DrPh Session 3 - Tufts...
20
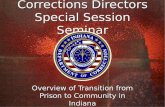
1 DrPH Seminar Session 3 Quantitative Synthesis – Focusing on Heterogeneity Qualitative Synthesis – e.g., GRADE Mei Chung, PhD, MPH Research Assistant Professor Nutrition/Infection Unit, Department of Public Health and Community Medicine, Tufts School of Medicine FORMULATE STUDY QUESTION ESTABLISH PROTOCOL CRITICAL APPRAISAL PAPER SELECTION per PROTOCOL DATA EXTRACTION and QUALITY ASSESSMENT ANALYSIS and INTERPRETATION WEIGHTED AVERAGE REGRESSION SENSITIVITY ANALYSIS LITERATURE SEARCH / RETRIEVAL Steps of Performing a Systematic Review Ask Identify Acquire Appraise Synthesize 1
Transcript of DrPh Session 3 - Tufts...

1
DrPH Seminar Session 3
Quantitative Synthesis – Focusing on Heterogeneity
Qualitative Synthesis
– e.g., GRADE
Mei Chung, PhD, MPH Research Assistant Professor
Nutrition/Infection Unit, Department of Public Health and Community Medicine, Tufts School of Medicine
FORMULATE STUDY QUESTIONESTABLISH PROTOCOL
CRITICAL APPRAISAL PAPER SELECTION per PROTOCOL
DATA EXTRACTION and QUALITY ASSESSMENT
ANALYSIS and INTERPRETATIONWEIGHTED AVERAGE
REGRESSIONSENSITIVITY ANALYSIS
LITERATURE SEARCH / RETRIEVAL
Steps of Performing a Systematic Review
Ask
Identify
Acquire
Appraise
Synthesize
1

2
Meta-analysis 101
n The term “meta-analysis” typically referred to meta-analysis of study-level, summary data
n The term “pooled analysis” typically referred to meta-analysis of individual-level data across different studies
n Conventional meta-analysis methods and software are designed for combining RCTs (comparisons of ES between two independent groups)
2
Reasons for Meta-analysis
n Improve the power to detect a small difference if the individual studies are small
n Improve the precision of the effect measure n Compare the efficacy of alternative interventions
and assess consistency of effects across study and patient characteristics
n Gain insights into statistical heterogeneity n Help to understand controversy arising from
conflicting studies or generate new hypotheses to explain these conflicts
n Force rigorous assessment of the data
3

3
Principles of Combining Data for Basic Meta-analyses
n For each analysis, one study should contribute only one treatment effect.
n The effect estimate may be for a single outcome or a composite.
n The outcome being combined should be the same (or similar-based on clinical plausibility) across studies.
n Know your question. The question drives your study selection, synthesis, and interpretation of the results.
4
Things to Know about the Data before Combining
n Biological and clinical plausibility n Scale of effect measure n Studies with small number of events do
not give reliable estimates
5

4
True Associations May Disappear When You Combine Data Inappropriately
6
Apparent Association May Be Seen When There is None
7

5
Changes in the Same Scale May Have Different Meaning
Effe
ct o
f int
eres
t
Variable of interest
A
B
C
DBoth A–B and C–D involve a change of one absolute unit. A–B change (1 to 2) represents a 100% relative change. C–D change (7 to 8) represents only a 14% relative change.
8
Commonly Encountered Comparative Effect Measures
Type of Data Corresponding Effect Measure
Continuous Mean difference (e.g., mmol, mmHg) Standardize mean difference (effect size) Correlation
Dichotomous Odds ratio, risk ratio, risk difference
Time to event Hazard ratio
9

6
What Is the “Average (Overall)” Treatment-Control BP Difference?
10
Study N Mean difference
mmHg
95% CI
A 554 -6.2 -6.9 to -5.5
B 304 -7.7 -10.2 to -5.2
C 39 -0.1 -6.5 to 6.3
Simple Average
(−6.2) + (−7.7) + (−0.1) 3
= −4.7 mmHg
n
xX
k
ii∑
== 1
11
Study N Mean difference
mmHg
95% CI
A 554 -6.2 -6.9 to -5.5
B 304 -7.7 -10.2 to -5.2
C 39 -0.1 -6.5 to 6.3

