DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and...

of 16
-
Upload
deba-p-sarma -
Category
Documents
-
view
220 -
download
0
Transcript of DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and...
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
1/16
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
2/16
Clinical Featur es
Desmoplastic melanoma (DM) is a rare variant of spindle cell melanoma and an uncommon form of melanoma,
comprising 4% of all melanomas. DM was first described by Conley et al. in 1971 as an inconspicuous superficial
melanocytic lesion of the head and neck, preceding the development of a bulky dermal and subcutaneous tumor [1].
The tumor presents in older individuals as a flesh-colored or variably pigmented nodule measuring on average 2 cm.
It is usually seen on sun-exposed skin (37%) but also on mucosal and acral sites. Males are affected more often than
women, with the exception of the lower limbs. If prominent neurotropism is present, which occurs in at least 30% of
cases, nerve invasion can produce dysesthesias or nerve palsies. DM often is difficult to detect clinically, since half lack
pigmentation. Pale lesions, in particular, are mistaken clinically for basal cell carcinoma, dermatofibroma, or scar.
Pigmentation often is due to an associated lentigo maligna or superficial spreading melanoma. Unusual presentations
include young age, an erythematous nodule, or alopecia. Ulceration is uncommon.
Histopathology (Figure s 1, 2, 3, 4)
DM is composed of usually non-pigmented fusiform melanocytes which often resemble fibroblasts (Figure 1). The
atypical melanocytes are embedded within collagen bundles and may be associated with mild to marked stromal
fibrosis. Phenotypical heterogeneity is under-recognized and desmoplasia may be seen throughout the tumor or in
combination with conventional melanoma (combined DM) [3, 4]. Ultrastructurally, the desmoplastic component
appears to derive from melanocytes that have undergone adaptive fibroplasia [2]. Most often the spindle cells are
arranged in a haphazard fashion, but are sometimes arranged in parallel bundles or in storiform configurations. The
spindle cells are usually mildly to moderately atypical, although cells with larger, more hyperchromatic nuclei are often
seen. Paucicellular variants of DM, in particular, are easily missed on small biopsy specimens. Junctional components
are sometimes minimal or absent. Mitotic rate is variable but often is low, with abnormal forms in the more cellular
tumors. The overlying epidermis may be thinned or thickened with clusters of lymphocytes located at the tumor
periphery. Neurotropism is a common feature (seen in up to 30%) and neural differentiation with a malignant
peripheral nerve sheath-like histology may be seen [5-8]. Neurotropism may be peri- or intraneural and may extend
beyond the desmoplastic component. An osteogenic variant has been reported [9].
The spindle cells in DM are positive for S-100 protein (Figure 2), although sometimes within only a few nuclei (Table
1). Neuron-specific enolase (NSE) and smooth muscle actin (SMA) may be positive, while HMB45 (Figure 3) and
Melan-A (MART-1) and are usually negative [10-13]. Microphthalmia transcription factor (MITF) may (Figure 4) or
may not be positive No single specific marker is yet available to differentiate desmoplastic melanomas from other
tumors [14].
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
3/16
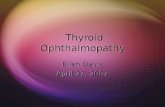
Figure 1. Dermal spindle cell neoplasm.
Figure 2. The tumor cells are focally positive for S-100 protein
Figure 3. Tumor cells are negative for HMB-45
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
4/16
Figure 4. Tumor cells show strongly positive nuclear stain with MITF.
Prognosis and Treatment
Desmoplastic melanoma was reported in the older literature as having a worse prognosis when compared to other
types of melanoma. However, recent findings suggest that prospectively diagnosed and definitively treated lesions
show the same survival rate as the usual forms of melanoma when various histologic parameters and risk factors arecontrolled. Expression of N-cadherin may portend a poorer prognosis, however [15]. Treatment is with wide local
excision.
Spindle Cell (Squam ous Cell) Carcinom a.
Clinical Featur es
Squamous cell carcinoma is the second most common cutaneous malignancy after basal cell carcinoma. The uncommon
spindle cell variant occurs commonly on sun-exposed surfaces of elderly patients as a plaque or as an enlarging tan to
red nodule, often with surface ulceration and crusting. The spindle cell (squamous cell) carcinoma (SCSCC) may beassociated with previous skin injury, including trauma and radiotherapy.
Histopathology (Figure s 5, 6, 7, 8)
Four histopathologic categories of squamous cell carcinoma are described: conventional, spindle cell, acantholytic, and
verrucous. In the uncommon spindle cell variant, atypical spindle cells emanate from the epidermis and form whorls
intermingling with strands of collagen (Figures 1, 2). Within the dermis, the cells form intertwining fascicles and
bundles. Individual tumor cells have indistinct borders and contain eosinophilic cytoplasm. Nuclei are hyperchromatic
or vesicular and elongated. Nuclei may be pleomorphic and contain multiple nucleoli. Mitotic activity is brisk and
atypical forms may be seen. With cellular pleomorphism and tumor giant cell formation, the tumors can bear a closeresemblance to atypical fibroxanthoma. In fact, prior to the advent of immunohistochemistry, these lesions were often
misdiagnosed. Connection of malignant tumor cells to the epidermis or foci of more typical squamous differentiation
favor spindle cell carcinoma. Cytokeratin stains (Figure 7) are usually helpful. In addition, SCSCC can stain positively
with mesenchymal markers such as vimentin (Figure 8) and smooth muscle actin.
Recently it has been suggested that p63 may be a useful marker for SCSCC; Dotto et al. reports a series of 13 cases of
SCSCC in which nuclear expression was seen in all cases, while focal labeling was seen in only 2/4 cutaneous
leiomyosarcomas and 2/10 atypical fibroxanthomas [16].
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
5/16
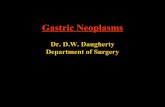
Figure 5. Ulcerating tumor infiltrates into the dermis and is composed of solid nests of squamoid cells as well as
pleomorphic spindle cells.
Figure 6. The squamoid cells blend into the spindle cells
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
6/16
Figure 7. Both epithelial and spindle cells are positive for CK AE 1/3 (Cytokeratin).
