Down Syndrome and the Risk of Severe RSV Infection: A Meta ...Down Syndrome and the Risk of Severe...
12
Division of Pediatrics, Department of Pediatric Pulmonology and Cardiology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile Dr Beckhaus reviewed and collected the data, conducted the analyses, drafted the initial manuscript, and reviewed and revised the manuscript; Dr Castro-Rodriguez conceptualized and designed the study, reviewed the data, drafted the initial manuscript, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. DOI: https://doi.org/10.1542/peds.2018-0225 To cite: Beckhaus AA and Castro-Rodriguez JA. Down Syndrome and the Risk of Severe RSV Infection: A Meta-analysis. Pediatrics. 2018;142(3):e20180225 CONTEXT: Down syndrome (DS) is the most common chromosomal condition in live-born infants worldwide, and lower respiratory infection caused by respiratory syncytial virus (RSV) is a leading cause of hospital admissions. OBJECTIVE: To evaluate RSV-associated morbidity among children with DS compared with a population without DS. DATA SOURCES: Four electronic databases were searched. STUDY SELECTION: All cohorts or case-control studies of DS with an assessment of RSV infection and the associated morbidity or mortality were included without language restriction. DATA EXTRACTION: Two reviewers independently reviewed all studies. The primary outcomes were hospital admission and mortality. Secondary outcomes included length of hospital stay, oxygen requirement, ICU admission, need for respiratory support, and additional medication use. RESULTS: Twelve studies ( n = 1 149 171) from 10 different countries met the inclusion criteria; 10 studies were cohort studies, 1 study was retrospective, and 1 study had both designs. DS was associated with a higher risk of hospitalization (odds ratio [OR]: 8.69; 95% confidence interval [CI]: 7.33–10.30; I 2 = 11%) and mortality (OR: 9.4; 95% CI: 2.26 –39.15; I 2 = 38%) compared with what was seen in controls. Children with DS had an increased length of hospital stay (mean difference: 4.73 days; 95% CI: 2.12–7.33; I 2 = 0%), oxygen requirement (OR: 6.53; 95% CI: 2.22–19.19; I 2 = 0%), ICU admission (OR: 2.56; 95% CI: 1.17–5.59; I 2 = 0%), need for mechanical ventilation (OR: 2.56; 95% CI: 1.17–5.59; I 2 = 0%), and additional medication use (OR: 2.65 [95% CI: 1.38–5.08; I 2 = 0%] for systemic corticosteroids and OR: 5.82 [95% CI: 2.66 –12.69; I 2 = 0%] for antibiotics) than controls. LIMITATIONS: DS subgroups with and without other additional risk factors were not reported in all of the included studies. CONCLUSIONS: Children with DS had a significantly higher risk of severe RSV infection than children without DS. Down Syndrome and the Risk of Severe RSV Infection: A Meta-analysis Andrea A. Beckhaus, MD, Jose A. Castro-Rodriguez, MD, PhD abstract PEDIATRICS Volume 142, number 3, September 2018:e20180225 REVIEW ARTICLE by guest on June 30, 2020 www.aappublications.org/news Downloaded from
Transcript of Down Syndrome and the Risk of Severe RSV Infection: A Meta ...Down Syndrome and the Risk of Severe...

Division of Pediatrics, Department of Pediatric Pulmonology and Cardiology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
Dr Beckhaus reviewed and collected the data, conducted the analyses, drafted the initial manuscript, and reviewed and revised the manuscript; Dr Castro-Rodriguez conceptualized and designed the study, reviewed the data, drafted the initial manuscript, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 0225
To cite: Beckhaus AA and Castro-Rodriguez JA. Down Syndrome and the Risk of Severe RSV Infection: A Meta-analysis. Pediatrics. 2018;142(3):e20180225
CONTEXT: Down syndrome (DS) is the most common chromosomal condition in live-born infants worldwide, and lower respiratory infection caused by respiratory syncytial virus (RSV) is a leading cause of hospital admissions.OBJECTIVE: To evaluate RSV-associated morbidity among children with DS compared with a population without DS.DATA SOURCES: Four electronic databases were searched.STUDY SELECTION: All cohorts or case-control studies of DS with an assessment of RSV infection and the associated morbidity or mortality were included without language restriction.DATA EXTRACTION: Two reviewers independently reviewed all studies. The primary outcomes were hospital admission and mortality. Secondary outcomes included length of hospital stay, oxygen requirement, ICU admission, need for respiratory support, and additional medication use.RESULTS: Twelve studies (n = 1 149 171) from 10 different countries met the inclusion criteria; 10 studies were cohort studies, 1 study was retrospective, and 1 study had both designs. DS was associated with a higher risk of hospitalization (odds ratio [OR]: 8.69; 95% confidence interval [CI]: 7.33–10.30; I2 = 11%) and mortality (OR: 9.4; 95% CI: 2.26–39.15; I2 = 38%) compared with what was seen in controls. Children with DS had an increased length of hospital stay (mean difference: 4.73 days; 95% CI: 2.12–7.33; I2 = 0%), oxygen requirement (OR: 6.53; 95% CI: 2.22–19.19; I2 = 0%), ICU admission (OR: 2.56; 95% CI: 1.17–5.59; I2 = 0%), need for mechanical ventilation (OR: 2.56; 95% CI: 1.17–5.59; I2 = 0%), and additional medication use (OR: 2.65 [95% CI: 1.38–5.08; I2 = 0%] for systemic corticosteroids and OR: 5.82 [95% CI: 2.66–12.69; I2 = 0%] for antibiotics) than controls.LIMITATIONS: DS subgroups with and without other additional risk factors were not reported in all of the included studies.CONCLUSIONS: Children with DS had a significantly higher risk of severe RSV infection than children without DS.
