Drug Resistant TB PMDT Status and...
30
Drug Resistant TB PMDT Status and Challenges DR ROHIT SARIN MD, DTCD, FNCCP DIRECTOR NATIONAL INSTITUTE OF TB & RESPIRATORY DISEASES SRI AUROBINDO MARG : NEW DELHI
Transcript of Drug Resistant TB PMDT Status and...

Drug Resistant TB PMDT Status and Challenges
DR ROHIT SARIN MD, DTCD, FNCCP
DIRECTOR
NATIONAL INSTITUTE OF TB & RESPIRATORY DISEASES
SRI AUROBINDO MARG : NEW DELHI

Estimated number of MDR-TB Cases, 2012*
~ 2/3 third of all cases are in 4 countries Russian Federation
46,000 (15% of global MDR burden)
India 64,000
(22% of global MDR burden)
China 59,000
(20% of global MDR burden)
* among notified TB cases
South Africa 8,100
(3% of global MDR burden)
3.6% new cases 20.2% previously
treated cases

India v/s top 12 high MDR burden countries
26%
5%
190%
30%
87%
102%

Countries that had reported at least one XDR-TB case -
2012
92 countries
9.6% MDR TB cases have XDR TB
16.5%MDR-TB cases with additional resistance to
fluoroquinolones

• India has world’s highest MDR-TB burden
• 64,000 emerging annually among notified PTB cases
•Sub-national drug resistance surveys (2005-09)
• 2.4% MDR in new, 15% MDR in previously treated cases
• 21-24% Ofx resistance, 4-7% XDR in MDR isolates
•National drug resistance survey underway
Burden of DR TB- Indian Scenario
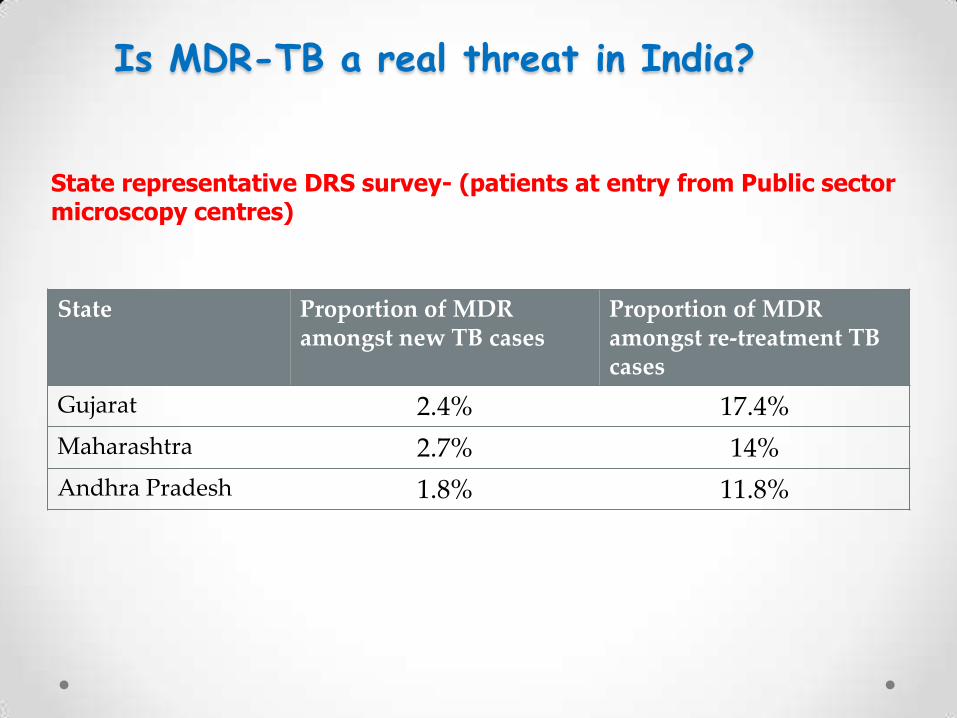
Is MDR-TB a real threat in India?
State Proportion of MDR amongst new TB cases
Proportion of MDR amongst re-treatment TB cases
Gujarat 2.4% 17.4%
Maharashtra 2.7% 14%
Andhra Pradesh 1.8% 11.8%
State representative DRS survey- (patients at entry from Public sector microscopy centres)