Figure 8. Both epithelial and spindle cells are positive for Vimentin.
Prognosis and Treatment
Spindle-cell squamous cell carcinoma is a poorly differentiated variant of squamous cell carcinoma with the potential
for an aggressive clinical course. One-third of cutaneous squamous cell carcinomas that metastasize are of this type.
Treatment is surgical. Metastases usually first occur to the regional lymph nodes.
Spindle Cell Atypical Fibroxan thom a.
Clinical Featur es
Atypical fibroxanthoma (AFX) usually arises in sun-exposed skin of the head and neck in older patients, often on the
nose and cheek. Therapeutic radiation is a predisposing factor, with tumors usually appearing more than a decade
following treatment. AFX usually presents as a nodule, which is sometimes ulcerated. The surface may be reddened
and polypoid, resembling a capillary hemangioma.
Histopathology (Figure s 9, 10)
AFX is a highly cellular mesenchymal tumor. There is an extensive proliferation of spindled to polygonal cells (Figures
9 and 10), which in the usual form closely resemble malignant fibrous histiocytoma (MFH) of the deep soft tissues.
AFX are expansile, dermal nodules that may reach the epidermis causing pressure atrophy. Often there is a
connection to the overlying epidermis. In other cases, an uninvolved portion of overlying dermis, or grenz zone, is
present. In addition, the tumor can compress skin appendages latererally. AFX does not extensively involve the
subcutis and does not invade deeper structures. Areas adjacent to the lesion may show solar elastosis, vascular
dilation, and capillary proliferation. Hemorrhage can be extensive, with the associated presence of hemosiderin-laden
macrophages. Scattered inflammatory cells can be seen. In contrast with the usual type of AFX, the spindle cell
variant is not pleomorphic, although most cases contain scattered giant cells of varying proportion [17, 18]. Sclerosis
may be prominent and the lesion may be active mitotically. This morphology creates diagnostic difficulties because of
its resemblance to other malignant spindle cell tumors. An absence of junctional nesting argues against malignant
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
7/16
melanoma, although caution must be taken as some spindle cell desmoplastic melanomas lack a junctional component.
Differentiation from spindle cell melanoma is suggested by lack of an overlying in-situ melanoma component and
absence of S-100 staining in tumor cells. The cells of AFX are HMB-45 negative (Table 1). Spindle cell carcinomas
show positive staining for cytokeratin and often keratinocyte dysplasia or Bowens disease is present at the edge of the
lesion. Leiomyosarcoma can be confused with this variant of AFX. AFX, however, is desmin negative and shows only
focal actin positivity. The neoplastic cells of AFX are positive for vimentin and CD68 (Figure 11). Matthew et al.
reported CK117 positivity in 15/16 AFX, suggesting that c-kit may be a sensitive marker [19].
Figure 9. Diffusely infiltrating dermal tumor.
Figure 10. The tumor is composed of predominantly pleomorphic polygonal cells.
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
8/16
Figure 11. Tumor cells show positivity with CD68 immunostain.
Prognosis and Treatment
Although AFX may be indistinguishable from MFH histologically, the prognosis is excellent following conservative
excision. Most authors agree that larger tumors (>2 cm) which extensively invade subcutaneous tissue such as fascia
or muscle, or show necrosis or vascular invasion, should be diagnosed as MFH. Lack of H-ras and K-ras mutations in
AFX but presence in MFH further suggest biologic differences between these two entities [20].
Derm atofibrosarcom a Protuberans.Clinical Featur es
Dermatofibrosarcoma protuberans (DFSP) is a neoplasm regarded as a superficial low-grade sarcoma. The lesion most
commonly presents in young to middle-aged persons on the trunk or proximal extremities as an indurated plaque
with one or more associated gray-white nodules. DFSP presents less often at other body sites, including the head,
neck, and distal extremities [21, 22]. Early lesions are sharply-demarcated or plaque-like, often with peripheral red or
blue discoloration. At this stage, lesions may clinically resemble morpheaform basal cell carcinoma. Advanced lesions
are fungating and ulcerated. Sometimes the tumors contain gelatinous or translucent areas corresponding
microscopically to myxoid change. Hemorrhage and cystic degeneration can occur.
DFSP exhibits slow and persistent growth, often over several years. There is evidence that many tumors develop
during childhood and become clinically apparent later in life. Congenital and childhood forms are known, but may not
come to attention early because of difficulty in clinical detection [23-25].
Histopathology (Figur es 12, 13, 14)
DFSP shows a dense proliferation of monotonous spindle cells that diffusely infiltrate the dermis and subcutis (Figure
12). The center of the tumor is composed of slender fibroblasts which contain moderately-enlarged, tapered nuclei and
are arranged around inconspicuous vessels in a distinctive storiform configuration (Figure 13). Occasional mitoses are
seen but are not abundant. Atypical forms are usually not seen. The tumor may extend to the epidermis or,
alternatively, a grenz zone is seen. Lateral extension of the tumor beyond the dermal component may be marked but
subtle. DFSP has a characteristic pattern of subcutaneous infiltration, including growth along septa and between
lipocytes in a honeycomb configuration or horizontally layered, parallel to the epidermal surface. Other findings in
DSFP are seen rarely, including multinucleated giant cells, hypercellular zones, and myoid or myofibroblastic
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
9/16
differentiation [26-28]. Occasional tumors contain myxoid areas, and when prominent, the storiform pattern becomes
less apparent. Unusual variants include sclerosing [29, 30] and pigmented types. Histology with a discrete fascicular or
herringbone pattern may suggest fibrosarcomatous transformation. The mitotic rate is usually, but not always,
higher when this occurs, although occasional examples of DFSP demonstrate up to 35 mitotic figures per high power
field [31]. It is currently unclear whether fibrosarcomatous areas are more common in recurrent lesions. Recent
studies have shown this not to be the case.
The tumor cells in DSFP stain immunohistochemically with CD34 (Figure 14), the human progenitor cell antigen, in a
significant proportion of its cells, making CD34 a highly sensitive marker for this entitiy. Care should be taken not to
interpret entrapped CD34 + dermal dendritic cells as tumor cells.