7
Weighted Average
(554 x −6.2) + (304 x −7.7) + (39 x −0.1) 554 + 304 + 39
= −6.4 mmHg
∑
∑
=
== k
ii
k
iii
w
xwX
1
1
12
Study N Mean difference
mmHg
95% CI
A 554 -6.2 -6.9 to -5.5
B 304 -7.7 -10.2 to -5.2
C 39 -0.1 -6.5 to 6.3
General Formula: Weighted Average Effect Size (d+)
∑
∑
=
=+ = k
ii
k
iii
w
dwd
1
1
where: di = effect size of the ith study wi = weight of the ith study k = number of studies
13

8
Calculation of Weights
n Generally the inverse of the variance of treatment effect (that captures both study size and precision)
n Different formula for odds ratio, risk ratio, risk difference
n Readily available in books and software
14
Heterogeneity (Diversity)
n Is it reasonable (are studies characteristics and effects sufficiently similar) to estimate an average effect?
n Types of heterogeneity – Clinical diversity – Methodological diversity – Statistical heterogeneity
15

9
Clinical Diversity
Are the studies of similar treatments, populations, settings, design, etc., such that an average effect would be clinically meaningful?
16
Methodological Diversity
Are the studies of similar design and conduct such that an average effect would be meaningful?
17 17

10
Statistical Heterogeneity
n Is the observed variability of effects greater than that expected by chance alone?
n Two statistical measures are commonly used to assess statistical heterogeneity – Cochran’s Q-statistics – I2 index
18
Cochran’s Q-Statistics χ2 (chi-square) Test for Homogeneity
( )21
2)1( +
=− −== ∑ ddwQ ii
k
idfkχ
di = effect measure d+ = weighted average
19
Q-statistics measures between study variation
19

11
20
I2 Index and its Interpretation
• I2 describes the percentage of total variation in study estimates that is due to heterogeneity rather than chance.
• The value of I2 index ranges from 0% to 100%. • A value of 25% is considered as low heterogeneity, 50% as
moderate, and 75% as large. • The I2 index is independent of the number of studies in the
meta-analysis. It could be compared directly between meta-analyses.
2 max ,11
QHk⎛ ⎞= ⎜ ⎟−⎝ ⎠
22
2
1HIH−
=
Higgins JPT, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–560.
21 A Meta-analysis with a Large Degree of Heterogeneity

12
22
Choi et al. Developmental Fluoride Neurotoxicity: A Systematic Review and Meta-Analysis
Heterogeneity
n Diversity of studies in a meta-analysis n Typically abundant n Arguably the most important role of meta-
analytic methodologies is to quantify, explore, and explain between-study heterogeneity

13
Statistical heterogeneity
Statistical heterogeneity exists when the results of the individual studies are not “consistent” among themselves
Clinical heterogeneity
Methodological heterogeneity
Biases
Chance
Statistical heterogeneity
Clinical vs. statistical heterogeneity
n Clinical and methodological heterogeneity is abundant. Our aim is to explore it, and use these observations to formulate interesting hypotheses.
n Often, but not always, clinical and methodological heterogeneity will result in a statistically significant test
n Chance, technical issues or biases may result in statistically significant results in heterogeneity tests

14
HETEROGENEOUS TREATMENT EFFECTS
IGNORE INCORPORATEESTIMATE(insensitive) EXPLAIN
FIXED EFFECT MODEL
DO NOT COMBINE WHEN
HETEROGENEITY IS PRESENT
RANDOM EFFECTS MODEL
SUBGROUP ANALYSES
META-REGRESSION(control rate, covariates)
Dealing with Heterogeneity 26
Lau J, et al. Quantitative synthesis in systematic review. Ann Intern Med 1997; 127:826.
Fixed- vs. Random-Effects Meta-analysis
n Fixed Effect Model (FEM): Assumes a common treatment effect.
n Random Effect
Model (REM): In contrast with the FEM, the REM accounts for between study variation.
27

