resources
– Develop innovative patient-centered initiatives
– Advance the Community Health Worker role and workforce
– Enhance the Community Health Worker knowledge-base and inform local practice
4
PATIENT STORY
Marielena Chacon-Travis Community Health Worker
Northern Manhattan Perinatal Partnership SKATE Program
Columbia University Medical Center Ross A. Frommer
Vice President for Government & Community Affairs and Associate Dean
Like us on Facebook, Follow us on Twitter

Presidential Race – a View from 2014
Will Make a Good President
Yes No
Hillary Rodham Clinton 43% 53% Jeb Bush 29% 59% Chris Christie 24% 64% Rand Paul 26% 60% Rick Perry 24% 62%
2016 General Election Hillary Rodham Clinton 34% “The Republican Candidate” 40%
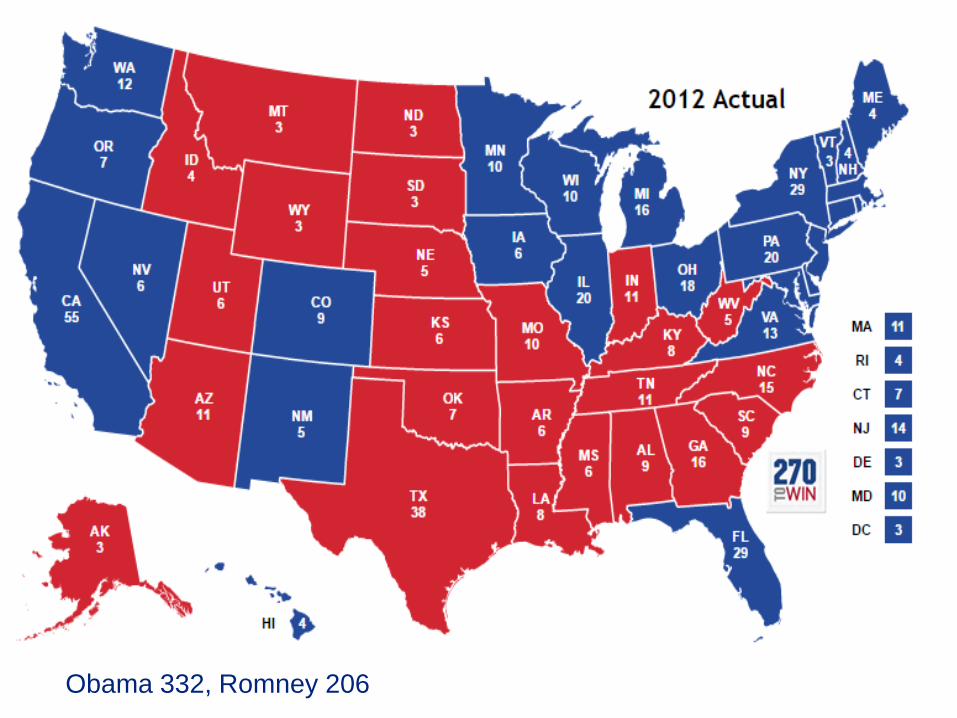
Obama 332, Romney 206