Almost all cases of DFSP express the chromosomal translocation t (17:22) when investigated with the newest
molecular techniques, including multiplex reverse transcription polymerase chain reaction (RT-PCR) and fluorescence
in situ hybridization (FISH) [32]. The translocation results in a fusion of the collagen type I I (COL1A1) gene on
chromosome 17 with the platelet-derived growth factor beta (PDGF) on chromosome 22 and is most commonly
located on a ring chromosome. The fusion transcript leads to constitutive activation of the PFGR protein tyrosine
kinase, resulting in uncontrolled tumor growth. DFSP has been found to differ from other soft tissue tumors with
similar histology by the expression of this distinct set of genes. In addition, PDGFBR, the receptor for PDGF, is highly
expressed in DFSP, suggesting an autocrine stimulatory loop that may contribute to tumorigenesis [33].
Figure 12. Diffuse monotonous spindle cell infiltration in dermis.
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
10/16
Figure 13. Storiform pattern
Figure 14. The tumor cells are strongly positive for CD34.
Prognosis and Treatment.
While generally indolent, the tumor possesses a tendency for progressive growth, recurrence, and rarely distant
metastasis. With wide excision and careful pathologic examination of surgical margins, even local recurrence is
extremely low [34]. In one large study of 218 DFSP patients, there was no significant difference in crude cumulative
incidence of local relapses between primary and recurrent disease and in cases with positive and negative margins
[35].
Fibrosarcomatous or malignant fibrous histiocytomatous transformation can occur, although the effect on the biologic
behavior of such a transformation is controversial. Adequacy of wide excision may be more important to prognosis
than the presence of the sarcomatous component per se [36-40]. Transformation to a fibrosarcomatous component
has been associated with microsatellite instability [41] and p53 mutations [41, 42].
Cutaneous Leiomyosarcoma.
Clinical Featur es
Primary leiomyosarcomas (LMS) of the skin are relatively rare sarcomas, reported infrequently in the literature. LMS
of the skin are divided into dermal and subcutaneous types. The dermal type is discussed here and tends to develop in
adults of middle to older age. It arises as one or several dermal or subcutaneous nodules, most often on the hip, thigh,
or knee [43]. Other locations, including the face and scrotum, are reported[44]. Many tumors are present for years
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
11/16
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
12/16
Figure 16. Higher magnification of the dermal spindle cell tumor.
Figure 17. The tumor cells are positive for SMA (smooth muscle antigen) on immunostain
Prognosis and Treatment
In a series of 65 primary cutaneous LMS reported by Fields et al. and in smaller series reported by other authors [46,
48], LMS can recur, sometimes due to incomplete surgical excision [51]. None metastasize, despite high mitotic
activity and marked cytologic atypia [53] in some cases. Recurrent tumors may be more atypical and located deeply
[51]. Reported cases of metastases appear in the older literature [54].
Summary
Spindle cell malignancies of the skin, some of which are not particularly common, are nevertheless seen by the
practicing dermatologists and pathologists. Such tumors are not always easily differentiated on histologic findings alone
and many, if not all, must be confirmed with immunohistochemical staining (Table 1). A thorough familiarity with
these lesions is a necessity, as prognosis and treatment may be different.
-
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
13/16
Table 1. Immunohistochemical Staining in Spindle Cell Malignancies of the Skin
Correspondence
Deba P Sarma, MD
Department of Pathology
Creighton University Medical Center
Omaha, Nebraska USA 68131
debasarma@creighton .edu
References
1. Conley, J., R. Lattes, and W. Orr, Desmoplastic malignant melanoma (a rare variant of spindle cell melanoma).
Cancer, 1971. 28(4): p. 914-36. (s)
2. From, L., et al., Origin of the desmoplasia in desmoplastic malignant melanoma. Hum Pathol, 1983. 14(12): p. 1072-
80. (s)
3. Busam, K.J., et al., Cutaneous desmoplastic melanoma: reappraisal of morphologic heterogeneity and prognostic
factors. Am J Surg Pathol, 2004. 28(11): p. 1518-25. (s)
4. McCarthy, S.W., R.A. Scolyer, and A.A. Palmer, Desmoplastic melanoma: a diagnostic trap for the unwary.Pathology, 2004. 36(5): p. 445-51. (s)
5. Cruz, J., J.S. Reis-Filho, and J.M. Lopes, Malignant peripheral nerve sheath tumour-like primary cutaneous
malignant melanoma. J Clin Pathol, 2004. 57(2): p. 218-20. (s)
6. Tsao, H., A.J. Sober, and R.L. Barnhill, Desmoplastic neurotropic melanoma. Semin Cutan Med Surg, 1997. 16(2): p.
131-6. (s)
7. Kossard, S., E. Doherty, and E. Murray, Neurotropic Melanoma. A variant of desmoplastic melanoma. Arch
Dermatol, 1987. 123(7): p. 907-12. (s)
8. Bruijn, J.A., et al., Desmoplastic melanoma: clinicopathologic aspects of six cases. Dermatology, 1992. 185(1): p. 3-8.
(s)
9. Emanuel, P.O., et al., Aggressive osteogenic desmoplastic melanoma: a case report. J Cutan Pathol, 2007. 34(5): p.
423-6. (s)
10. Hoang, M.P., et al., CD34 expression in desmoplastic melanoma. J Cutan Pathol, 2001. 28(10): p. 508-12. (s)
11. King, R., et al., Microphthalmia transcription factor expression in cutaneous benign, malignant melanocytic, and
nonmelanocytic tumors. Am J Surg Pathol, 2001. 25(1): p. 51-7. (s)
12. Granter, S.R., et al., Microphthalmia transcription factor: not a sensitive or specific marker for the diagnosis of
desmoplastic melanoma and spindle cell (non-desmoplastic) melanoma. Am J Dermatopathol, 2001. 23(3): p. 185-9.