15
Weights of the Fixed Effect and Random Effects Models
*1*
vvw
ii +=
ii vw 1=
Random Effects Weight Fixed Effect Weight
where: vi = within study variance
v* = between study variance
28
Commonly used Statistical Methods for Combining 2x2 Tables
Odds Ratio
Risk Ratio
Risk Difference
Fixed Effect Model
Mantel-Haenszel Peto Exact
Inverse variance weighted
Mantel-Haenszel
Inverse variance weighted
Inverse variance weighted
Random Effects Model
DerSimonian& Laird DerSimonian& Laird
DerSimonian& Laird
29

16
30 Figure 1. An example of a fixed-effects MA
Figure ㄉ. An example of a random-effects MA
Borenstein et al. A basic introduction to fixed-effect and random-effects models for meta-analysis Res. Syn. Meth. 2010, 1 97--111
Dealing with HeterogeneityHETEROGENEOUS
TREATMENT EFFECTS
IGNORE INCORPORATEESTIMATE(insensitive) EXPLAIN
FIXEDEFFECTS MODEL
DO NOT COMBINEWHEN
HETEROGENEITYIS PRESENT
RANDOMEFFECTSMODEL
SUBGROUPANALYSES
META-REGRESSION(control rate,covariates)

17
Trea
tmen
t effe
ct
Trea
tmen
t effe
ct
variable of interest
META-REGRESSION modeling summary data
OVERALL ESTIMATE combining summary data
RESPONSE SURFACE modeling individual patient data
varia
ble 2
Trea
tmen
t effe
ct
variable 1Tr
eatm
ent e
ffect
SUBGROUP ANALYSES differentiating effects in subgroups
Summary: Statistical Models of Combining 2x2 Tables
n Most meta-analyses of clinical trials combine treatment effects (risk ratio, odds ratio, risk difference) across studies to produce a common estimate, using either a fixed effect or random effects model.
n In practice, the results using these two models are similar when there is little or no heterogeneity.
n When heterogeneity is present, the random effects model generally produces a more conservative result (smaller Z-score) with a similar estimate but with a wider confidence interval. However, there are rare exceptions of extreme heterogeneity where random effects model may yield counterintuitive results.
33

18
Caveats
n Many assumptions are made in meta-analyses, care is needed in the conduct and interpretation.
n Most meta-analyses are retrospective exercises, suffering from all the problems of being an observational design.
n We cannot make up missing information or fix poorly collected, analyzed, or reported data.
34 34
Summary n Basic meta-analyses can be easily carried out with
one of many readily available statistical software. n Relative measures are more likely to be
homogeneous across studies and is generally preferred.
n Random effects model is the appropriate statistical model in most instances.
n Decision to do a meta-analysis should be based on a well-formulated question, appreciation of the heterogeneity of the data, and understanding of how the results will be used.
35

19
Q & A
36
Qualitative Synthesis
n Also called, Grading Strength of Evidence – Distinct from rating quality of articles/
studies – Many tools, e.g. GRADE
n Qualitative synthesis is required for a systematic review – Meta-analysis is optional
37

20
GRADE
WHO GRADE process http://cebgrade.mcmaster.ca/ WHO guidelines and GRADE: An overview summary (60 minutes) http://cebgrade.mcmaster.ca/Summary/index.html
38
Dividing Homework
n Session 4: Mock expert panel – Jefferson T et al. Vaccines for preventing
influenza in healthy adults. Cochrane Database Syst Rev. 2010 Jul 7;(7):CD001269. doi: 10.1002/14651858.CD001269.pub4. Review. Update in: Cochrane Database Syst Rev. 2014;3:CD001269. PubMed PMID: 20614424. l Three outcomes : Three students (what a
coincidence!)
39