Down Syndrome and the Risk of Severe RSV Infection: A Meta-analysisAndrea A. Beckhaus, MD, Jose A. Castro-Rodriguez, MD, PhD
abstract
PEDIATRICS Volume 142, number 3, September 2018:e20180225 REVIEW ARTICLE by guest on June 30, 2020www.aappublications.org/newsDownloaded from

Acute lower respiratory tract infections (LRTIs) are a leading cause of hospital admissions and pediatric mortality worldwide.1 Respiratory syncytial virus (RSV) accounts for a great majority of cases, affecting 70% of children <1 year of age and nearly 100% of children <2 years of age.2 Acute respiratory infections caused by RSV, particularly acute bronchiolitis, create an important economic burden (with a high number of visits to emergency units and outpatient clinics), requiring hospital admissions in up to 3% of cases.3, 4
Down syndrome (DS) is the most common chromosomal condition, with a worldwide estimated incidence of 1 in 800 live births.5 In the United States, the live birth prevalence of DS in recent years (2006–2010) was estimated at 12.6 per 10 000 live births (95% confidence interval [CI]: 12.4–12.8), with ∼5300 births annually.6 Respiratory problems are a frequent cause of morbidity and mortality in this population. Respiratory morbidity includes airway obstruction with consequent sleep-related breathing disorders as well as recurrent respiratory infections with a wide range of severity, including viral upper respiratory tract infections, viral or bacterial LTRIs, and wheezing disorders.5 Children with DS may suffer from certain anatomic abnormalities, such as macroglossia, pharyngeal hypotonia, adenoid enlargement, and airway malacia, which may be associated with other underlying conditions, such as gastroesophageal reflux, swallowing dysfunction, congenital heart disease (CHD), hypotonia, and immunologic dysfunction.5 All these factors contribute to the respiratory morbidity observed in DS. Respiratory infections are the leading cause of hospitalization in children with DS.7 Most individuals who are affected have at least 1 hospital admission, with multiple
hospitalizations being common. A high proportion of these occur during the first year of life8 and are associated with significant costs.9
Therefore, our objective in this systematic review is to evaluate RSV-associated morbidity in children with DS compared with those without DS.
METHODS
Search and Selection Criteria
We searched 4 electronic databases (Medline, the Cochrane Central Register of Controlled Trials, Latin American and Caribbean Literature on Health Sciences database, and the Cumulative Index to Nursing and Allied Health Literature) up to May 2017. The search was conducted by using the following keywords: (Down syndrome) AND (respiratory syncytial virus) OR (respiratory infection). We also searched other nonbibliographic data sources, such as through Web searching, references of the included publications, and pharmaceutical industry Web sites. The inclusion criteria were (1) cohorts or case-control (C-C) studies of DS, (2) assessment of RSV infection (by any laboratory diagnosis test) and the associated morbidity, and (3) no language restriction. The exclusion criteria were (1) no specific RSV analysis, (2) a DS morbidity description with an absence of a control group (CG) with which to compare, and (3) reviews, letters, or abstracts because of the lack of full information about the included studies. The primary outcomes in this systematic review were hospital admission and mortality. Secondary outcomes included length of hospital stay (LOS), oxygen requirement, admission to the ICU, need for respiratory support, and additional medication use (ie, in addition to the patient’s baseline). When data from participants with DS without additional risk factors (eg, CHD or prematurity) were reported, the
group without any additional risk factors was used for calculations.
Data Abstraction and Assessment of Risk of Bias
Titles, abstracts, and citations were independently analyzed by 2 independent investigators (A.A.B. and J.A.C.R.), and any disagreement was resolved after discussion. From the full texts, the reviewers independently assessed all studies for inclusion on the basis of the criteria for population intervention, study design, and outcomes. After obtaining full reports about potentially relevant trials, they independently assessed eligibility. If the information was incomplete, they attempted to contact the authors. The risk of bias from including certain studies was assessed according to the Newcastle–Ottawa scale.10
Data Analysis
We calculated pooled odds ratios (ORs) with 95% CIs for categorical outcomes and mean differences with 95% CIs for continuous outcomes. Heterogeneity was assessed by using the I2 test (≤25% absence of bias, 26%–39% unimportant, 40%–60% moderate, and 60%–100% substantial bias).11 For all outcomes measured, a fixed-effects meta-analysis was used when low heterogeneity was present (I2 < 40%), and a random-effects meta-analysis was performed when high heterogeneity was detected (I2 ≥ 40%) to address the variation across the included studies. Data from cohort and retrospective studies were pooled together and into separate meta-analyses. The meta-analyses were performed by using Review Manager 5.3 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark).