(s)
13. Anstey, A., et al., Desmoplastic malignant melanoma. An immunocytochemical study of 25 cases. Am J
http://scholar.google.ca/scholar?q=Granter%2C%2BS.R.%2C%2Bet%2Bal.%2C%2BMicrophthalmia%2Btranscription%2Bfactor%3A%2Bnot%2Ba%2Bsensitive%2Bor%2Bspecific%2Bmarker%2Bfor%2Bthe%2Bdiagnosis%2Bof%2Bdesmoplastic%2Bmelanoma%2Band%2Bspindle%2Bcell%2B%28non-desmoplastic%29%2Bmelanoma.%2BAm%2BJ%2BDermatopathol%2C%2B2001.%2B23%283%29%3A%2Bp.%2B185-9.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=King%2C%2BR.%2C%2Bet%2Bal.%2C%2BMicrophthalmia%2Btranscription%2Bfactor%2Bexpression%2Bin%2Bcutaneous%2Bbenign%2C%2Bmalignant%2Bmelanocytic%2C%2Band%2Bnonmelanocytic%2Btumors.%2BAm%2BJ%2BSurg%2BPathol%2C%2B2001.%2B25%281%29%3A%2Bp.%2B51-7.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Hoang%2C%2BM.P.%2C%2Bet%2Bal.%2C%2BCD34%2Bexpression%2Bin%2Bdesmoplastic%2Bmelanoma.%2BJ%2BCutan%2BPathol%2C%2B2001.%2B28%2810%29%3A%2Bp.%2B508-12.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Emanuel%2C%2BP.O.%2C%2Bet%2Bal.%2C%2BAggressive%2Bosteogenic%2Bdesmoplastic%2Bmelanoma%3A%2Ba%2Bcase%2Breport.%2BJ%2BCutan%2BPathol%2C%2B2007.%2B34%285%29%3A%2Bp.%2B423-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Bruijn%2C%2BJ.A.%2C%2Bet%2Bal.%2C%2BDesmoplastic%2Bmelanoma%3A%2Bclinicopathologic%2Baspects%2Bof%2Bsix%2Bcases.%2BDermatology%2C%2B1992.%2B185%281%29%3A%2Bp.%2B3-8.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Kossard%2C%2BS.%2C%2BE.%2BDoherty%2C%2Band%2BE.%2BMurray%2C%2BNeurotropic%2BMelanoma.%2BA%2Bvariant%2Bof%2Bdesmoplastic%2Bmelanoma.%2BArch%2BDermatol%2C%2B1987.%2B123%287%29%3A%2Bp.%2B907-12.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Tsao%2C%2BH.%2C%2BA.J.%2BSober%2C%2Band%2BR.L.%2BBarnhill%2C%2BDesmoplastic%2Bneurotropic%2Bmelanoma.%2BSemin%2BCutan%2BMed%2BSurg%2C%2B1997.%2B16%282%29%3A%2Bp.%2B131-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Cruz%2C%2BJ.%2C%2BJ.S.%2BReis-Filho%2C%2Band%2BJ.M.%2BLopes%2C%2BMalignant%2Bperipheral%2Bnerve%2Bsheath%2Btumour-like%2Bprimary%2Bcutaneous%2Bmalignant%2Bmelanoma.%2BJ%2BClin%2BPathol%2C%2B2004.%2B57%282%29%3A%2Bp.%2B218-20.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=McCarthy%2C%2BS.W.%2C%2BR.A.%2BScolyer%2C%2Band%2BA.A.%2BPalmer%2C%2BDesmoplastic%2Bmelanoma%3A%2Ba%2Bdiagnostic%2Btrap%2Bfor%2Bthe%2Bunwary.%2BPathology%2C%2B2004.%2B36%285%29%3A%2Bp.%2B445-51.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Busam%2C%2BK.J.%2C%2Bet%2Bal.%2C%2BCutaneous%2Bdesmoplastic%2Bmelanoma%3A%2Breappraisal%2Bof%2Bmorphologic%2Bheterogeneity%2Band%2Bprognostic%2Bfactors.%2BAm%2BJ%2BSurg%2BPathol%2C%2B2004.%2B28%2811%29%3A%2Bp.%2B1518-25.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=From%2C%2BL.%2C%2Bet%2Bal.%2C%2BOrigin%2Bof%2Bthe%2Bdesmoplasia%2Bin%2Bdesmoplastic%2Bmalignant%2Bmelanoma.%2BHum%2BPathol%2C%2B1983.%2B14%2812%29%3A%2Bp.%2B1072-80.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Conley%2C%2BJ.%2C%2BR.%2BLattes%2C%2Band%2BW.%2BOrr%2C%2BDesmoplastic%2Bmalignant%2Bmelanoma%2B%28a%2Brare%2Bvariant%2Bof%2Bspindle%2Bcell%2Bmelanoma%29.%2BCancer%2C%2B1971.%2B28%284%29%3A%2Bp.%2B914-36.%0A&hl=en&lr=&btnG=Search -
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
14/16
Dermatopathol, 1994. 16(1): p. 14-22. (s)
14. Ohsie, S.J., et al., Immunohistochemical characteristics of melanoma. J Cutan Pathol, 2008. 35(5): p. 433-44. (s)
15. Attis, M.G., et al., Differential expression of N-cadherin distinguishes a subset of metastasizing desmoplastic
melanomas. Hum Pathol, 2006. 37(7): p. 899-905. (s)
16. Dotto, J.E. and E.J. Glusac, p63 is a useful marker for cutaneous spindle cell squamous cell carcinoma. J Cutan
Pathol, 2006. 33(6): p. 413-7. (s)
17. Longacre, T.A., B.R. Smoller, and R.V. Rouse, Atypical fibroxanthoma. Multiple immunohistologic profiles. Am J
Surg Pathol, 1993. 17(12): p. 1199-209. (s)
18. Bruecks, A.K., S.A. Medlicott, and M.J. Trotter, Atypical fibroxanthoma with prominent sclerosis. J Cutan Pathol,
2003. 30(5): p. 336-9. (s)
19. Mathew, R.A., et al., CD117 immunoreactivity in atypical fibroxanthoma. Am J Dermatopathol, 2008. 30(1): p. 34-
6. (s)
20. Sakamoto, A., et al., H-, K-, and N-ras gene mutation in atypical fibroxanthoma and malignant fibrous
histiocytoma. Hum Pathol, 2001. 32(11): p. 1225-31. (s)
21. Rabinowitz, L.G., et al., Acrally occurring dermatofibrosarcoma protuberans in children and adults. J Dermatol
Surg Oncol, 1994. 20(10): p. 655-9. (s)
