![[MS-OXOAB]: Offline Address Book (OAB) File Format and Schema... · The Offline Address Book (OAB) File Format and Schema describes the offline address book (OAB) version 2, OAB version](https://static.fdocuments.us/doc/165x107/5eaa3b08de880701d656f56f/ms-oxoab-offline-address-book-oab-file-format-and-schema-the-offline.jpg)
Dr hassaan...(OAB)
35
-
Upload
aswan-university- -
Category
Health & Medicine
-
view
121 -
download
1
Transcript of Dr hassaan...(OAB)


OVERACTIVE BLADDER SYNDROMEPRACTICAL VIEW
By
Hassaan Ali GadAssistant lecturer of urology and Andrology
Aswan University [email protected]
OUTLINE
Introduction… Definition and Prevalence.Bladder Anatomy and Physiology. Etiology and Pathophysiology OAB.Diagnosis and evaluation of OAB.Treatment of OAB.

Definition of OAB
• The International Continence Society (ICS) defines OAB as:
• The presence of “urinary urgency, usually accompanied by frequency and nocturia, with or without urge incontinence, in the absence of UTI or other pathology.”
• OAB is defined based on symptoms and Known as( Overactive Bladder Syndrome)

Sudden compelling desire to pass urine that is difficult to defer urgency
Patient considers that he/she voids too often by dayNormal is < 8 times per 24 hours
Frequency
Waking to urinate during sleep hours considered a clinical problem if frequency is greater than twice a night
Nocturia
Involuntary leakage accompanied by or immediately preceded by urgency
Urge urinaryincontinence (UUI)
OAB with UUI OAB “wet”
OAB without UUI OAB “dry”
Time from first sensation of urgency to voiding Warning time
Terminology

It affects approximately 17%
of the adult
Women < Men
prevalence increase with age
Dry OAB< wet OAB
PREVALENCE

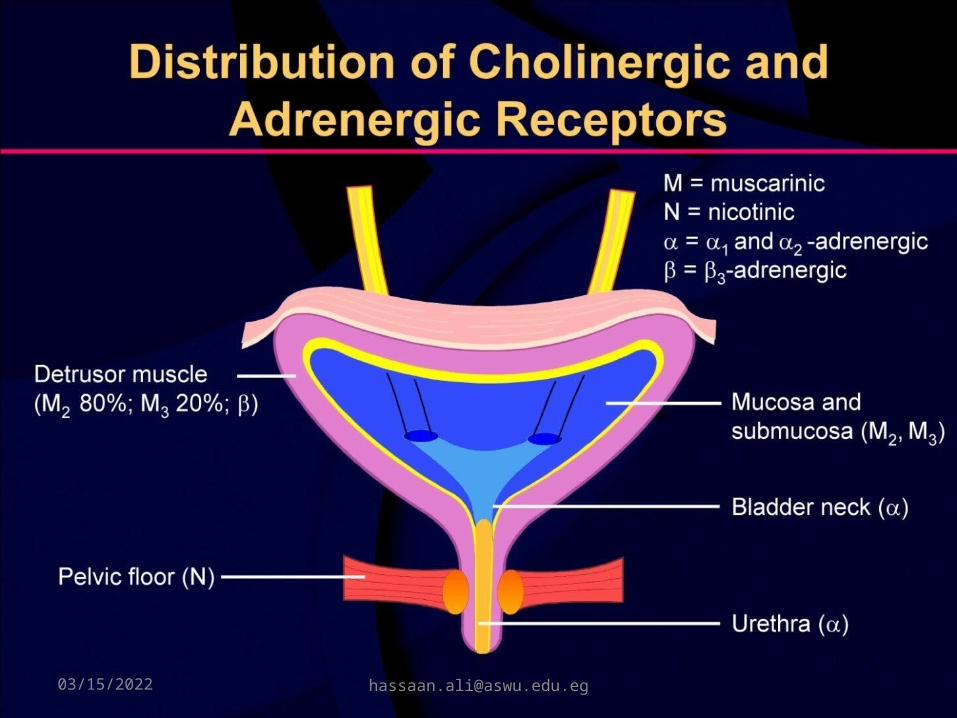
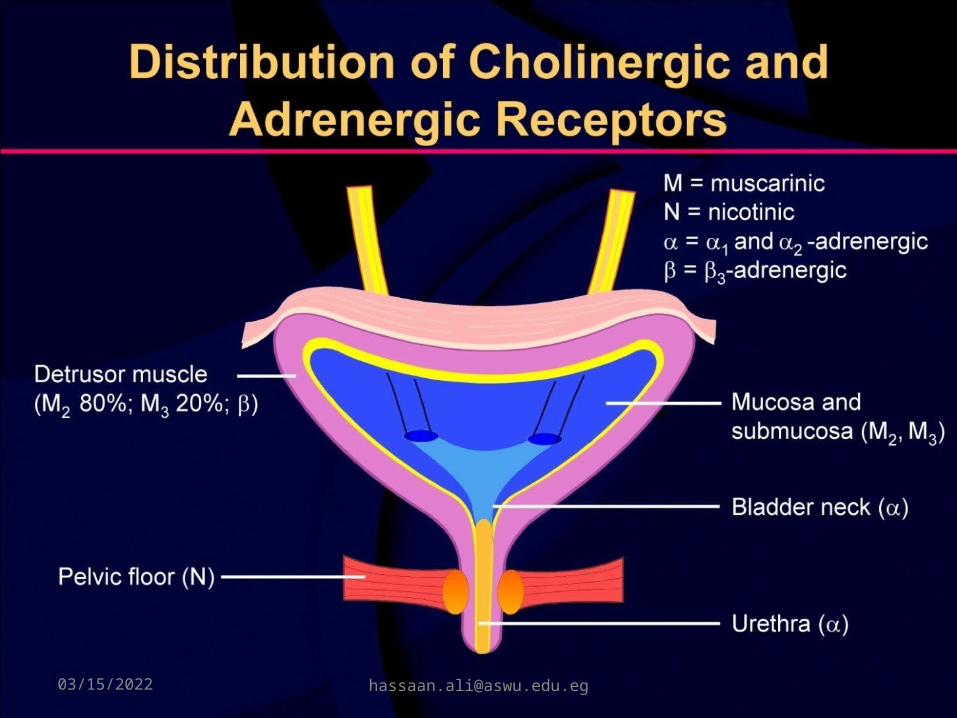
Bladder Anatomy and Physiology