RESULTS
A total of 36 studies were initially identified in the databases and other
BECKHAUS and CASTRO-RODRIGUEZ2 by guest on June 30, 2020www.aappublications.org/newsDownloaded from

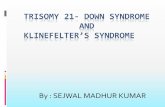
sources (Fig 1). After excluding 3 duplicates, we reviewed 33 abstracts. Eighteen studies were excluded because they did not meet inclusion criteria. Fifteen full-text articles were evaluated, and after excluding 3 studies, 12 studies fulfilled the inclusion criteria for the qualitative and quantitative synthesis. These 12 studies (n = 1 149 171 children: 3662 children with DS and 1 145 509 children without DS) were published from 2004 to 2017.12 – 23 Ten studies were cohort studies, 12 – 16, 18– 20, 22, 23 1 study was a C-C study, 21 and 1 study had both designs.17 Most studies included participants up to 2 years of age, 12 – 14, 16, 17, 22, 23 whereas some studies included all pediatric ages.15, 18 – 21 Six studies were conducted in Europe, 12 –14, 16, 22, 23 3 studies were conducted in Asia, 15, 18, 21 2 studies were conducted in the United States, 17, 19 and 1 study was
conducted in Latin America.20 A detailed description of these 12 studies is shown in Table 1, and a description of our quality assessment is presented in Table 2.
Primary Outcomes
Hospital Admissions
The authors of 6 studies reported differences in RSV hospital admissions between children with DS and children without DS.12, 13, 16, 19, 22, 23 DS was associated with higher odds of admission (pooled OR: 8.69; 95% CI: 7.33–10.30; I2 = 11%) with the absence of bias (Fig 2). Excluding studies with no description of additional risk factors and studies that included a population with DS with known additional risk factors, the same results were obtained (pooled OR: 16.66; 95% CI: 7.22–38.46; I2 = 0%).13, 22 The authors of 1 study reported that
the age distribution also tended to be different between both groups, with children with DS continuing to have more hospitalizations for RSV during their second year of life than controls.22 Similar results were obtained when only data from prospective studies were analyzed (data not shown).
The authors of 1 study compared children with CHD with children with DS who had CHD or did not have CHD. The study revealed that DS appeared to be associated with a higher risk of hospital admission compared with CHD without DS (OR: 1.89; 95% CI: 1.30–2.74).14
Mortality
The authors of 5 studies reported RSV mortality.12, 20 –23 Children with DS had a statistically increased risk of mortality than children without DS (pooled OR: 9.4; 95% CI: 2.26–39.15;
PEDIATRICS Volume 142, number 3, September 2018 3
Records iden�fied by searching databases (n = 36)
Addi�onal records iden�fied in other sources (n = 0)
Records a�er duplicates were eliminated (n = 33)
Examined abstracts (n = 33)
Excluded records (n = 18)
Full-text ar�cles in which eligibility was evaluated (n = 15)
Full-text ar�cles excluded; did not meet inclusion criteria or met
exclusion criteria (n = 3)
Studies included in qualita�ve synthesis (n = 12)
Studies included in quan�ta�ve synthesis (meta-analysis)
(n = 12)
FIGURE 1Process of study selection.
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

BECKHAUS and CASTRO-RODRIGUEZ4
TABL
E 1
Sum
mar
y of
Incl
uded
Stu
dies
Auth
or, y
Coun
try
Stud
y De
sign
Incl
uded
Par
ticip
ants
Outc
omes
No. P
artic
ipan
ts, n
Age
Fjae
rli e
t al, 12
20
04No
rway
RCCh
ildre
n <2
y o
f age
hos
pita
lized
for
RSV
bron
chio
litis
co
mpa
red
with
all
child
ren
<2 y
of a
ge li
ving
in
sam
e ar
ea id
entifi
ed fr
om o
ffici
al p
opul
atio
ns
stat
istic
s an
d ho
spita
l rec
ords
(DS
: 52;
CG:
58 1
27);
DS g
roup
incl
uded
par
ticip
ants
with
add
ition
al r
isk
fact
ors
(4 c
hild
ren
with
CHD
)
Hosp
ital a
dmis
sion
s, m
orta
lity,
ne
ed o
f mec
hani
cal
vent
ilatio
n, L
OS
DS: 5
2; C
G: 5
8 127
DS m
edia
n: 9
mo;
CG
med
ian:
6
mo
Bloe
mer
s et
al, 13
20
07Ne
ther
land
sRC
and
PC
RC: c
hild
ren
with
DS
man
aged
by
DS s
tudy
gro
up,
data
obt
aine
d fr
om m
edic
al r
ecor
ds; P
C: b
irth
pr
ospe
ctiv
e co
hort
of c
hild
ren
with
DS
man
aged
un
til 2
y o
f age
. DS:
with
out a
dditi
onal
ris
k fa
ctor
s 21
6 (1
03 in
ret
rosp
ectiv
e st
udy
and
113
in
pros
pect
ive
stud
y); C
G: 2
76 s
iblin
gs o
f the
bir
th
coho
rt. P
artic
ipan
ts w
ith C
HD a
nd p
rem
atur
ity w
ere
incl
uded
in th
is s
tudy
, but
onl
y th
e no
n–hi
gh-r
isk
popu
latio
n w
ith D
S w
as in
clud
ed in
ana
lysi
s.
Hosp
ital a
dmis
sion
s, m
orta
lity,
ne
ed o
f mec
hani
cal
vent
ilatio
n, n
eed
of
supp
lem
enta
l oxy
gen,
LOS
DS: 2
16; C
G: 2
76DS
ran
ge: 0
–24
mo;
CG
rang
e:
0–24
mo
Med
rano
Lóp
ez
et a
l, 14 2
009
Spai
nPC
Mul
ticen
tric
stu
dy in
clud
ing
indi
vidu
als
with
CHD
and
pa
rtic
ipan
ts w
ith D
S (w
ith a
nd w
ithou
t CHD
) <2
y
of a
ge w
ith L
RTI.
