[Doi 10.1001%2Fjama.299.12.1446] J. M. Holroyd-leduc -- What Type of Urinary Incontinence Does This...
11
THE RATIONAL CLINICAL EXAMINATION What Type of Urinary Incontinence Does This Woman Have? Jayna M. Holroyd-Leduc, MD Cara Tannenbaum, MD, MSc Kevin E. Thorpe, MMath Sharon E. Straus, MD, MSc PATIENT SCENARIO A 70-year-old woman comes to the phy- sician’s office for follow-up of hyper- tension. Her medical history is other- wise unremarkable and her medications include a -blocker. She has 4 grown children who were all delivered vagi- nally. She says that she has been expe- riencing involuntary leakage of urine for several years and recently heard from a friend that there may be treat- ment options. Together, she and her physician decide to evaluate this issue further and schedule an office visit for the following week. To fully deter- mine what treatment options will be best for this patient, it is important to determine what type of urinary incon- tinence she has. What is the most ac- curate way to determine the type of uri- nary incontinence during an office assessment? WHY DETERMINE THE TYPE OF URINARY INCONTINENCE? Urinary incontinence, defined as involuntary leakage of urine, affects up to 55% of women. 1,2 It can be divided into several different types, including stress, urge, mixed, over- flow, and functional incontinence. The symptom of stress incontinence is involuntary leakage on effort or exertion, or on sneezing or cough- ing, 1 and it is the result of weak pel- vic floor muscles, poor intrinsic sphincter function, increased ure- thral mobility, or all of the above Author Affiliations: Divisions of Geriatrics and Gen- eral Internal Medicine, and Knowledge Translation Pro- gram, University of Calgary, Calgary, Alberta, Canada (Drs Holroyd-Leduc and Straus); Institut Universi- taire de Geriatrie de Montreal, Montreal, Quebec, Canada (Dr Tannenbaum); Knowledge Translation Pro- gram, University of Toronto/St Michael’s Hospital, Toronto, Ontario, Canada (Dr Straus and Mr Thorpe); and Department of Public Health Sciences, University of Toronto, Toronto, Ontario (Mr Thorpe). Corresponding Author: Jayna M. Holroyd-Leduc, MD, Foothills Medical Centre, 1403 29th St NW, Calgary, AB, Canada T2N 2T9 (jayna.holroyd-leduc @calgaryhealthregion.ca). The Rational Clinical Examination Section Editors: David L. Simel, MD, MHS, Durham Veterans Affairs Medical Center and Duke University Medical Center, Durham, NC; Drummond Rennie, MD, Deputy Editor. Context Urinary incontinence is a prevalent condition and treatment options can de- pend on what type of incontinence is present. Objective To systematically review the evidence about the most accurate way to determine the type of urinary incontinence during an office assessment. Data Sources A search of MEDLINE using Ovid (1966-July 2007) and EMBASE (1980- July 2007), and the bibliographies of retrieved articles to identify relevant studies. Search terms included urinary incontinence, diagnostic tests, medical history taking, physi- cal examination, cough stress test, and urodynamics. Study Selection English-language articles were identified that addressed the office diagnosis of urinary incontinence in adults, in which data was not limited to case re- ports. Cohort studies of patients undergoing history, physical examination, and/or of- fice procedures (excluding urodynamics) for diagnosing the type of urinary inconti- nence were included. Case-control studies were considered when there was insufficient data available from cohort studies. The accepted reference standard for categoriza- tion of incontinence type was diagnosis confirmed by an expert, urodynamic studies, or both. Data Extraction Two investigators independently appraised study quality and ex- tracted relevant data. Minimum inclusion criteria were completion of an appropriate reference standard in all patients and the ability to extract relevant data. Data Synthesis Forty articles were identified for inclusion. A random-effects model was used for quantitative synthesis. Minimal data was available for men. In women, simple questions modestly helped diagnose stress urinary incontinence (summary posi- tive likelihood ratio [LR], 2.2; 95% confidence interval [CI], 1.6-3.2; summary nega- tive LR, 0.39; 95% CI, 0.25-0.61) but are more helpful in diagnosing urge urinary in- continence (summary positive LR, 4.2; 95% CI, 2.3-7.6; summary negative LR, 0.48; 95% CI, 0.36-0.62). A positive bladder stress test may help diagnose stress urinary incontinence (summary LR, 3.1; 95% CI, 1.7-5.5); however, a negative test is not as useful (summary LR, 0.36; 95% CI, 0.21-0.60). A systematic assessment combining the history, physical examination, and results of bedside tests to establish a clinical di- agnosis appears to be of modest value in diagnosing stress urinary incontinence (sum- mary positive LR, 3.7; 95% CI, 2.6-5.2; summary negative LR, 0.20; 95% CI, 0.08- 0.51). The systematic assessment is less helpful in diagnosing urge urinary incontinence (summary positive LR, 2.2; 95% CI, 0.55-8.7; summary negative LR, 0.63; 95% CI, 0.34-1.17). Conclusions The most helpful component for diagnosing urge urinary inconti- nence is a history of urine loss associated with urgency. A bladder stress test may be helpful for diagnosing stress urinary incontinence. JAMA. 2008;299(12):1446-1456 www.jama.com 1446 JAMA, March 26, 2008—Vol 299, No. 12 (Reprinted) ©2008 American Medical Association. All rights reserved. Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
Upload
crhistian-toribio-dionicio -
Category
Documents
-
view
212 -
download
0
description
What Type of Urinary Incontinence Does This Woman Have
Transcript of [Doi 10.1001%2Fjama.299.12.1446] J. M. Holroyd-leduc -- What Type of Urinary Incontinence Does This...
-
THE RATIONALCLINICAL EXAMINATION
What Type of Urinary IncontinenceDoes This Woman Have?Jayna M. Holroyd-Leduc, MDCara Tannenbaum, MD, MScKevin E. Thorpe, MMathSharon E. Straus, MD, MSc
PATIENT SCENARIOA70-year-oldwoman comes to the phy-sicians office for follow-up of hyper-tension. Her medical history is other-wise unremarkable andhermedicationsinclude a -blocker. She has 4 grownchildren who were all delivered vagi-nally. She says that she has been expe-riencing involuntary leakage of urinefor several years and recently heardfrom a friend that there may be treat-ment options. Together, she and herphysician decide to evaluate this issuefurther and schedule an office visit forthe following week. To fully deter-mine what treatment options will bebest for this patient, it is important todetermine what type of urinary incon-tinence she has. What is the most ac-curate way to determine the type of uri-nary incontinence during an officeassessment?
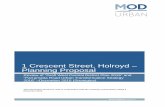
WHY DETERMINE THE TYPEOF URINARY INCONTINENCE?Urinary incontinence, defined asinvoluntary leakage of urine, affectsup to 55% of women.1,2 It can bedivided into several different types,including stress, urge, mixed, over-flow, and functional incontinence.The symptom of stress incontinenceis involuntary leakage on effort orexertion, or on sneezing or cough-ing,1 and it is the result of weak pel-vic floor muscles, poor intrinsicsphincter function, increased ure-thral mobility, or all of the above
Author Affiliations: Divisions of Geriatrics and Gen-eral InternalMedicine, andKnowledge Translation Pro-gram, University of Calgary, Calgary, Alberta, Canada(Drs Holroyd-Leduc and Straus); Institut Universi-taire de Geriatrie de Montreal, Montreal, Quebec,Canada (Dr Tannenbaum); Knowledge Translation Pro-gram, University of Toronto/St Michaels Hospital,Toronto, Ontario, Canada (Dr Straus andMr Thorpe);and Department of Publ ic Health Sciences,
University of Toronto, Toronto, Ontario (Mr Thorpe).Corresponding Author: Jayna M. Holroyd-Leduc,MD, Foothills Medical Centre, 1403 29th St NW,Calgary, AB, Canada T2N 2T9 ([email protected]).TheRationalClinical ExaminationSectionEditors:DavidL. Simel, MD,MHS, Durham Veterans Affairs MedicalCenter and Duke University Medical Center, Durham,NC; Drummond Rennie, MD, Deputy Editor.
Context Urinary incontinence is a prevalent condition and treatment options can de-pend on what type of incontinence is present.
Objective To systematically review the evidence about the most accurate way todetermine the type of urinary incontinence during an office assessment.
DataSources A search ofMEDLINE usingOvid (1966-July 2007) and EMBASE (1980-July 2007), and the bibliographies of retrieved articles to identify relevant studies. Searchterms included urinary incontinence, diagnostic tests, medical history taking, physi-cal examination, cough stress test, and urodynamics.
