
Dr. Mahmoud H. Taleb 1 Lecture 10: Antifungal therapy.
53
Dr. Mahmoud H. Taleb Dr. Mahmoud H. Taleb 1 Lecture 10 : Antifungal therapy
-
Upload
kristopher-hart -
Category
Documents
-
view
219 -
download
0
Transcript of Dr. Mahmoud H. Taleb 1 Lecture 10: Antifungal therapy.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 11
Lecture 10:Antifungal therapy

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 22
44 - -Fungal infections and antifungal Fungal infections and antifungal AgentsAgents
Fungal infections are usually more difficult to treat than bacterial infections, because fungal organisms grow slowly and because fungal infections often occur in tissues that are poorly penetrated by antimicrobial agents (e.g., devitalized or avascular tissues).
- Therapy of fungal infections usually requires prolonged treatment.-Advances in medical technology, including organ and bone marrow
transplantation, cytotoxic chemotherapy, the widespread use of indwelling intravenous (IV) catheters, and the increased use of potent broad-spectrum antimicrobial agents all have contributed to thedramatic increase in the incidence of fungal infections worldwide.
-Superficial mycoses are among the most common infections in the World.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 33
-Systemic fungal infection-Mucocutaneous candidiasis may occur in three forms,
oropharyngeal, esophageal, and vulvovaginal disease.- Superficial mycotic infections of the skin are referred to as dermatophytoses.( Tinae capities- Tinae pedis, Tinae, corporis, Tinae cruris, Tinae ungum) .
-A general approach to treatment of superficial mycotic infections includes keeping the infected area dry and clean and limiting exposure to the infected reservoir.
•* *Topical agents generally are considered to be first-line therapy for infections of the skin .
• * * Oral therapy is preferred when the infection is extensive or severe .

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 44
Antifngal drugs1 -Amphotericin B
-Amphotericin B is one of a family of some 200 polyene macrolide antibiotics.Mechanism of action:
-The antifungal activity of amphotericin B depends principally on its binding to a sterol moiety, primarily ergosterol that is present in the membrane of sensitive fungi. By virtue of their interaction with these sterols, polyenes appear to form pores or channels that increase the permeability of the membrane, allowing leakage of a variety of small molecules.
-Amphotericin has a lesser affinity for the mammalian cell membrane component cholesterol, but this interaction does account for most adverse toxic effects associated with this drug.Pharmacokinetics:
-Gastrointestinal absorption of all amphotericin B formulations is negligible . -It is administered as repeated daily intravenous infusions.
-Amphotericin B is highly bounded to protein and its major route of elimination is by metabolism, with little intact drug detected in urine or bile.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 55
Clinical use: -Amphotericin B is most commonly used to treat serious disseminated yeast and
dimorphic fungal infections in immunocompromised hospitalized patients.Adverse effects:
-The major acute reaction to intravenous amphotericin B formulations is fever and chills.
-Nephrotoxicity is the most common and the most serious long-term toxicity of amphotericin B administration.
-Nausea, vomiting, and anorexia are a persistent problem for some patients.-Hypochromic, normocytic anemia may occur. Decreased production of
erythropoietin is the probable mechanism.
2 -FlucytosineFlucytosine is a fluorinated pyrimidine related to fluorouracil and floxuridine.Mechanism of action:
-Flucytosine is converted to 5-fluorouracil inside the cell by the fungal enzyme cytosine deaminase. Subsequently, 5-fluorouracil metabolites interfere with fungal DNA synthesis by inhibiting thymidylate synthetase. Incorporation of these metabolites into fungal RNA may inhibit protein synthesis.
-The selective action of flucytosine is due to the lack or low levels of cytosine deaminase in mammalian cells.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 66
Figure ( 34 ) Mode of action of flucytosine. 5-FdUMP = 5-fluorodeoxyuridine 5'-monophosphate; dTMP = deoxythymidine 5'-monophosphate.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 77
Pharmacokinetics: -Flucytosine is absorbed rapidly and well from the gastrointestinal tract .
-It is widely distributed in the body, with a volume of distribution that approximates total body water, and is minimally bound to plasma proteins.
-Approximately 80% of a given dose is excreted unchanged in the urine. -Flucytosine concentration in CSF is about 65% to 90% of that found
simultaneously in the plasma. The drug also appears to penetrate into the aqueous humor.Clinical uses:
-Flucytosine is used predominantly in combination with amphotericin B, flucytosine caused no added toxicity. When it is used as monotherapy, resistance and clinical failure are common.Adverse effects:
-Flucytosine may depress the bone marrow and lead to leukopenia and thrombocytopenia - Rash, nausea, vomiting, diarrhea, and severe enterocolitis have been noted.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 88
3 - Griseofulvin -This agent inhibits fungal growth by binding to the
microtubules responsible for mitotic spindle formation, as the drug inhibits fungal mitosis. Ineffective topically, griseofulvin is administered orally but has poor gastrointestinal absorption; absorption can be improved by microcrystalline processing of the drug and by taking the drug with fatty meals.
-Griseofulvin is metabolized in the liver. The drug binds to keratin precursor cells and newly synthesized keratin in the stratum corneum of the skin, hair, and nails, stopping the progression of dermatophyte infection.
-Griseofulvin is usually well tolerated. Headache is common with initiation of therapy. Hepatotoxicity, dermatitis, and gastrointestinal distress also occur.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 99
4 -Imidazoles and TriazolesThe azole antifungals include two broad classes, imidazoles and triazoles, which share the same antifungal spectrum and mechanism of action. The systemic triazoles are metabolized more slowly and have less effect on human sterol synthesis than do the imidazoles.Mechanism of action:
The major effect of imidazoles and triazoles on fungi is inhibition of 14- α -sterol demethylase, thus impair the biosynthesis of ergosterol for the cytoplasmic membrane and lead to the accumulation of 14-α-methylsterols. These methylsterols may disrupt the close packing of acyl chains of phospholipids, impairing the functions of certain membrane-bound enzyme systems .

