Downloaded from on January 28, 2020 by ... · Page 2 27 Abstract: 28 Crimean-Congo hemorrhagic...
23
Page 1 Low-Density Macroarray for Rapid Detection and Identification of 1 Crimean-Congo Hemorrhagic Fever Virus 2 3 Crimean-Congo Hemorrhagic Fever Virus Macroarray 4 5 Roman Wölfel * , Bundeswehr Institute of Microbiology, Munich, Germany 6 Janusz T. Paweska, National Institute for Communicable Diseases, Sandringham, South Africa 7 Nadine Petersen, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 8 Antoinette A. Grobbelaar, National Institute for Communicable Diseases, Sandringham, South 9 Africa 10 Patricia A. Leman, National Institute for Communicable Diseases, Sandringham, South Africa 11 Roger Hewson, Health Protection Agency, Porton Down, Salisbury, UK 12 Marie-Claude Georges-Courbot, Unit of Biology of Viral Emerging Infections, Institute Pas- 13 teur, Lyon, France 14 Anna Papa, Microbiology Department, Medical School, Aristotle University of Thessaloniki, 15 Greece 16 Volker Heiser, Chipron GmbH, Berlin, Germany 17 Marcus Panning, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 18 Stephan Günther, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 19 Christian Drosten, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 20 21 22 * Dr. Roman Wölfel, Bundeswehr Institute of Microbiology, Dept. for Medical Biological Re- 23 connaissance & Verification, Neuherbergstrasse 11, 80937 Munich, Germany. Phone +49-89- 24 3168-3894, Fax +49-89-3168-3292, Email: [email protected] 25 26 Copyright © 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved. J. Clin. Microbiol. doi:10.1128/JCM.01920-08 JCM Accepts, published online ahead of print on 18 February 2009 on March 2, 2020 by guest http://jcm.asm.org/ Downloaded from
Transcript of Downloaded from on January 28, 2020 by ... · Page 2 27 Abstract: 28 Crimean-Congo hemorrhagic...

Page 1
Low-Density Macroarray for Rapid Detection and Identification of 1
Crimean-Congo Hemorrhagic Fever Virus 2
3
Crimean-Congo Hemorrhagic Fever Virus Macroarray 4
5
Roman Wölfel*, Bundeswehr Institute of Microbiology, Munich, Germany 6
Janusz T. Paweska, National Institute for Communicable Diseases, Sandringham, South Africa 7
Nadine Petersen, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 8
Antoinette A. Grobbelaar, National Institute for Communicable Diseases, Sandringham, South 9
Africa 10
Patricia A. Leman, National Institute for Communicable Diseases, Sandringham, South Africa 11
Roger Hewson, Health Protection Agency, Porton Down, Salisbury, UK 12
Marie-Claude Georges-Courbot, Unit of Biology of Viral Emerging Infections, Institute Pas-13
teur, Lyon, France 14
Anna Papa, Microbiology Department, Medical School, Aristotle University of Thessaloniki, 15
Greece 16
Volker Heiser, Chipron GmbH, Berlin, Germany 17
Marcus Panning, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 18
Stephan Günther, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 19
Christian Drosten, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany 20
21
22
* Dr. Roman Wölfel, Bundeswehr Institute of Microbiology, Dept. for Medical Biological Re-23
connaissance & Verification, Neuherbergstrasse 11, 80937 Munich, Germany. Phone +49-89-24
3168-3894, Fax +49-89-3168-3292, Email: [email protected] 25
26
Copyright © 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.01920-08 JCM Accepts, published online ahead of print on 18 February 2009
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 2
Abstract: 27
Crimean-Congo hemorrhagic fever (CCHF) is a tick-borne viral zoonosis which occurs through-28
out Africa, Eastern Europe, and Asia and results in an approximately 30% fatality rate. A RT-29
PCR assay including a competitive internal control was developed on the basis of the most up-to-30
date genome information. Biotinylated amplification products were hybridised to DNA macroar-31
rays on the surface of polymer supports and hybridisation events were visualized by incubation 32
with a streptavidin-horse radish peroxidase (HRP) conjugate and the formation of a visible sub-33
strate precipitate. Optimal assay conditions were established for detection of as few as 6.3 ge-34
nome copies per reaction. 18 geographic and historic diverse CCHF virus strains representing all 35
clinical relevant isolates were detected. The feasibility of the assay for clinical diagnosis was 36
