Dr Nicole Hancock - Royal Hobart Hospital - Clinical Redesign & Patient Flow Through ED
52
Dr Nicole Hancock Emergency Department Management Conference 16 July 2015
-
Upload
informa-australia -
Category
Healthcare
-
view
67 -
download
2
Transcript of Dr Nicole Hancock - Royal Hobart Hospital - Clinical Redesign & Patient Flow Through ED
Dr Nicole HancockEmergency Department Management Conference
16 July 2015
Background- our hospital and ED
Royal Hobart Hospital- physical evolution
The evolving inpatient clinician here today
Inpatient species
Some stories of evolution of the species
Key drivers for evolution

• Australia’s second oldest hospital.
• Tasmania’s largest hospital and its major referral centre at tertiary level.
• Provides acute, sub acute, mental health and aged care inpatient and ambulatory services
• 550 beds: 460 acute overnight and 90 day beds.

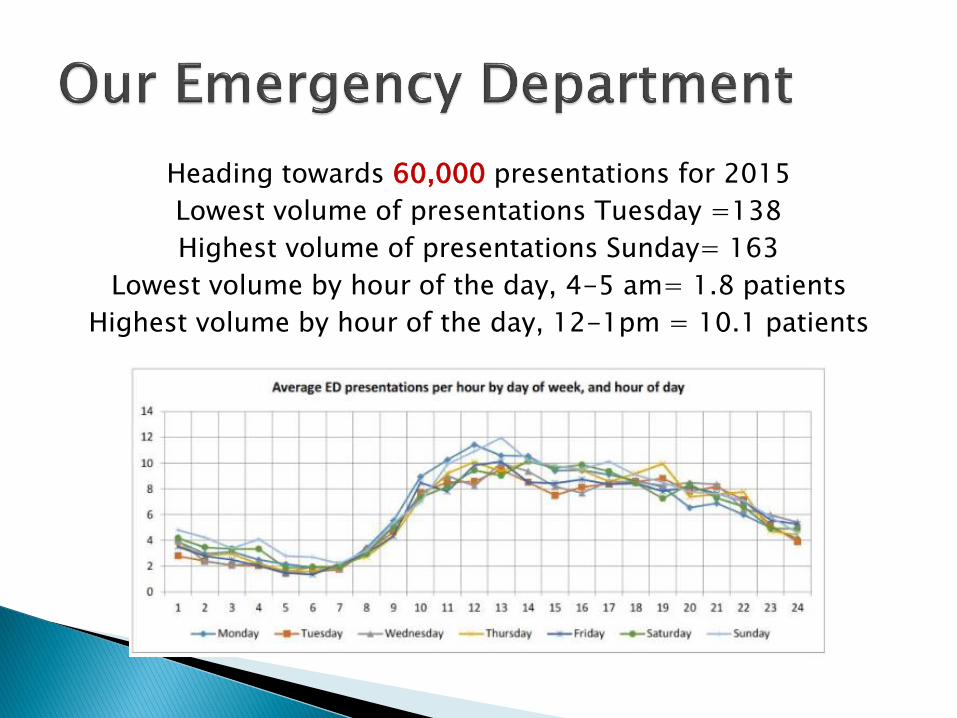
Heading towards 60,000 presentations for 2015
Lowest volume of presentations Tuesday =138
Highest volume of presentations Sunday= 163
Lowest volume by hour of the day, 4-5 am= 1.8 patients
Highest volume by hour of the day, 12-1pm = 10.1 patients
Discharged patient group 59.8%
Admitted patient group are 34.1% of presentations
Did not wait 4.2%
ADMITTED TO:26 % EMU = ED short stay unit
22% General Medicine9% General Surgery
6 % Paediatrics6% Psychiatry
Constantly evolving to meet the continuing challenges of increased presentations, inpatient
bed access, ambulance ramping etc
NEAT funding and other initiatives (largely with $$$) have partly driven this evolution
Tasmanian born and bred
UTAS graduate- MBBS 1993
Specialist Qualification 2001- General Physician
Returned to RHH- various roles over this period
Currently- Head of Department, General Medicine and Assessment and Planning Unit
Clinical Lead in Clinical Redesign, RHH.


Early in career:
a lot of decisions/interactions were driven by the desire to please and to belong
Self-absorbed, petulant
Now:
not shy of raising the difficult and challenging questions
trusted
develops relationships leading to benefits for individuals and also the service and patients.

It is because there is a wide variety of inpatient species (in our workforce)
AND in my opinion, one of Clinical Redesigns’ goals is to assist evolution of the species…….