Is XDR TB a real threat in India?
High XDR / pre-XDR levels out of XDR suspects undergoing Second-line Drug Susceptibility Testing at NRLs
Source: National TB Institute, Bangalore

The case of Mumbai and the
“TDR-TB outbreak” – Jan 2012
Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C. Totally drug-resistant tuberculosis in India. Clin Infect Dis. 2012 Feb 15;54(4):579–81.
March 2012 – WHO and CTD took a stand:
• Such cases pose a formidable challenge to clinicians
and public health authorities
• No reliable definition beyond XDR-TB
• Improvements in the accuracy of drug susceptibility
testing to certain drugs
• Release of innovative new drugs will, however,
change this position in future.
• India turned this crisis into opportunities for
improvements in Mumbai and country wide

RNTCP PMDT Vision
Plan of PMDT service expansion
By 2012-13:
o Complete geographical coverage for PMDT services (achieved)
o DST for all smear-positive re-treatment TB cases at diagnosis (597
districts achieved)
By 2015:
o + DST for all smear negative TB (re-treatment) cases & any HIV TB case
registered under RNTCP (expected by March 2014)
By 2017:
o 120 C-DST labs being established and strengthened
o Xpert-MTB-Rif in 950 sites at districts and medical colleges across the
country
o Treat at least 40,000 MDR cases annually by 2017 (120 DR TB Centers)
o Treat ~ 160,000 MDR-TB & ~4,100 XDR-TB cases over next 5 yrs (2012-17)

District wise coverage of RNTCP
PMDT services under various
MDR-TB suspect criteria by districts
–Feb 2014
CRITERIA A 107
CRITERIA B 151
CRITERIA C 446

PMDT Diagnostic Services
Status & Update

Technology used to diagnose MDR-TB by districts –Feb
2014
LPA 428
CBNAAT 208

A&N Islands
Arunachal Pradesh
Chandigarh
D&N Haveli
Daman & Diu
Goa
Karnataka
Lakshadweep
Meghalaya
Mizoram
Nagaland
Pondicherry
Sikkim
Tripura
Haryana
Delhi
Gujarat
Andhra Pradesh
Assam
Manipur
Punjab
Kerala
West Bengal
Jammu & Kashmir
Himachal Pradesh
Rajasthan
Maharashtra
Tamil Nadu
Orissa
Madhya Pradesh
Chhatisgarh
Uttar Pradesh
Uttaranchal
Jharkhand
Bihar
TRC
HARYANANDTC
AIIMS-2
RNTCP Culture & DST Labs Network
(January, 2014)
LRS
NTI
JALMA
Med Col / NGO / Private Labs (Certified)
IRL (Certified )
IRL (Under Process)
Med Col / NGO / Private Labs (Under Process)
National Reference Labs
Gurgaon
By Technology - Solid Culture: 37 - LPA: 43 - Liquid Culture:14 - CB-NAAT : 80
C-DST Labs - 54 SLDST - 6 (3 NRLs and 2 IRL, 1-NGO)
CB-NAAT Sites

RNTCP Policy on CB-NAAT
• Use of CB-NAAT endorsed as a rapid molecular diagnostic tool
in following programmatic situations:
o For Diagnosis of Rif Resistance – MDR TB Suspects (A,B,C)
o For MTB positive results –
• Treat as per RNTCP guidelines
o For Rif Resistance results
• Re-treatment cases – Treat with MDR TB Regimen
• New cases – Re-confirm with LPA (LC/Solid in S-ve cases) and Treat
with MDR TB Regimen after confirming Rif Resistance
o For CB NAAT results from private sector
• For TB (acceptable if QA – Re-calibration of machine done annually)
• For R resistant results in new cases - re-confirm with
o LPA in S+ve cases or
o Liquid/Solid C-DST in S-ve Cases

RNTCP TB Xpert Project
supported by WHO, STOP TB Partnership,
UNITAID & USAID
• Under this project, 40 CB-NAAT machines and cartridges
are provided to the country to scale-up rapid molecular
diagnosis of TB and Rif resistance (MDR-TB)
• Innovate to engage private sector through public-private
mix (PPM) initiatives to improve access to rapid testing of
patients who attend both public and private sector