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1010
Specific agents *Ketoconazole
-Ketoconazole , administered orally, has been replaced by itraconazole for the treatment of all mycoses except when the lower cost of ketoconazole outweighs the advantage of itraconazole. Ketoconazole was the first oral azole introduced into clinical use. It is distinguished from triazoles by its greater propensity to inhibit mammalian cytochrome P450 enzymes, it is less
selective for fungal P450 than are the newer azoles . -Ketoconazole sometimes is used to inhibit excessive production of
glucocorticoids in patients with Cushing's syndrome. -Nausea, vomiting, and anorexia occur commonly with ketoconazole,
especially when high doses are prescribed. Epigastric distress can be reduced by taking ketoconazole with food.
-At high doses, ketoconazole causes a clinically significant reduction in testosterone synthesis, This hormonal effect have led to the use of
ketoconazole as a potential adjunctive treatment for prostatic carcinoma.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1111
Figure ( 35 ) Mode of action of ketoconazole.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1212
Antifungal spectrum: Ketoconazole is active against many fungi, including Histoplasma,
Blastomyces, Candida,and Coccidioides, but not aspergillus species. Although itraconazole has largely replaced ketoconazole in the treatment of most mycoses because of its broader spectrum, greater potency, and fewer adverse effects, ketoconazole, as a second-line drug, is a less expensive alternative for the treatment of mucocutaneous candidiasis. Strains of several fungal species that are resistant to ketoconazole have been identified.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1313
Pharmacokinetics: Ketoconazole is only administered orally . It requires gastric acid
for dissolutioand is absorbed through the gastric mucosa. Drugs that raise gastric pH, such as antacids, or that interfere with gastric acid secretion, such as H2-histamine receptor blockers and proton-pump inhibitors, impair absorption. Administering acidifying agents, such as cola drinks, before taking the drug can improve absorption in patients with achlorhydria. Ketoconazole is extensively bound to plasma proteins. Although penetration into tissues is limited, it is effective in the treatment of histoplasmosis in lung, bone, skin, and soft tissues. The drug does not enter the CSF. Extensive metabolism occurs in the liver, and excretion is primarily through the bile. Levels of parent drug in the urine are too low to be effective against mycotic infections of the urinary tract.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1414
Adverse effects: 1 -In addition to allergies, dose-dependent gastrointestinal disturbances, including
nausea, anorexia, and vomiting, are the most common adverse effects of ketoconazole treatment .
2 -Endocrine effects, such as gynecomastia, decreased libido, impotence, and menstrual irregularities, result from the blocking of androgen and adrenal steroid synthesis by ketoconazole. Transient increases in serum transaminases are found
in from 2 to 10 percent of patients .Frank hepatitis occurs rarely but requires immediate cessation of treatment.
Drug interactions and contraindications: By inhibiting cytochrome P450, ketoconazole can potentiate the toxicities of drugs such as cyclosporine, phenytoin, tolbutamide, and warfarin, among others . Rifampin, an inducer of the cytochrome P450 system, can shorten the duration of action of ketoconazole and the other azoles. Drugs that decrease gastric acidity, such as H2-receptor blockers, antacids, proton-pump inhibitors, and sucralfate, can decrease absorption of ketoconazole. Ketoconazole and amphotericin B should not be used together, because the decrease in ergosterol in the fungal membrane reduces the fungicidal action of amphotericin B . Finally, ketoconazole is teratogenic in animals, and it should not be given during pregnancy.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1515
*Itraconazole -Itraconazole lacks ketoconazole's corticosteroid suppression, while
retaining most of ketoconazole's pharmacological properties and expanding the antifungal spectrum.
-Itraconazole is lipophilic and water insoluble and requires a low gastric pH for absorption .
-Oral bioavailability is variable, only 50 to 60% when taken with food and 20% or less when the drug is taken on an empty stomach.
-Itraconazole is metabolized in the liver. It is both a substrate for and a potent inhibitor of CYP3A4.
-The native drug and metabolite are >99% bound to plasma proteins. Neither appears in urine or CSF. - Itraconazole is usually well tolerated but can be associated with nausea and epigastric distress. - High doses may cause hypokalemia, hypertension, and edema.- Hepatotoxicity occurs in fewer than 5% of cases and is usually manifested by reversible liver enzyme elevations.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1616
*Fluconazole -Fluconazole is almost completely absorbed from the gastrointestinal
tract and its bioavailability is unaltered by food or gastric acidity. -About 80% of the drug is excreted unchanged in the urine, and 10%
is excreted unchanged in the feces. -A single dose of 150 mg is effective in uncomplicated vaginal
candidiasis. -Fluconazole is very effective in the treatment of infections with
most Candida spp.-Fluconazole is well tolerated. Nausea, vomiting, abdominal pain,
diarrhea, and skin rash have been reported in fewer than 3% of patients. - Alopecia has been reported as a common adverse event in patients receiving prolonged high-dose therapy.
*Voriconazole
*Posaconazole