validated with acute phase patient samples from South Africa, Iran and Pakistan. The assay pro-37
vides a specific, sensitive, and rapid method for CCHF virus detection without requiring sophisti-38
cated equipments. It has usefulness for clinical diagnosis and surveillance of CCHF infections 39
under limited laboratory conditions in developing countries or in field situations. 40
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 3
Introduction 41
Crimean–Congo haemorrhagic fever (CCHF) is a severe viral infection transmitted by hard-42
ticks (Ixodidae) of the genus Hyalomma. It has a case fatality rate around 30% and can be trans-43
mitted from human to human in the nosocomial setting (14,22). The disease is endemic in large 44
areas of Sub-Saharan Africa and the Middle-/Far East, as well as in Eastern Europe. A significant 45
increase of cases has recently been observed in countries such as Kosovo, Albania, Turkey, Iran 46
and Greece (1,9,15-18,20,21,23). The causative CCHF virus is an enveloped, segmented nega-47
tive-stranded RNA virus family Bunyaviridae, genus Nairovirus. It is classified as a biosafety-48
level four agent. 49
Due to clinical similarity between CCHF and other diseases, proper triage and isolation of 50
patients depends on laboratory confirmation (15). Available diagnostic methods include virus 51
culture, antigen-specific enzyme-linked immunoassay (EIA), antibody-specific EIA, and reverse-52
transcription polymerase chain reaction (RT-PCR) (2,4,5,24). Virus detection is necessary in the 53
acute stage of disease and RT-PCR provides the best sensitivity (8). 54
Conventional RT-PCR protocols take up to 8 h for cDNA synthesis, amplification, gel 55
analysis, and in some instances a second round of nested amplification (3,19). Sequencing of RT-56
PCR products is needed for strain identification. Real-time RT-PCR for CCHFV is difficult to 57
develop due to a remarkable genetic variability between virus strains (11,25,26). Current proto-58
cols are often not appropriate for field-based outbreak investigations, and may be difficult to im-59
plement in those countries where CCHF virus is endemic. Simpler, field-compatible assays are 60
required. Such an approach is described here. 61
A robust one-step RT-PCR assay with an internal control was established, using the most 62
recent genome information. Based on our prior experiences (25), the assay was formulated for 63
compatibility with an inexpensive and simple non fluorescent DNA macro array hybridisation 64
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 4
platform. Detection was possible with the naked eye, using simple and robust biotin / strepta-65
vidin-HRP conjugate chemistry in combination with a tetramethyl-benzidine (TMB) substrate 66
resulting in the formation of a clearly visible dark precipitate at array positions where DNA-DNA 67
hybridisations took place. No gel analysis was necessary. The possible patterns of hybridisation 68
spots were sufficiently heterogeneous to facilitate reliable differentiation between virus strains. 69
Validation was done on strain collections from several collaborating biosafety level-four facili-70
ties, essentially covering the full range of global diversity of CCHF virus (Figure 1). Clinical 71
evaluation utilized a comprehensive panel of original clinical samples from confirmed cases of 72
CCHF, collected over almost 20 years by a WHO reference facility. 73
Material and Methods 74
Virus strains 75
Eighteen CCHF virus strains representing all genetic lineages described worldwide (7) were 76
selected from the strain collections of participating laboratories (Table 1). The material was quan-77
tified by real-time RT-PCR (25) and tested by the conventional CCHF virus assay described here. 78
RNA from all strains was successfully amplified. 79
Clinical samples 80
Clinical material was provided by the Special Pathogens Unit of the National Institute for 81
Communicable Diseases, Sandringham, South Africa. A total of 63 serum samples from 31 con-82
firmed CCHF patients, received from 1986 to 2006 and stored at -70°C, were tested. Of the 31 83
confirmed cases of CCHF included in the study, 27 occurred in widely separated locations in 84
South Africa and Namibia, three in Iran, and one in Pakistan. Serum had been collected 1 to 18 85