Study Selection English-language articles were identified that addressed the officediagnosis of urinary incontinence in adults, in which data was not limited to case re-ports. Cohort studies of patients undergoing history, physical examination, and/or of-fice procedures (excluding urodynamics) for diagnosing the type of urinary inconti-nence were included. Case-control studies were considered when there was insufficientdata available from cohort studies. The accepted reference standard for categoriza-tion of incontinence type was diagnosis confirmed by an expert, urodynamic studies,or both.
Data Extraction Two investigators independently appraised study quality and ex-tracted relevant data. Minimum inclusion criteria were completion of an appropriatereference standard in all patients and the ability to extract relevant data.
Data Synthesis Forty articles were identified for inclusion. A random-effects modelwas used for quantitative synthesis. Minimal data was available for men. In women,simple questions modestly helped diagnose stress urinary incontinence (summary posi-tive likelihood ratio [LR], 2.2; 95% confidence interval [CI], 1.6-3.2; summary nega-tive LR, 0.39; 95% CI, 0.25-0.61) but are more helpful in diagnosing urge urinary in-continence (summary positive LR, 4.2; 95% CI, 2.3-7.6; summary negative LR, 0.48;95% CI, 0.36-0.62). A positive bladder stress test may help diagnose stress urinaryincontinence (summary LR, 3.1; 95% CI, 1.7-5.5); however, a negative test is not asuseful (summary LR, 0.36; 95% CI, 0.21-0.60). A systematic assessment combiningthe history, physical examination, and results of bedside tests to establish a clinical di-agnosis appears to be of modest value in diagnosing stress urinary incontinence (sum-mary positive LR, 3.7; 95% CI, 2.6-5.2; summary negative LR, 0.20; 95% CI, 0.08-0.51). The systematic assessment is less helpful in diagnosing urge urinary incontinence(summary positive LR, 2.2; 95% CI, 0.55-8.7; summary negative LR, 0.63; 95% CI,0.34-1.17).
Conclusions The most helpful component for diagnosing urge urinary inconti-nence is a history of urine loss associated with urgency. A bladder stress test may behelpful for diagnosing stress urinary incontinence.JAMA. 2008;299(12):1446-1456 www.jama.com
1446 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
(FIGURE 1). The symptom of urgeincontinence is involuntary leakageaccompanied or immediately pro-ceeded by urgency (a sudden strongneed to void),1 and it results fromdetrusor overactivity. Mixed inconti-nence is the combination of stressand urge incontinence. Women withmixed incontinence can have bothstress and urge symptoms with thesame incontinence episode, whileothers can experience discrete epi-sodes of stress or urge incontinence.Overflow incontinence is associatedwith overdistention of the bladdercaused by obstruction (eg, pelvicorgan prolapse) or a neurologicalcondition (eg, spinal cord injury).Functional incontinence is inconti-nence resulting from cognitive, func-tional, or mobility difficulties in aperson who may or may not havelower urinary tract deficits.Most primary treatment options,
such as lifestyle modifications and be-havioral treatments, do not vary by typeof incontinence. However, it is impor-tant to determine the type of urinary in-continence because some treatment op-tions do vary according to incontinencetype. For example, there are surgicaltreatment options for stress inconti-nence andpharmacological options (eg,anticholinergic medications) for treat-ing urge incontinence.3,4
Prevalence of Urinary Incontinence
The prevalence of urinary inconti-nence varies depending on the sexand age group examined. The defini-tion of urinary incontinence used(daily vs weekly vs monthly vs anyepisodes of involuntary leakage) alsoimpacts reported prevalence rates.The overall prevalence of urinaryincontinence among older womenranges from 17% to 55%, with dailyincontinence ranging from 3% to17%.2 Among middle-aged andyounger women, the overall preva-lence ranges from 12% to 42%.2
Stress, urge, and mixed inconti-nence are the most common types ofincontinence amongwomen. Stress uri-nary incontinence is the prominent
type of incontinence among youngerwomen, with approximately one-halfto two-thirds of incontinence beingstress.2 As women age, urge urinary in-
continence becomes more prevalent.In the older age group, urge andmixedincontinence make up approximatelytwo-thirds to three-fourths of reported
Figure 1. Female Pelvis and Pelvic Floor Anatomy
Uterus
SAGITTAL VIEW
ANGLE OF VIEW
Pelvic floor
Rectum
Internalurethralsphincter
Externalurethralsphincter
Detrusormuscle
Bladder
Coccygeus
Pelvic floor muscles
Levator ani
Iliococcygeus
Pubococcygeus
Puborectalis
Obturatorinternus muscle
Colon
Colon
Rectum
Uterus
Vagina
Bladder (detrusor muscle exposed)
Urethra
Pelvic floor muscles in relation to pelvic organsA
Bladder and bladder neckB
UrethraVagina
Urethra
URINARY INCONTINENCE
2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 26, 2008Vol 299, No. 12 1447
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
incontinence. Thus, among womenwith urinary leakage, those youngerthan 65 years have a prior probabilityof isolated stress urinary incontinenceof approximately 50% to 66%,while theprevalence among older women (65years) decreases to approximately 25%to 33%, because other causes emergewith aging.
