Drug Targets 2013(1)
35
MD214/PO202: Drug Targets
description
Drugs
Transcript of Drug Targets 2013(1)

MD214/PO202: Drug Targets
Overview
• The nature of drug targets • How drugs interact with their targets
(specificity and selectivity) • Law of mass action and occupancy derivations • The concepts of agonists and antagonists
“Receptive substances”
• Paul Ehrlich: Best known for his work on immunity for which he was awarded the Nobel Prize for Medicine/Physiology in 1908.
• Ehrlich developed the concept of “Receptive substances” to which chemical substances bind to produce effects
• Binding involves weak bonds

Drug-target interactions
• Receptors • Ion channels • Enzymes • Transporters
• All proteins in nature

Protein structure
• Revise/update your knowledge of the four major levels of protein structure (p2-4 of Golan)
• Primary structure • Secondary structure • Tertiary structure • Quaternary structure
• Drug binding sites
Receptors as targets
• James Black: his invention of propranolol, the beta receptor antagonist is considered to be one of the most important contributions to clinical medicine and pharmacology of the 20th century.
• He later developed H2 receptor antagonists as antiulcer compounds.
• In 1988, he was awarded the Nobel Prize in Medicine.
More about receptors
• Receptors are large proteins • Most common drug target. Specific drug
binding site (analogous to the active site of an enzyme) that acts as a target for a particular group of related drugs
• Important means of communication, linked to other molecules within the cell
• Trigger a response in that cell • Found in: Cell membrane, Cytosol, Nucleus
Endogenous ligands
• The body’s own ‘drugs’ • Drugs bind to receptors in the same way that
endogenous ligands bind to receptors • For example, adrenaline is the endogenous
ligand for beta receptors. Isoprenaline (isoproterenol) is a synthetic drug that binds to this same receptor.

Enzymes as targets
• John Vane: He found that aspirin inhibits the action of prostaglandins — substances that are liberated when tissues are perturbed producing inflammation, pain and fever in the body.
• He also found that low dose aspirin stops the production in platelets of thromboxane, which causes platelets to stick together to plug any ruptures in blood vessels.