DS: 2
79 (
105
with
out C
HD);
CG:
805.
Indi
vidu
als
with
CHD
wer
e st
udie
d, b
ut th
e pr
emat
urity
con
ditio
n w
as e
xclu
ded.
Hosp
ital a
dmis
sion
s, n
eed
of m
echa
nica
l ven
tilat
ion,
ad
mis
sion
to P
ICU,
LOS
DS: 2
79; C
G: 8
05DS
med
ian:
10
mo;
CG
med
ian:
8.
5 m
o
Meg
ged
and
Schl
esin
ger, 15
20
10
Isra
elRC
Revi
ew o
f med
ical
rec
ords
of 2
22 c
hild
ren
with
DS
hosp
italiz
ed b
ecau
se o
f uns
peci
fied
reas
ons;
CG
was
the
gene
ral p
opul
atio
n w
ith R
SV in
fect
ion
(DS:
22
2; C
G: n
ot r
epor
ted)
; no
desc
ript
ion
of a
dditi
onal
ri
sk fa
ctor
s
Mor
talit
y, n
eed
of m
echa
nica
l ve
ntila
tion,
LOS
DS: 2
22; C
G: n
ot r
epor
ted
—
Kris
tens
en e
t al, 16
20
12De
nmar
kPC
Popu
latio
n-ba
sed
coho
rt s
tudy
to e
valu
ate
risk
and
se
veri
ty o
f RSV
hos
pita
lizat
ion
in c
hild
ren
with
ch
roni
c co
nditi
ons
<2 y
of a
ge (
DS: 3
99; C
G: 4
51 80
6);
no d
escr
iptio
n of
add
ition
al r
isk
fact
ors
Hosp
ital a
dmis
sion
s, m
orta
lity,
LO
SDS
: 399
; CG:
451
806
DS r
ange
: 0–2
3 m
o; C
G ra
nge:
0–
23 m
o
Zach
aria
h et
al, 17
20
12Un
ited
Stat
esRC
and
C-C
RSV
hosp
italiz
atio
n da
ta a
nd b
irth
dat
a of
chi
ldre
n w
ith a
nd w
ithou
t DS
<2 y
of a
ge (
2 di
ffere
nt
data
base
s an
d st
ate
cens
us).
Data
base
1: D
S 63
0;
CG n
ot r
epor
ted.
Dat
abas
e 2:
DS
not r
epor
ted;
CG
not r
epor
ted.
C-C
stu
dy o
f clin
ical
feat
ures
of R
SV
betw
een
DS a
nd n
on-D
S ad
mis
sion
s: D
S 35
(16
w
ithou
t oth
er r
isk
fact
ors)
; CG
48. P
artic
ipan
ts w
ith
CHD
and
prem
atur
ity w
ere
incl
uded
in th
is s
tudy
, bu
t onl
y th
e no
n–hi
gh-r
isk
popu
latio
n w
ith D
S w
as
incl
uded
in a
naly
sis.
Hosp
ital a
dmis
sion
s, n
eed
of
mec
hani
cal v
entil
atio
n, L
OS,
use
of b
ronc
hodi
lato
rs, u
se
of s
yste
mic
cor
ticos
tero
ids,
us
e of
ant
ibio
tics
Data
base
1: D
S 63
0; C
G no
t re
port
ed. D
atab
ase
2: D
S no
t re
port
ed; C
G no
t rep
orte
d.
C-C:
DS
35 (
16 w
ithou
t oth
er
risk
fact
ors)
; CG
48
Data
base
1: D
S ra
nge:
0–2
3 m
o
Zhan
g et
al, 18
20
13Ch
ina
PCCh
ildre
n 1
mo
to 1
4 y
of a
ge a
dmitt
ed to
the
PICU
fo
r se
vere
RSV
LRT
I wer
e m
anag
ed d
urin
g ho
spita
lizat
ion
(DS:
13
[9 w
ithou
t oth
er r
isk
fact
ors]
; CG
158)
; ind
ivid
uals
with
chr
onic
pr
eexi
stin
g co
nditi
ons
wer
e ex
clud
ed in
this
stu
dy.
Need
of v
entil
ator
y su
ppor
t, LO
S in
PIC
U, m
orta
lity
DS: 1
3; C
G: 1
58To
tal:
med
ian
3 m
o (1
mo
to 3
y)
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

I2 = 38%) with unimportant bias (Fig 3). When only data from prospective studies were analyzed, results maintained their significance (data not shown). The single study that only included individuals with DS without additional risk factors revealed no mortality in both groups.22 Additionally, the authors of 1 study found DS to be a risk factor for mortality among children with severe RSV LRTI.18
Secondary Outcomes
LOS
The authors of 9 studies evaluated LOS (although data for meta-analysis were limited to 2 studies15, 22), with more days being seen in children with DS than in controls (pooled mean difference: 4.73 days; 95% CI: 2.12–7.33; I2 = 0%) and without bias. The single study that only included individuals with DS without additional risk factors revealed similar results.22 The authors of the rest of the studies had similar findings, with a longer LOS being seen in children with DS than in controls, but not enough data were available to perform a meta-analysis.12– 14, 16, 17, 19, 20
Oxygen Requirement
The authors of 3 studies reported oxygen use during RSV infection.13, 20, 22 Children with DS were more likely to require oxygen support than controls (pooled OR: 6.53; 95% CI: 2.22–19.19; I2 = 0%) without bias (Fig 4A). When only data of prospective studies were analyzed, similar results were obtained (data not shown). When only data of prospective studies or studies that only included individuals with DS without additional risk factors were analyzed, similar results were obtained (data not shown).
