Sleep Disorders Basics of Sleep Basics of Sleep Stages REM and NREM Sleep.
Upload
shintadeviiCategory
view
6download
0description
SLEEP APNEA AND ITS CONSEQUENCESalim Surani, MD, MPH, MSHM, FACP, FCCP, FAASM
SRS
SNORING PATIENT
Sleep and watchfulness, both of them when immoderate constitutes diseasehippocrates
SRS
SNORING PATIENT
Bible states that Solomons bed was guarded by 60 valliant men throughout the night for fear of death (song of solomon 3:7-8)
In 1945 F. Scott Fitzgerald wrote: In the real darl night of the soul it is always three o clock in the morning
since the 1800s various epidemiological reviews have shown that peak mortality occurs early in the morning.
SRS
SNORING PATIENT
In US 50 million adults have difficulty in sleeping
10 million usually discuss their sleep problems with physicians
5 million receive sleeping pill prescription
SRS
SLEEP DISORDER
Obstructive sleep apnea Central sleep apnea Insomnia Parasomnia
SRS
SLEEP DISORDERS
Falls under following 4 categories DIMS (insomnia), disorder of initiating and
maintaining sleep DOES (OSA, Narcolepsy & sleep deprivation),
disorder of excessive sleeping DOSWS (jet leg, work change etc) disorder of sleep
wake schedule Dysfunction associated with sleep, sleep stages, or
partial arousal (parasomnias)
SRS
OBSTRUCTIVE SLEEP APNEA
AIR FLOW
RESPIRATORYEFFORT
SRS
CENTRAL APNEA
Air flow
Resp effort
Abd movm.
SRS
MIXED APNEA
Air Flow
Resp Effort
Abd movm
SRS
HYPOPNEA
Hypopnea is the reduction of air flow accompanied by 02 desaturation of 4% or more
The number of apnea and hypopnea per hour is termed the respiratory distress index (RDI) or the apnea hypopnea index (AHI)
SRS
RESPIRATORY DISTURBANCE INDEX
RDI 0-5/hour: Normal RDI 5-20/hour: gray zone RDI > 20/hour: Apneic
SRS
SNORING PATIENT
History: Described in 4th century B.C. by Aelianus: I am informed that Dionysis through daily gluttony and intemperance, increased to an extraordinary degree of corpulency and fatness, by reason whereof he had much adoe to take breath. Because of his obesity, he was afflicted with shortness of breath and fits of chocking. So the physicians prescribed that he should get lonf fine needles which they thrust through his ribs; and belly whenever he fell into a very deep sleep
SRS
SNORING PATIENT
The syndrome was described by Charles Dickens in the 19th century novel Posthumous Papers of the Pickwick Club as Joe the Fat boy. The character was described as having plethora, obesity, snoring, psychological changes, and the name young dropsy which elegantly describe right heart failure.
SRS
DEFINITION OF OSA
The upper limit of normal is five apneas/hr. Because apneas normally increase with age, an AI greater than 10/hr is pathologic.
The occurrence and severity of the disordered breathing event, the degree of disruption of sleep, and symptoms determine the need for and the type of therapy.
SRS
DISORDERS COMMONLY ASSOCIATED WITH OBSTRUCTIVE SLEEP APNEA
Obesity Nasal Obstruction Adenoidal and Tonsillar Hypertrophy Macroglossia Retrognathia, Micrognathia Acromegaly Hypothyroidism
SRS
PREVALENCE OF OSA
1. The incidence of OSA is not known 2. Approx. 22% of patients referred to sleep study
are diagnosed with OSA. 3. OSA may affect 2-3% of the population, although
its prevalence has been reported to range from 1% to 15% in the general population.
4. 25% to 37% of people over 65 yrs may be affected.