Specificity of drugs for receptors
• “Lock and key” • Receptors are specific for a particular drug • However, some drugs bind to more than one
receptor type, and thus are termed “non-selective”, e.g. Imipramine, a tricyclic antidepressant
Receptor Receptor Drug /Drug +
Law of Mass Action
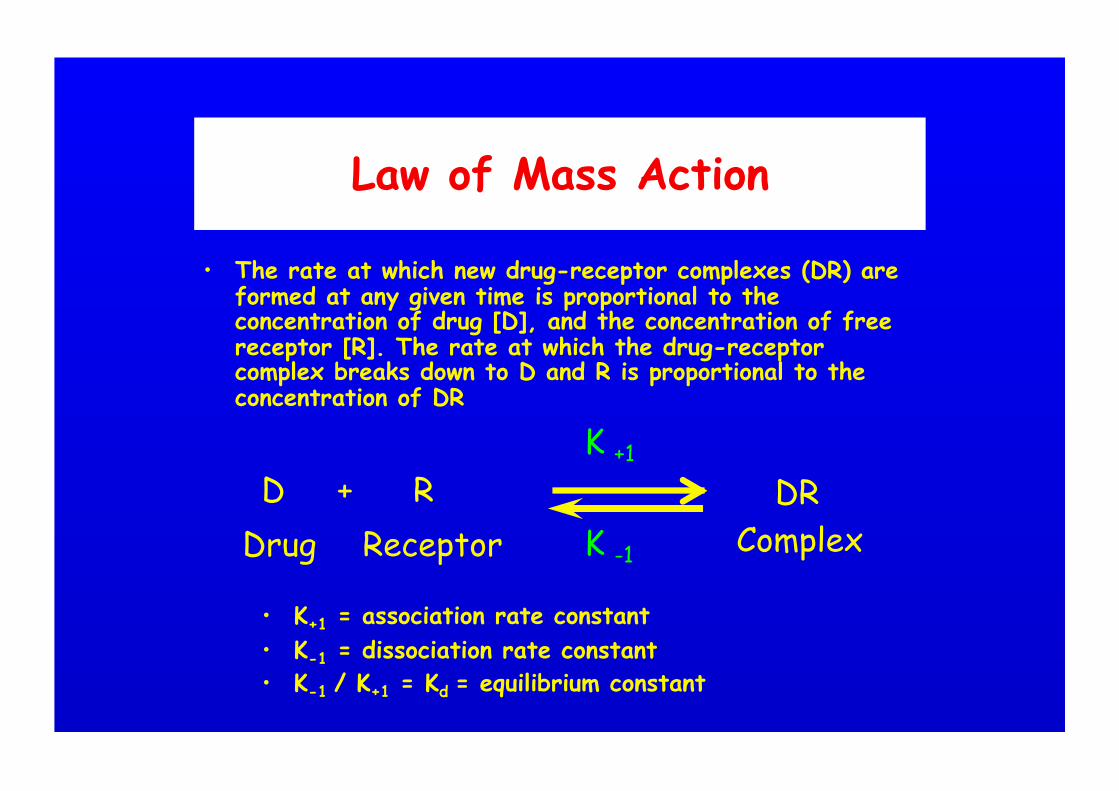
• The rate at which new drug-receptor complexes (DR) are formed at any given time is proportional to the concentration of drug [D], and the concentration of free receptor [R]. The rate at which the drug-receptor complex breaks down to D and R is proportional to the concentration of DR
Complex + DR D
Drug R
Receptor K -1
K +1
• K+1 = association rate constant • K-1 = dissociation rate constant • K-1 / K+1 = Kd = equilibrium constant
Affinity
• Tendency of a drug to bind to a receptor • Measured by Kd • This measurement enables us to compare the
affinities of drugs, i.e. How avidly they bind to their target receptor
© 2005 Elsevier
Nature of binding
• Drugs usually bind in a reversible fashion (as depicted in the law of mass action equation)
• Make sure to revise/update your knowledge of the types of bonds (summarised on p3 of Golan), listed below in order of binding strength (weakest to strongest)
• Van der Waals forces • Hydrogen bonds • Ionic interactions • Covalent bonds
Example of Imatinib
• Imatinib is a highly selective inhibitor of the BCR-Abl tyrosine kinase fusion protein (see p5 of Golan)
• Imatinib interacts with specific amino acid residues that possess hydrophobic side chains via van der Waals forces and hydrogen bonding
• The binding causes a conformational change in the active site of the enzyme, inhibiting its catalytic activity
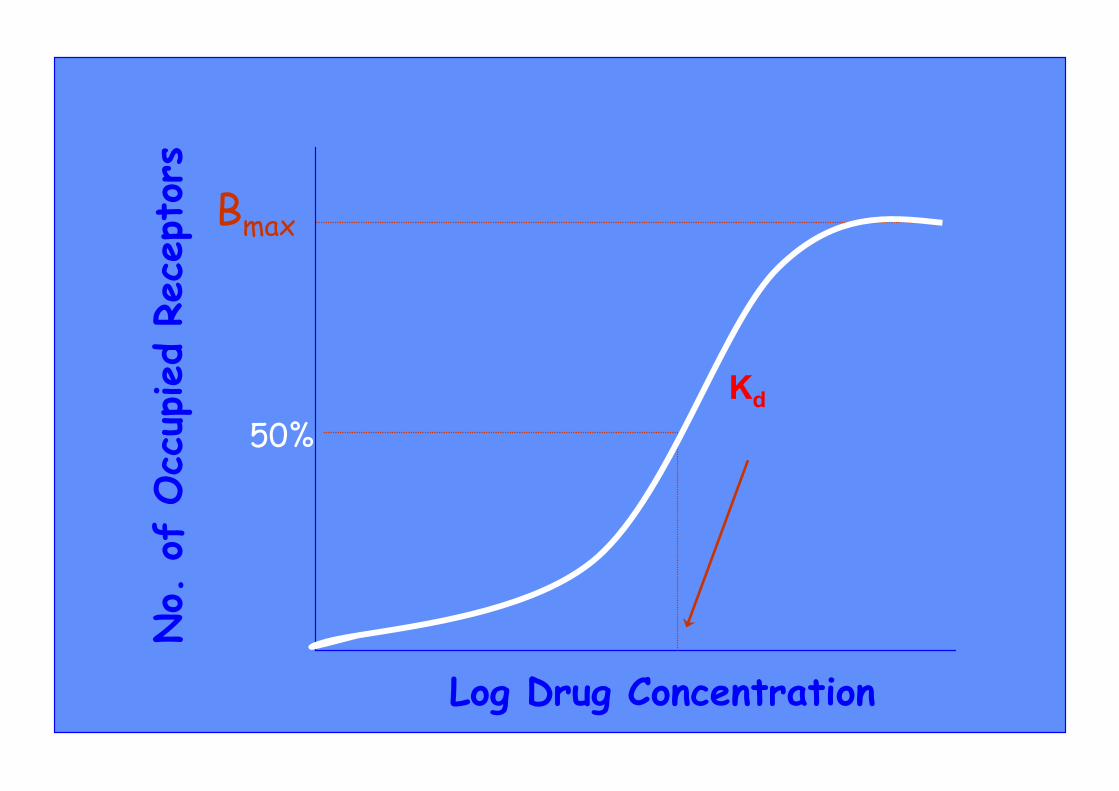
Drug-receptor occupancy curves
• As the concentration of drug in the vicinity of its receptor is increased, then the proportion of receptors occupied increases
• As there are a finite number of receptors, a concentration point will be reached when all of these receptors are occupied
• A drug-receptor occupancy curve can be graphically depicted and certain parameters can be derived
• The following graphs depict such a curve, the second using a log scale to create a sigmoid (s-shaped) curve
No.