L1
L2
L3
Sympathetic nerve supply
Sympathetic
chain
Hypogastric
ganglion
Hypogastric
nerve internal sphincter relaxes Urethra
External sphincter
Parasympathetic nerve supply
S2
S3
S4
S2
S3
S4
Pelvic nerve contraction of the detrussor muscle
Pudendal nerve external sphincter relaxes
Somatic nerve supply
Bladder Anatomy and Physiology
ETIOLOGY OAB
The knowledge of OAB is incomplete.The etiology of OAB is complex and poorly
understood.Neurological hypothesis.The myogenic hypothesis.Increased sensitivity of afferent nerves.

Neurological hypothesisMost of the time the bladder control is modulated in an
inhibitory fashion by the dienchephalic and cerebral cortex.
• damage to the brain can induce DO by reducing
suprapontine inhibition.• damage to axonal pathways in the spinal cord allows
the expression of primitive spinal bladder reflexes. • synaptic plasticity leads to reorganization of sacral
activity, with the emergence

The myogenic hypothesisStructural deformation of detrusor muscle, Increased production of (NGF) → → growth and
maintenance of sympathetic and sensory neurones,
Partial denervation (denervation superactivity), Metabolic effects (free radicals, lipid
peroxidases). Detrusor hypertrophy (↑metabolic demands,
↓ blood flow → ischamia and anoxia neurones).

Increased sensitivity of afferent nerves
Low Ph, increased urine osmolality → release of mediators as: nitric oxide and neurokinin A → sensitization of submucosal afferents.
Sensitization of C-fiber (unmyelinated) afferents.

Clinical Evaluation

Clinical Evaluation
The diagnosis of OAB is symptom based and involves: Careful history, physical exam, Urinalysis.
Urodynamics, cystoscopy and diagnostic renal and bladder ultrasound should not be used in the initial workup of the uncomplicated patient.
Urodynamic study or cystoscopy Refractory or complicated cases of OAB Prior to invasive surgery.

Urodynamic study

Urodynamic findings:
-Cystometry: spontaneous bladder contractions during the filling phase → → ↑ intravesical pressure.
Ambulatory urodynamic monitoring is better than the conventional filling cystometry, as motor overactivity of the detrusor is more frequently detected.

Differential Diagnosis of OAB
Men Benign prostatic
hyperplasia (BPH) Prostate cancer Diabetes Postsurgical incontinence Bladder outlet
obstruction (BOO) Urethral stricture Neurogenic bladder Bladder stones
WomenUTIBladder cancerDiabetesMultiple sclerosisSUIRecent pelvic surgeryNeurogenic bladderProlapseUrethral obstructionAtrophic vaginitisPostsurgical incontinence


Treatment of OAB

Treatment of OAB
First-Line Treatments - Behavioral therapySecond-Line Treatments -Medication -Combined therapy: behavioral and pharmacologic
therapyThird-line Treatments:
– Botulinum A-toxin– Neuromodulation
Additional Treatments: -Augmentation cystoplasty or urinary diversion

Behavioral Modifications
Dietary ChangesFluid ManagementPelvic Muscle Exercises (Kegel exercises)BiofeedbackBladder Retraining.