ICU Admissions
The authors of 2 studies reported ICU admissions as an outcome.20, 22 Children with DS had a higher risk of
PEDIATRICS Volume 142, number 3, September 2018 5
Auth
or, y
Coun
try
Stud
y De
sign
Incl
uded
Par
ticip
ants
Outc
omes
No. P
artic
ipan
ts, n
Age
Stag
liano
et a
l, 19
2015
Unite
d St
ates
RCRS
V ho
spita
lizat
ion
data
of c
hild
ren
with
and
with
out
DS w
ithin
Tri
care
a <3
y o
f age
(DS
: 842
; CG:
632
358)
; pa
rtic
ipan
ts w
ith a
dditi
onal
ris
k fa
ctor
s w
ere
incl
uded
(23
% h
emod
ynam
ical
ly s
igni
fican
t CHD
, 28
% p
rem
atur
ity, a
nd 2
% c
hron
ic lu
ng d
isea
se)
Hosp
ital a
dmis
sion
s, n
eed
of
resp
irat
ory
supp
ort,
LOS
DS: 8
42; C
G: 6
32 35
8—
Galle
guill
os
et a
l, 20 2
016
Chile
RCRS
V ho
spita
lizat
ion
data
of c
hild
ren
<14
y of
age
w
ith a
nd w
ithou
t DS
(DS:
58;
CG:
58)
; par
ticip
ants
w
ith a
dditi
onal
ris
k fa
ctor
s w
ere
incl
uded
(15
%
hem
odyn
amic
ally
sig
nific
ant C
HD a
nd 1
0% c
hron
ic
lung
dis
ease
)
Mor
talit
y, n
eed
of r
espi
rato
ry
supp
ort,
need
of
supp
lem
enta
l oxy
gen,
ad
mis
sion
to P
ICU,
LOS
, use
of
sys
tem
ic c
ortic
oste
roid
s,
use
of a
ntib
iotic
s
DS: 5
8; C
G: 5
8DS
med
ian:
26.
4 m
o; C
G m
edia
n:
11.8
mo
Lee
et a
l, 21 2
016
Taiw
anC-
CCh
ildre
n <1
8 y
of a
ge a
dmitt
ed to
the
PICU
for
seve
re R
SV L
RTI (
DS: 9
; CG:
177
); no
des
crip
tion
of
addi
tiona
l ris
k fa
ctor
s
Mor
talit
y, n
eed
of r
espi
rato
ry
supp
ort,
LOS
in P
ICU
DS: 9
; CG:
177
Tota
l med
ian:
5.3
mo
Sánc
hez-
Luna
et
al, 22
201
7Sp
ain
PCIn
divi
dual
s w
ith D
S re
crui
ted
afte
r bi
rth
and
mat
ched
w
ith 1
con
trol
(ex
clus
ion
of in
divi
dual
s w
ith o
ther
ri
sk fa
ctor
s); R
SV h
ospi
taliz
atio
n fo
r ch
ildre
n w
ith
DS <
1 y
of a
ge a
nd a
sses
smen
t of d
isea
se s
ever
ity
(DS:
93;
CG:
68)
; ind
ivid
uals
with
chr
onic
pre
exis
ting
cond
ition
s w
ere
excl
uded
in th
is s
tudy
.
Hosp
ital a
dmis
sion
s, m
orta
lity,
ne
ed o
f res
pira
tory
sup
port
, ne
ed o
f sup
plem
enta
l oxy
gen,
ad
mis
sion
to P
ICU,
LOS
in
PICU
, LOS
DS: 9
3; C
G: 6
8DS
mea
n ±
SD:
7.4
± 5
.4 m
o; C
G m
ean
± S
D: 8
.4 ±
6.1
mo
Grut
et a
l, 23
2017
Swed
enRC
RSV
hosp
italiz
atio
n an
d bi
rth
data
for
child
ren
with
DS
, mat
ched
with
2 c
ontr
ols
each
, <2
y of
age
, 3
diffe
rent
dat
abas
es (
DS: 8
14; C
G: 1
628)
; no
desc
ript
ion
of a
dditi
onal
ris
k fa
ctor
s
Hosp
ital a
dmis
sion
s, m
orta
lity
DS: 8
14; C
G: 1
628
—
PC, p
rosp
ectiv
e co
hort
; RC,
ret
rosp
ectiv
e co
hort
; —, n
ot a
pplic
able
. a
US D
epar
tmen
t of D
efen
se’s
hea
lth c
are
prog
ram
.