Regularly forget that they work in a hospital with an Emergency Department
Struggles to find their way to the ED
No knowledge of risks linked to prolonged ED journey time for inpatients or need for inpatient responsiveness
Delights in retelling anecdotes from a decade ago relating to ED and apparent poor performance

Goes into ED regularly, knows most of the senior staff
Works in a unit/department where others have ignoramus-traits
Trying to get the team to see the bigger picture with significant resistance
Frustrated/despondent- hopefully can see if they can become trainee supervisor, there may be some hope!
Visits the ED occasionally
Understands the risks of prolonged inpatient journeys in ED and importance of inpatient responsiveness
Explores in some detail reports from inpatient teams of issues with ED
Often unaware of all the good things happening in ED
May often be in a senior role in the hospital
Sends out directives to ask others to act
Physically struggling to walk the walk and walk the talk thus limiting effectiveness

Knows the ED and staff well- likes to visit “just to chat”
Often critical of inpatient colleagues in this setting
Understands the risks of prolonged inpatient journeys in ED and importance of inpatient responsiveness
(Probably should have done ED training!)
Comes to work to do their best and attempts to be “friends” with everyone- quite a likeable person
Some lonerangerus traits but more like a “dog with a bone”
Gets frustrated easily, limiting effectiveness
In ED regularly
Understands the risks of prolonged inpatient journeys in ED and importance of inpatient responsiveness
Gets in there and walks the walk and walks the talk when on duty
May be in a team where lonerangerus traits can evolve BUT if has traits of the directivus, may have quite a chance of getting others to walk the talk/evolve.

Knows where ED is and visits intermittently.
Understands the risks of prolonged inpatientjourneys in ED and importance of inpatientresponsiveness
Often in a senior role
Truly believes people are doing all the rightthings when it comes to inpatientresponsiveness to ED

Rarely visits ED. Has heard a bit about the dangers of ED for
inpatients and blames ED for this. Thinks ED hold onto patients too long YET
insists that ED should not make a referral until they know what is going on.
Believes ED regularly rings the wrong unit for inpatient referrals
Requests “serum rhubarb” (and the result) before agreeing to come and see an inpatient in ED
Visits ED regularly
Understands the risks of prolonged inpatient journeys in ED and importance of inpatient responsiveness
Do not believe they can make a difference
Lacking in self-confidence
Thrives in a group with other species and high chance of evolution
THE LIST COULD GO ON……

What does this all mean?
Why does it matter?
Clinical champions from the inpatient group.
Important to identify the different traits Engage a group of people with diverse traits Bringing diverse traits together can increase
effectiveness and speed evolution of thoughts and actions
Critical to identify are:
Those with predominant traits of the Walkthetalkituswith a bit of Lonerangerus who can draw on some of theDirectivus traits when needed.
To demonstrate evolution of the inpatient species, I would like to. tell a couple of stories
We identified a resistant group of Ignorami.
We joined them up with a Walkthetalkitus.
We did not start with the topic of ED.


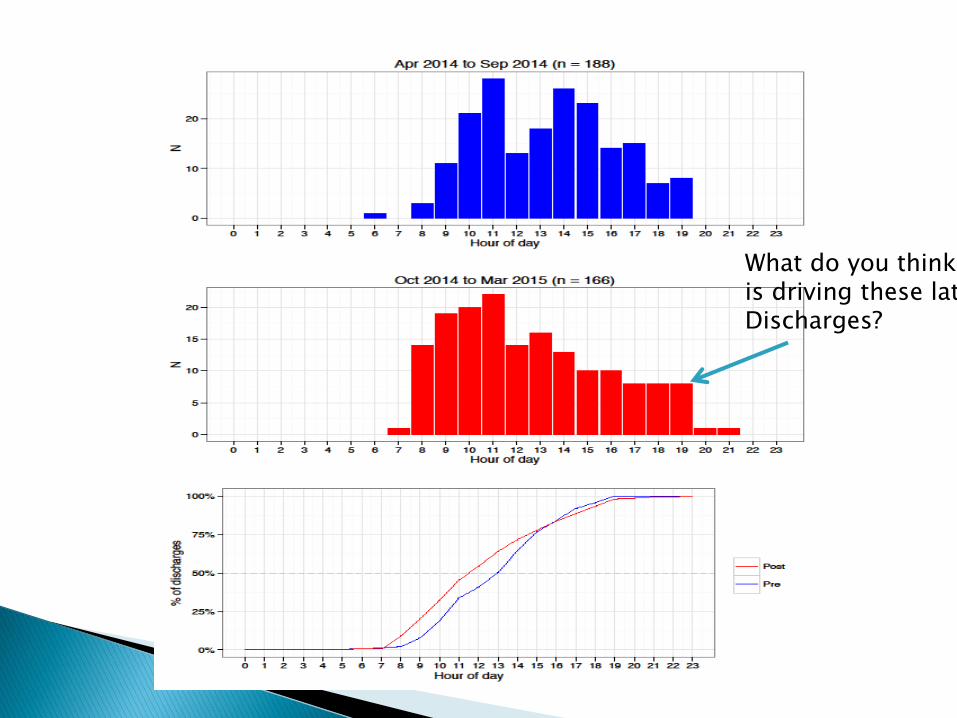
What do you thinkis driving these lateDischarges?