2016 Results
Trump 306 Clinton 232
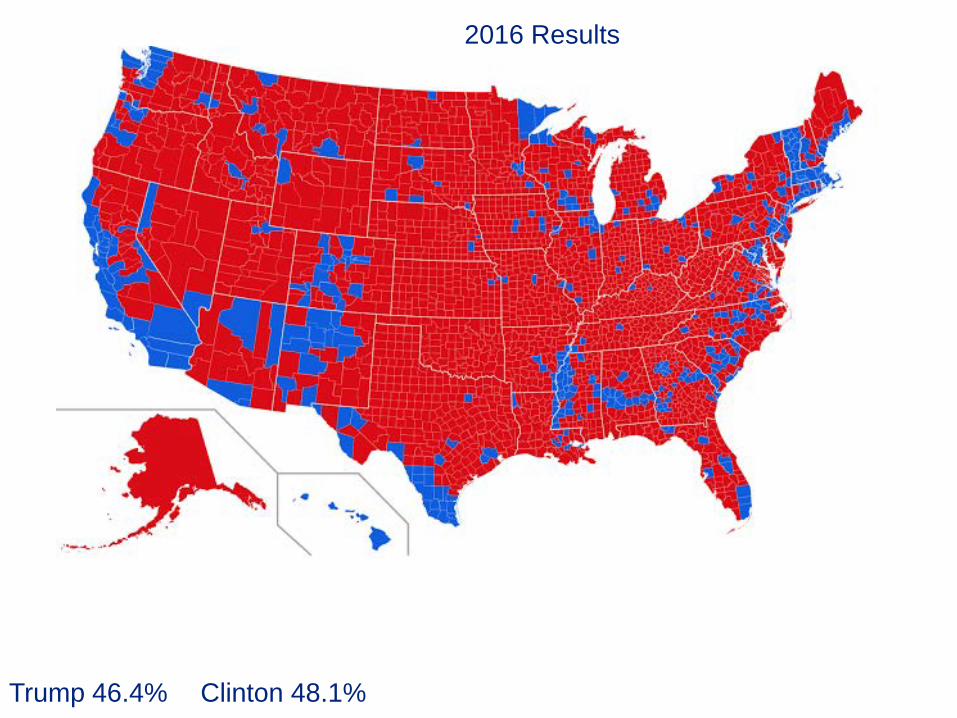
2016 Results
Trump 46.4% Clinton 48.1%

538.Com chances of winning

Polling Data
Direction of the Country Right Direction Wrong Track
RCP Average 31% 62%
President Obama Approve Disapprove RCP Average 52% 47%
Congress Approve Disapprove RCP Average 15% 76%
ACA Approve Disapprove October Kaiser 45% 45%

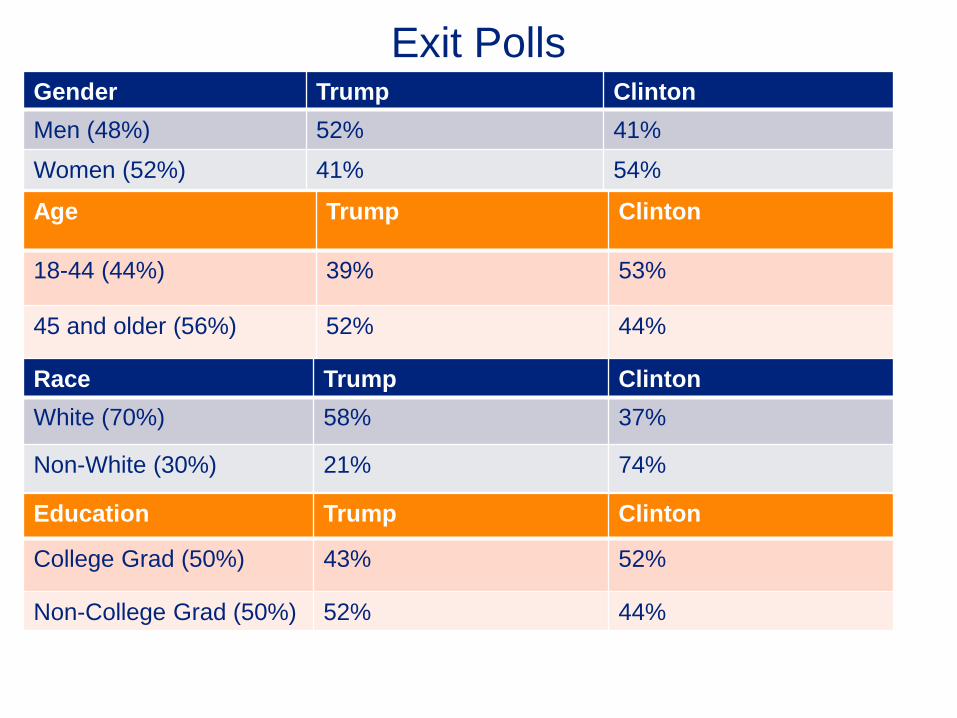
Exit Polls
Age Trump Clinton
18-44 (44%) 39% 53%
45 and older (56%) 52% 44%
Gender Trump Clinton Men (48%) 52% 41%
Women (52%) 41% 54%
Race Trump Clinton White (70%) 58% 37%
Non-White (30%) 21% 74%
Education Trump Clinton
College Grad (50%) 43% 52%
Non-College Grad (50%) 52% 44%

Current Congress Senate: 54 Republicans, 44 Democrats, 2 Independents (D)
House: 246 Republicans, 186 Democrats, 3 Vacancies (1/2)
Next Congress Senate: 52 Republicans, 46 Democrats, 2 Independents (D)
House: 239 Republicans, 194 Democrats, 2 TBD