Assessment of WomenWith Incontinence
Generalist physicians may identify awomanwith incontinence through thereview of systems during a routine visitor the patient may initiate discussionabout incontinence problems. If awoman reports leaking urine, she is in-continent and the symptoms should notbe ignored. The assessment of incon-tinence should help the physician un-derstand the type of incontinence,whileidentifying potentially modifiable con-tributing factors.3
The history should include the na-ture and impact of incontinence symp-toms, gynecological and obstetrical his-tory, relevant coexisting diseases (eg,diabetes, stroke, dementia, parkinson-ism, and arthritis), current medica-tions, functional status including mo-bility and sensory impairments, reviewof environmental factors (social, cul-tural, and physical) and lifestyle fac-tors (exercise and fluid intake), previ-ous treatment history, and current goalsand expectations of treatment.5
Symptoms. Determining whetherurine is involuntarily lost with effortor exertion, or on coughing or sneez-ing, is commonly used to help iden-tify stress incontinence.1 For example,a woman can be asked, Do you loseurine during sudden physical exer-tion, lifting, coughing, or sneezing?6
To help diagnose urge incontinence,the person is asked about the associa-tion between involuntary urinaryleakage and feelings of urinaryurgency.1 An example of such a ques-tion is Do you experience such astrong and sudden urge to void thatyou leak before reaching the toilet?6
A number of questionnaires exist tohelp differentiate these conditions in a
more standardized way. Urge inconti-nence is also more likely to be associ-ated with large volume urine loss,while the volume of urine lost withepisodes of stress incontinence tendsto be small. However, the amount ofurine lost during an incontinence epi-sode of any type can depend on theamount of urine present in the blad-der at that time.Physical Examination.Aphysical ex-
amination is an important component ofthe assessment, because it may detectmodifiable factors or associated condi-tions andhelp determine the type of uri-nary incontinence. The American Col-lege of Obstetricians and Gynecologistspractice guidelines (level C evidence:consensus and expert opinion) and theInternational Consultation on Inconti-nence committee (level of evidence notgiven) both suggest that every womanpresenting with symptoms of inconti-nence undergo a general examinationduring assessment for incontinence thatincludes a gynecological, an abdomi-nal, a rectal, and a neurological exami-nation.5,7 The gynecological examina-tion includes examinationof the externalgenitalia, vagina, and perineum to as-sess for excoriations, masses, prolapse,and abnormal perineal sensation. Uri-nary incontinence and pelvic organ pro-lapse are separate clinical entities that of-ten coexist.1 Pelvic organ prolapse canobstruct voiding and women may haveto reduce their prolapse to void.Womenwith pelvic organ prolapse and largepostvoid residual urine volumes shouldbe evaluated for voidingdysfunction (eg,outlet obstruction, detrusor hypotonia).The rectal examination assesses for
fecal impaction and rectal tone. Theneurological examination focuses onthe sacral nerves and lower body. Pel-vic floor muscle strength can be deter-mined by asking the patient to con-tract their pelvic floormuscleswhile theexaminer performs a digital vaginal ex-amination. Because many women donot know how to consciously contracttheir pelvic floor muscles, they can beinstructed to contract themuscles theywould use to keep from passing gas orto stop themselves from voiding.