days (Mean 6 days, SD 2.8 days) after the onset of disease. Viral load of the stored samples was 86
quantified by real-time RT-PCR (25), ranging from 1,6 × 103 to 5 × 10
8 genome copies per mL 87
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 5
(mean 106 genome copies per mL). In addition, a panel of 128 serum samples collected from 88
healthy individuals was also included in the study as negative controls. 89
RNA standards and Internal Control 90
A synthetic RNA standard was generated by amplifying the full S segment of CCHF virus 91
strain BT-958 (EF123122) as described before (13). After TA-cloning in E. coli plasmid pCR2.1 92
(Invitrogen, Germany) and sequencing, a clone with a correct insert sequence was selected and 93
the complete insert including a plasmid-derived T7 promoter was amplified by PCR. RNA was 94
transcribed from the purified PCR product with the MegaScript T7 in vitro transcription kit (Am-95
bion, USA). The DNA template was removed by DNase 1 and RNA was purified by affinity 96
chromatography (RNeasy columns, Qiagen, Germany) before spectrophotometric quantification. 97
A competitive internal control was constructed by overlap-extension PCR as described previously 98
(10). The resulting construct contained a 350 bp fragment of the CCHF virus S segment and 70 99
bp of an unrelated sequence motif. It was cloned back in pCR 2.1 and transferred into RNA as 100
described above. 101
RT-PCR 102
A 50 µL reaction contained 1 X reaction buffer (One-step RT-PCR kit, Qiagen, Germany), 103
200 µmol/L dNTP, 200 nM of each primer as listed in Table 2, 2 µL of one-step RT-PCR kit en-104
zyme mix, and 5 µL RNA extract. For subsequent hybridisation to the macroarrays, a pre-105
formulated biotinylated primer mixture (LCD-Array Kit, Chipron GmbH, Germany) was used 106
instead of the conventional primers. Amplification in a conventional PCR cycler (Primus 25, 107
Peqlab, Germany) comprised 50°C 30 min, 95°C 15 min, 40 cycles of 94°C 30 sec, 55°C 30 sec, 108
72°C 60 sec. 109
Array HybridisationLow Cost, low Density (LCD) DNA macroarrays are based on trans-110
parent, pre-structured polymer supports containing eight identical arrays in well-separated, indi-111
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 6
vidually addressable hybridisation fields (Figure 1 A). The outer dimensions of 50 × 50 mm al-112
lowed the use of economical transmission-light film scanners to generate images with 10 µm 113
resolution for data analysis. Arrays were manufactured by Chipron GmbH using contact-free 114
piezo dispensing technology. Capture probes were spotted in duplicates leading to the formation 115
of a 9 × 9 pattern, with average spot diameters of 325 µm (Figure 1 B). Twenty different CCHF 116
virus-specific capture probes between 16 and 25 nucleotides in length were selected (Table 2). 117
Each probe was designed to detect a broad range of sequence diversity at its binding site, i.e., 118
probes were not designed for specificity but for breadth of detection. Four capture probes for the 119
competitive internal control RT-PCR product were included in each array. Additional functional 120
control probes with an unrelated sequence motif were placed in three corners of each field, in 121
order to visualize successful hybridisation and staining steps, and to provide orientation marks for 122
signal analysis. Hybridisation of biotinylated RT-PCR products, labelling and staining was done 123
with the LCD-Array Detection Kit (Chipron, Germany) according to manufacturers instructions. 124
In brief, 10 µL of the biotinylated RT-PCR products were combined with 24 µL of a formamide-125
based hybridisation buffer. These mixtures were applied to the individual fields of the macroar-126
rays and hybridised for 30 min at 37°C in a standard incubator. Following a 2 min washing step 127
in the supplied wash buffer (low stringency), the arrays were dried for 10 seconds by airstream 128
using a simple compressed-air can. Dried arrays were incubated for 5 minutes (room tempera-129
ture) with the provided labelling solution (HRP-streptavidin conjugate). After a final wash-and-130
dry step (2 min, as above) 30 µl of TMB substrate was added to each field for staining (3 minutes 131
at room temperature). The reaction was stopped by rinsing the chip in the last wash buffer for 10 132