Senate Results
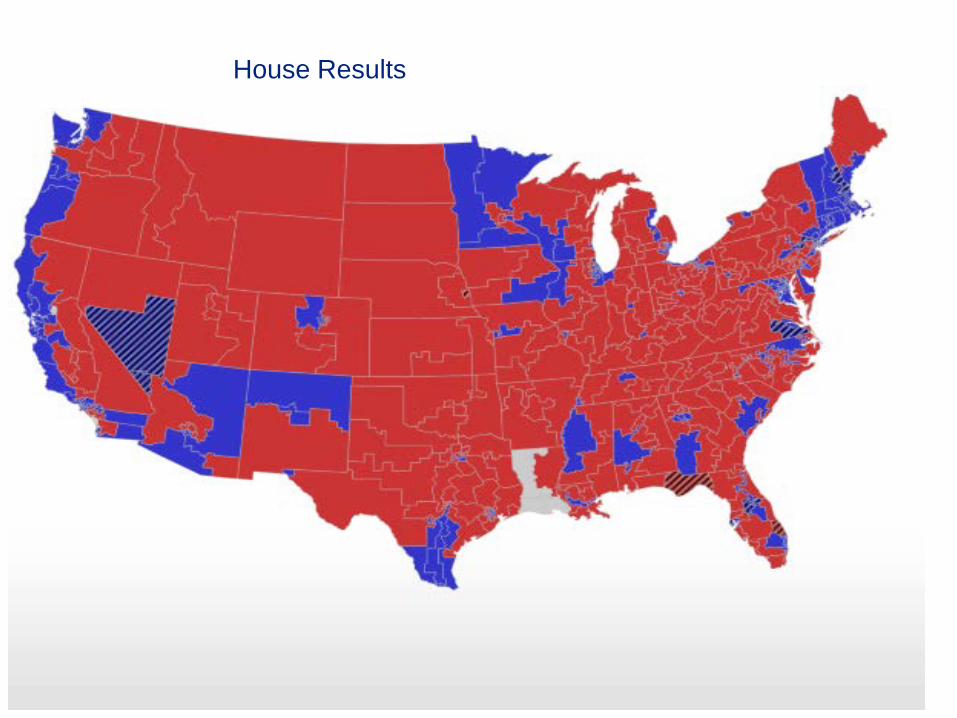
House Results

Races for Governor

NYS / NYP PPS UpdatePPS Project Advisory Committee
December 7, 2016
1
Post-Election Update: DSRIP is still here to stay.
Jason Helgerson (11/10/16):
“All – With the election results, many have raised questions regarding implications for DSRIP. We wanted to share the following points to help clarify some concerns.
– DSRIP is not part of the Affordable Care Act (ACA) and would not be affected by legislative attempts related to the ACA.
– DSRIP is part of a waiver amendment agreement with CMS, authorized through March 2020 and run by the state government.
– Health care system reform and Value Based Payment efforts will continue as these are industry drivers for improved quality and sustainability. Medicare has adopted VBP as part of their program policy and commercial payers are pursuing similar arrangements.
The tremendous efforts by the State and the PPSs to transform the system under DSRIP will continue. Please keep focused on the DSRIP goals and projects, and maintain the collaborative and positive work you and your staff have accomplished so far. Proceed with Fact-based Optimism.”
2

NYS DSRIP Timeline
End of 2016
DY2 Q3 (12/31/16)
DY2 Q2 Remediation
MY3 Q2 Performance
“DSRIP Midpoint”
3
We are here.

NYS DSRIP Timeline: Midpoint Assessment
The Mid-Point Assessment requirements are outlined in Section VI.d in Attachment I to the STCs of the waiver. The requirements indicate that at a minimum, the following elements will be assessed:
Compliance with the approved DSRIP project plan
Compliance with the required core components for projects
Non-duplication of Federal funds;
An analysis and summary of relevant data on performance on metrics and indicators to this point in time;
The benefit of the project to the Medicaid and uninsured population and to the health outcomes of all patients served by the project (examples include number of readmissions, potentially preventable admissions, or adverse events that will be prevented by the project);
An assessment of project governance including recommendations for how governance can be improved to ensure success. The composition of the performing provider system network from the start of the project until the midpoint will be reviewed.
The opportunity to continue to improve the project by applying any lessons learned or best practices that can increase the likelihood of the project advancing the three part aim; and
Assessment of current financial viability of all lead providers participating on the DSRIP project.
4

NYS DSRIP Timeline: Midpoint Assessment (2)
5
NYP PPS: Midpoint Assessment Results
Independent Assessor Identified Opportunities for Improvement:
1. Collaborator Engagement in Projects
2. Funds Flow to Collaborators
3. Investment in Cultural Competency / Health Literacy Efforts
4. Patient Engagement for Two Projects (HIV CoE, Palliative Care)
5. Project Requirement for One Project (ED Care Triage)
NYP PPS submitted response on 12/1/16 – identifying opportunities to
reflect PPS efforts that are not captured by standard quarterly
reporting.
6