Prevalence of OSA
Study Location
n Age Range
Prevalence of AHI>5 (95%CI)
Prevalence of AHI15 (95%CI)
Men Women Men Women
Wisconsin 626 30-60 24 (19-28)
9 (6-12)
9 (6-11)
4(2-7)
Penn 1741 20-99 17 (15-20)
Not given 7 (6-9)
2(2-3)
Spain 400 30-70 26 (20-32)
28(20-35)
14 (10-18)
7(3-11)
SRS
SYMPTOMS OF OSA
The typical patient is male (6:1 to 10:1), middle-age to elderly (apneas increase with age), overweight (80%), hypertensive (50-90%) who presents with a history of snoring and hypersomnolence.
As opposed to patients with obesity hypoventilation syndrome, apneics have normal daytime ABGs.
The Multiple Sleep Latency Test (MSLT) was developed to objectively evaluate excessive daytime sleepiness (EDS).
SRS
History: Be specific
Differentiate true sleepiness from fatigue, apathy, depression, etc.
Ask specific situational questions such as: Do you fall asleep reading, watching TV, driving Try for semi-specific answer s such as: always, frequent, occasionally, rarely, or never
SRS
HISTORY : ONSET AND COURSE
Duration of sleepiness complaint Rapidity of onset : days or weeks versus months or
years Age of onset of sleepiness Variability of sleepiness over time Family history of sleepiness
SRS
HISTORY : SLEEP QUANTITY AND SCHEDULE Usual sleep - wake schedule Work time versus non -working variation Shift work and travel Relationship of diurnal sleepiness to nocturnal sleep
quantity Previous perceived sleep needs
SRS
HISTORY : KNOWN DISEASES OR SLEEP DISTURBING FACTORS
Previous head trauma Diseases causing pain, for example: _Arthritis _COPD Drugs and alcohol Environmental disturbances
SRS
HISTORY : OBSERVED BEHAVIOR
History from bed partner is very important Ask about both nocturnal and diurnal behavior _Sleepiness _Snoring _Apneas _Abnormal movements
SRS
MORBIDITY OF OSA
Restless sleep, EDS, intellectual deterioration, personality changes, and behavioral disorders can lead to job loss and life-threatening complications for those who operate motor vehicles and equipment.
Physiologic complications: chronic hypoventilation, hypertension, pulmonary hypertension, cor pulmonale, nocturnal arrhythmias, unexplained nocturnal death.
SRS
TREATMENT APPROACHES FOR PATIENTS WITH OSA
Medical therapy -weight loss -lateral position for sleeping -avoidance of sedative and alcohol -nasal and oral appliances -pharmacological agents * protriptyline * progesterone -oxygen -nasally applied continuous positive airway
pressure
SRS
TREATMENT (cont.)
Surgical Therapy -Treatment of discrete obstruction -Uvulopalatopharyngoplasty -Tracheostomy -Sectioning and advancement of the hyoid -gastroplasty and gastric bypass
SRS
Should all snorers be evaluated?
1. No symptoms or witnessed apneas-advice 2. No symptoms but witnessed apneas-advice 3. Symptoms or excessive witnessed apneas-formal
sleep study and evaluation
SRS
Risk Factors for OSA
Gender (male/female 2:1) Obesity (>120% ideal body weight) Neck size (> 17 male, >15 female) Age (middle age highest risk) Tonsillar hypertrophy Craniofacial abnormalities Retrognathia, Micrognathia Endocrinopathies (Hypothyroidism, acromegaly) Alcohol, sedative or hypnotic use.