seconds followed by a drying step. 133
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 7
Statistical analysis 134
The Statgraphics Plus 5 Software Package (Umex, Germany) was used for all analysis. Pro-135
bit analysis used as its input dataset the cumulative hit rates in parallel reactions and their respec-136
tive target RNA concentrations. It determined a continuous dose-response relationship (response 137
rate of the assay dependent of the dose of RNA per reaction) with 95% confidence intervals (CI) 138
(12). 139
Results 140
The design of a novel broad-range CCHF virus RT-PCR was based on all 139 full or partial 141
s-gene sequences of CCHF virus as available in GenBank by autumn 2007 (6,7,13). Three addi-142
tional sequences were determined de novo from virus strains kept at several collaborating bio-143
safety-level four laboratories (25). Two conserved binding sites for primers were identified, re-144
sulting in a RT-PCR amplicon of 280 bp. In designing these primers, primer 3´-ends on the third 145
codon position were avoided. Degenerated ("wobble") positions in primers were not used, in or-146
der to guarantee reliable re-synthesis of primers. Instead, mismatched base pairings were adjusted 147
by mixing of defined oligonucleotides. The stable non-Watson-Crick base pairing T:G was not 148
strictly adjusted for. At each of the two binding sites, three differential primers were thus selected 149
which covered in summary the observed range of sequence heterogeneity at the binding sites. 150
The assay was optimized for sensitivity by titration of essential RT-PCR reaction mix com-151
ponents. The assay amplified a broad range of CCHF virus strains (Table 1, data not shown). To 152
determine the analytical sensitivity, limiting log10 dilution series were amplified from represen-153
tative strains Bangui BT-958, Turkey 4348/02, and ArD 39554. Down to 800, 1000 and 780 cop-154
ies per mL, respectively, could be detected. 155
To identify samples with RT-PCR inhibition, a synthetic internal control RNA was de-156
signed. To ensure amplification of the molecule without additional (possibly interfering) primers, 157
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 8
an internal control was chosen that contained the same primer binding sites as CCHF virus (com-158
petitive internal control) (10). To ensure that it did not out-compete even low amounts of virus 159
RNA in the reaction, the control was used at low concentration (see below) and its length was 160
extended over that of the virus, providing an inherent amplification disadvantage. The construct 161
was 350 bp instead of 280 bp in length, through insertion of a random sequence by overlap-162
extension PCR. 163
Functionality was evaluated in cross-titration experiments containing different amounts of 164
CCHF virus RNA and internal control RNA, respectively. When CCHF virus RNA was absent, 165
the internal control was amplified clearly (Figure 2). In the presence of increasing concentrations 166
of CCHF virus RNA, amplification of the internal control was either lower or absent because of 167
competitive inhibition by amplification of the CCHF virus genomic target (Figure 2). With in-168
creasing concentrations of internal control in reactions containing constantly low levels of CCHF 169
virus RNA (60 copies per reaction) it was demonstrated that no inhibition of virus amplification 170
was imposed by competitive effects of the internal control. A working concentration of 200 cop-171
ies of internal control per reaction was chosen for all further assays. 172
Oligonucleotides were now transformed into ready-made reaction mixtures containing pro-173
prietary modifications which allowed hybridisation of amplification products to LCD arrays. The 174
limit of modified RT-PCR was analysed by testing a series of human sera, spiked with synthetic 175
full-length S segment RNA from 100,000 to 10 copies per mL. On each concentration step, five 176
replicate test reactions were conducted and the results subjected to probit analysis. Statistically 177
constant detection could be achieved with as little as 10 copies of RNA per reaction (data not 178
shown). Sporadic detection was possible down to a single copy per reaction. Probit analysis de-179
termined a 95% detection limit of 540 copies per mL of serum, corresponding to 6.3 genome cop-180