A&N Islands
Arunachal Pradesh
Chandigarh
D&N Haveli
Daman & Diu
Goa
Karnataka
Lakshadweep
Meghalaya
Mizoram
Nagaland
Pondicherry
Sikkim
Tripura
Haryana
Delhi
Gujarat
Andhra Pradesh
Assam
Manipur
Punjab
Kerala
West Bengal
Jammu & Kashmir
Himachal Pradesh
Rajasthan
Maharashtra
Tamil Nadu
Orissa
Madhya Pradesh
Chhatisgarh
Uttar Pradesh
Uttaranchal
Jharkhand
Bihar
TB Xpert Project Sites
X – Decentralized DST
P – PPM X
X
P
X
X
X
X
X
P
P
P
P
P
P
P
P
P
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X X
X
X
X
X
• GoI - place 10 urban site machines in Govt. institutes
• Advocacy to have PPM • All 40 sites innovate for PPM
models

TBXpert Project – Facility Reporting Sheet
All 40 sites to report on…
A. Number of patients referred from Private providers
B. Of A, Number of new and relapse cases detected with
MTB positive and Rif sensitive / indeterminate
C. Of A, Number of Rif resistant cases detected
D. Number of new cases with Rif Resistance sent to RNTCP
certified lab for re-confirmation
E. Of D, number re-confirmed

Second Line DST – Scale up Plan
• Existing SLDST – 7 Labs
• SL DST Proficiency Testing to be completed o In the 37 planned labs
• By 2Q 2014 –7 Labs JALMA Agra, IRLs -Hyderabad, Nagpur, Jaipur,
Delhi, Ajmer and JJ Mumbai )
• By 2014 – 13, IRLs-Pune, Bangalore, Cuttack, Puducherry, Karnal,
Chennai, Guwahati, Kolkata, Indore , Lucknow, PGI Chandigarh, GMC
Jamnagar, AIIMS New Delhi
• By 2015 – 16 IRL- Patiala, Agra, Raipur, Ranchi, Indore, Patna, GMC
Silliguri, RMRC Bhubaneswar, BMHRC-Bhopal, GMC-Vishakhapatnam,
BHU-Varanasi, KIMS- Hubli, Bhagalpur, Madurai, Raichur, Jodhpur
o Extended to private labs already certified by RNTCP for FLD

Priorities for lab strengthening
• Optimally utilize all existing technology for
diagnosis (LPA and CB-NAAT )and follow-up culture
(Solid and Liquid)
• Expedite the development and proficiency testing
for liquid culture
• Rapid Implementation of NIKSHAY PMDT module at
all laboratories

Innovative PPM initiatives to increase access
• Initiative for Promoting Affordable, Quality TB Tests (IPAQT) is a consortium of 50 private diagnostic laboratories
• Established agreements with Cepheid Inc, Hain LifeScience and Becton Dickenson to allow access to concessional prices for Xpert MTB/RIF, first-line line probe assays, and
liquid culture in the private sector
• Participating laboratories need to be accredited to assure quality; they must report confirmed cases to RNTCP; they must adhere to a ceiling price when charging patients
• Laboratories participating in IPAQT have approximately 3000 franchisee laboratories and over 10 000 specimen collection centres across India, thus increasing access to rapid, accurate and affordable diagnostics for patients seeking care in the country’s extensive private sector

Diagnostic Challenges & Solutions Deployed
Challenges
• Access to rapid molecular DST limited due to weak case finding systems and sample transport systems
• Setting up of Liquid Culture Labs – Infrastructure upgrades to BSL III & HR • Foreseeable follow up capacity crisis in most of the states on shift to Criteria C with rapid molecular tests
• Limited access to Second Line DST due to lack of systems • Lack of clarity on RNTCP policy for CB-NAAT and R&R systems
Solutions
• Streamlining systems and training to improve suspect identification, prompt sample collection & transport systems from PHIs/DMCs
• State to take the ownership • Enhance coordination to fast-track BSL III & HRD for LC labs • FU capacity enhancement through — 1 sample per follow up culture policy — Fast track application of potential labs
to reach proficiency stage with NRLs — Budget for C-DST Schemes - private
labs
• State to expedite SLD PT • Clear policy on CB-NAAT, Lab SOP & QA updated with CB-NAAT indicators