SRS
Workup of OSA
Screening overnight oximetry (optional) Overnight Polysomnography (gold standard) 1st night diagnostic study 2nd night therapeutic with CPAP Split night study Ambulatory study
SRS
Consequence of sleep apnea
Nocturnal arrhythmia Hypertension Right and Left heart failure MI Pulmonary Hypertension CVA Cognitive impairment Sexual dysfunction Accidents Death
SRS
Delivery of Positive airway pressure
CPAP BIPAP Auto CPAP Nasal Ventilator
SRS
CPAP
Treatment of choice Most effective noninvasive therapy for
sleep apneaCPAP has shown to reduce
apnea/hypopnea, daytime sleepiness and improve neuropsychiatric function
SRS
CPAP PROBLEM
Patient acceptability Patient acceptability.... Patient acceptabilityAverage night time use of 4.8 hrs
SRS
Common complaints with CPAP
Nocturnal arousals Rhinitis, Nasal irritation, and dryness Aerophagia Mask and Mouth Leaks Fascial skin discomfort Difficulty with exhalation Claustrophobia Chest and Back Pain
SRS
Dental Appliances
Useful in patient who fail CPAP Patients with retrognathia, micrognathia Best oral appliance unknown not universally effectiveNo study on compliance or effect on sleep
SRS
Surgery for OSA
Nasal surgery Removal of Tonsils/adenoids UPPP LAUP ? laser assisted UPP Genioiglossus advancement Maxillomandibular advancement Tracheostomy
SRS
UPPP
Effective in 50%-60% of patients with sleep apnea
effectiveness defined liberally as a 50% reduction in RDI
Results better in those patients with retropalatal obstructions
Normal Sleep and the Heart
NREM Sleep sympathetic neural activity heart rate and CO Blood pressure (dipping) arrhythmogenicity
REM Sleep sympathetic tone Heart rate variability, generally Blood pressure variable Sinus pauses/arrhythmia not uncommon
Recordings of Sympathetic-Nerve Activity (SNA) and Mean Blood Pressure (BP)
Somers V et al. N Engl J Med 1993;32
ABnormal Sleep and the Heart
NREM Sleep + SDB sympathetic activity heart rate Blood pressure (non-dipping) arrythmogenicity
REM Sleep + SDB symptathetic tone Heart rate variability Blood pressure variable arrhythmias
Acute cardiovascular consequences of OSA
Related to Hypoxia
Hypercapnia
Increased intrathoracic pressure
Arousals
Brainstem mediated: 1. ventilation2. sympathetic neural outflow
Hypoxia
Weir, NEJM, 2005
SNA
RESP200
100
0
BP
Somers, J Clin Invest, 1995
Sympathetic Neural MechanismsIntra-neural Recordings - SLEEP
Normal OSA
Increased Sympathetic ToneDuring Wakefulness
Somers et al, J Clin Invest, 1995
MSNA
HEALTH CONSEQUENCES
FRAGMENTED SLEEP Sleepiness Productivity School grades Motor vehicle
accidents Mood changes
depression Senility
INTERMITTENT HYPOXIA Hypertension Stroke Coronary disease Heart failure Diabetes Obesity Metabolic syndrome PCOS Impotence Pregnancy complications
Hypertension
Independent risk factor Treatment of OSA
improves BP control Screen for ALL new
hypertensives with obesity and/or history of loud snoring
STROKE
70% of stroke victims have OSA
Cause vs effect vs both?
Treatment of OSA improves stroke outcome and survival
Drager et al; Am J Resp Crit Care Med 2005;172:613-8
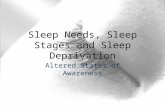
SDB and Carotid Artery Atherosclerosis in Humans
Drager et al; Am J Rep Crit Care Med 2007; 176:706
CPAP Therapy Improves Sub-clinical Atherosclerosis
Effect of SDB on Stroke and Death
Yaggi et al; N Engl J Med 2005;353:2034
Young et al. Sleep 2008;31:1071-8
Untreated SDB is associated with increased risk for death
Acute coronary syndrome
CARDIAC ARRHYTHMIAS
OSA and bradyarrhythmia
Bradycardia, AV blocks, asystole can occur in 10% of OSA pts
Mostly in REM and associated desaturation Occurs during the apneic episode
Reversed with CPAP Recent European Multicenter polysomnographic
study showed presence of OSA in 60% of pts with pacemaker 68% of pts with AV block have OSA
Garrigue S et al. Circulation 2007;115:1703-9.