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1717
*Miconazole -Miconazole is a broad-spectrum imidazole antifungal agent used in the topical
treatment of cutaneous dermatophyte infections and mucous membrane Candida infections, such as vaginitis .
-Minimal absorption occurs from skin or mucous membrane surfaces. -Local irritation to skin and mucous membranes can occur with topical use;
headaches, urticaria, and abdominal cramping have been reported with treatment for vaginitis.
*Clotrimazole -Clotrimazole is a broad-spectrum fungistatic imidazole drug used in the topical
treatment of oral, skin, and vaginal infections with C. albicans. It is also employed in the treatment of infections with cutaneous dermatophytes.
-Topical use results in therapeutic drug concentrations in the epidermis and mucous membranes; less than 10% of the drug is systemically absorbed .
-Although clotrimazole is generally well tolerated, local abdominal cramping, increased urination, and transient liver enzyme elevations have been reported.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1818
5 -Allylamines *Terbinafine
Terbinafine is the drug of choice for treating dermatophytoses and, especially, onychomycoses (fungal infections of nails). It is better tolerated, requires shorter duration of therapy, and is more effective than either itraconazole or griseofulvin.Mechanism of action:
Terbinafine inhibits fungal squalene epoxidase, thereby decreasing the synthesis of ergosterol. This plus the accumulation of toxic amounts of squalene result in the death of the fungal cell. [Note: Significantly higher concentrations of terbinafine are needed to inhibit human squalene epoxidase, an enzyme required for the cholesterol synthetic pathway.]

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1919
Figure (36) Mode of action of terbinafine.
Antifungal spectrum : The drug is primarily fungicidal. Antifungal activity is limited to dermatophytes and Candida albicans. Therapy is prolonged usually about 3 months but considerably shorter than that with griseofulvin.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2020
Pharmacokinetics: Terbinafine is orally active, although its bioavailability is only 40 % due to first-pass metabolism. Absorption is not significantly enhanced by food. Terbinafine is greater than 99 % bound to plasma proteins. It is deposited in the skin, nails, and fat.
Terbinafine accumulates in breast milk and therefore, should not be given to nursing mothers. A prolonged terminal half-life of 200 to 400 hours may reflect the slow release from these tissues. Terbinafine is extensively metabolized prior to urinary excretion. Patients with either moderate renal impairment or hepatic cirrhosis have reduced clearance.
Adverse effects: The most common adverse effects due to terbinafine are gastrointestinal disturbances (diarrhea, dyspepsia, and nausea), headache, and rash. Taste and visual disturbances have been reported as well as transient elevations in serum liver enzyme levels. All adverse effects resolve upon drug discontinuation. Rarely, terbinafine may cause hepatotoxicity and neutropenia. 6- Echinocandins: Caspofungin, micafungin, and anidulafungin7- Tolnaftate
-

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2121
8-Polyene Antifungal Antibiotics (Nystatin) -Nystatin is structurally similar to amphotericin B and has the same
mechanism of action. - Nystatin is not absorbed from the gastrointestinal tract, skin, or vagina.
-Nystatin is useful only for candidiasis and is supplied in preparations intended for cutaneous, vaginal, or oral administration for this purpose .
-Infections of the nails and hyperkeratinized or crusted skin lesions do not respond .
-Topical preparations include ointments, creams, and powders, all of which contain 100,000 units/g.
-An oral suspension that contains 100,000 units/ml of nystatin is given four times a day. - Too toxic for systemic use, nystatin is limited to the topical treatment of superficial infections caused by C. albicans.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2222
9-Benzoic Acid and Salicylic Acid.
10 -Ciclopirox Olamin
11 -Undecylenic Acid-

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2323
Chemotherapy of protozoal Chemotherapy of protozoal infectionsinfections
Protozoal infections are common among people in Protozoal infections are common among people in underdeveloped tropical and subtropical countries, where underdeveloped tropical and subtropical countries, where sanitary conditions, hygienic practices, and control of the sanitary conditions, hygienic practices, and control of the vectors of transmission are inadequate. However, with vectors of transmission are inadequate. However, with increased world travel, protozoal diseases such as amebiasis, increased world travel, protozoal diseases such as amebiasis, giardiasis, trichomoniasis, leishmaniasis, Toxoplasmosis, giardiasis, trichomoniasis, leishmaniasis, Toxoplasmosis, trypanosomiasis, and malaria are no longer confined to trypanosomiasis, and malaria are no longer confined to specific geographic locales. Protozoal diseases are thus less specific geographic locales. Protozoal diseases are thus less easily treated than bacterial infections, and many of the easily treated than bacterial infections, and many of the antiprotozoal drugs cause serious toxic effects in the host, antiprotozoal drugs cause serious toxic effects in the host, particularly on cells showing high metabolic activity, such as particularly on cells showing high metabolic activity, such as neuronal, renal tubular, intestinal, and bone marrow stem cells. neuronal, renal tubular, intestinal, and bone marrow stem cells. Most antiprotozoal agents have not proved to be safe for Most antiprotozoal agents have not proved to be safe for pregnant patients. Drugs used to treat protozoal infections are pregnant patients. Drugs used to treat protozoal infections are summarized in Figure summarized in Figure