of
Occ
upied
Rece
ptor
s
Log Drug Concentration
Bmax
50% Kd

No.
of
Occ
upied
Rece
ptor
s
Log Drug Concentration
Bmax
50%
Bmax indicates the density of receptors at maximum binding
Kd (equilibrium constant) = concentration of drug required to occupy 50% of receptors
Spare receptors • Usually a maximum response is seen at less
than 100% receptor occupancy • Unoccupied receptors termed “spare” or
“reserve” • This may be due: 1. Receptor remaining activated after the
agonist uncouples, enabling the same agonist to activate several receptors
2. Intracellular cascades of signals generated by receptor activation, i.e. amplification of signal downstream

Processing of signals
• Involves the deployment of second messengers produced intracellularly following drug-receptor binding
• This has the potential for the signal to be amplified through a cascade of biochemical activations
• One example is the production of the secondary messenger cyclic AMP (cAMP) by activation of the enzyme adenylyl cyclase, which can activate several protein kinases
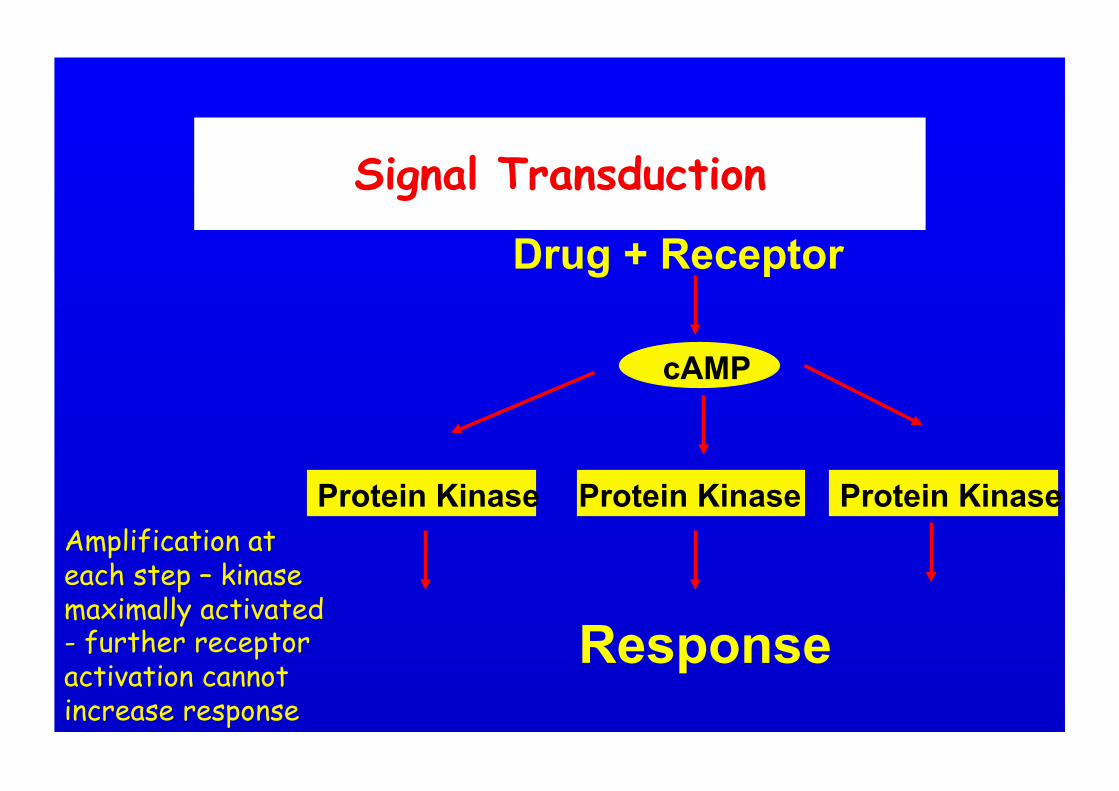
Drug + Receptor
Response
cAMP
Protein Kinase Protein Kinase Protein Kinase Amplification at each step – kinase maximally activated - further receptor activation cannot increase response
Signal Transduction
Cellular regulation of drug-receptor interactions (p10 of Golan)
• Drug-induced interaction often has a lasting impact on receptor’s subsequent responsivesness
• Tachyphylaxis: diminishing effects of the drug over time due to desensitization (homologous, where effects of one type of receptor are diminished or heterologous where effects at two or more receptors are diminished)
• Inactivation: loss of ability of receptor to respond to stimulation by ligand
• Refractory state: period where receptors are unresponsive to further activation