22. Mizushima, J., et al., Dermatofibrosarcoma protuberans of the sole. Dermatology, 1996. 192(3): p. 280-2. (s)
23. Maire, G., et al., A clinical, histologic, and molecular study of 9 cases of congenital dermatofibrosarcoma
protuberans. Arch Dermatol, 2007. 143(2): p. 203-10. (s)
24. Martin, L., et al., The atrophic variant of dermatofibrosarcoma protuberans in childhood: a report of six cases. Br J
Dermatol, 1998. 139(4): p. 719-25. (s)
25. Weinstein, J.M., et al., Congenital dermatofibrosarcoma protuberans: variability in presentation. Arch Dermatol,
2003. 139(2): p. 207-1 1. (s)
26. Sigel, J.E., W.F. Bergfeld, and J.R. Goldblum, A morphologic study of dermatofibrosarcoma protuberans: expansion
of a histologic profile. J Cutan Pathol, 2000. 27(4): p. 159-63. (s)
27. Llatjos, R., et al., Palisading and verocay body-prominent dermatofibrosarcoma protuberans: a report of three
cases. Histopathology, 2000. 37(5): p. 452-5. (s)
28. Oliveira-Soares, R., et al., Dermatofibrosarcoma protuberans: a clinicopathological study of 20 cases. J Eur Acad
Dermatol Venereol, 2002. 16(5): p. 441-6. (s)
29. Sabater- Marco, V., et al., Sclerosing dermatofibrosarcoma protuberans (DFSP): an unusual variant with focus on
the histopathologic differential diagnosis. Int J Dermatol, 2006. 45(1): p. 59-62. (s)
30. Diaz-Cascajo, C., W. Weyers, and S. Borghi, Sclerosing dermatofibrosarcoma protuberans. J Cutan Pathol, 1998. 25
(8): p. 440-4. (s)
31. Connelly, J.H. and H.L. Evans, Dermatofibrosarcoma protuberans. A clinicopathologic review with emphasis on
fibrosarcomatous areas. Am J Surg Pathol, 1992. 16(10): p. 921-5. (s)
32. Patel, K.U., et al., Dermatofibrosarcoma protuberans COL1A1-PDGFB fusion is identified in virtually all
dermatofibrosarcoma protuberans cases when investigated by newly developed multiplex reverse transcription
polymerase chain reaction and fluorescence in situ hybridization assays. Hum Pathol, 2008. 39(2): p. 184-93. (s)
http://scholar.google.ca/scholar?q=Patel%2C%2BK.U.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%2BCOL1A1-PDGFB%2Bfusion%2Bis%2Bidentified%2Bin%2Bvirtually%2Ball%2Bdermatofibrosarcoma%2Bprotuberans%2Bcases%2Bwhen%2Binvestigated%2Bby%2Bnewly%2Bdeveloped%2Bmultiplex%2Breverse%2Btranscription%2Bpolymerase%2Bchain%2Breaction%2Band%2Bfluorescence%2Bin%2Bsitu%2Bhybridization%2Bassays.%2BHum%2BPathol%2C%2B2008.%2B39%282%29%3A%2Bp.%2B184-93.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Connelly%2C%2BJ.H.%2Band%2BH.L.%2BEvans%2C%2BDermatofibrosarcoma%2Bprotuberans.%2BA%2Bclinicopathologic%2Breview%2Bwith%2Bemphasis%2Bon%2Bfibrosarcomatous%2Bareas.%2BAm%2BJ%2BSurg%2BPathol%2C%2B1992.%2B16%2810%29%3A%2Bp.%2B921-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Diaz-Cascajo%2C%2BC.%2C%2BW.%2BWeyers%2C%2Band%2BS.%2BBorghi%2C%2BSclerosing%2Bdermatofibrosarcoma%2Bprotuberans.%2BJ%2BCutan%2BPathol%2C%2B1998.%2B25%288%29%3A%2Bp.%2B440-4.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Sabater-Marco%2C%2BV.%2C%2Bet%2Bal.%2C%2BSclerosing%2Bdermatofibrosarcoma%2Bprotuberans%2B%28DFSP%29%3A%2Ban%2Bunusual%2Bvariant%2Bwith%2Bfocus%2Bon%2Bthe%2Bhistopathologic%2Bdifferential%2Bdiagnosis.%2BInt%2BJ%2BDermatol%2C%2B2006.%2B45%281%29%3A%2Bp.%2B59-62.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Oliveira-Soares%2C%2BR.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%3A%2Ba%2Bclinicopathological%2Bstudy%2Bof%2B20%2Bcases.%2BJ%2BEur%2BAcad%2BDermatol%2BVenereol%2C%2B2002.%2B16%285%29%3A%2Bp.%2B441-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Llatjos%2C%2BR.%2C%2Bet%2Bal.%2C%2BPalisading%2Band%2Bverocay%2Bbody-prominent%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Ba%2Breport%2Bof%2Bthree%2Bcases.%2BHistopathology%2C%2B2000.%2B37%285%29%3A%2Bp.%2B452-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Sigel%2C%2BJ.E.%2C%2BW.F.%2BBergfeld%2C%2Band%2BJ.R.%2BGoldblum%2C%2BA%2Bmorphologic%2Bstudy%2Bof%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Bexpansion%2Bof%2Ba%2Bhistologic%2Bprofile.%2BJ%2BCutan%2BPathol%2C%2B2000.%2B27%284%29%3A%2Bp.%2B159-63.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Weinstein%2C%2BJ.M.%2C%2Bet%2Bal.%2C%2BCongenital%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Bvariability%2Bin%2Bpresentation.%2BArch%2BDermatol%2C%2B2003.%2B139%282%29%3A%2Bp.%2B207-11.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Martin%2C%2BL.%2C%2Bet%2Bal.