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2424Figure ( 37) Summary of antiprotozoal agents.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2525
1-Metronidazole1-Metronidazole- Metronidazole is clinically effective in trichomoniasis, amebiasis, and giardiasis, as - Metronidazole is clinically effective in trichomoniasis, amebiasis, and giardiasis, as
well as in a variety of infections caused by obligate anaerobic bacteria, including well as in a variety of infections caused by obligate anaerobic bacteria, including Bacteroides, Clostridium,Bacteroides, Clostridium, and microaerophilic bacteria such as and microaerophilic bacteria such as HelicobacterHelicobacter and and CampylobacterCampylobacter species. species.
- Metronidazole is a prodrug that requires reduction before it becomes active. The - Metronidazole is a prodrug that requires reduction before it becomes active. The enzyme, pyruvate-ferredoxin oxidoreductase, found only in anaerobic organisms, enzyme, pyruvate-ferredoxin oxidoreductase, found only in anaerobic organisms, reduces metronidazole and thereby activates the drug. Reduced metronidazole reduces metronidazole and thereby activates the drug. Reduced metronidazole disrupts replication and transcription and inhibits DNA repair.disrupts replication and transcription and inhibits DNA repair.
- Preparations of metronidazole are available for oral, intravenous, intravaginal, and - Preparations of metronidazole are available for oral, intravenous, intravaginal, and topical administration. The drug has complete and rapid absorption after oral topical administration. The drug has complete and rapid absorption after oral intake. - The half-life of metronidazole in plasma is about 8 hours, and its volume intake. - The half-life of metronidazole in plasma is about 8 hours, and its volume of distribution is approximately that of total-body water.of distribution is approximately that of total-body water.
- The most frequently observed adverse reactions to metronidazole include nausea, The most frequently observed adverse reactions to metronidazole include nausea, vomiting, cramps, diarrhea, and a metallic taste. - The urine is often dark or red vomiting, cramps, diarrhea, and a metallic taste. - The urine is often dark or red brown.brown.
- While metronidazole has been taken during all stages of pregnancy with no apparent - While metronidazole has been taken during all stages of pregnancy with no apparent adverse effects, its use during the first trimester generally is not advised.adverse effects, its use during the first trimester generally is not advised.
- Other clinically effective 5-nitroimidazoles closely related in structure and activity Other clinically effective 5-nitroimidazoles closely related in structure and activity to metronidazole are tinidazole and ornidazole.to metronidazole are tinidazole and ornidazole.
- Although tinidazole and metronidazole are equally effective, tinidazole is given in a - Although tinidazole and metronidazole are equally effective, tinidazole is given in a shorter course and is better tolerated.shorter course and is better tolerated.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2626
Tinidazole:Tinidazole: Tinidazole Tinidazole is a second-generation nitroimidazole that is similar is a second-generation nitroimidazole that is similar
to to metronidazole metronidazole in spectrum of activity, absorption, adverse in spectrum of activity, absorption, adverse effects and drug interactions effects and drug interactions Tinidazole Tinidazole is as effective as is as effective as metronidazolemetronidazole, with a shorter course of treatment, yet is more , with a shorter course of treatment, yet is more expensive than genericexpensive than generic metronidazole.metronidazole.
2-Diloxanide furoate2-Diloxanide furoateIt is an effective luminal amebicide but is not active against tissue trophozoites. In the It is an effective luminal amebicide but is not active against tissue trophozoites. In the
gut, diloxanide furoate is split into diloxanide and furoic acid; about 90% of the gut, diloxanide furoate is split into diloxanide and furoic acid; about 90% of the diloxanide is rapidly absorbed and then conjugated to form the glucuronide, which diloxanide is rapidly absorbed and then conjugated to form the glucuronide, which is promptly excreted in the urine. The unabsorbed diloxanide is the active is promptly excreted in the urine. The unabsorbed diloxanide is the active antiamebic substance. The mechanism of action of diloxanide furoate is unknown.antiamebic substance. The mechanism of action of diloxanide furoate is unknown.
Diloxanide furoate is considered the drug of choice for asymptomatic luminal Diloxanide furoate is considered the drug of choice for asymptomatic luminal infections. It is used with a tissue amebicide, usually metronidazole, to treat infections. It is used with a tissue amebicide, usually metronidazole, to treat serious intestinal and extra intestinal infections. Diloxanide furoate does not serious intestinal and extra intestinal infections. Diloxanide furoate does not produce serious adverse effects. Flatulence is common, but nausea and abdominal produce serious adverse effects. Flatulence is common, but nausea and abdominal cramps are infrequent and rashes are rare. The drug is not recommended in cramps are infrequent and rashes are rare. The drug is not recommended in pregnancy.pregnancy.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2727
3-Paromomycin3-Paromomycin
4- Furazolidone4- Furazolidone- 5- Chloroquine:5- Chloroquine:
6- Emetine and dehydroemetine: 6- Emetine and dehydroemetine:
7- Iodoquinol: 7- Iodoquinol:
8- Other protozoal agents8- Other protozoal agentsPentamidine, Eflornithine, Nifurtimox, Melarsoprol, Pentamidine, Eflornithine, Nifurtimox, Melarsoprol,
Sodium stibogluconate, Amphotericin, , Sodium stibogluconate, Amphotericin, , Tetracyclines, Spiramicin, suramin and Fumagillin.Tetracyclines, Spiramicin, suramin and Fumagillin.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2828
Chemptherapy of Helminthic Chemptherapy of Helminthic DiseasesDiseases
- Most intestinal helminthic infections may not be - Most intestinal helminthic infections may not be associated with clearly defined manifestation of associated with clearly defined manifestation of disease, but they can cause significant pathology. One disease, but they can cause significant pathology. One factor that determines the pathogenicity of helminths is factor that determines the pathogenicity of helminths is their population density. Light infections may be fairly their population density. Light infections may be fairly well tolerated, whereas high populations of intestinal well tolerated, whereas high populations of intestinal helminths can result in predictable disease presentations. helminths can result in predictable disease presentations. Helminthic infections include nematode,cestode and Helminthic infections include nematode,cestode and trematode infections as shown in table (8).trematode infections as shown in table (8).
- Anthelmintics are drugs that act either locally to expel - Anthelmintics are drugs that act either locally to expel worms from the gastrointestinal tract or systemically to worms from the gastrointestinal tract or systemically to eradicate adult helminths or developmental forms that eradicate adult helminths or developmental forms that invade organs and invade organs and tissues. tissues.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2929
1- Benzimidazoles (BZAs)1- Benzimidazoles (BZAs)- The BZAs, exemplified - The BZAs, exemplified by mebendazole, flubendazole and albendazole.by mebendazole, flubendazole and albendazole. BZAs produce BZAs produce
many biochemical changes in susceptible nematodes including inhibition of many biochemical changes in susceptible nematodes including inhibition of
mitochondrial fumarate reductase, reduced glucose transport, and uncoupling of mitochondrial fumarate reductase, reduced glucose transport, and uncoupling of
oxidative phosphorylation, but their primary action likely is to inhibit microtubule oxidative phosphorylation, but their primary action likely is to inhibit microtubule
polymerization by binding to β-tubulin. polymerization by binding to β-tubulin.
- The selective toxicity of these agents results because the BZAs bind parasite β-tubulin - The selective toxicity of these agents results because the BZAs bind parasite β-tubulin
with much higher affinity than they do the mammalian protein.with much higher affinity than they do the mammalian protein.
- Appropriate doses of mebendazole, flubendazole and albendazole are highly effective - Appropriate doses of mebendazole, flubendazole and albendazole are highly effective
in treating ascariasis, enterobiasis, trichuriasis, and hookworm as well as less in treating ascariasis, enterobiasis, trichuriasis, and hookworm as well as less
common human nematode infections.common human nematode infections.
- These drugs are active against both larval and adult stages of nematodes that cause - These drugs are active against both larval and adult stages of nematodes that cause
these infections. Immobilization and death of susceptible gastrointestinal parasites these infections. Immobilization and death of susceptible gastrointestinal parasites
occur slowly, and their clearance from the GI tract may not be complete until several occur slowly, and their clearance from the GI tract may not be complete until several
days after treatment.days after treatment.
- Albendazole is superior to mebendazole in curing hookworm and trichuriasis infections - Albendazole is superior to mebendazole in curing hookworm and trichuriasis infections
in children, especially when used as a single dose.in children, especially when used as a single dose.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3030
PharmacokineticsPharmacokinetics- Tablet formulations of mebendazole are poorly and erratically absorbed, the tablets - Tablet formulations of mebendazole are poorly and erratically absorbed, the tablets