• Down-regulation: prolonged receptor activation induces the cell to endocytose and sequester receptors in endocytic vesicles
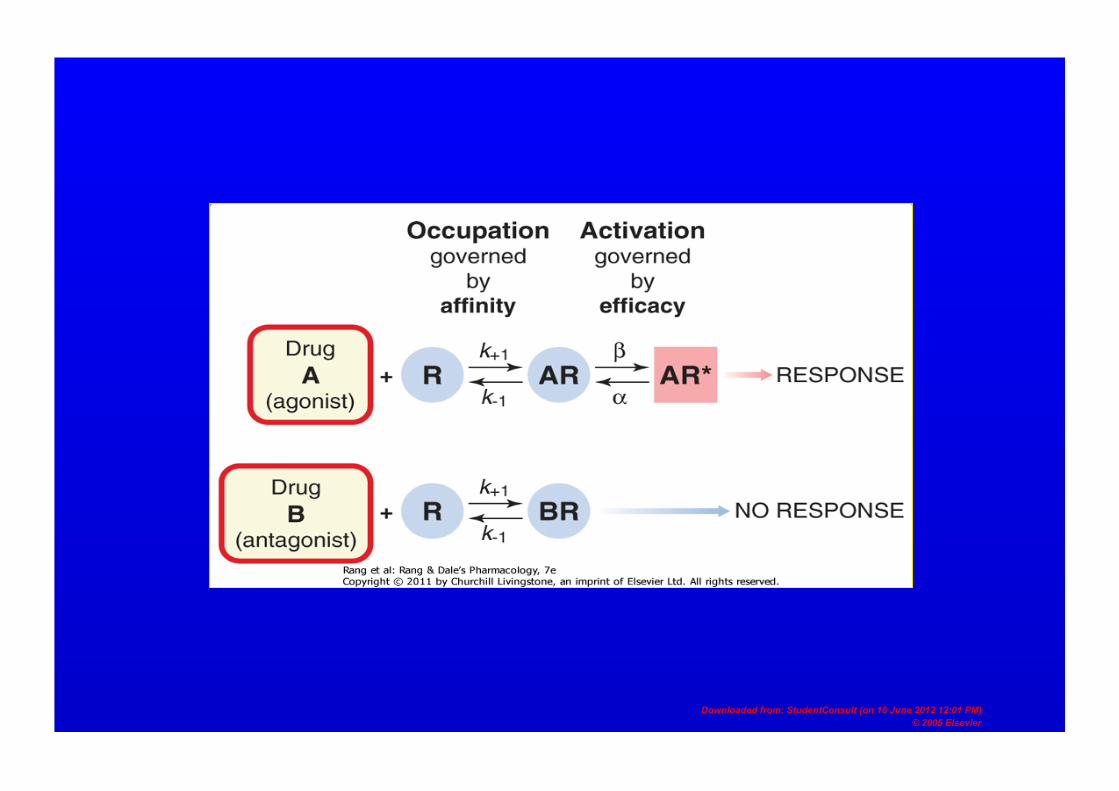
Types of interaction
• Receptors are modelled as being in an active or inactive state
• Agonist: favours the active receptor confirmation, binds to a receptor and causes an effect
• Antagonist: a drug that prevents the agonist-induced activation of the receptor
• Partial agonists and inverse agonists do not fit neatly into this simple definition of agonist and antagonist
Downloaded from: StudentConsult (on 18 June 2012 12:01 PM) © 2005 Elsevier
Downloaded from: StudentConsult (on 18 June 2012 12:01 PM) © 2005 Elsevier
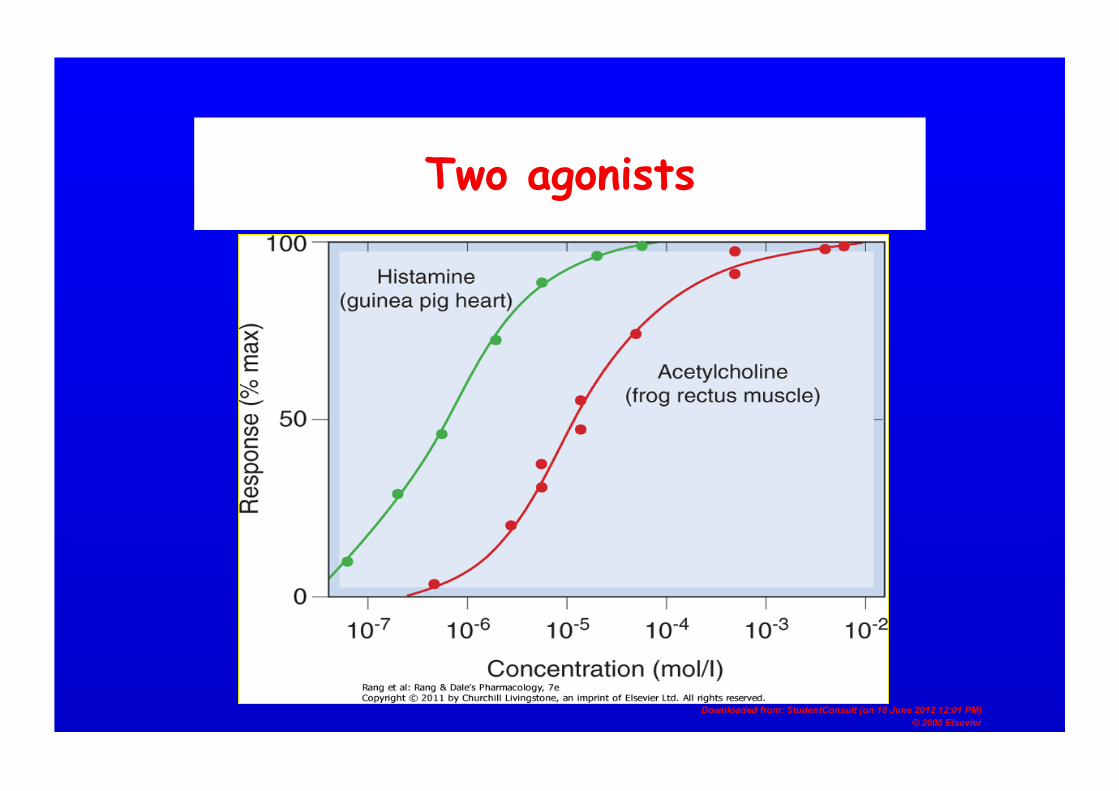
Two agonists
Antagonists
• NB Classification of antagonists can vary between texts
• We will use the classification of Rang and Dale (2011), which divides into 2 types:
• Competitive antagonists • Non-competitive antagonists
