Metabolic Diseases of the Bone Osteoporosis Osteomalacia Paget’s Gout Bone Tumors.

Prepared by Dr.Salah Mohammad FatihMBChB,DMRD,FIBMS(radiology)

X-rayIsotope US CT MRI

1-Plain bone radiograph

Initially, a musculoskeletal lesion should be simply imaged with a plain film. It should be remembered that plain films remain the most reliable imaging method for assessment of both biological activity and probable histological diagnosis of an osseous lesion.

Signs of bone diseases in plain X-ray are;

1-Decreased bone density2-Increased bone density
(sclerosis).3- Periosteal reaction4- Cortical thickening5- Alteration in the trabecular pattern6- Alteration in the shape of a bone7-Altreration in bone age

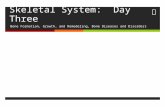
Localize (lytic area or area of ‘ bone distruction’)
Generalize

Giant cell tumor

osteoporosis

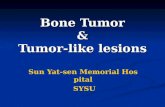
2-increased bone density (sclerosis).
Focal Generalized

Osteopetrosis

osteosarcoma

It refers to excessive bone produced by the periosteum, which occur in response to infection , trauma & tumors

Patterns of periosteal reaction;

1- Linear




Also involve laying down of new bone by the periosteum,but the process is very slow & it has the same homogeneous density as does the normal cortex& there is no separate lines or specules of calcification as seen in a periosteal reaction

causes 1- chronic osteomylitis. 2-healed truama 3- response to chronic stress or benign
tumor

Chronic osteomylitis

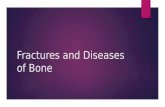
Usually involving a reduction in the no. of trabeculae with an alteration in the remaining trabeculae.
e.g in osteoporosis, there is reduction in the no. of the trabeculae & remaining trabiculae are more prominent than usual associated with thinning of the cortex.
in paget‘s disease , there is thickening of the trabeculae & associated with thickening of the cortex & bone expansion

Local osteoporosis Normal

Paget disease

Congenital Acquired , e.g Acromegaly, expanding bone
tumors



US can not demonstrate bone pathology but does have a complementary imaging role;
Dtecting tenosynovitis, tendon tear & rupture.
In diagnosis of ostiomyelitis

Technetium-99m lablled phosphate complexes

Dtection of metastasis. Detection of oseomylitis . Determination of whether a lesion in solitary or multiple. Investigation of clinically suspected lesion when the Plain
radiograph is –ve. Investigation of radiographically equivocal cases whether is
significant or not.
Investigation of pain full prosthesis .


Is only needed in selected cases. Indications for bone CT are1. Demonstrating abnormalities in the areas where
plain films are frequently difficult to be interpretated for exam. Spine , hip &pelvis
2. As a guide for bone biopsy.
3. Demonstration of the extent &characterization of the bone tumor in selected cases to complement MRI




Play a vital important role in musculoskeletal disorders.
In can demonstrate bone marrow directly but calcified tissues & cortical bones produces no signal.
MRI particularly good for showing soft tissue abnormalities

Disc herniation & spinal cord or nerve root compression.
Dx of bone metastasis. Extend of primary bone tumor. To image soft tissue masses To Dx osteomyelitis & shows any soft
tissue abscess. To Dx avascular necrosis & other joint
pathologies



Bone disease can be devided in to; 1- focal: lytic , sclerotic or mixed solitory multiple 2- generalized; where all the bones show
diffuse increase or decease in bone density 3- alteration in the trabecular pattern or
changes in the shape

Lytic Sclerotic Mixed

Radiological approach for diagnosis of solitary bone lesions
to decide whether the lesion is benign (i.e. stable or very slow growing) or
whether the lesion is aggressive (malignant tumor or infection).

1. Age of the patient. This can be an extremely important determinant
in some lesions in which the age range of occurrence may be quite narrow. For example,
Malignant osseous lesions in patients under one year of age are usually metastatic neuroblastoma.
Malignant osseous lesions in the age range of 1 to 30 years are usually osteosarcoma or Ewing's sarcoma.
Malignant osseous lesions in the 30- to 60-years range most commonly will be either chondrosarcoma, primary lymphoma, or malignant fibrous histiocytoma,
Malignant lesions in the age range over 50 most commonly will be due to metastatic disease or multiple myeloma.

Three different types of locations should be noted:
1- the particular bone that is involved. ( long bone ,flat bone , small bones)
3- the location in a transverse axis. (central, eccentric, or a cortically-based epicenter).
3- the location in a longitudinal axis of a long bone. (epiphysis, metaphysis or diaphysis).
Certain lesion occur at the certain sites;E.g. Osteomyelitis characteristically occur in the metaphyseal
areas specially of the knee & lower tibia whereas giant cell tumor occur in subarticular areas


i.e. Zone of transition of the lesion from abnormal to normal bone;
A wide zone of transition denotes an aggressive lesion.
A narrow zone is a much less aggressive lesion.
well defined sclerotic edge is almost certainly benign.

Any destruction of the adjacent cortex indicates an aggressive lesion such as a malignant tumor or osteomyelitis

Bone expansion with an intact well formed cortex usually indicate a slow growing lesion such as an encondroma or fibrous dysplasia.

Presence of an active periosteal reaction in the absence of the trauma usually indicates an aggressive lesion

. Cortical breakthrough of a bone lesion to create a soft tissue mass generally suggest an aggressive lesion(infection or tumor) .
ill define soft tissue swelling adjacent to focal bone disruction lesion suggest infection .
well define soft tissue swelling adjacent to the bone lesion suggest neoplasm& such soft tissue masses will often distort but not obliterate nearby muscle planes.

Common terminology includes ; "geographic" (well-defined or map-like lesion, the least aggressive
pattern), "moth-eaten" (holes, with less well-defined margins, appearing
more aggressive) "permeative" (a poorly demarcated pattern which is often very
difficult to visualize and represents a highly aggressive lesion)

allow categorization of a lesion as bone producing versus cartilage producing.
Diffuse ill defined calcification within the lesion suggest osteoid lesion .
presence of a patchy calcification of popcorn or stippled type with density more than normal bone usually indicate cartilagenous tumor

Generally, a larger lesion (greater than 5 cm) is more likely to be malignant or aggressive, but there are many exceptions to this statement, and other determinants are generally more important than this one.

This is the last most important point , since polyostotic lesions automatically restrict the number of disease processes that might be considered. For example,
nonaggressive polyostotic lesions should be confined to; fibrous dysplasia Paget's disease Histiocytosis multiple exostosis multiple enchondromatosis Aggressive polyostotic lesions would be confined to osseous metastases multiple myeloma primary bone tumor with osseous metastases, multifocal osteomyelitis, aggressive histiocytosis, and multifocal
vascular bone tumors.