SDB: Cardiac ArrhythmiasSHHS Data
Mehra R et al. Am J Res Crit Care Med 2006;173:910-916
SDB: Cardiac Arrhythmias
Arrhythmia Type Unadjusted Odds Ratio
Odds Ratio* (95% CI) Adjusted for Age, Sex,
BMI
Odds Ratio* (95% CI) Adjusted for Age, Sex, BMI, CHD
Nonsustained ventricular tachycardia
4.64 (1.4814.57)
3.72 (1.1312.2) 3.40 (1.0311.2)
Complex ventricular ectopy
1.96 (1.283.00)
1.81 (1.162.84) 1.74 (1.112.74)
Atrial fibrillation 5.66 (1.5620.52)
3.85 (1.0014.93) 4.02 (1.0315.74)
Mehra R et al. Am J Res Crit Care Med 2006;173:910-916
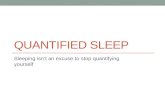
Gami, A. S. et al. Circulation 2004;110:364-367
Increased Prevalence of OSA in AFib Compared with General Cardiology Patients
OSA and Recurrence of A-Fib
Pts with a-fib/flutter referred for electrical cardioversion 43 had a formal sleep study resulting in the diagnosis
of OSA 79 randomly selected post-cardioversion patients
matched pts without prior sleep study
Kanagala, R. et al. Circulation 2003;107:2589-2594
Kanagala, R. et al. Circulation 2003;107:2589-2594
12 mo Recurrence AFib after DCCV
OSA and Risk of Incident Atrial Fibrillation
Mayo Clinic center for sleep medicine, 1987-2003
3,542 consecutive Olmsted County adults
No current or past history of AF First diagnostic polysomnography
49 14 yo BMI 33 9
Gami AS et al. JACC 2007;49:565
Incidence of AF by OSA Status
P = 0.002
Gami AS et al. JACC 2007;49:565
OSA, AHI, and O2 desaturations are risk markers for incident AF by 5 years follow-up
BMI independently predicts AF
O2 desaturation independently predicts AF
Gami AS et al. JACC 2007;49:565
Take-homes about a-fib
OSA is very common (48%) in patients with a-fib OSA is an independent risk factor for developing a-
fib (OR = 4) A-fib patients who are cardioverted and have
untreated OSA have a 2.5 X increased risk of recurrence compared with treated OSA patients
Makes sense to identify and treat OSA
OSA and PVCs
PVCs reported in 66% of pts with OSA (0-12% in the general population)
No conclusive data that OSA causes PVCs
Occurs mostly during apneic periods When O2 sats fall below 60%
May be seen more often in pts with concurrent CHF, comorbid CVD
Guilleminault C et al. Am J Cardiol 1983;52:490-4Hoffstein V. Chest 1995;106:466.
Shepard JW Jr et al. Chest 1985;88:335-340.
OSA and PVCs
Treatment with CPAP Randomized control 1 month trial
OSA and systolic dysfunction 58% reduction in PVCs and nocturnal urinary norepinephrine concentrations
No evidence to support atrial overdrive pacing as a treatment for OSA.
Ryan CM et al. Thorax 2005;60:781-785.
Sudden Death and OSA
Patients with OSA had high risk of nocturnal SDPatients without OSA had highest SD 0600-1200 hrs
Gami, NEJM 2005
Coronary Artery Disease and OSA
High prevalence of OSA in patients with CAD Prevalence 37-76%
CAD present by angiography in 20-68% of patients with OSA
Does it matter?
Cardiac Ischemia and OSA
ST-segment depression common during apneic events in sleep of OSA patients More frequent in more severe OSA
Philip et al. Sleep. 16:558-559, 1993
Correlate with oxygen desaturation and complaints of nocturnal angina.
CPAP therapy normalizes ST depression in sleep. Peled et al. J. Am. Coll. Cardiol. 34:1744, 1999.
In a five year follow-up of patients with established CAD, higher mortality in patients with OSA (38%) compared to those without OSA (9%)
Peker et al. Am J. Respir. Crit. Care. 162:81-86, 2000.
Observational Cohort
>1600 men (50 yo) followed for 10.1 years
36% of patients with severe OSA refused CPAP
Marin JM et al. Lancet 2005; 365: 1046-53.
BMI 30.3
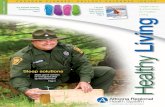
Conclusions: Treatment of OSA is associated with a reduction in cardiac deaths, but not in MACE or MACCE, after PCI. Screening for, and treating, OSA in patients with CAD who may undergo PCI may result in decreased cardiac death.