should be chewed before swallowing and concentrations of the drug in plasma are should be chewed before swallowing and concentrations of the drug in plasma are low and do not reflect the dosage taken.low and do not reflect the dosage taken.
- Albendazole is variably and erratically absorbed after oral administration; absorption is - Albendazole is variably and erratically absorbed after oral administration; absorption is enhanced by the presence of fatty foods and possibly by bile salts.enhanced by the presence of fatty foods and possibly by bile salts.
Clinical UsesClinical Uses Mebendazole always is taken orally, and the same dosage schedule applies to adults Mebendazole always is taken orally, and the same dosage schedule applies to adults
and children more than 2 years of age. For treatment of enterobiasis, a single 100-mg and children more than 2 years of age. For treatment of enterobiasis, a single 100-mg tablet is taken; a second should be given after 2 weeks. For control of ascariasis, tablet is taken; a second should be given after 2 weeks. For control of ascariasis, trichuriasis, or hookworm infections, the recommended regimen is 100 mg of trichuriasis, or hookworm infections, the recommended regimen is 100 mg of mebendazole taken in the morning and evening for 3 consecutive days (or a single mebendazole taken in the morning and evening for 3 consecutive days (or a single 500-mg tablet administered once). 500-mg tablet administered once). If the patient is not cured 3 weeks after treatment, a second course should be given. If the patient is not cured 3 weeks after treatment, a second course should be given.
- Like mebendazole, albendazole provides safe and highly effective therapy against - Like mebendazole, albendazole provides safe and highly effective therapy against infections with gastrointestinal nematodes, including mixed infections of infections with gastrointestinal nematodes, including mixed infections of AscarisAscaris, , TrichurisTrichuris, and hookworms. For treatment of enterobiasis, ascariasis, trichuriasis, and , and hookworms. For treatment of enterobiasis, ascariasis, trichuriasis, and hookworm infections, albendazole is taken as a single oral 400-mg dose by adults hookworm infections, albendazole is taken as a single oral 400-mg dose by adults and children more than 2 years of age. In children between the ages of 12 and 24 and children more than 2 years of age. In children between the ages of 12 and 24 months, the WHO recommends a reduced dose of 200 mg.months, the WHO recommends a reduced dose of 200 mg.
- Overall, the BZAs have excellent safety profiles.- Overall, the BZAs have excellent safety profiles.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3131
Adverse Reactions, Contraindications, & CautionsAdverse Reactions, Contraindications, & Cautions
Short-term mebendazole therapy for intestinal nematodes Short-term mebendazole therapy for intestinal nematodes is nearly free of adverse effects. Mild nausea, vomiting, is nearly free of adverse effects. Mild nausea, vomiting, diarrhea, and abdominal pain have been reported diarrhea, and abdominal pain have been reported infrequently. Rare side effects, usually with high-dose infrequently. Rare side effects, usually with high-dose therapy, are hypersensitivity reactions (rash, urticaria), therapy, are hypersensitivity reactions (rash, urticaria), agranulocytosis, alopecia, and elevation of liver agranulocytosis, alopecia, and elevation of liver enzymes.enzymes.
Mebendazole is teratogenic in animals and therefore Mebendazole is teratogenic in animals and therefore contraindicated in pregnancy. It should be used with contraindicated in pregnancy. It should be used with caution in children under 2 years of age because of caution in children under 2 years of age because of limited experience and rare reports of convulsions in this limited experience and rare reports of convulsions in this age group.age group.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3232
2- Pyrantel pamoate2- Pyrantel pamoate- Pyrantel pamoate is a agonist at the nicotinic acetylcholine receptor, and its - Pyrantel pamoate is a agonist at the nicotinic acetylcholine receptor, and its
actions result in depolarization and spastic paralysis of the helminth muscle.actions result in depolarization and spastic paralysis of the helminth muscle.- Its selective toxicity occurs primarily because the neuromuscular junction of - Its selective toxicity occurs primarily because the neuromuscular junction of
helminth muscle is more sensitive to the drug than is mammalian muscle. helminth muscle is more sensitive to the drug than is mammalian muscle. Anthelmintic ActionsAnthelmintic ActionsPyrantel is effective against mature and immature forms of susceptible Pyrantel is effective against mature and immature forms of susceptible
helminths within the intestinal tract but not against migratory stages in the helminths within the intestinal tract but not against migratory stages in the tissues or against ova.tissues or against ova.
Pyrantel pamoate Pyrantel pamoate along with along with mebendazolemebendazole, is effective in the treatment of , is effective in the treatment of infectionscaused by roundworms, pinworms, and hookworms. infectionscaused by roundworms, pinworms, and hookworms. Clinical UsesClinical Uses
The standard dose is 11 mg (base)/kg (maximum, 1 g), given orally once with or The standard dose is 11 mg (base)/kg (maximum, 1 g), given orally once with or without food. For pinworm the dose is repeated in 2 weeks, and cure rates without food. For pinworm the dose is repeated in 2 weeks, and cure rates are greater than 95%. are greater than 95%.
. Pyrantel should be used with caution in patients with liver dysfunction, since . Pyrantel should be used with caution in patients with liver dysfunction, since low, transient aminotransferaseelevations have been noted in a small low, transient aminotransferaseelevations have been noted in a small number of patients. Experience with the drug in pregnant women and number of patients. Experience with the drug in pregnant women and children under age 2 years is limited.children under age 2 years is limited.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3333
3- Niclosamide3- Niclosamide Niclosamide is a second-line drug for the treatment of most tapeworm Niclosamide is a second-line drug for the treatment of most tapeworm
infections.infections.UsesUsesThe adult dose of niclosamide is 2 g once, given in the morning on an empty The adult dose of niclosamide is 2 g once, given in the morning on an empty
stomach. The tablets must be chewed thoroughly and are then stomach. The tablets must be chewed thoroughly and are then swallowed with water.swallowed with water.
T Saginata T Saginata (Beef Tapeworm), (Beef Tapeworm), T Solium T Solium (Pork Tapeworm), and (Pork Tapeworm), and Diphyllobothrium Latum Diphyllobothrium Latum (Fish Tapeworm) . Infrequent, mild, and (Fish Tapeworm) . Infrequent, mild, and transitory adverse events include nausea, vomiting, diarrhea, and transitory adverse events include nausea, vomiting, diarrhea, and abdominal discomfort. The consumption of alcohol should be avoided abdominal discomfort. The consumption of alcohol should be avoided on the day of treatment and for 1 day afterward. The safety of the drug on the day of treatment and for 1 day afterward. The safety of the drug has not been established in pregnancy or for childrenhas not been established in pregnancy or for children under 2 years of under 2 years of age.age.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3434
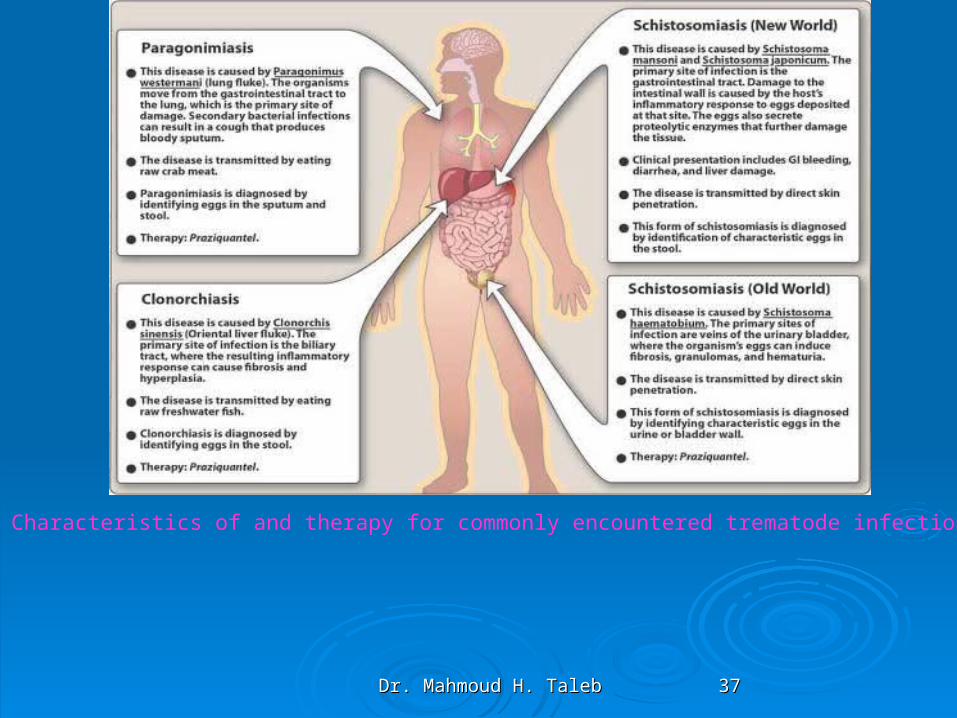
4- 4- PraziquantelPraziquantel
- - The neuromuscular effects of praziquantel appear to The neuromuscular effects of praziquantel appear to increase parasite motility leading to spastic increase parasite motility leading to spastic paralysis. The drug increases calcium permeability paralysis. The drug increases calcium permeability through parasite-specific ion through parasite-specific ion channels-. It is the most effective of the drugs used channels-. It is the most effective of the drugs used
in the treatment of schistosomiasisin the treatment of schistosomiasis,,
5- Oxamniquine5- OxamniquineOxamniquine is an alternative to praziquantel for the treatment of Oxamniquine is an alternative to praziquantel for the treatment of
S mansoni S mansoni infections. It has also been used extensively for infections. It has also been used extensively for mass treatment. Itmass treatment. It is not effective against is not effective against S haematobium.S haematobium.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3535
6- Thiabendazole6- ThiabendazoleThiabendazole is an alternative to ivermectin for the Thiabendazole is an alternative to ivermectin for the
treatment of strongyloidiasis and cutaneous larva treatment of strongyloidiasis and cutaneous larva migrans.migrans.
7- Diethylcarbamazine Citrate7- Diethylcarbamazine CitrateDiethylcarbamazine is a drug of choice in the treatment Diethylcarbamazine is a drug of choice in the treatment
of filariasis.of filariasis.
8- Other anthelmintics8- Other anthelmintics
-- Emetine and hydroemetine.-- Emetine and hydroemetine.
- Bithionol.- Bithionol.
--Suramin.--Suramin.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3636
Figure () Characteristics of and therapy for commonly encountered nematode infections
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3737
Figure () Characteristics of and therapy for commonly encountered trematode infections.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3838
Figure (41) Characteristics of and therapy for commonly encountered cestode infections.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3939
Antiscabietic and antipediculosis drugsAntiscabietic and antipediculosis drugs
1- Sulfur1- Sulfur2-Crotamiton2-Crotamiton3-Lindane (Hexachlorocyclohexane)3-Lindane (Hexachlorocyclohexane)4- Permethrin( Ectomethrin, Tick tack, lice nock, zehuze)4- Permethrin( Ectomethrin, Tick tack, lice nock, zehuze)5- Malathion5- Malathion6- Other alternatives scabicedes6- Other alternatives scabicedes *Benzyl benzoate *Benzyl benzoate ( Benzanil, Scabicide).( Benzanil, Scabicide). * Ivermectin* Ivermectin

