Drugs & lactation
29
Drugs&Lactation Prof Aboubakr Elnashar Benha University Hospital, Egypt Email: [email protected] Aboubakr Elnashar
-
Upload
aboubakr-mohamed-elnashar -
Category
Health & Medicine
-
view
317 -
download
8
description
Drugs and Lactation Aboubakr Elnashar
Transcript of Drugs & lactation

Drugs&Lactation
Prof Aboubakr Elnashar Benha University Hospital, Egypt Email: [email protected]
Aboubakr Elnashar

•Breast-feeding has many benefits.
•Potential harm to the nursing infant
from maternal drugs is a reason to discontinue
breast-feeding.
•Physicians receive little education about breast-
feeding and even less training on the effects of
maternal drugs on the nursing infant.
Aboubakr Elnashar

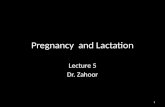
•The mammary tissue in the breast is composed
of clusters of milk-producing alveolar cells
surrounding a central lumen.
Aboubakr Elnashar

Aboubakr Elnashar

A ducts
B lobules
C dilated section of duct to hold milk
D nipple
E fat
F pectoralis major muscle
G chest wall/rib cage
Enlargement:
A normal duct cells
B basement membrane
C lumen (center of duct)
Aboubakr Elnashar

The effect of drugs on the nursing infant
depends on 1.Transfer of drug into Breast Milk
2.The amount of breast milk consumed by the
infant.
3. The pharmacologic activity of the drug:
absorption, distribution, metabolism and
elimination by the infant.
4. Condition of the infant: Greater precaution for infants
premature or
compromised or
in the first week of life than for older, healthy infants.
Aboubakr Elnashar

Transfer of dugs into Breast Milk
•Nearly all drugs transfer into breast milk to some
extent.
•Notable exceptions are heparin and insulin {too
large to cross biological membranes}.
•Drug transfer from maternal plasma to milk is,
with rare exceptions, by passive diffusion across
biological membranes.
Aboubakr Elnashar

• Factors affecting drug transfer
I. The maternal serum drug concentration.
Aboubakr Elnashar

II. Drugs:
protein binding,
lipid solubility,
molecular weight and
ionization
•Transfer is greatest
low protein binding
high lipid solubility.
Small molecular weight
weakly basic drugs
Aboubakr Elnashar

III. Milk composition
Milk at the end of a feed (hindmilk) contains
considerably more fat than foremilk and may
concentrate fat-soluble drugs.
Aboubakr Elnashar

IV. Age of infant:
•In the early postpartum period, large gaps
between the mammary alveolar cells allow many
dugs to pass. These gaps close by the 2nd week
of lactation.
•Premature babies & infants less than 1 month
have a different capacity to absorb and excrete
drugs than older infants.
Thus, extra caution is needed for these infants.
Aboubakr Elnashar

Calculation of infant exposure to drugs
The infant dose (mg/kg)
I. D infant (mg/kg/day)= C maternal (mg/L) x
M/PAUC x V infant (L/kg/day) •Cmaternal= maternal plasma concentration • M/PAUC ratio = milk to plasma concentration ratio area under curve. •Vinfant= volume of milk ingested
II. As a percentage of the maternal dose (mg/kg).
The volume of milk ingested by infants is
commonly estimated as 0.15 L/kg/day. An arbitrary cut-off of 10% has been selected as a
guide to the safe use of drugs during lactation.
Aboubakr Elnashar

WHO classification of drugs during
breastfeeding (2002)
1. Compatible with breastfeeding
2. Compatible with breastfeeding {occasional mild side
effects} Monitor infant for side effects
3. Avoid if possible. {significant side effects} Monitor
infant for side-effects
4. Avoid if possible. {May inhibit lactation}. Monitor for
amount of milk
5. Contraindicated {dangerous side effects}
Aboubakr Elnashar

WHO Classification DRUGS during
BREASTFEEDING (2002)
1. Compatible with breastfeeding
There are no known or theoretical
contraindications for their use, and it is
considered safe for the mother to take the drug
and continue to breastfeed.
Aboubakr Elnashar

2. Compatible with breastfeeding {Occasional mild side-effects} Monitor infant for side-effects
•If side-effects:
stop the drug, and
find an alternative.
If the mother cannot stop the drug, she may need
to stop breastfeeding and feed her baby artificially
until her treatment is completed.
Aboubakr Elnashar

3. Avoid if possible {significant side effects}
Monitor infant for side-effect
Aboubakr Elnashar

Psychotropic drugs,
anti-anxiety,
antidepressant, and
antipsychotic ,
when given to nursing mothers for long periods
could alter short-term and long-term central
nervous system function.
Aboubakr Elnashar

4. Avoid if possible {May inhibit lactation}
However, if a mother has to take one of these drugs for a short period, she does not need to give artificial milk to her baby. She can off set the possible decrease in milk production by encouraging her baby to suckle more frequently. Estrogen COC Ergometrin Thiazides
Aboubakr Elnashar

5. Contraindicated {Dangerous side-effects}.
If they are essential:
stop breast feeding until treatment is completed.
If treatment is prolonged, she may need to stop
breastfeeding altogether.
There are very few drugs in this category apart
from anticancer drugs and radioactive
substances.
Aboubakr Elnashar

Aboubakr Elnashar

Aboubakr Elnashar

lithium (infant dose as high as 80% of the weight-
adjusted maternal dose) and
amiodarone (infant dose up to 50%) should be
avoided due to high infant exposure and potential
for significant toxicity.
For drugs with greater inherent toxicity such as
cytotoxic agents,
ergotamine,
gold salts,
immunosuppressives and
isotretinoin, the cut-off of 10% is too high and
breastfeeding is contraindicated.
Aboubakr Elnashar

AMERICAN
ACADEMY
OF
PEDIATRICS
(2001)
Aboubakr Elnashar

Before prescribing drugs to lactating women
1. Is drug really necessary? If drugs are required,
consultation between the pediatrician and the
mother’s physician can be most useful in
determining what options to choose.
Aboubakr Elnashar

2. The safest drug should be chosen e.g. acetaminophen rather than aspirin for analgesia. 3. If there is a possibility that a drug may present
a risk to the infant, consideration should be given
to measurement of blood concentrations in the
nursing infant.
4. Drug exposure to the nursing infant may be
minimized
Aboubakr Elnashar

Minimizing Potential Risk to Nursing Infants
from Maternal Medications
General considerations
•Use topical therapy when possible.
•Drugs that are safe for the nursing infant’s age
are generally safe for the breast-feeding mother.
•Drugs that are safe in pregnancy are not always
safe in breast-feeding mothers {nursing infant must independently metabolize and excrete the medication}.
Aboubakr Elnashar

Medication selection
•Choose medications with the shortest half-life
and highest protein-binding ability.
•Choose medications that are well-studied in
infants.
•Choose medications with the poorest oral
absorption.
•Choose medications with the lowest lipid
solubility.
Aboubakr Elnashar

Medication dosing
•Administer single daily-dose drugs just before
the longest sleep interval for the infant, usually
after the bed-time feeding.
•Breast-feed infant immediately before medication
dose when multiple daily doses are needed.
Aboubakr Elnashar

Aboubakr Elnashar