CP1281042-1
Cardiac Death After PCI
Cassar et al: JACC, 2007
0
2
4
6
8
10
12
0 12 24 36 48 60
%
Months after PCI175 151 118 94 69 49196 161 139 107 85 68
P=0.027
Treated OSA
Untreated OSA
Pulmonary Hypertension and OSA
No prospective incidence data available No relative risk data available Related more to BMI and daytime hypoxemia (lung
function) Available studies in mild disease
(mean PAP 20-25 mm Hg) Modest treatment effects in reducing PAP
In the evaluation of patients with PAH, an assessment of SDB is recommended. Quality of evidence: low; net benefit: small/weak; strength of recommendation: C.
In the evaluation of a patient with PAH for SDB, polysomnography is recommended if OSA is suspected as the etiology, if a screening test result for OSA is positive, or if a high clinical suspicion for OSA is present. Quality of evidence: expert opinion; net benefit: intermediate; strength of recommendation: E/B.
In the management of patients with OSA, routine evaluation for the presence of PAH is not recommended. Quality of evidence: low; net benefit: none; strength of recommendation: I
In patients with OSA and PAH, treatment of OSA with positive airway pressure therapy should be provided with the expectation that pulmonary pressures will decrease, although they may not normalize, particularly when PAH is more severe. Quality of evidence: low; net benefit: small/weak; strength of recommendation: C.
Summary of Recommendations:
2004
Features of "syndrome Z"
Hypertension Central obesity Insulin resistance Hyperlipidaemia Obstructive sleep
apnoea
Leptin - a hormone produced predominantly in white adipose tissue.
Leptin levels increase exponentially with increasing fat mass. Leptin inhibits the synthesis of hypothalamic neuropeptide Y
(NPY), a potent stimulator of food intake. Downregulation of NPY results in increased sympathetic
nervous system outflow and energy expenditure. Activate thyroid, growth hormone, and gonadal axes and
suppress the pituitary-adrenal axis. Directly inhibits intracellular lipid by reducing fatty-acid and
triglyceride synthesis and, concomitantly, by increasing lipid oxidation
Just blame it on LEPTIN
Obesity is a leptin-resistant state. Treatment with subcutaneous leptin reduces
weight in all mammalian species tested. Leptin-induced weight loss is completely specific
for loss of adipose tissue, whereas food restriction results in loss of both adipose tissue and lean body mass.
Copyright restrictions may apply.
Ozturk, L. et al. Arch Otolaryngol Head Neck Surg 2003;129:538-540.
Positive correlation of plasma leptin levels with apnea-hypopnea index
CPAP and leptin
Prevalence of sleep apnea in men with erectile dysfunctionHirshkowitz, M., Karacan, I., Arcasoy, M.O., Acik, G., Narter, E.M., Williams, R.L.
Sleep studies were performed on 1,025 patients complaining of erectile dysfunction.
Overall prevalence of sleep apnea activity in this sample was: 43.8 percent with AI 5; 27.9 percent with AI 10; and 19.6 percent with AI 15.
These results confirm that sleep apnea activity is common in men with erectile dysfunction.
CPAP therapy resolved the erectile dysfunction in 13 out of 17 patients.
Sleep-Disordered Breathing & School Performance in Children Identified 1st graders
performing at the bottom 10% percent of grade level
Found over 20% had OSA All were offered surgery
(tonsillectomy and adenoidectomy), but only half accepted
All children who had surgery improved their grades, the others stayed the same
Gozal, Pediatrics, 1998.
Non-arteritic anterior ischemic optic neuropathy
Sudden, painless, irreversible, non-progressive visual loss
Mojon et al found that twelve (71%) of their 17 patients with NAION had SAS, compared to only 3 (18%) of 17 controls (P=005)
Arch Ophthalmol 120 (2002),
57% of pts with NTG, compared to 3% of non-glaucoma patients had a positive sleep history (P=0.001).