Anticholinergic AgentsOxybutyninOxybutynin transdermalTolterodineSolifenacin Trospium chlorideDarifenacin
Medication

Darifenacin Trospium chloride
Solifenacin Tolterodine Oxybutynin
Tertiary amine Quaternary amine
Tertiary amine Tertiary amine Tertiary amine Chemical stracture
More M3 selective
Non selective Non selective Non selective Non selective Receptor
Poor 20% Poor 10% Good 90% Good 75% Poor 15% Oral bioaviablity
13- 19hours 12- 20hours 45- 86hours 2hoursER 9hrs
2hourspatch8hrsER 12hrs
Half-life
7.5-15 mg/Day
20-40 mg/Day 5-10 mg/Day 1-2 mg Twice Day
5 mg 3 times Day
Dosing
•Dry mouth Constipation
•Dry mouth•Constipation
•Dry mouth•Constipation
•Dry mouth•Constipation• Blurred vision• Drowsiness
•Dry mouth•Constipation• Blurred vision• Drowsiness
Side effects

Oxybutynin Transdermal
Translucent matrix-type patch Twice-weekly application


Intravesical BTX InjectionBotox can suppress ACh release from cholinergic
terminalsBotox can inhibit aberrant sensory neurotransmitter Botox can treat OAB in both sensory and motorResponse rate in non-neurogenic OAB about 60-80%
with duration of response around 6-12 months. Risk of urinary retentionAnd Patients may need to self catheterise

Intradetrusor onabotulinumtoxinA 100 units diluted in 10ml saline in 30 injection sites

Sacral NeuromodulationSacral nerve stimulation InterStim®: Implanted neurostimulation of sacral nervesS3:Stimulation of the sacral roots has effectively
suppressed the hyperactivity, relying on the known reflex response of the detrusor muscle to stimulate the somatic component of the sacral plexus (which aborts and inhibits detrusor contractilit
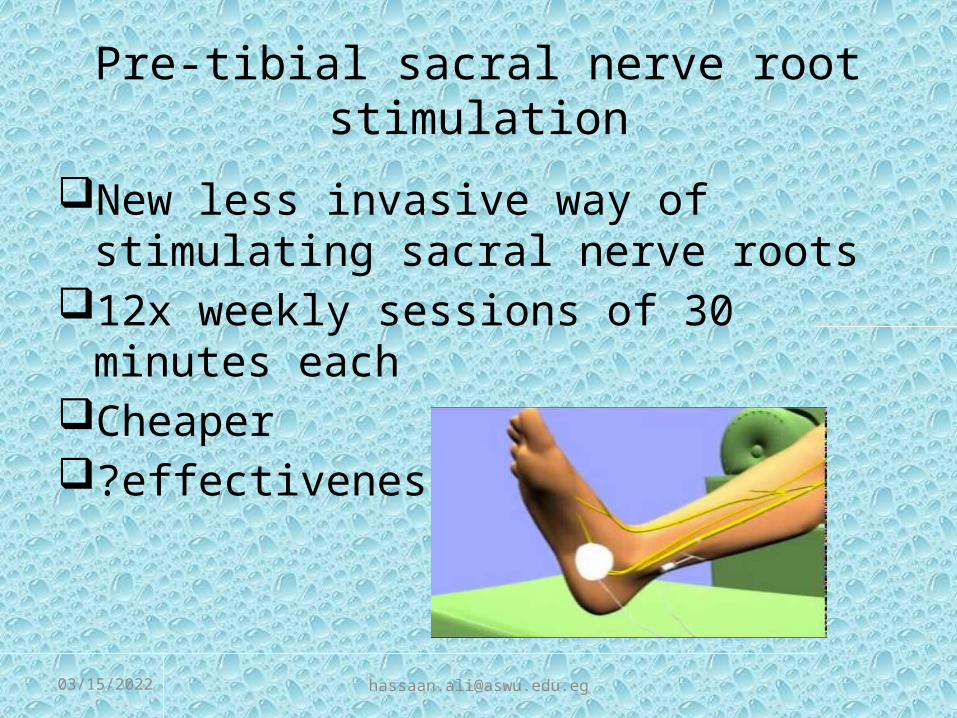
Pre-tibial sacral nerve root stimulation
New less invasive way of stimulating sacral nerve roots
12x weekly sessions of 30 minutes eachCheaper ?effectiveness

Additional Treatments:
Indwelling catheters (including transurethral, suprapubic, etc.) are not recommended as a management strategy for OAB because of the adverse risk/benefit balance except as a last resort in selected patients.In rare cases, augmentation cystoplasty or urinary diversion for severe, refractory, complicated OAB patients may be considered.

Resources
• American Urological Association (AUA)• www.auanet.org
• International Continence Society (ICS)• www.icsoffice.org
• Society for Urodynamics & Female Urology (SUFU)
• www.sufuorg.com
• American Urogynecological Society (AUGS)• www.augs.org

THANK YOU



![[MS-OXPFOAB]: Offline Address Book (OAB) Public Folder ...... · offline address book (OAB). The Offline Address Book (OAB) Public Folder Retrieval Protocol enables OAB data to be](https://static.fdocuments.us/doc/165x107/5f0b91d77e708231d4312968/ms-oxpfoab-offline-address-book-oab-public-folder-offline-address.jpg)