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4040
Table(8) Summary of anthelmintic agents.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4141

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4242
Antiviral drugsAntiviral drugsVirusesVirusesViruses are autonomous infectious particles that differ widely Viruses are autonomous infectious particles that differ widely
from other microorganisms in a number of characteristics: from other microorganisms in a number of characteristics: they have no cellular structurethey have no cellular structure,, consisting only consisting only of proteins and of proteins and nucleic acidnucleic acid (DNA or RNA). (DNA or RNA). They have metabolic systems of They have metabolic systems of their owntheir own, but rather depend on the synthetic mechanism, but rather depend on the synthetic mechanism of a of a living host cell, whereby the viruses uset normal cellular living host cell, whereby the viruses uset normal cellular metabolismmetabolism by delivering their own genetic information, i.e., by delivering their own genetic information, i.e., nucleic acid, into the host cellnucleic acid, into the host cell..
The host cell accepts the nucleic acid and proceeds to produce The host cell accepts the nucleic acid and proceeds to produce the components of new viruses in accordance with the genetic the components of new viruses in accordance with the genetic information it contains.information it contains.
Viruses infect bacteria (so-called bacteriophages), plants, Viruses infect bacteria (so-called bacteriophages), plants, animals, and humans.animals, and humans.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4343
Figure ( )Essential Characteristics of VirusesFigure ( )Essential Characteristics of Viruses