ies per reaction (95% CI: 4.3-14.3 copies per assay, p=0.05). 181
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 9
Hybridisation to LCD arrays was evaluated next. All 18 virus reference strains listed in Table 1 182
were amplified and hybridised (Figure 3). Signals after the hybridisation and staining procedure 183
were clearly visible to the naked eye. Repeated testing of a virus sample showed constantly iden-184
tical hybridisation patterns (data not shown). The whole protocol took less than 4 h and up to 48 185
samples could easily be analysed in parallel. Documentation images as shown in Figure 3 were 186
obtained using a standard slide scanner purchased from a department store. Array hybridisation 187
provided the same sensitivity as gel detection, as shown in Figure 2. However, at virus concentra-188
tions below 1,000 copies per reaction, some of the capture probes which generated only weak 189
byridisation signals at higher template concentrations were not visible. This might limit the abil-190
ity to discriminate certain CCHF virus strains in samples with very low viral load. 191
The specificity of the RT-PCR assay was verified using purified genomic nucleic acids 192
from culture supernatant or high-titered patient containing pathogens that cause diseases resem-193
bling CCHF infections: Bacillus anthracis, Bacillus cereus, Bacillus subtilis, Coxiella burnetii, 194
Cytomegalovirus, Dengue virus types1-4, Dugbe virus, Ebola virus strain Gulu, Epstein Barr 195
virus, Hepatitis C virus, Japanese encephalitis virus, Lassa virus strain AV, Leptospira interro-196
gans, Listeria monocytogenes, Monkeypox virus, Neisseria menigitidis, Plasmodium falciparum, 197
Poliomyelitis virus types 1, 2, 3, Rabies virus, Rickettsia prowazekii, Rickettsia rickettsii, Rift 198
Valley Fever virus, Ross River virus, Sindbis Virus, Venezuelan Equine Encephalitis virus, West 199
Nile virus strain Uganda, Yellow Fever virus. None of these materials, including Dugbe virus 200
(strain AF014014), a non-pathogenic Nairovirus related to CCHF virus, showed any reactivity. 201
None of these reactions showed any random reactivity, i.e. additional non-specific bands in gel 202
electrophoresis or background hybridisation (data not shown). 203
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 10
Clinical application 204
A total of 63 serum samples from 31 confirmed CCHF patients, received from 1986 to 205
2006, were tested after they had been stored at -70°C for up to 6 years. Of the 31 confirmed cases 206
of CCHF included in the study, 27 occurred in widely separated locations in South Africa and 207
Namibia, three in Iran, and one in Pakistan. Serum had been collected 1 to 18 days (Mean 6 days, 208
SD 2.8 days) after the onset of disease. Viral load of the stored samples was quantified by real-209
time RT-PCR (25), ranging from 1,6 × 103 to 5 × 10
8 genome copies per mL (mean 10
6, SD 20 210
genome copies per mL). All samples were positive in all assays. Serial samples of same patients 211
showed identical hybridisation patterns (Figure 4). All tested clinical samples from different 212
CCHF endemic regions could be distinguished on the basis of their hybridisation pattern (com-213
pare Figure 3). 214
A panel of 128 serum samples collected from healthy individuals was also used as negative 215
controls. All negative samples showed amplification of the internal control, but no CCHF virus-216
specific signal in the hybridisation assay (data not shown). 217
Discussion 218
The remarkable genetic variability of all known CCHF virus isolates involves a risk of hu-219
man infection by divergent strains which current protocols may not detect. At the same time, 220
even very simple versions of current assays may fail in basic laboratory settings typically encoun-221
tered in countries were CCHF is endemic. Compared to current molecular assays such as nested 222
RT-PCR or real-time RT-PCR, the identification of the amplicons by hybridisation to up to 20 223
different capture probes gives additional sequence verification. Compared to real-time RT-PCR it 224
is more reliable for new virus strains, which may not be conserved at the binding site of a single 225
hybridisation probe. The assay does not depend on expensive lab infrastructure and therefore it 226