TABL
E 1
Cont
inue
d
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

ICU admission than controls (pooled OR: 2.56; 95% CI: 1.17–5.59; I2 = 0%) without bias. Additionally, 1 study revealed that in children with CHD, having DS was not associated with a higher risk of ICU admission (OR: 1.42; 95% CI: 0.77–2.63).14 The single study that only included individuals with DS without additional risk factors revealed no difference between both groups.22
Need for Respiratory Support
The authors of 6 studies reported the necessity for respiratory support during RSV infection.12, 13, 17, 19, 20, 22 DS was associated with a higher risk of needing mechanical ventilation compared with what was seen in controls (pooled OR: 4.56; 95% CI: 2.17–9.58; I2 = 57%) although with moderate bias (Fig 4B). When only data of prospective studies or studies that only included individuals with DS without additional risk factors were analyzed, similar results were obtained (data not shown). When data from prospective studies were analyzed, similar results were obtained (data not shown). Additionally, the authors of 1 study reported that in children with CHD, having DS was not associated with a higher need for mechanical ventilation (OR: 1.34; 95% CI: 0.90–1.98).14
Additional Medication Use
The authors of 1 study17 reported a higher chance of prescription of bronchodilators in patients with DS with no additional risk factors than in controls (OR: 5.16; 95% CI: 1.31–20.34). The authors of 2 studies17, 20 reported a higher use of antibiotics and a higher use of systemic corticosteroids in children with DS compared with controls (pooled OR: 2.65 [95% CI: 1.38–5.08; I2 = 0%] and pooled OR: 5.82 [95% CI; 2.66–12.69; I2 = 0%], respectively). The single study that only included individuals with DS without additional risk factors revealed similar results.17
BECKHAUS and CASTRO-RODRIGUEZ6
TABL
E 2
Risk
of B
ias
of th
e In
clud
ed P
rosp
ectiv
e an
d C-
C St
udie
s
Stud
y Ty
pe, A
utho
r, y
Sele
ctio
nCo
mpa
rabi
lity
of C
ohor
ts
Base
d on
the
Desi
gn o
r An
alys
is
Outc
ome
Repr
esen
tativ
enes
s of
the
Expo
sed
Coho
rt
Sele
ctio
n of
the
None
xpos
ed
Coho
rt
Asce
rtai
nmen
t of
Expo
sure
Dem
onst
ratio
n Th
at O
utco
me
of
Inte
rest
Was
Not
Pr
esen
t at S
tart
of
Stu
dy
Asse
ssm
ent o
f Ou
tcom
eFo
llow
-up
Long
En
ough
for
Outc
omes
to
Occu
r
Adeq
uacy
of
Follo
w-u
p
Pros
pect
ive
Fj
aerl
i et a
l, 12 2
004
√√
√√
√√
√√
Bl
oem
ers
et a
l, 13 2
007
√√
√√
√√
√√
M
edra
no L
ópez
et a
l, 14 2
009
√√
√√
—√
—√
M
egge
d an
d Sc
hles
inge
r, 15 2
010
——
√√
—√
√√
Kr
iste
nsen
et a
l, 16 2
012
√√
√√
√√
√√
Za
char
iah
et a
l, 17 2
012
√√
√√
√√
√√
Zh
ang
et a
l, 18 2
013
√√
√√
√√
√√
St
aglia
no e
t al, 19
201
5√
√√
√√
√√
√
Galle
guill
os e
t al, 20
201
6√
√√
√√
√√
√
Sánc
hez-
Luna
et a
l, 22 2
017
√√
√√
√√
√√
Gr
ut e
t al, 23
201
7√
√√
√√
√√
√C-
C
Zach
aria
h et
al, 17
201
2√
√—
√√
√√
—
Lee
et a
l, 21 2
016
√√
—√
√√
√—
—, n
ot a
pplic
able
.
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 142, number 3, September 2018 7
FIGURE 2Pooled ORs and 95% CIs for the number of hospital admissions because of RSV infection between children with DS and children without DS. df, degrees of freedom; M-H, Mantel-Haenszel test.
FIGURE 3Pooled ORs and 95% CIs for mortality because of RSV infection between children with DS and children without DS. df, degrees of freedom; M-H, Mantel-Haenszel test.
FIGURE 4A, Pooled ORs and 95% CIs for oxygen requirement because of RSV infection between children with DS and children without DS. B, Pooled ORs and 95% CIs for mechanical ventilation support because of RSV infection between children with DS and children without DS. df, degrees of freedom; M-H, Mantel-Haenszel test.
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

DISCUSSION
This systematic review with a meta-analysis of 12 studies that were conducted in 10 different countries around the world revealed that children with DS are at a significantly higher risk of having severe RSV infection (higher hospital admission, mortality, LOS, oxygen requirement, ICU admission, need for ventilator support, and additional medication use) than children without DS with the absence of bias in the vast majority these outcomes.
Because DS is the most common chromosomal disorder worldwide and given that RSV is associated with ∼28% of all acute LRTI episodes and 13% to 22% of all acute LRTI mortality in young children, 24 the results of the current study carry high importance and consequences for public health. Therefore, any potential strategy to reduce RSV infection (eg, prophylaxis with monoclonal antibodies or new vaccines25) in children with DS could decrease their morbidity and mortality.
Palivizumab, a humanized monoclonal antibody, is used for prophylaxis against RSV and reduces hospitalizations in children at high risk (eg, those with chronic lung disease, hemodynamically significant CHD, neuromuscular disease, immunodeficiency, and/or prematurity) <2 years of age.26 –30 Currently, the American Academy of Pediatrics does not recommend the routine use of palivizumab to prevent RSV infection in patients with DS who do not qualify for other reasons (eg, CHD, chronic lung disease, airway clearance issues, or prematurity) because insufficient data are available to recommend palivizumab prophylaxis routinely for children with Down syndrome.31, 32
However, according to the present systematic review and the results of our meta-analysis, children with DS have a 9 times higher mortality
risk and an 8.7 times higher risk of hospitalization because of RSV than children without DS. There is also a high economic burden on families and health care systems. They have a 6.5-fold higher risk of a supplemental oxygen requirement, a 2.7-fold increased risk of ICU admission, and a 4.7-fold higher risk of need for ventilator support and on average spend 4.7 days longer in the hospital. Our analysis also revealed that even in children with DS without additional risk factors (eg, CHD or prematurity), they had significantly more risk.