%2C%2BThe%2Batrophic%2Bvariant%2Bof%2Bdermatofibrosarcoma%2Bprotuberans%2Bin%2Bchildhood%3A%2Ba%2Breport%2Bof%2Bsix%2Bcases.%2BBr%2BJ%2BDermatol%2C%2B1998.%2B139%284%29%3A%2Bp.%2B719-25.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Maire%2C%2BG.%2C%2Bet%2Bal.%2C%2BA%2Bclinical%2C%2Bhistologic%2C%2Band%2Bmolecular%2Bstudy%2Bof%2B9%2Bcases%2Bof%2Bcongenital%2Bdermatofibrosarcoma%2Bprotuberans.%2BArch%2BDermatol%2C%2B2007.%2B143%282%29%3A%2Bp.%2B203-10.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Mizushima%2C%2BJ.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%2Bof%2Bthe%2Bsole.%2BDermatology%2C%2B1996.%2B192%283%29%3A%2Bp.%2B280-2.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Rabinowitz%2C%2BL.G.%2C%2Bet%2Bal.%2C%2BAcrally%2Boccurring%2Bdermatofibrosarcoma%2Bprotuberans%2Bin%2Bchildren%2Band%2Badults.%2BJ%2BDermatol%2BSurg%2BOncol%2C%2B1994.%2B20%2810%29%3A%2Bp.%2B655-9.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Sakamoto%2C%2BA.%2C%2Bet%2Bal.%2C%2BH-%2C%2BK-%2C%2Band%2BN-ras%2Bgene%2Bmutation%2Bin%2Batypical%2Bfibroxanthoma%2Band%2Bmalignant%2Bfibrous%2Bhistiocytoma.%2BHum%2BPathol%2C%2B2001.%2B32%2811%29%3A%2Bp.%2B1225-31.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Mathew%2C%2BR.A.%2C%2Bet%2Bal.%2C%2BCD117%2Bimmunoreactivity%2Bin%2Batypical%2Bfibroxanthoma.%2BAm%2BJ%2BDermatopathol%2C%2B2008.%2B30%281%29%3A%2Bp.%2B34-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Bruecks%2C%2BA.K.%2C%2BS.A.%2BMedlicott%2C%2Band%2BM.J.%2BTrotter%2C%2BAtypical%2Bfibroxanthoma%2Bwith%2Bprominent%2Bsclerosis.%2BJ%2BCutan%2BPathol%2C%2B2003.%2B30%285%29%3A%2Bp.%2B336-9.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Longacre%2C%2BT.A.%2C%2BB.R.%2BSmoller%2C%2Band%2BR.V.%2BRouse%2C%2BAtypical%2Bfibroxanthoma.%2BMultiple%2Bimmunohistologic%2Bprofiles.%2BAm%2BJ%2BSurg%2BPathol%2C%2B1993.%2B17%2812%29%3A%2Bp.%2B1199-209.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Dotto%2C%2BJ.E.%2Band%2BE.J.%2BGlusac%2C%2Bp63%2Bis%2Ba%2Buseful%2Bmarker%2Bfor%2Bcutaneous%2Bspindle%2Bcell%2Bsquamous%2Bcell%2Bcarcinoma.%2BJ%2BCutan%2BPathol%2C%2B2006.%2B33%286%29%3A%2Bp.%2B413-7.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Attis%2C%2BM.G.%2C%2Bet%2Bal.%2C%2BDifferential%2Bexpression%2Bof%2BN-cadherin%2Bdistinguishes%2Ba%2Bsubset%2Bof%2Bmetastasizing%2Bdesmoplastic%2Bmelanomas.%2BHum%2BPathol%2C%2B2006.%2B37%287%29%3A%2Bp.%2B899-905.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Ohsie%2C%2BS.J.%2C%2Bet%2Bal.%2C%2BImmunohistochemical%2Bcharacteristics%2Bof%2Bmelanoma.%2BJ%2BCutan%2BPathol%2C%2B2008.%2B35%285%29%3A%2Bp.%2B433-44.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Anstey%2C%2BA.%2C%2Bet%2Bal.%2C%2BDesmoplastic%2Bmalignant%2Bmelanoma.%2BAn%2Bimmunocytochemical%2Bstudy%2Bof%2B25%2Bcases.%2BAm%2BJ%2BDermatopathol%2C%2B1994.%2B16%281%29%3A%2Bp.%2B14-22.%0A&hl=en&lr=&btnG=Search -
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
15/16
33. Linn, S.C., et al., Gene expression patterns and gene copy number changes in dermatofibrosarcoma protuberans.
Am J Pathol, 2003. 163(6): p. 2383-95. (s)
34. DuBay, D., et al., Low recurrence rate after surgery for dermatofibrosarcoma protuberans: a multidisciplinary
approach from a single institution. Cancer, 2004. 100(5): p. 1008-16. (s)
35. Fiore, M., et al., Dermatofibrosarcoma protuberans treated at a single institution: a surgical disease with a high
cure rate. J Clin Oncol, 2005. 23(30): p. 7669-75. (s)
36. Szollosi, Z. and Z. Nemes, Transformed dermatofibrosarcoma protuberans: a clinicopathological study of eight
cases. J Clin Pathol, 2005. 58(7): p. 751-6. (s)
37. Abbott, J.J., A.M. Oliveira, and A.G. Nascimento, The prognostic significance of fibrosarcomatous transformation in
dermatofibrosarcoma protuberans. Am J Surg Pathol, 2006. 30(4): p. 436-43. (s)
38. Szollosi, Z., et al., Transformed dermatofibrosarcoma protuberans: real time polymerase chain reaction detection
of COL1A1-PDGFB fusion transcripts in sarcomatous areas. J Clin Pathol, 2007. 60(2): p. 190-4. (s)
39. Diaz-Cascajo, C., et al., Dermatofibrosarcoma protuberans with fibrosarcomatous areas: a clinico-pathologic and
immunohistochemic study in four cases. Am J Dermatopathol, 1997. 19(6): p. 562-7. (s)
40. Mentzel, T., et al., Fibrosarcomatous ("high-grade") dermatofibrosarcoma protuberans: clinicopathologic and
immunohistochemical study of a series of 41 cases with emphasis on prognostic significance. Am J Surg Pathol, 1998.