PMDT Treatment Services
Status & Challenges

Y2007 Y2008 Y2009 Y2010 Y2011 Y2012 Y2013
Sum of MDRTB cases initiated on Rx 62 190 1174 2182 3369 14146 20765
Sum of MDRTB Suspects 309 1511 8144 11001 17696 105706 181021
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
0
5000
10000
15000
20000
25000
DRTB Case finding effort
Sum of MDRTB cases initiated on Rx Sum of MDRTB Suspects
Cumulative data up to December 2013
MDRTB Suspects tested 325316
MDRTB Put on Rx 41860
XDR TB Put on Treatment 490


Analysis of reasons of not initiating
lab confirmed MDR TB cases on treatment
Consolidated data for 1Q12
131, 5% 163, 6%
98, 4%
37, 1%
173, 7%
234, 9%
1819, 68%
Died
Referred
Not willing for Rx
Not traced
Being traced
PreRx eval
On MDR Rx
N = 2625

Interim 12 month outcomes
(latest 4 quarters 2Q11-1Q12)
Patients registered
Culture negative
Culture Positive
Culture not known
Death Default
4670 2392 (51%) 432 (9%) 517 (11%) 695 (15%) 597 (13%)
Patients registered
Success Rate
Failure Death Default
3606 1738 (48%) 263 (7%) 773 (21%) 708 (20%)
Treatment outcomes – Latest 4 Cohorts (2010)
• High level of second line drug resistance (Ofx ~ 24%) • Heavily treatment experienced cohorts • Gaps in case holding capacity

Attrition = Loss due to death, default, treatment stopped
due to any reason, failure and switched to XDR regimen
10% 9%
24%
12% 11% 11%
20% 16%
12%
17% 17% 16% 15% 19% 19%
16% 15% 17%
24%
18%
39%
19% 20% 21%
27% 25%
23%
31% 27% 27% 26% 26% 27% 27%
41%
55%
69%
54%
47%
54% 54%
44% 47%
55% 53%
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
1Q07
2Q07
3Q07
4Q07
1Q08
2Q08
3Q08
4Q08
1Q09
2Q09
3Q09
4Q09
1Q10
2Q10
3Q10
4Q10
1Q11
2Q11
3Q11
4Q11
1Q12
% loss at 6 month % loss at 12 month % loss at 24 month
Actions Required: • Review districts to address quality gaps with
indicators like • % put on Rx, • % culture not known and • % defaults
• Underperforming districts to be closely supervised and monitored
• Intensify supervision (use job-aides) and monitoring

Treatment Challenges & Solutions Deployed
Challenges
• ~ 10% loss from Dx to Rx : — Delay in treatment initiation in spite of
rapid DST — Tracing patients due to poor case
holding
• Limited DR TB Centers and bed capacity to cope with enhanced case load due to Criteria C with LPA/CB-NAAT
• Low treatment outcomes due to high interim attrition of patients – Culture Not Known, Default, Died
• Manual information management
• SLD logistic & supply chain management
Solutions
• Shift to Criteria C with LPA/CB-NAAT • CB-NAAT to offer decentralized DST and same day diagnosis • Improve DOTS, timely results and coordination
• Fast-track DR-TB Centre • Strengthen districts capacity for ambulatory PTE, ADR management • DR TB Centre Scheme in 2014
• Reinforce counseling, FU & ADR Mx •Intensify SME for improve case holding •Integrated Rx Algorithm for DR TB •Bedaquiline – controlled introduction
•NIKSHAY for PMDT in 2014
•Good packing & storage of PWBs • More Store Assist, Outsource SCM

Priorities in 2014
• Focus to enhance quality of services through intensified supervision and
monitoring
• Scaling up Second Line DST capacity across India
• Streamlining TB Notification, Lab surveillance and NIKSHAY
• Further strengthening PPM and developing Urban TB Control models
• Finalization and Dissemination of STCI & Partnership Guidelines
• Involvement of Large Corporate Hospitals under new RNTCP NGO PP
Schemes to facilitate
o TB Notification
o Sample collection centres under Private – Private partnership
o DR TB Centre
o C-DST Lab……….etc.

Thank You!