Dr Kirsten Way - University of Queensland - Creating Mentally Healthy Workplaces: WHS compliance or...
22
Creating Mentally Healthy Workplaces: WHS compliance or best practice - where’s the line? Dr Kïrsten Way, Manager Employee Health, Safety and Wellbeing
-
Upload
informa-australia -
Category
Business
-
view
756 -
download
0
Transcript of Dr Kirsten Way - University of Queensland - Creating Mentally Healthy Workplaces: WHS compliance or...
Creating Mentally Healthy Workplaces: WHS compliance or best practice - where’s the line?
Dr Kïrsten Way, Manager Employee Health, Safety and Wellbeing

We’ve come a long way
• Explicitly acknowledged in scope of legislation
• Better definitions
• National and international governmental recognition of the problem, media interest
• Employer and Industry acknowledgement of hazards and risk
• WHS guidance now available
• Investigation and enforcement by regulators
Recent cases

Work-Related
The current conversation
Mental Health
Psychosocial Hazards
Group-level vs Individual-level

Psychosocial Hazards WHAT ARE PSYCHOSOCIAL HAZARDS?
• Work-related stress • Workplace Bullying
• Fatigue • Work-related violence and
aggression

Stress Response
Psychological Injury/Illness
(depression, anxiety, burnout, emotional
distress, sleep disturbance, suicide)
Physical Illness (CVD, MSDs,
immune deficiency,
gastrointestinal disorders)
Poor Health Behaviours
(exercise, diet, alcohol
consumption and smoking)

Is there evidence of exposure to risk?

Is there evidence of failure to manage the risk?

Stage Controls -‐ Bullying
Before the Event
• Job Design and Management • Commitment • Complaint Handling Procedures,
• Support and Coaching • Reward respec=ul behaviour
• Policies and Procedures • Instruc@on, Training & Supervision
• HR Systems • Regular monitoring
During the Event
• INTERVENE EARLY • Quick risk assessment, then ins@tute procedures
• Encourage people to act • ENSURE PROCEDURES ARE IMPLEMENTED
A8er the Event
• Media@on or Inves@ga@on as appropriate
• Ensure consequences occur • Relevant external agencies?
• Employee assistance services
• Return to work/case management
• Organisa@onal Development

Two Examples

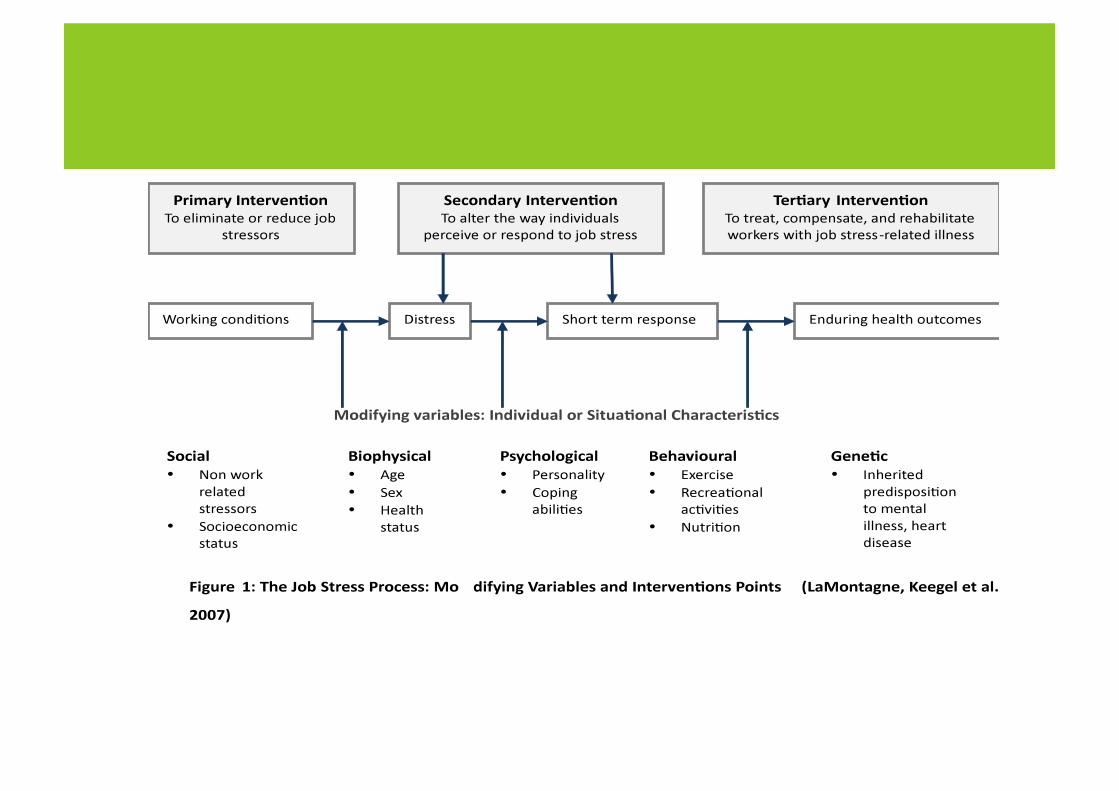
PRIMARY PREVENTION
PEOPLE AT WORK
Hazard identification
Risk assessment
Implement controls
SECONDARY INTERVENTION
Improves workplace outcomes by: ! Responding to early
indicators of absence, injury and illness
TERTIARY INTERVENTION
Injury treatment
Injury management
Rehabilitation & Return-to-Work
Complaints/Invest