A recent report revealed a decrease in hospitalization rates because of RSV in the United States (between 1997 and 2012) in non–high-risk infants as well as among those with chronic lung disease and high-risk CHD but not among those with DS without CHD.33 Indeed, this latter group had the highest hospitalization rate trend in this period.33 In 2015, the total charges for infants with DS who were hospitalized for RSV increased from $10 141 (US dollars) to $18 217 (from 1997 to 2012, respectively); in contrast, charges for non–high-risk infants increased from $6983 to $11 273.33 The authors of a recent prospective study of 532 Canadian children with DS who received palivizumab reported a 3.6-fold reduction in the incidence rate ratio of RSV-related hospitalizations during the first 2 years of life.34 A recent Japanese multicenter postmarketing surveillance study about palivizumab prophylaxis against RSV infection in 138 children with DS without hemodynamically significant CHD revealed palivizumab prophylaxis to be safe and effective for the prevention of LRTI caused by RSV. Only 2 (0.7%) children were hospitalized.35 However, it is important to note that hospitalization might be a weak proxy outcome because the threshold to admit a patient with DS might be lower. More cost-utility studies used
to determine the efficacy of RSV immunoprophylaxis in this specific high-risk patient population need to be done.
A limitation of the present systemic review is that not all of the studies had a subgroup of participants with DS with CHD and without CHD or other additional risk factors, but almost all results were similar when only studies with data of participants with DS without other risk factors were considered. However, the present review had strengths. In regard to methodology, according to the Newcastle–Ottawa scale, the risk of bias of the 12 included studies was reasonably low, the total number of participants was considerably high (n = 3662 children with DS and 1 145 509 children without DS; 1 149 171 children in total), and the outcomes selected had importance for the patients and also public health implications. It is important to remark that the vast majority of the outcomes that were analyzed had no or unimportant bias.
CONCLUSIONS
This systematic review reveals that children with DS are at a significantly higher risk of having severe RSV infections (higher hospital admission, mortality, LOS, oxygen requirement, ICU admission, need for respiratory support, and additional medication use) than children without DS.
BECKHAUS and CASTRO-RODRIGUEZ8
ABBREVIATIONS
C-C: case-controlCG: control groupCHD: congenital heart diseaseCI: confidence intervalDS: Down syndromeLOS: length of hospital stayLRTI: lower respiratory tract
infectionOR: odds ratioRSV: respiratory syncytial virus
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

REFERENCES
1. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375(9725):1545–1555
2. Bueno SM, González PA, Riedel CA, Carreño LJ, Vásquez AE, Kalergis AM. Local cytokine response upon respiratory syncytial virus infection. Immunol Lett. 2011;136(2):122–129
3. Hall CB, Weinberg GA, Iwane MK, et al. The burden of respiratory syncytial virus infection in young children. N Engl J Med. 2009;360(6):588–598
4. Pavia AT. Viral infections of the lower respiratory tract: old viruses, new viruses, and the role of diagnosis. Clin Infect Dis. 2011;52(suppl 4):S284–S289
5. Watts R, Vyas H. An overview of respiratory problems in children with Down’s syndrome. Arch Dis Child. 2013;98(10):812–817
6. de Graaf G, Buckley F, Skotko BG. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States. Am J Med Genet A. 2015;167A(4):756–767
7. Tenenbaum A, Hanna RN, Averbuch D, Wexler ID, Chavkin M, Merrick J. Hospitalization of children with Down syndrome. Front Public Health. 2014;2:22
8. Fitzgerald P, Leonard H, Pikora TJ, Bourke J, Hammond G. Hospital admissions in children with Down syndrome: experience of a population-based cohort followed from birth. PLoS One. 2013;8(8):e70401
9. Dawson AL, Cassell CH, Oster ME, et al. Hospitalizations and associated costs in a population-based study of children
with Down syndrome born in Florida. Birth Defects Res A Clin Mol Teratol. 2014;100(11):826–836
10. Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2011. Available at: www. ohri. ca/ programs/ clinical_ epidemiology/ oxford. asp. Accessed January 1, 2018
11. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560
12. Fjaerli HO, Farstad T, Bratlid D. Hospitalisations for respiratory syncytial virus bronchiolitis in Akershus, Norway, 1993-2000: a population-based retrospective study. BMC Pediatr. 2004;4(1):25
13. Bloemers BL, van Furth AM, Weijerman ME, et al. Down syndrome: a novel risk factor for respiratory syncytial virus bronchiolitis–a prospective birth-cohort study. Pediatrics. 2007;120(4). Available at: www. pediatrics. org/ cgi/ content/ full/ 120/ 4/ e1076
14. Medrano López C, García-Guereta Silva L, Lirio Casero J, García Pérez J; Grupo CIVIC, Grupo de Trabajo de Infecciones de la Sociedad Española de Cardiología Pediátrica y Cardiopatías Congénitas. Respiratory infections, Down’s syndrome and congenital heart disease: the CIVIC 21 study [in Spanish]. An Pediatr (Barc). 2009;71(1):38–46
15. Megged O, Schlesinger Y. Down syndrome and respiratory syncytial virus infection. Pediatr Infect Dis J. 2010;29(7):672–673
16. Kristensen K, Hjuler T, Ravn H, Simões EA, Stensballe LG. Chronic diseases, chromosomal abnormalities, and