can be applied more easily in basic laboratory settings or in the field. The use of an array of short 227
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 11
DNA capture probes (16–25 nt in length) gives a basic genotyping capacity, even though it may 228
not be sufficient for final CCHF virus strain characterization especially in samples with low viral 229
load (compare Figure 2). Nevertheless, preliminary genotyping can be very helpful in a diagnos-230
tic situation when a possible PCR contamination has to be ruled out as a real positive reaction in 231
most cases will provide a hybridisation pattern different from the positive control. The assay pro-232
vides an economical, rapid, and convenient method to identify CCHF virus in acute phase human 233
serum samples without requiring sophisticated equipment. It might prove useful for clinical diag-234
nosis and surveillance of CCHF under basic laboratory conditions in developing countries or in 235
outbreak investigations. 236
Acknowledgments 237
The research described herein is part of the Medical Biological Defence Research Program 238
of the Bundeswehr Joint Medical Service. It was sponsored in parts by the European Union 239
Framework Program 6 (EU FP6) “Viral Haemorrhagic Fevers/Variola-PCR”. Opinions, interpre-240
tations, conclusions, and recommendations are those of the authors and are not necessarily en-241
dorsed by any governmental agency, department or other institutions. 242
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 12
References 243
1. Alavi-Naini, R., A. Moghtaderi, H. R. Koohpayeh, B. Sharifi-Mood, M. Naderi, M. 244
Metanat, and M. Izadi. 2006. Crimean-Congo hemorrhagic fever in Southeast of Iran. 245
J.Infect. 52:378-382. 246
2. Burt, F. J., P. A. Leman, J. C. Abbott, and R. Swanepoel. 1994. Serodiagnosis of Cri-247
mean-Congo haemorrhagic fever. Epidemiol.Infect. 113:551-562. 248
3. Burt, F. J., P. A. Leman, J. F. Smith, and R. Swanepoel. 1998. The use of a reverse 249
transcription-polymerase chain reaction for the detection of viral nucleic acid in the diag-250
nosis of Crimean-Congo haemorrhagic fever. J.Virol.Methods 70:129-137. 251
4. Burt, F. J., R. Swanepoel, and L. E. Braack. 1993. Enzyme-linked immunosorbent as-252
says for the detection of antibody to Crimean-Congo haemorrhagic fever virus in the sera 253
of livestock and wild vertebrates. Epidemiol.Infect. 111:547-557. 254
5. Casals, J. and G. H. Tignor. 1974. Neutralization and hemagglutination-inhibition tests 255
with Crimean hemorrhagic fever-Congo virus. Proc.Soc.Exp.Biol.Med. 145:960-966. 256
6. Chamberlain, J., N. Cook, G. Lloyd, V. Mioulet, H. Tolley, and R. Hewson. 2005. Co-257
evolutionary patterns of variation in small and large RNA segments of Crimean-Congo 258
hemorrhagic fever virus. J.Gen.Virol. 86:3337-3341. 259
7. Deyde, V. M., M. L. Khristova, P. E. Rollin, T. G. Ksiazek, and S. T. Nichol. 2006. 260
Crimean-Congo hemorrhagic fever virus genomics and global diversity. J.Virol. 80:8834-261
8842. 262
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 13
8. Drosten, C., S. Gottig, S. Schilling, M. Asper, M. Panning, H. Schmitz, and S. Gun-263
ther. 2002. Rapid detection and quantification of RNA of Ebola and Marburg viruses, 264
Lassa virus, Crimean-Congo hemorrhagic fever virus, Rift Valley fever virus, dengue vi-265
rus, and yellow fever virus by real-time reverse transcription-PCR. J.Clin.Microbiol. 266
40:2323-2330. 267
9. Drosten, C., D. Minnak, P. Emmerich, H. Schmitz, and T. Reinicke. 2002. Crimean-268
Congo hemorrhagic fever in Kosovo. J.Clin.Microbiol. 40:1122-1123. 269
10. Drosten, C., M. Weber, E. Seifried, and W. K. Roth. 2000. Evaluation of a new PCR 270
assay with competitive internal control sequence for blood donor screening. Transfusion 271
40:718-724. 272
11. Duh, D., A. Saksida, M. Petrovec, I. Dedushaj, and T. vsic-Zupanc. 2006. Novel one-273
step real-time RT-PCR assay for rapid and specific diagnosis of Crimean-Congo hemor-274
rhagic fever encountered in the Balkans. J.Virol.Methods 133:175-179. 275
12. Fink, H. and G. Hund. 1965. [Probit analysis with programmed computers]. Arzneimit-276
telforschung. 15:624-630. 277
13. Hewson, R., J. Chamberlain, V. Mioulet, G. Lloyd, B. Jamil, R. Hasan, A. Gmyl, L. 278
Gmyl, S. E. Smirnova, A. Lukashev, G. Karganova, and C. Clegg. 2004. Crimean-279