Competitive Antagonists
• This type of antagonism is at the binding site of the endogenous ligand
• Reversible: Most common and most important type of antagonism
• Irreversible: Covalent bond formation
Downloaded from: StudentConsult (on 18 June 2012 12:01 PM) © 2005 Elsevier
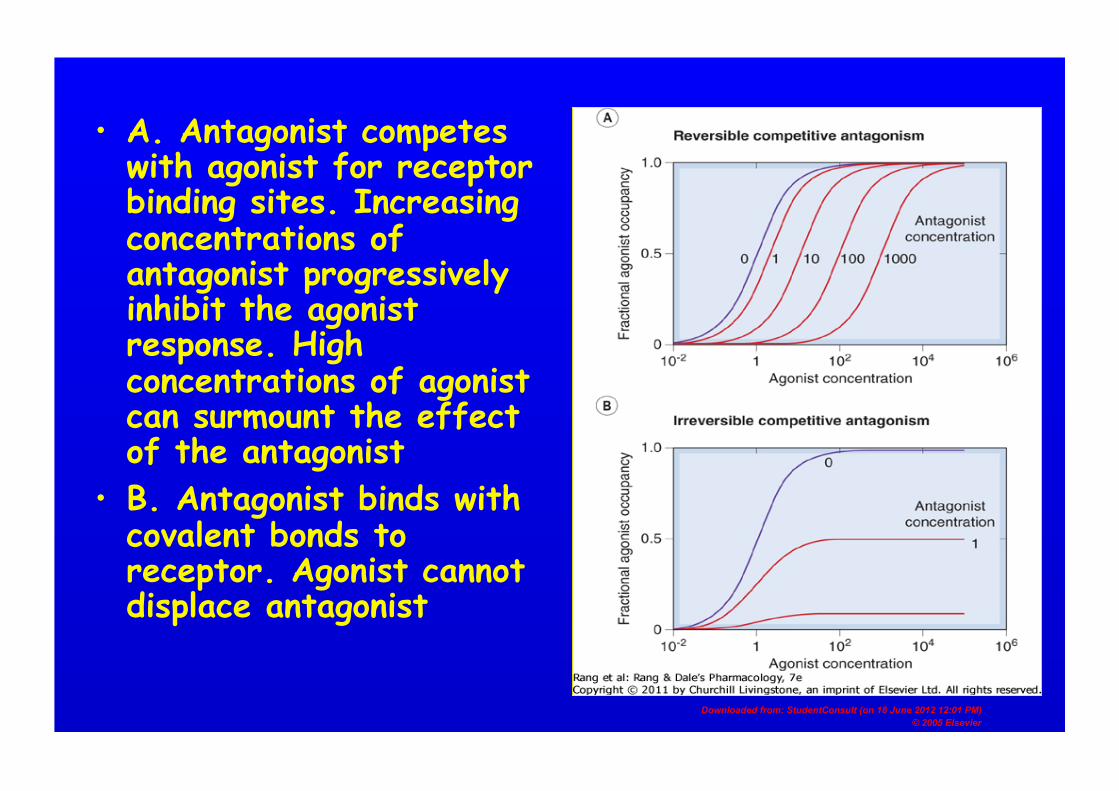
• A. Antagonist competes with agonist for receptor binding sites. Increasing concentrations of antagonist progressively inhibit the agonist response. High concentrations of agonist can surmount the effect of the antagonist
• B. Antagonist binds with covalent bonds to receptor. Agonist cannot displace antagonist

Non-competitive antagonism
• Antagonist blocks at some point other than the receptor binding site
• May bind to another site on the receptor (allosteric inhibition)
• May block the signal transduction process

Other types of agonists
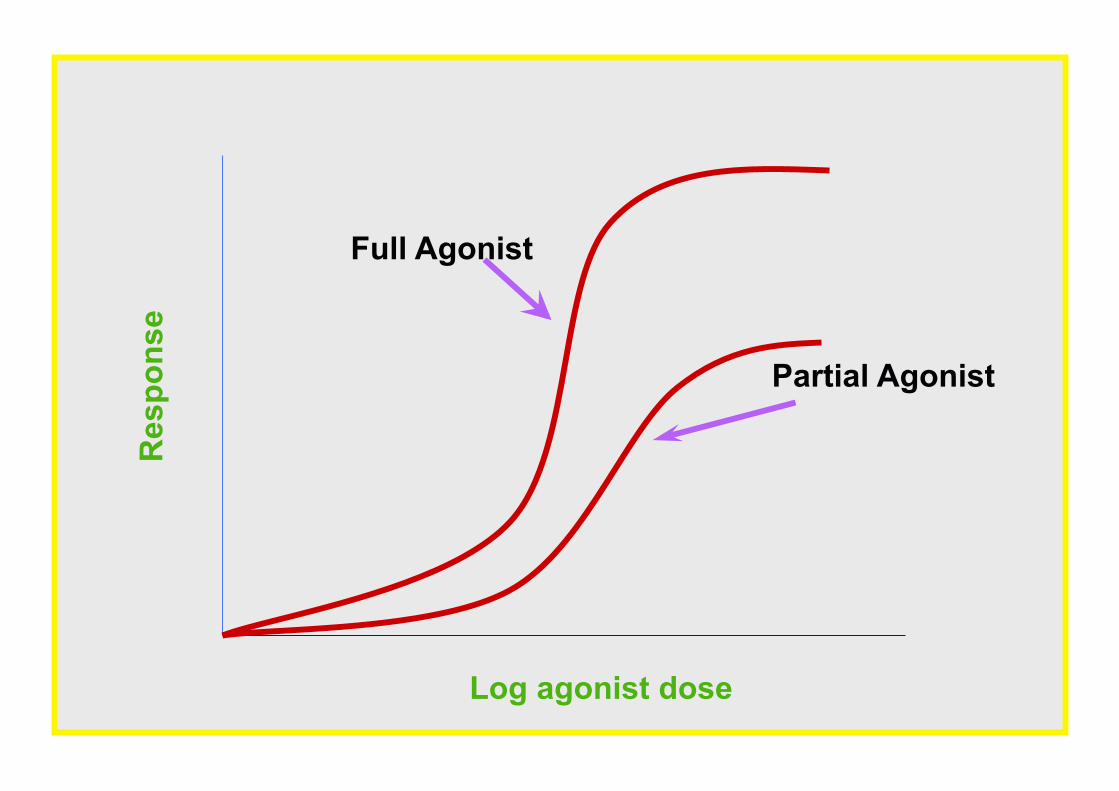
Partial Agonists