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4444

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4545
Figure () The major sites of antiviral drug action.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4646

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4747
Viruses are obligate intracellular parasites; their Viruses are obligate intracellular parasites; their replication depends primarily on synthetic processes replication depends primarily on synthetic processes of the host cell. Consequently, to be effective, of the host cell. Consequently, to be effective, antiviral agents must either block viral entry into or antiviral agents must either block viral entry into or exit from the cell or be active inside the host cell. exit from the cell or be active inside the host cell. NonselectiveNonselective inhibitors of virus replication may inhibitors of virus replication may interfere with host cell function and produce toxicity. interfere with host cell function and produce toxicity. The search for chemicals that inhibit virus-specific The search for chemicals that inhibit virus-specific functions is currently one of the most active areas of functions is currently one of the most active areas of pharmacologic investigation. Research in antiviral pharmacologic investigation. Research in antiviral chemotherapy began in the early 1950s, when the chemotherapy began in the early 1950s, when the search for anticancer drugs generated several new search for anticancer drugs generated several new compounds capable of inhibiting viral DNA compounds capable of inhibiting viral DNA synthesis. synthesis.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4848
Recent research has focused on the identification of agents with Recent research has focused on the identification of agents with greater selectivity, in vivo stability, and lack of toxicity. greater selectivity, in vivo stability, and lack of toxicity. Selective antiretroviral agents that inhibit a critical HIV-1 Selective antiretroviral agents that inhibit a critical HIV-1 enzyme such as reverse transcriptase or the protease required enzyme such as reverse transcriptase or the protease required for final packaging of the virus particle have become for final packaging of the virus particle have become available. In many viral infections, replication of the virus available. In many viral infections, replication of the virus peaks at or before the manifestation of clinical symptoms. peaks at or before the manifestation of clinical symptoms. Optimal clinical efficacy in many viral illnesses therefore Optimal clinical efficacy in many viral illnesses therefore depends either on early initiation of therapy (eg, acyclovir for depends either on early initiation of therapy (eg, acyclovir for treatment of varicella or zoster infection) or on prevention of treatment of varicella or zoster infection) or on prevention of infection (eg, chemoprophylaxis against influenza A using a infection (eg, chemoprophylaxis against influenza A using a neuraminidase inhibitor or amantadine. Alternatively, potent neuraminidase inhibitor or amantadine. Alternatively, potent inhibition of viral replication may be of clinical benefit in inhibition of viral replication may be of clinical benefit in chronicchronic illnesses such as HIV infection or viral hepatitisillnesses such as HIV infection or viral hepatitis..