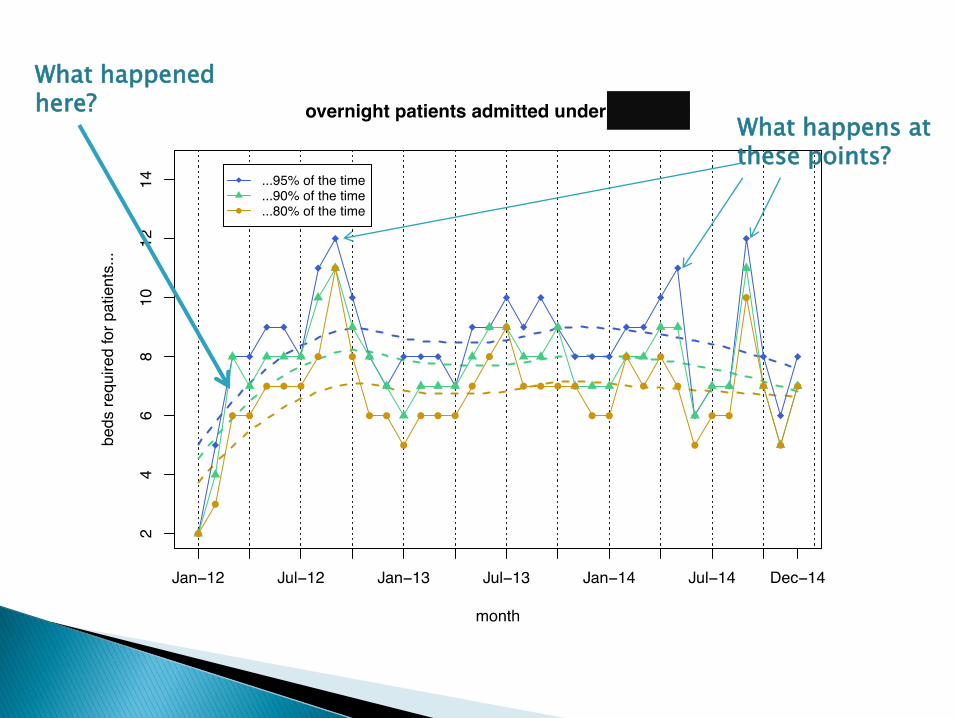
What happenedhere?
What happens atthese points?

Dear Nicole,
Could you please clarify:
Today we have a 54yo man without co-morbidities who needs a procedure within the next day or so.The inpatient service who perform that procedure has asked for the patient to be admitted under general medicine and advised that they will do the procedure during the admission.
I would like confirmation that: This is current admission policy This is an appropriate patient centred approach to a
patient with a single system problem.

Ignorami
+ data
+ wanting to do better
+ feedback
= building trust
= push the boundaries, start asking the hard questions
=evolution
We identified a significantly influential head of unitthat believed that their registrars see ED inpatientreferrals within 15 minutes.
He also believed that ED were regularly referringinappropriate patients to their service.
We joined some Lonerangeri together to come upwith a way to evaluate these beliefs and developsome ideas on how to “myth bust”