• Produce a lower response than full agonists • Reduced response not due to decreased binding
affinity, but decreased efficacy • As partial agonists bind to same site, they can
reduce the response produced by a full agonist, thus can act as competitive antagonist
• An example is aripiprazole, a partial agonist of dopamine receptors used in the treatment of schizophrenia
Res
pons
e
Log agonist dose
Full Agonist
Partial Agonist
Downloaded from: StudentConsult (on 18 June 2012 12:01 PM) © 2005 Elsevier
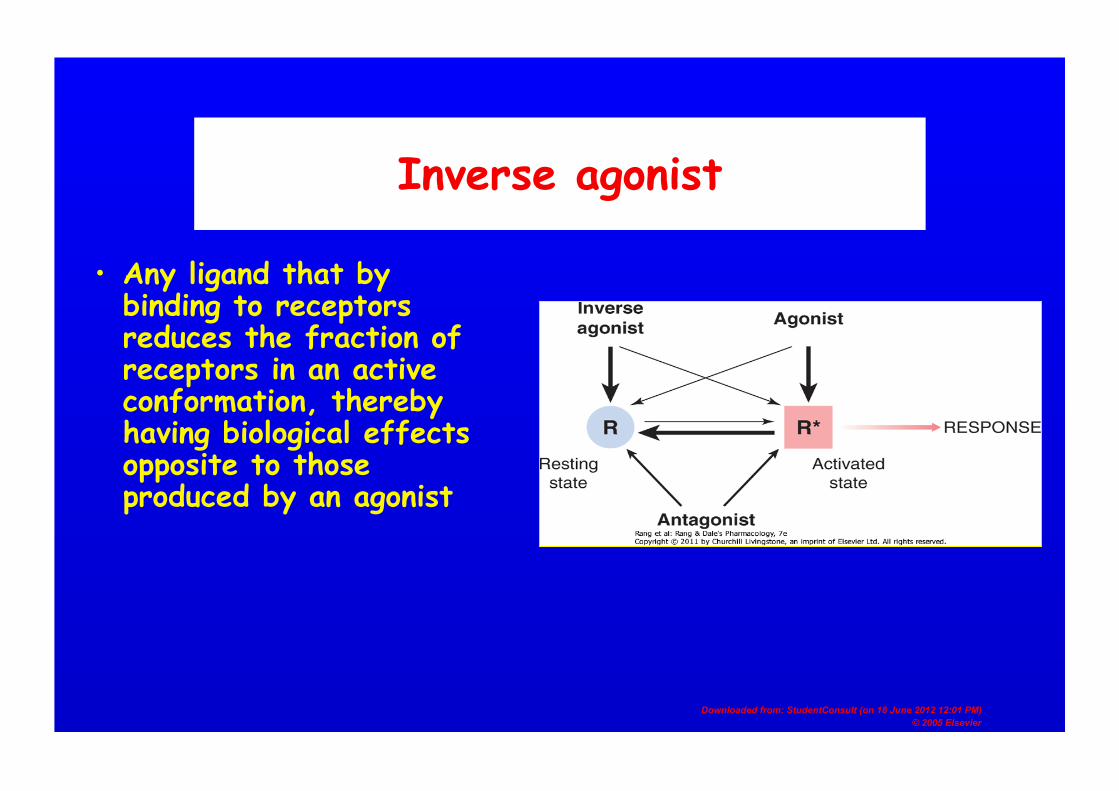
Inverse agonist
• Any ligand that by binding to receptors reduces the fraction of receptors in an active conformation, thereby having biological effects opposite to those produced by an agonist
Downloaded from: StudentConsult (on 18 June 2012 12:01 PM) © 2005 Elsevier
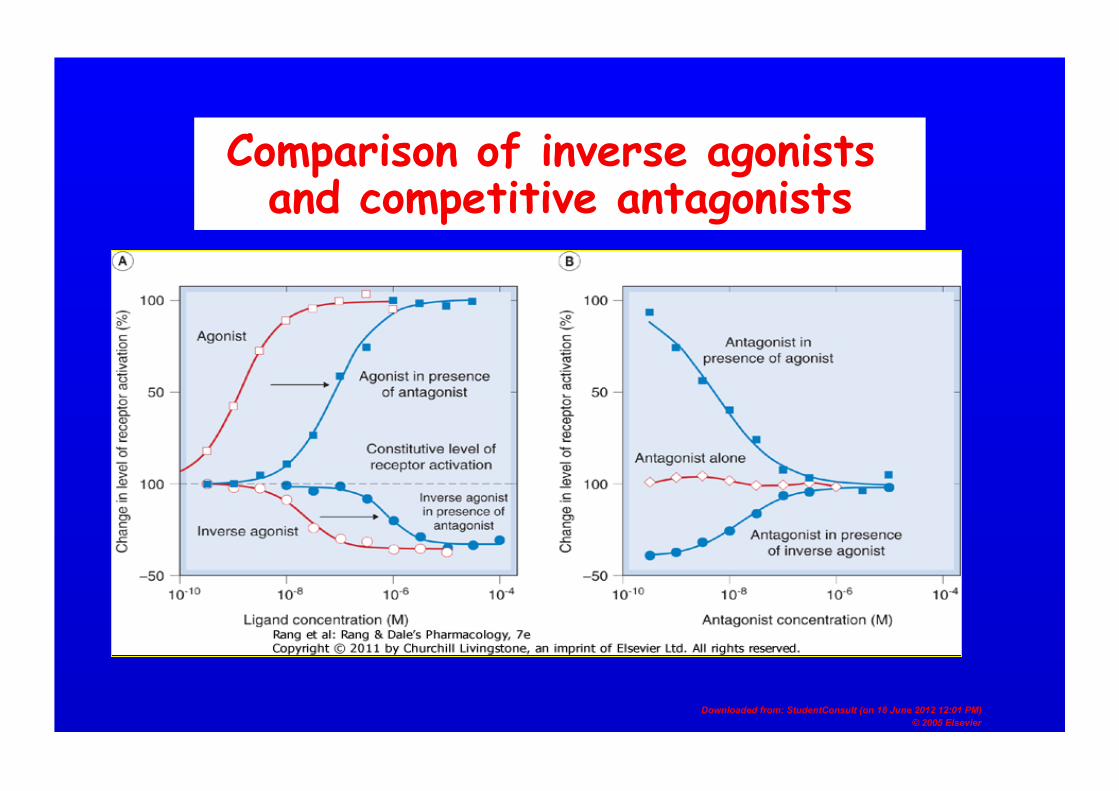
Comparison of inverse agonists and competitive antagonists
Nonreceptor antagonism
• Chemical antagonism: inactivates agonist by forming a complex with it, e.g. Protamine is a basic protein that binds to heparin forming an inactive complex
• Physiological antagonism: activates or blocks a receptor that mediates a response physiologically opposite to that of the receptor for an agonist, e.g. Beta blockers counteract the tachycardia associated with excessive thyroid hormone stimulation in hyperthyroidism
Summary
• Most drug targets are protein in nature • Drugs interact in a specific way with their
targets, typically weak, reversible associations • The receptor is the most commonly encountered
drug target • Receptor occupancy can be graphically depicted
and parameters derived from it • Receptor activation produces intracellular events
and can have a lasting impact on receptors • Drugs can interact with receptors as either
agonists or antagonists • There are different types of agonists and
antagonists