22(5): p. 576-87. (s)
41. Takahira, T., et al., Microsatellite instability and p53 mutation associated with tumor progression in
dermatofibrosarcoma protuberans. Hum Pathol, 2004. 35(2): p. 240-5. (s)
42. Sasaki, M., et al., Dermatofibrosarcoma protuberans: an analysis of proliferative activity, DNA flow cytometry and
p53 overexpression with emphasis on its progression. Pathol Int, 1999. 49(9): p. 799-806. (s)
43. Jensen, M.L., et al., Intradermal and subcutaneous leiomyosarcoma: a clinicopathological and
immunohistochemical study of 41 cases. J Cutan Pathol, 1996. 23(5): p. 458-63. (s)
44. Limaiem, F., et al., Primary cutaneous leiomyosarcoma: a histological and immunohistochemical study of 4 cases.
Pathologica, 2007. 99(6): p. 415-9. (s)
45. Chow, J., et al., Cutaneous leiomyosarcoma: case reports and review of the literature. Ann Plast Surg, 1987. 18(4):
p. 319-22. (s)
46. Kaddu, S., et al., Cutaneous leiomyosarcoma. Am J Surg Pathol, 1997. 21(9): p. 979-87. (s)
47. Karroum, J.E., E.G. Zappi, and C.J. Cockerell, Sclerotic primary cutaneous leiomyosarcoma. Am J Dermatopathol,
1995. 17(3): p. 292-6. (s)
48. Valeriani, M., etal., Recurrent cutaneous leiomyosarcoma. J Exp Clin Cancer Res, 1998. 17(1): p. 83-5. (s)
49. Berzal-Cantalejo, F., et al., Desmoplastic cutaneous leiomyosarcoma: case report and review of the literature. J
Cutan Pathol, 2006. 33 Suppl 2: p. 29-31. (s)
50. Choy, C., A. Cooper, and S. Kossard, Primary cutaneous diffuse leiomyosarcoma with desmoplasia. Australas J
Dermatol, 2006. 47(4): p. 291-5. (s)
51. Bellezza, G., et al., Primary cutaneous leiomyosarcoma: a clinicopathological and immunohistochemical study of 7
cases. Int J Surg Pathol, 2004. 12(1): p. 39-44. (s)
52. Swanson, P.E., et al., Primary cutaneous leiomyosarcoma. A histological and immunohistochemical study of 9 cases,
with ultrastructural correlation. J Cutan Pathol, 1988. 15(3): p. 129-41. (s)
http://scholar.google.ca/scholar?q=Szollosi%2C%2BZ.%2Band%2BZ.%2BNemes%2C%2BTransformed%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Ba%2Bclinicopathological%2Bstudy%2Bof%2Beight%2Bcases.%2BJ%2BClin%2BPathol%2C%2B2005.%2B58%287%29%3A%2Bp.%2B751-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Diaz-Cascajo%2C%2BC.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%2Bwith%2Bfibrosarcomatous%2Bareas%3A%2Ba%2Bclinico-pathologic%2Band%2Bimmunohistochemic%2Bstudy%2Bin%2Bfour%2Bcases.%2BAm%2BJ%2BDermatopathol%2C%2B1997.%2B19%286%29%3A%2Bp.%2B562-7.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Takahira%2C%2BT.%2C%2Bet%2Bal.%2C%2BMicrosatellite%2Binstability%2Band%2Bp53%2Bmutation%2Bassociated%2Bwith%2Btumor%2Bprogression%2Bin%2Bdermatofibrosarcoma%2Bprotuberans.%2BHum%2BPathol%2C%2B2004.%2B35%282%29%3A%2Bp.%2B240-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Swanson%2C%2BP.E.%2C%2Bet%2Bal.%2C%2BPrimary%2Bcutaneous%2Bleiomyosarcoma.%2BA%2Bhistological%2Band%2Bimmunohistochemical%2Bstudy%2Bof%2B9%2Bcases%2C%2Bwith%2Bultrastructural%2Bcorrelation.%2BJ%2BCutan%2BPathol%2C%2B1988.%2B15%283%29%3A%2Bp.%2B129-41.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Bellezza%2C%2BG.%2C%2Bet%2Bal.%2C%2BPrimary%2Bcutaneous%2Bleiomyosarcoma%3A%2Ba%2Bclinicopathological%2Band%2Bimmunohistochemical%2Bstudy%2Bof%2B7%2Bcases.%2BInt%2BJ%2BSurg%2BPathol%2C%2B2004.%2B12%281%29%3A%2Bp.%2B39-44.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Choy%2C%2BC.%2C%2BA.%2BCooper%2C%2Band%2BS.%2BKossard%2C%2BPrimary%2Bcutaneous%2Bdiffuse%2Bleiomyosarcoma%2Bwith%2Bdesmoplasia.%2BAustralas%2BJ%2BDermatol%2C%2B2006.%2B47%284%29%3A%2Bp.%2B291-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Berzal-Cantalejo%2C%2BF.%2C%2Bet%2Bal.%2C%2BDesmoplastic%2Bcutaneous%2Bleiomyosarcoma%3A%2Bcase%2Breport%2Band%2Breview%2Bof%2Bthe%2Bliterature.%2BJ%2BCutan%2BPathol%2C%2B2006.%2B33%2BSuppl%2B2%3A%2Bp.%2B29-31.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Valeriani%2C%2BM.%2C%2Bet%2Bal.%2C%2BRecurrent%2Bcutaneous%2Bleiomyosarcoma.%2BJ%2BExp%2BClin%2BCancer%2BRes%2C%2B1998.%2B17%281%29%3A%2Bp.%2B83-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Karroum%2C%2BJ.E.%2C%2BE.G.%2BZappi%2C%2Band%2BC.J.%2BCockerell%2C%2BSclerotic%2Bprimary%2Bcutaneous%2Bleiomyosarcoma.%2BAm%2BJ%2BDermatopathol%2C%2B1995.