46
Start of 2nd referral
Triage to
Decision to
Admit
Request for
Admission
Accepted for
Admission
In-patient
Team
Review
Patient
Ready
Transfer to
Inpatient
Bed
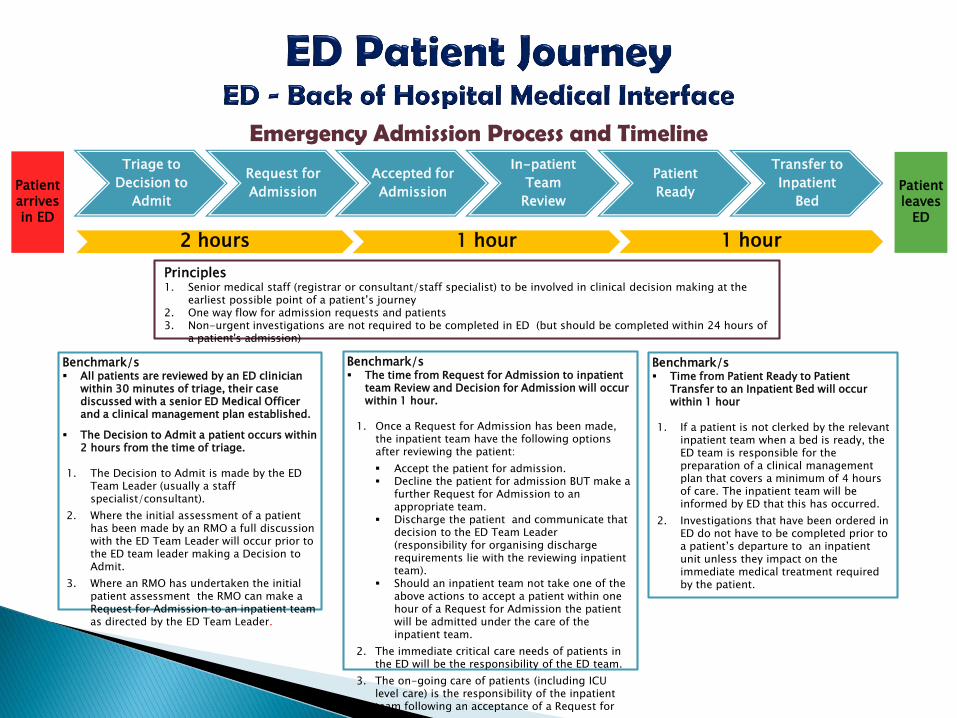
Emergency Admission Process and Timeline
Benchmark/s All patients are reviewed by an ED clinician
within 30 minutes of triage, their case discussed with a senior ED Medical Officer and a clinical management plan established.
The Decision to Admit a patient occurs within 2 hours from the time of triage.
1. The Decision to Admit is made by the ED Team Leader (usually a staff specialist/consultant).
2. Where the initial assessment of a patient has been made by an RMO a full discussion with the ED Team Leader will occur prior to the ED team leader making a Decision to Admit.
3. Where an RMO has undertaken the initial patient assessment the RMO can make a Request for Admission to an inpatient team as directed by the ED Team Leader.
Principles1. Senior medical staff (registrar or consultant/staff specialist) to be involved in clinical decision making at the
earliest possible point of a patient’s journey2. One way flow for admission requests and patients3. Non-urgent investigations are not required to be completed in ED (but should be completed within 24 hours of
a patient's admission)
Patient arrives in ED
Patient leaves
ED
2 hours 1 hour 1 hour
Benchmark/s The time from Request for Admission to inpatient
team Review and Decision for Admission will occur within 1 hour.
1. Once a Request for Admission has been made, the inpatient team have the following options after reviewing the patient:
Accept the patient for admission. Decline the patient for admission BUT make a
further Request for Admission to an appropriate team.
Discharge the patient and communicate that decision to the ED Team Leader (responsibility for organising discharge requirements lie with the reviewing inpatient team).
Should an inpatient team not take one of the above actions to accept a patient within one hour of a Request for Admission the patient will be admitted under the care of the inpatient team.
2. The immediate critical care needs of patients in the ED will be the responsibility of the ED team.
3. The on-going care of patients (including ICU level care) is the responsibility of the inpatient team following an acceptance of a Request for Admission.
Benchmark/s Time from Patient Ready to Patient
Transfer to an Inpatient Bed will occur within 1 hour
1. If a patient is not clerked by the relevant inpatient team when a bed is ready, the ED team is responsible for the preparation of a clinical management plan that covers a minimum of 4 hours of care. The inpatient team will be informed by ED that this has occurred.
2. Investigations that have been ordered in ED do not have to be completed prior to a patient’s departure to an inpatient unit unless they impact on the immediate medical treatment required by the patient.
Delusio
+ data
+ business rules
+ feedback
= action and interest
= evolution towards walkthetalkitus traits
Lonerangeri
+ Lonerangeri
+ Lonerangeri
+ Lonerangeri
+ maybe a couple of Notsurewhattodo
= very effective team, evolving nicely and learning skills to support evolution of the
Ignorami in their individual departments/units
EVOLUTION OF the INPATIENT SPECIES
GETTING THE RIGHT SPECIES TOGETHER
With DATA
Building TRUST
Whilst WALKING THE TALK
Will support your own clinical redesign journey.