PRIMARY INTERVENTION
Hazard identification
Risk assessment
Implement controls
TERTIARY INTERVENTION
Injury treatment
Injury management
Rehabilitation & Return-to-Work
Complaint work
SECONDARY INTERVENTION
RESOLVE AT WORK
Improves workplace outcomes by:
! Responding to early indicators of absence, injury and illness
! Identifying contributing workplace factors
! Integrating WHS, injury management and RTW

The Resolve Framework
1. Referral 2. Initial contact 3. Assessment 4. Intervention and reporting 5. Case conference and reporting 6. Implement and Review
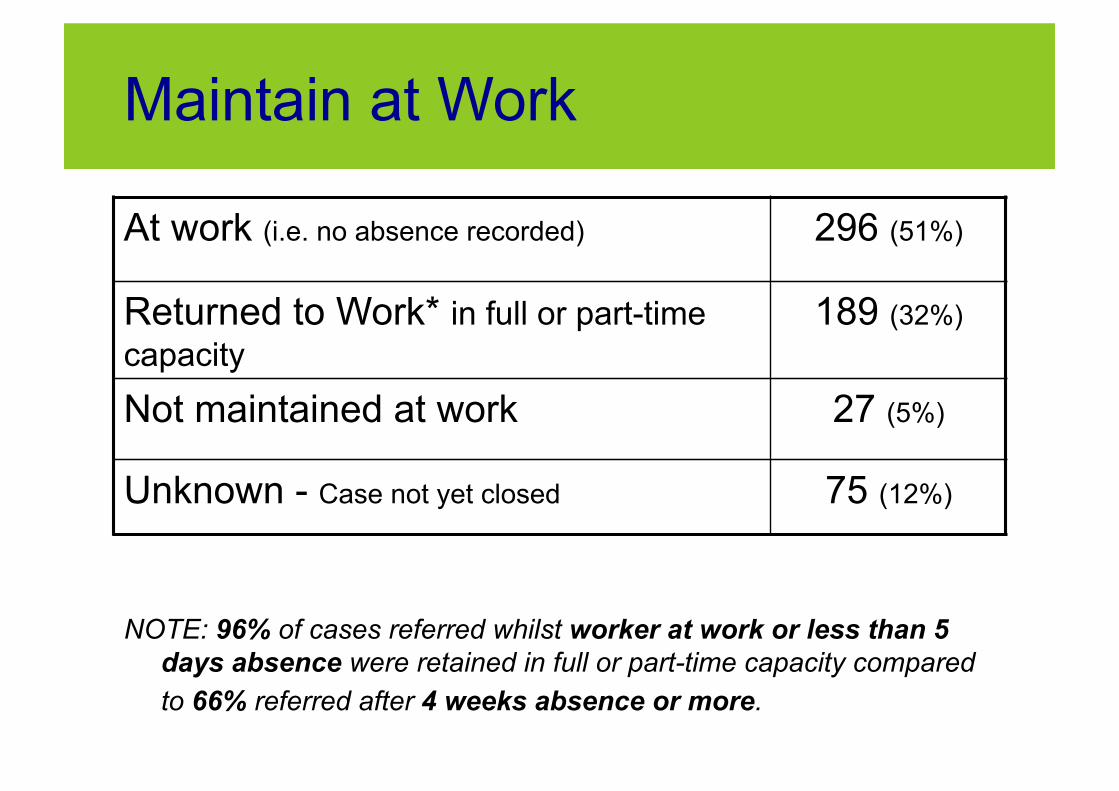
Maintain at Work
At work (i.e. no absence recorded) 296 (51%)
Returned to Work* in full or part-time capacity
189 (32%)
Not maintained at work 27 (5%)
Unknown - Case not yet closed 75 (12%)
NOTE: 96% of cases referred whilst worker at work or less than 5 days absence were retained in full or part-time capacity compared to 66% referred after 4 weeks absence or more.

What are the challenges in compliance for psychosocial hazards?

1. Definitions in law versus general understanding of issues in the community
2. Scope confusions 3. Cumulative nature of the risk (for some
hazards) 4. Number of players in the regulatory
space 5. Limited avenues for personal redress 6. Broader issues of causation/interplay with
design and management of work 7. “Helpers” being unhelpful

So where’s the line?
What is the evidence of exposure to risk? What is the evidence of failure to manage the risk? As WHS professionals - group-level is the key
Some final thoughts
• Regulators continue to respond to complaints and incidents
• There is a strategic push to ensure psychosocial hazards are managed through primary prevention

Some final thoughts
• Raising mental health awareness is not enough
• The EAP and resilience training trap • Resilience, engagement, wellness, and
other confusions • Fatigue vs Violence vs Bullying vs Stress • Focus on non-trivial issues

How do your activities relate to compliance and best practice?




![Unit 1 Where’s your pen pal from?. Where’s your pen pal from? [pæl ]](https://static.fdocuments.us/doc/165x107/56649dd95503460f94acec0b/unit-1-wheres-your-pen-pal-from-wheres-your-pen-pal-from-pael-.jpg)