%2B17%283%29%3A%2Bp.%2B292-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Kaddu%2C%2BS.%2C%2Bet%2Bal.%2C%2BCutaneous%2Bleiomyosarcoma.%2BAm%2BJ%2BSurg%2BPathol%2C%2B1997.%2B21%289%29%3A%2Bp.%2B979-87.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Chow%2C%2BJ.%2C%2Bet%2Bal.%2C%2BCutaneous%2Bleiomyosarcoma%3A%2Bcase%2Breports%2Band%2Breview%2Bof%2Bthe%2Bliterature.%2BAnn%2BPlast%2BSurg%2C%2B1987.%2B18%284%29%3A%2Bp.%2B319-22.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Limaiem%2C%2BF.%2C%2Bet%2Bal.%2C%2BPrimary%2Bcutaneous%2Bleiomyosarcoma%3A%2Ba%2Bhistological%2Band%2Bimmunohistochemical%2Bstudy%2Bof%2B4%2Bcases.%2BPathologica%2C%2B2007.%2B99%286%29%3A%2Bp.%2B415-9.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Jensen%2C%2BM.L.%2C%2Bet%2Bal.%2C%2BIntradermal%2Band%2Bsubcutaneous%2Bleiomyosarcoma%3A%2Ba%2Bclinicopathological%2Band%2Bimmunohistochemical%2Bstudy%2Bof%2B41%2Bcases.%2BJ%2BCutan%2BPathol%2C%2B1996.%2B23%285%29%3A%2Bp.%2B458-63.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Sasaki%2C%2BM.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%3A%2Ban%2Banalysis%2Bof%2Bproliferative%2Bactivity%2C%2BDNA%2Bflow%2Bcytometry%2Band%2Bp53%2Boverexpression%2Bwith%2Bemphasis%2Bon%2Bits%2Bprogression.%2BPathol%2BInt%2C%2B1999.%2B49%289%29%3A%2Bp.%2B799-806.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Takahira%2C%2BT.%2C%2Bet%2Bal.%2C%2BMicrosatellite%2Binstability%2Band%2Bp53%2Bmutation%2Bassociated%2Bwith%2Btumor%2Bprogression%2Bin%2Bdermatofibrosarcoma%2Bprotuberans.%2BHum%2BPathol%2C%2B2004.%2B35%282%29%3A%2Bp.%2B240-5.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Mentzel%2C%2BT.%2C%2Bet%2Bal.%2C%2BFibrosarcomatous%2B%28%22high-grade%22%29%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Bclinicopathologic%2Band%2Bimmunohistochemical%2Bstudy%2Bof%2Ba%2Bseries%2Bof%2B41%2Bcases%2Bwith%2Bemphasis%2Bon%2Bprognostic%2Bsignificance.%2BAm%2BJ%2BSurg%2BPathol%2C%2B1998.%2B22%285%29%3A%2Bp.%2B576-87.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Diaz-Cascajo%2C%2BC.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%2Bwith%2Bfibrosarcomatous%2Bareas%3A%2Ba%2Bclinico-pathologic%2Band%2Bimmunohistochemic%2Bstudy%2Bin%2Bfour%2Bcases.%2BAm%2BJ%2BDermatopathol%2C%2B1997.%2B19%286%29%3A%2Bp.%2B562-7.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Szollosi%2C%2BZ.%2C%2Bet%2Bal.%2C%2BTransformed%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Breal%2Btime%2Bpolymerase%2Bchain%2Breaction%2Bdetection%2Bof%2BCOL1A1-PDGFB%2Bfusion%2Btranscripts%2Bin%2Bsarcomatous%2Bareas.%2BJ%2BClin%2BPathol%2C%2B2007.%2B60%282%29%3A%2Bp.%2B190-4.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Abbott%2C%2BJ.J.%2C%2BA.M.%2BOliveira%2C%2Band%2BA.G.%2BNascimento%2C%2BThe%2Bprognostic%2Bsignificance%2Bof%2Bfibrosarcomatous%2Btransformation%2Bin%2Bdermatofibrosarcoma%2Bprotuberans.%2BAm%2BJ%2BSurg%2BPathol%2C%2B2006.%2B30%284%29%3A%2Bp.%2B436-43.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Szollosi%2C%2BZ.%2Band%2BZ.%2BNemes%2C%2BTransformed%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Ba%2Bclinicopathological%2Bstudy%2Bof%2Beight%2Bcases.%2BJ%2BClin%2BPathol%2C%2B2005.%2B58%287%29%3A%2Bp.%2B751-6.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Fiore%2C%2BM.%2C%2Bet%2Bal.%2C%2BDermatofibrosarcoma%2Bprotuberans%2Btreated%2Bat%2Ba%2Bsingle%2Binstitution%3A%2Ba%2Bsurgical%2Bdisease%2Bwith%2Ba%2Bhigh%2Bcure%2Brate.%2BJ%2BClin%2BOncol%2C%2B2005.%2B23%2830%29%3A%2Bp.%2B7669-75.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=DuBay%2C%2BD.%2C%2Bet%2Bal.%2C%2BLow%2Brecurrence%2Brate%2Bafter%2Bsurgery%2Bfor%2Bdermatofibrosarcoma%2Bprotuberans%3A%2Ba%2Bmultidisciplinary%2Bapproach%2Bfrom%2Ba%2Bsingle%2Binstitution.%2BCancer%2C%2B2004.%2B100%285%29%3A%2Bp.%2B1008-16.%0A&hl=en&lr=&btnG=Searchhttp://scholar.google.ca/scholar?q=Linn%2C%2BS.C.%2C%2Bet%2Bal.%2C%2BGene%2Bexpression%2Bpatterns%2Band%2Bgene%2Bcopy%2Bnumber%2Bchanges%2Bin%2Bdermatofibrosarcoma%2Bprotuberans.%2BAm%2BJ%2BPathol%2C%2B2003.%2B163%286%29%3A%2Bp.%2B2383-95.%0A&hl=en&lr=&btnG=Search -
8/14/2019 DR SARMA'S DERMPATH: Common Spindle Cell Malignant Neoplasms of the Skin Differential Diagnosis and Review of the Literature. The Internet Journal o
16/16