11 out of 13 with a positive sleep history that underwent PSG were diagnosed OSA
NTG = NORMAL TENSION GLAUCOMAJ Glaucoma 10 (2001), pp. 17
CPAP therapy
CPAP
PAP provides a "pneumatic splint" by delivering an intraluminal pressure that is positive with reference to the atmospheric pressure.
PAP increases upper-airway cross-sectional area and volume in awake normal subjects and OSA patients with the largest change in the lateral dimensions.
A second mechanism by which PAP may affect upper airway size is by increasing lung volume. The increased lung volume provides a downward traction on the trachea (tracheal tug). This action is believed to stretch upper-airway structures and increase upper-airway size.
ThankyouAlsothankstoDrSSubramanyian andDrKRamar forProvidingsomeslides
Sleep Apnea and its consequenceSNORING PATIENTSNORING PATIENTSNORING PATIENTSLEEP DISORDERSLEEP DISORDERSOBSTRUCTIVE SLEEP APNEACENTRAL APNEAMIXED APNEAHYPOPNEARESPIRATORY DISTURBANCE INDEXSNORING PATIENTSNORING PATIENTDEFINITION OF OSADISORDERS COMMONLY ASSOCIATED WITH OBSTRUCTIVE SLEEP APNEAPREVALENCE OF OSAPrevalence of OSASYMPTOMS OF OSAHistory: Be specificHISTORY : ONSET AND COURSEHISTORY : SLEEP QUANTITY AND SCHEDULEHISTORY : KNOWN DISEASES OR SLEEP DISTURBING FACTORSHISTORY : OBSERVED BEHAVIORMORBIDITY OF OSATREATMENT APPROACHES FOR PATIENTS WITH OSATREATMENT (cont.)Should all snorers be evaluated? Risk Factors for OSAWorkup of OSAConsequence of sleep apneaDelivery of Positive airway pressureCPAPCPAP PROBLEMCommon complaints with CPAPDental AppliancesSurgery for OSAUPPPNormal Sleep and the HeartRecordings of Sympathetic-Nerve Activity (SNA) and Mean Blood Pressure (BP)ABnormal Sleep and the HeartAcute cardiovascular consequences of OSAHypoxiaSympathetic Neural MechanismsIntra-neural Recordings - SLEEPIncreased Sympathetic ToneDuring WakefulnessHEALTH CONSEQUENCESHypertensionSlide Number 47Slide Number 49Slide Number 50STROKESlide Number 52Slide Number 53Slide Number 54Slide Number 55Slide Number 56Acute coronary syndromeSlide Number 58Slide Number 59Slide Number 60Slide Number 61Slide Number 62Slide Number 63Slide Number 64Slide Number 65Slide Number 66Cardiac ArrhythmiasOSA and bradyarrhythmiaSDB: Cardiac ArrhythmiasSHHS DataSDB: Cardiac ArrhythmiasSlide Number 71OSA and Recurrence of A-FibSlide Number 73OSA and Risk of Incident Atrial FibrillationIncidence of AF by OSA StatusSlide Number 76Take-homes about a-fibOSA and PVCsOSA and PVCsSudden Death and OSACoronary Artery Disease and OSACardiac Ischemia and OSASlide Number 83Slide Number 84Cardiac Death After PCIPulmonary Hypertension and OSASlide Number 87Slide Number 88Slide Number 89Slide Number 90Slide Number 91Slide Number 92Slide Number 93Just blame it on LEPTINSlide Number 95Slide Number 96CPAP and leptinSlide Number 98Slide Number 99Slide Number 100Slide Number 101Prevalence of sleep apnea in men with erectile dysfunctionHirshkowitz, M., Karacan, I., Arcasoy, M.O., Acik, G., Narter, E.M., Williams, R.L. Slide Number 103Sleep-Disordered Breathing & School Performance in Children Slide Number 105Slide Number 106Slide Number 107Slide Number 108Slide Number 109Slide Number 110Slide Number 111Non-arteritic anterior ischemic optic neuropathySlide Number 113Slide Number 114CPAP therapyCPAPSlide Number 117