Congo haemorrhagic fever virus: sequence analysis of the small RNA segments from a 280
collection of viruses world wide. Virus Res. 102:185-189. 281
14. Hoogstraal, H. 1979. The epidemiology of tick-borne Crimean-Congo hemorrhagic fever 282
in Asia, Europe, and Africa. J.Med.Entomol. 15:307-417. 283
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 14
15. Jamil, B., R. S. Hasan, A. R. Sarwari, J. Burton, R. Hewson, and C. Clegg. 2005. 284
Crimean-Congo hemorrhagic fever: experience at a tertiary care hospital in Karachi, Paki-285
stan. Trans.R.Soc.Trop.Med.Hyg. 99:577-584. 286
16. Karti, S. S., Z. Odabasi, V. Korten, M. Yilmaz, M. Sonmez, R. Caylan, E. Akdogan, 287
N. Eren, I. Koksal, E. Ovali, B. R. Erickson, M. J. Vincent, S. T. Nichol, J. A. Comer, 288
P. E. Rollin, and T. G. Ksiazek. 2004. Crimean-Congo hemorrhagic fever in Turkey. 289
Emerg.Infect.Dis. 10:1379-1384. 290
17. Papa, A., S. Bino, A. Llagami, B. Brahimaj, E. Papadimitriou, V. Pavlidou, E. Velo, 291
G. Cahani, M. Hajdini, A. Pilaca, A. Harxhi, and A. Antoniadis. 2002. Crimean-292
Congo hemorrhagic fever in Albania, 2001. Eur.J.Clin.Microbiol.Infect.Dis. 21:603-606. 293
18. Papa, A., I. Christova, E. Papadimitriou, and A. Antoniadis. 2004. Crimean-Congo 294
hemorrhagic fever in Bulgaria. Emerg.Infect.Dis. 10:1465-1467. 295
19. Rodriguez, L. L., G. O. Maupin, T. G. Ksiazek, P. E. Rollin, A. S. Khan, T. F. 296
Schwarz, R. S. Lofts, J. F. Smith, A. M. Noor, C. J. Peters, and S. T. Nichol. 1997. 297
Molecular investigation of a multisource outbreak of Crimean-Congo hemorrhagic fever 298
in the United Arab Emirates. Am.J.Trop.Med.Hyg. 57:512-518. 299
20. Schwarz, T. F., H. Nitschko, G. Jager, H. Nsanze, M. Longson, R. N. Pugh, and A. K. 300
Abraham. 1995. Crimean-Congo haemorrhagic fever in Oman. Lancet 346:1230. 301
21. Schwarz, T. F., H. Nsanze, and A. M. Ameen. 1997. Clinical features of Crimean-302
Congo haemorrhagic fever in the United Arab Emirates. Infection 25:364-367. 303
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 15
22. Swanepoel, R., D. E. Gill, A. J. Shepherd, P. A. Leman, J. H. Mynhardt, and S. Har-304
vey. 1989. The clinical pathology of Crimean-Congo hemorrhagic fever. Rev.Infect.Dis. 305
11 Suppl 4:S794-S800. 306
23. Swanepoel, R., J. K. Struthers, A. J. Shepherd, G. M. McGillivray, M. J. Nel, and P. 307
G. Jupp. 1983. Crimean-congo hemorrhagic fever in South Africa. Am.J.Trop.Med.Hyg. 308
32:1407-1415. 309
24. Whitehouse, C. A. 2004. Crimean-Congo hemorrhagic fever. Antiviral Res. 64:145-160. 310
25. Wolfel, R., J. T. Paweska, N. Petersen, A. A. Grobbelaar, P. A. Leman, R. Hewson, 311
M. C. Georges-Courbot, A. Papa, S. Gunther, and C. Drosten. 2007. Virus detection 312
and monitoring of viral load in Crimean-Congo hemorrhagic fever virus patients. 313
Emerg.Infect.Dis. 13:1097-1100. 314
26. Yapar, M., H. Aydogan, A. Pahsa, B. A. Besirbellioglu, H. Bodur, A. C. Basustaoglu, 315
C. Guney, I. Y. Avci, K. Sener, M. H. Setteh, and A. Kubar. 2005. Rapid and quantita-316
tive detection of Crimean-Congo hemorrhagic fever virus by one-step real-time reverse 317
transcriptase-PCR. Jpn.J.Infect.Dis. 58:358-362. 318
319
320
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 16
Figures: 321
322
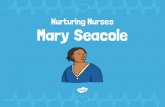
FIG. 1. Schematic diagram of microarray. A: Illustration of the 50 × 50 mm polymer support 323
with the eight identical, individually addressable array fields. B: Spotting pattern of one array 324
field. 20 CCHF virus-specific capture probes were spotted as vertical duplicates in a 9 × 9 pattern 325
with average spot diameters of 325 µm (positions 1-20). Four capture probes for the competitive 326
internal control RT-PCR product are included at the bottom of each array (positions 21). Addi-327
tional functional control probes to visualize successful hybridisation and staining are immobilized 328
in three angles of each field (positions ‘C’). 329
330
FIG. 2. RT-PCR amplification with the CCHF virus-specific assay (280-bp amplicon) and 331
the internal control (350-bp amplicon). A: Conventional 1.5% agarose gel analysis of the RT-332
PCR products. B: Specific hybridisation pattern of the same RT-PCR products on the macroarray. 333
Lane M: 100-bp molecular size ladder; lanes/fields 1-3: CCHF virus strain BT-958 in-vitro tran-334