congenital malformations as risk factors for respiratory syncytial virus hospitalization: a population-based cohort study. Clin Infect Dis. 2012;54(6):810–817
17. Zachariah P, Ruttenber M, Simões EA. Down syndrome and hospitalizations due to respiratory syncytial virus: a population-based study. J Pediatr. 2012;160(5):827–831.e1
18. Zhang Q, Guo Z, Langley JM, Bai Z. Respiratory syncytial virus-associated intensive care unit admission in children in Southern China. BMC Res Notes. 2013;6:447
19. Stagliano DR, Nylund CM, Eide MB, Eberly MD. Children with Down syndrome are high-risk for severe respiratory syncytial virus disease. J Pediatr. 2015;166(3):703–709.e2
20. Galleguillos C, Galleguillos B, Larios G, Menchaca G, Bont L, Castro-Rodriguez JA. Down’s syndrome is a risk factor for severe lower respiratory tract infection due to respiratory syncytial virus. Acta Paediatr. 2016;105(11):e531–e535
21. Lee YI, Peng CC, Chiu NC, Huang DT, Huang FY, Chi H. Risk factors associated with death in patients with severe respiratory syncytial virus infection. J Microbiol Immunol Infect. 2016;49(5):737–742
22. Sánchez-Luna M, Medrano C, Lirio J; RISK-21 Study Group. Down syndrome as risk factor for respiratory syncytial virus hospitalization: a prospective multicenter epidemiological study. Influenza Other Respir Viruses. 2017;11(2):157–164
23. Grut V, Söderström L, Naumburg E. National cohort study showed that infants with Down’s syndrome faced a high risk of hospitalisation for
PEDIATRICS Volume 142, number 3, September 2018 9
Accepted for publication May 29, 2018
Address correspondence to Jose A. Castro-Rodriguez, MD, PhD, Division of Pediatrics, School of Medicine, Pontificia Universidad Católica de Chile, Lira 44, 1er Piso, Casilla 114-D, Santiago, Chile. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

the respiratory syncytial virus. Acta Paediatr. 2017;106(9):1519–1524
24. Shi T, McAllister DA, O’Brien KL, et al; RSV Global Epidemiology Network. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958
25. Rezaee F, Linfield DT, Harford TJ, Piedimonte G. Ongoing developments in RSV prophylaxis: a clinician’s analysis. Curr Opin Virol. 2017;24:70–78
26. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. The IMpact-RSV Study Group. Pediatrics. 1998;102 (3, pt 1):531–537
27. Feltes TF, Cabalka AK, Meissner HC, et al; Cardiac Synagis Study Group. Palivizumab prophylaxis reduces hospitalization due to respiratory syncytial virus in young children with hemodynamically significant congenital heart disease. J Pediatr. 2003;143(4):532–540
28. Resch B, Pasnocht A, Gusenleitner W, Müller W. Rehospitalisations for respiratory disease and respiratory syncytial virus infection in preterm infants of 29-36 weeks gestational age. J Infect. 2005;50(5):397–403
29. Cabalka AK. Physiologic risk factors for respiratory viral infections and immunoprophylaxis for respiratory syncytial virus in young children with congenital heart disease. Pediatr Infect Dis J. 2004;23(suppl 1):S41–S45
30. Purcell K, Fergie J. Driscoll Children’s Hospital respiratory syncytial virus database: risk factors, treatment and hospital course in 3308 infants and young children, 1991 to 2002. Pediatr Infect Dis J. 2004;23(5):418–423
31. American Academy of Pediatrics Committee on Infectious Diseases. Respiratory syncytial virus. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012:609–618
32. American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee.
Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection [published correction appears in Pediatrics. 2014;134(6):1221]. Pediatrics. 2014;134(2):415–420
33. Doucette A, Jiang X, Fryzek J, Coalson J, McLaurin K, Ambrose CS. Trends in respiratory syncytial virus and bronchiolitis hospitalization rates in high-risk infants in a United States nationally representative database, 1997-2012. PLoS One. 2016;11(4):e0152208
34. Yi H, Lanctôt KL, Bont L, et al; CARESS investigators. Respiratory syncytial virus prophylaxis in Down syndrome: a prospective cohort study. Pediatrics. 2014;133(6):1031–1037
35. Kashiwagi T, Okada Y, Nomoto K. Palivizumab prophylaxis against respiratory syncytial virus infection in children with immunocompromised conditions or Down syndrome: a multicenter, post-marketing surveillance in Japan [published correction appears in Paediatr Drugs. 2018;20(3):291]. Paediatr Drugs. 2018;20(1):97–104
BECKHAUS and CASTRO-RODRIGUEZ10 by guest on June 30, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-0225 originally published online August 9, 2018; 2018;142;Pediatrics
Andrea A. Beckhaus and Jose A. Castro-RodriguezDown Syndrome and the Risk of Severe RSV Infection: A Meta-analysis
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/142/3/e20180225including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/142/3/e20180225#BIBLThis article cites 33 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/rsv_subRSVhttp://www.aappublications.org/cgi/collection/pulmonology_subPulmonologyhttp://www.aappublications.org/cgi/collection/disabilities_subChildren With Special Health Care Needsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 30, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-0225 originally published online August 9, 2018; 2018;142;Pediatrics
Andrea A. Beckhaus and Jose A. Castro-RodriguezDown Syndrome and the Risk of Severe RSV Infection: A Meta-analysis
http://pediatrics.aappublications.org/content/142/3/e20180225located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2018has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 30, 2020www.aappublications.org/newsDownloaded from