7
Note: As part of a December 2015 waiver amendment request to the federal Centers for Medicare and Medicaid Services, New York is seeking to slightly modify these percentages.
Source: New York State Department of Health, Attachment I—NY DSRIP Program Funding and Mechanics Protocol, April 2014.
15%
45%
65%
85%
20%
25%
15%
15%
15%
80%
60%
40%
20%
DSRIP Year 1 DSRIP Year 2 DSRIP Year 3 DSRIP Year 4 DSRIP Year 5
Project progress milestones Pay-for-reporting Pay-for-performance
We are here
NYS DSRIP Timeline: Shift from P4R to P4P
NYP PPS: P4R Progress
Domain Details
Governance
Committees
• Continue to meet monthly/bimonthly to review and
approve NYS Organizational Milestones
Projects
• All projects on-track to meet DY2Q4 (March 2017) project
requirements
• Patient engagement missed once in two projects
Organizational
Requirements• All milestones achieved to-date*
8*Workforce Comp/Benefits Analysis submitted for CMS appeal

NYP PPS: Transition to P4P Focus
9
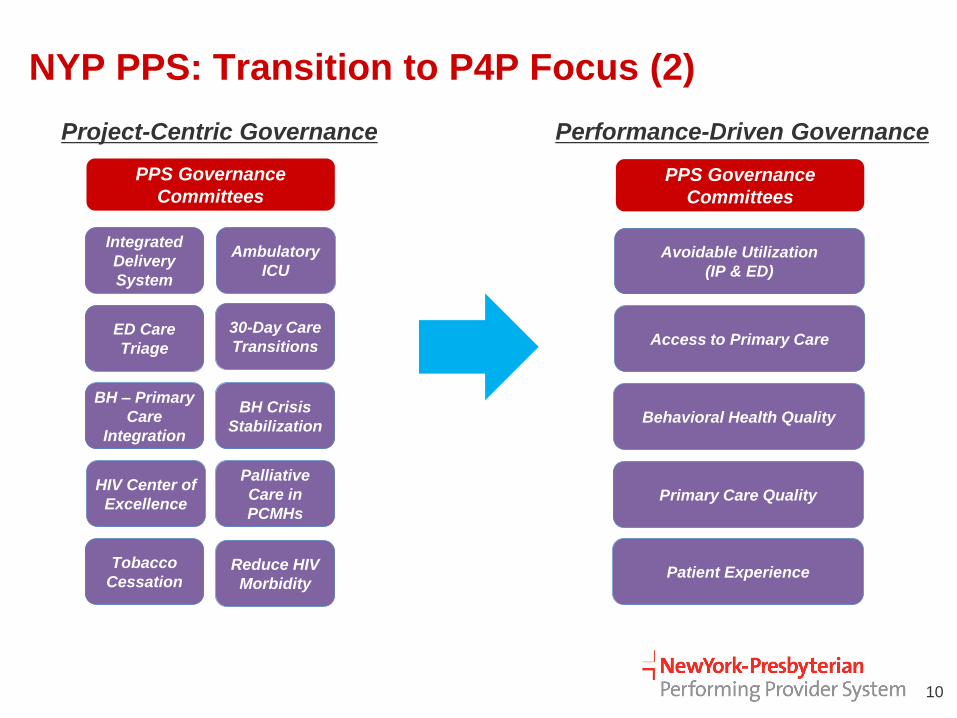
NYP PPS: Transition to P4P Focus (2)
10
Integrated
Delivery
System
Ambulatory
ICU
ED Care
Triage
30-Day Care
Transitions
BH – Primary
Care
Integration
BH Crisis
Stabilization
HIV Center of
Excellence
Palliative
Care in
PCMHs
Tobacco
CessationReduce HIV
Morbidity
PPS Governance
Committees
Project-Centric Governance Performance-Driven Governance
Avoidable Utilization
(IP & ED)
Access to Primary Care
Behavioral Health Quality
Primary Care Quality
PPS Governance
Committees
Patient Experience

NYP PPS: Transition to P4P Focus (3)
Anticipated Transition
PPS Governance Committees
focus on metrics / QI
opportunities
Distribution of performance
reports
Move beyond project-specific
reporting requirements (DY2 Q4)
Reorganize away from project
silos
Anticipated Challenges
Performance data
– 1+ year lag (directional)
– Not directly attributed to single
provider/organization
– Few data sources are identifiable /
actionable
QI achieved through population-
specific efforts vs. NYS reporting
/ messaging focused on projects
11
Immediate Focus: Assessing Quality
Improvement Opportunities

12


