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 4949
Pharmacokinetics:Pharmacokinetics: Administration of Administration of acyclovir acyclovir can be by can be by an intravenous, oral, or topical route. The drug an intravenous, oral, or topical route. The drug distributes well throughout the body, including the distributes well throughout the body, including the cerebrospinal fluid (CSF).cerebrospinal fluid (CSF). Acyclovir Acyclovir is partially is partially metabolized to an inactive product.metabolized to an inactive product.
Excretion into the urine occurs both by glomerular filtration Excretion into the urine occurs both by glomerular filtration and by tubular secretionand by tubular secretion. Acyclovir . Acyclovir accumulates in accumulates in patients with renal failure.patients with renal failure.
Adverse effectsAdverse effects: : Side effects of Side effects of acyclovir acyclovir treatment treatment depend on the route of administration. For example, depend on the route of administration. For example, local irritation may occur from topical application; local irritation may occur from topical application; headache, diarrhea, nausea, and vomiting may result headache, diarrhea, nausea, and vomiting may result after oral administration. Transient renal dysfunction may after oral administration. Transient renal dysfunction may occur at high doses or in a dehydrated patient receiving occur at high doses or in a dehydrated patient receiving the drug intravenously. the drug intravenously.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 5050
II. Treatment of Respiratory Virus II. Treatment of Respiratory Virus InfectionsInfections
A.A. Neuraminidase inhibitorsNeuraminidase inhibitors
B.B. Inhibitors of viral uncoatingInhibitors of viral uncoating
C.C. RibavirinRibavirin

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 5151
III. Treatment of Hepatic Viral InfectionsIII. Treatment of Hepatic Viral InfectionsA.A. InterferonInterferonB.B. LamivudineLamivudine
IV. Treatment of Herpes virus InfectionsIV. Treatment of Herpes virus InfectionsA.A. AcyclovirAcyclovirB.B. . Ganciclovir C. Penciclovir and . Ganciclovir C. Penciclovir and D. famciclovi E. VidarabineD. famciclovi E. VidarabineF. FoscarentF. Foscarent

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 5252
IV. Treatment of Herpes virus IV. Treatment of Herpes virus InfectionsInfections
A. AcyclovirA. AcyclovirHerpes simplex virus (HSV) Types 1 and 2, varicella-zoster virus (VZV)and some Herpes simplex virus (HSV) Types 1 and 2, varicella-zoster virus (VZV)and some
Epstein-Barr virus mediated infections are sensitive to Epstein-Barr virus mediated infections are sensitive to acycloviracyclovir. It is the treatment . It is the treatment of choice in HSV encephalitis.The most common use of of choice in HSV encephalitis.The most common use of acyclovir acyclovir is in therapy for is in therapy for genital herpes infections. It is also given prophylactically to seropositive patients genital herpes infections. It is also given prophylactically to seropositive patients before bone marrow and after heart transplants to protect such individuals during before bone marrow and after heart transplants to protect such individuals during posttransplant immunosuppressive treatments.posttransplant immunosuppressive treatments.
Mode of action:Mode of action: AcyclovirAcyclovir, is monophosphorylated in the cell by the herpes virus , is monophosphorylated in the cell by the herpes virus encoded enzyme, thymidine kinase . Therefore, virus-infected cells are most encoded enzyme, thymidine kinase . Therefore, virus-infected cells are most susceptible. The monophosphate analog is converted to the di- and triphosphate susceptible. The monophosphate analog is converted to the di- and triphosphate forms by the host cells. Acyclovir triphosphate competes with forms by the host cells. Acyclovir triphosphate competes with deoxyguanosine deoxyguanosine triphosphate triphosphate as a substrate for viral DNA polymerase and is itself incorporated into as a substrate for viral DNA polymerase and is itself incorporated into the viral DNA, causing premature DNA-chain terminationthe viral DNA, causing premature DNA-chain termination . .
Resistance:Resistance: Altered or deficient thymidine kinase and DNA polymerases have been found in some Altered or deficient thymidine kinase and DNA polymerases have been found in some
resistant viral strains and are most commonly isolated from immunocompromised resistant viral strains and are most commonly isolated from immunocompromised patients. Cross-resistance to the other cyclovirs occurs.patients. Cross-resistance to the other cyclovirs occurs.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 5353
V. Treatment of HIV InfectionV. Treatment of HIV Infection


