scribed RNA, lane/field 1: 6 × 106 copies per reaction (cps/rx), lane/field 2: 6 × 10
4 cps/rx, 335
lane/field 3: 6 cps/rx; lane/field 4: internal control RNA only; lane/field 5: control to which no 336
RNA was added. Note that both analysis methods visualize the suppression of the internal control 337
amplification by increasing concentrations of CCHF virus target RNA. 338
339
340
341
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 17
FIG. 3. A, Global distribution and phylogenetic relationships of CCHF virus strains se-342
lected for the design and validation of the assay: Phylogenetic analysis was based on NCBI-343
available 450bp sequences of CCHF virus small (S) segment and generated by the neighbour-344
joining method with TreeCon for Windows Version 1.3b (Yves van de Peer, University Kon-345
stanz, Germany). * These CCHF virus strains were not available for testing with the novel uni-346
versal CCHF virus qRT-PCR assay, but genetically closely related isolates have been tested. ** 347
Strain AP92 has also not been available for testing. It was isolated from a Rhipicephalus bursa 348
tick and has never been associated with human disease. 349
B, Representative hybridisation patterns of CCHF virus strains listed in table 2: Different 350
strains of CCHF virus show individual hybridisation patterns on the macroarray. However these 351
patterns are based only on sequence variability within an approximately 25-nt region of the 352
CCHF virus S segment. Therefore they cannot be considered unique for a specific CCHF virus 353
strain as shown in patterns 5 and 6. Dugbe virus, a non-pathogenic Nairovirus closely related to 354
CCHF virus is not detected by the CCHF virus-specific array. Note that the internal control spots 355
are not visible in the CCHF virus patterns as the amplification of the internal control RNA is sup-356
pressed in the presence of high concentrations of CCHF virus RNA (also compare Fig. 2). 357
358
FIG. 4. Serial samples of an acute case of CCHF. This example shows hybridisation patterns 359
obtained from serum samples on days 1, 5 and 9 days after onset of the disease. Viral load of the 360
samples (genome copies per reaction, cps/rx) was quantified by real-time RT-PCR as described 361
before (25). 362
363
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 18
364
365
TABLE 1. CCHF virus strains used for validation of the RT-PCR assay
CCHF virus isolate Origin NCBI-Genbank
Accession No. Log RNA copies per mL
7803 XinJiang China AF354296 5.2
Ug3010 Congo U88416 7.1
ArB 604 "1976" Congo U15092 5.4
SPU 190/00/18 Iran AY905654 5.8
SPU9/00/5 Iran AY905653 6.3
Baghdad-12 Iraq AJ538196 4.5
ArMg951 Madagascar U15024 9.3
ArD39554 Mauritania U15089 7.9
IbAr10200 Nigeria U88410 8.9
SPU 280/02/10 Pakistan AY905663 7.1
SPU 68/98 South Africa AY905639 6.5
SPU 60/89 South Africa AY905636 5.9
SPU 70/01 South Africa AY905650 6.2
SPU 51/01 South Africa AY905649 6.6
4348/02 Turkey DQ211649 4.0
SPU128/81/7 Uganda DQ076415 5.5
Hoti Yugoslavia (Kosovo) DQ133507 4.3
Bangui BT-958 Centralafric. Republic EF123122 6.9
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

Page 19
366
367
TABLE 2. Primer and Probe sequences used for RT-PCR and macroarray hybridi-sation
Name Sequence Position on CCHF virus
strain 10200 (U88410)
CC1a_for 5’-GTGCCACTGATGATGCACAAAAGGATTCCATCT 210-242
CC1b_for 5’-GTGCCACTGATGATGCACAAAAGGATTCTATCT 210-242
CC1c_for 5’-GTGCCACTGATGATGCACAAAAGGACTCCATCT 210-242
CC1a_rev 5’-GTGTTTGCATTGACACGGAAACCTATGTC 489-461
CC1b_rev 5’-GTGTTTGCATTGACACGGAAGCCTATGTC 489-461
CC1c_rev 5’-GTGTTTGCATTGACACGGAAACCTATATC 489-461
CCHF-01 5’-CAACAGGCTGCTCTCAAGTGGAG
CCHF-02 5’-CCAGCAGGCTGCTCTCAAGTGG
CCHF-03 5’-CCAACAAGCTGCCTTGAAATGG
CCHF-04 5’-CCAACAGGCTGCCTTGAAATGG
CCHF-05 5’-CCAACAGGCTGCTCTAAAGTGGAG
CCHF-06 5’-CCAACAAGCTGCCTTGAAGTGG
CCHF-07 5’-CAGCAGGCTGCTCTCAAGTGG
CCHF-08 5’-CAGCAGGCCGCTCTCAAGTG
CCHF-09 5’-CAACAGGCTGCTCTCAAATGGAG
CCHF-10 5’-CCAACATGCTGCTCTCAAGTGGA
CCHF-11 5’-AGCAAGCTGCCCTCAAGTGGA
CCHF-12 5’-TCAACAGGCTGCTCTAAAGTGGAGA
CCHF-13 5’-AGCAGGCAGCCCTCAAGTGG
CCHF-14 5’-CAACAAGCCGCCTTAAAGTGGAG
CCHF-15 5’-CAACAAGCCGCCTTGAAGTGG
CCHF-16 5’-CAACAGGCTGCCTTGAAGTGGA
CCHF-17 5’-CAACAGGCTGCTTTGAAATGGAG
CCHF-18 5’-CCAGCAGGCTGCTCTGAAGTG
CCHF-19 5’-CCAGCAGGCTGCTCTAAAGTGG
CCHF-20 5’-GCAGGCCGCCCTCAAGTG
434-456
on March 2, 2020 by guest
http://jcm.asm
.org/D
ownloaded from