Special Maneuvers. Special maneu-vers that can be performed at the of-fice assessment include the stress test,the Q-tip test, and the pad test. Thestress test involves observation for urineloss with coughing or Valsalva maneu-ver. This procedure can be performedwhile the patient is in the lithotomy po-sition or standing. Instantaneous urineleakage on coughing or during a Val-salva maneuver is a positive test and isconsistent with stress incontinence.The Q-tip test involves placement of
a lubricated cotton swab in the urethrato the level of the bladder neckwhile thewomen is in the lithotomy position.8
Change in the axis of the free end of theswab is thenmeasuredwhile thewomanperforms a Valsalva maneuver. The freeend should remain horizontal if no ana-tomical defect is present. If the free endmoves above thehorizontal, urethral hy-permobility is suspected, which can oc-cur in patients with stress inconti-nence. A goniometer can be used tomeasure the exact degreeof angle changefrom the nonstraining position.9
A pad test involves the continuouswearing of continence pads for a set pe-riod of time. The pads are weighed ontheir removal and checked for abnor-mal increases (15 g) in pad weightgain.10 A pad test is usually used to helpmake a general diagnosis of urinaryincontinence.Another component of the office as-
sessment includes measurement of thepostvoid residual urine volumebyusingeither an ultrasound bladder scanner orin-and-out bladder catheterization. Aurinalysis screening for hematuria, glu-cosuria, pyuria, and bacteriuria shouldalso be performed,1 along with othertests as indicated from the history andphysical examination.A bladder diary, whichmeasures the
frequency and volume of urine outputand the circumstances around urineleakage, can be completed by the pa-tient. A bladder diary can be used dur-ing the assessment of urinary inconti-nence and it may also be used tomonitor the effectiveness of treatment(to compare changes in urinary symp-toms before and during treatment).
URINARY INCONTINENCE
1448 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
When to Consider a Referralto an Incontinence SpecialistIf after completing an initial assess-ment the type of urinary incontinenceremains unclear, a referral to an incon-tinence specialist (urologist or urogy-necologist) can be considered. Otherreasons to consider referring to an in-continence specialist include a lack ofresponse to an adequate therapeutictrial, if a patient is interested in purs-ing further investigations and/or sur-gical options, if a patient has had pre-vious anti-incontinence surgery orradical pelvic surgery, or the presenceof symptomatic pelvic organ pro-lapse.11 The finding of hematuria in theabsence of infection, a history of recur-rent symptomatic urinary tract infec-tions, and abnormal postvoid residualurine volumes are also all indicationsto consider referring a patient for fur-ther evaluation.
METHODSAsearchofMEDLINEusingOvid (1966-July 2007) and EMBASE (1980-July2007) was completed to identify rel-evant studies. The search strategy in-cluded the terms: urinary incontinence,urine incontinence, stress urinary incon-tinence, urge urinary incontinence, over-flow urinary incontinence, incontinence,urinary leakage, diagnostic tests, symp-tomatology, symptom,medical history tak-ing, physical examination, pelvic exami-nation, cough stress test,Q-tip test,postvoidresidual urine volume measurement, ul-trasonography, urodynamics, and cystos-copy.We identifiedEnglish-language ar-ticles that addressed the office diagnosisof urinary incontinence in adult hu-mans, in which data was not limited tocase reports. Additional articles wereidentified from searching bibliogra-phies of retrieved articles. Details on thesearch strategy are available on request.Cohort studies of adult patients un-
dergoing history, physical examina-tion, and/or office procedures (exclud-ingurodynamics) fordiagnosing the typeof urinary incontinence were included.Case-control studies were consideredwhen there was insufficient data avail-able from cohort studies. The accepted
reference standard for categorization ofurinary incontinence type was diagno-sis confirmed by an expert in urinary in-continence (urologist or urogynecolo-gist), urodynamic studies (cystometry,uroflowmetry, pressure-flow voidingstudies, videofluoroscopy, Valsalva leakpoint pressure measurement), or both.Two reviewers (J.M.H.-L., C.T., or
S.E.S.) independently reviewed and se-lected relevant publications thatmet theinclusion criteria from the search re-sults. Minimum inclusion criteria werethe completion of an appropriate ref-erence standard in all patients and theability to extract relevant data. Differ-ences in assessment by the reviewerswere resolved through discussion anda third investigator was available if nec-essary. There was good agreement be-tween reviewers for review of full-textarticles (=0.83; 95% confidence in-terval [CI], 0.74-0.92). The investiga-tors also assessed study quality.Data ex-traction forms were used to extractinformation on index test, referencestandard, presence of blinding, andpopulation demographics.Summary likelihood ratios (LRs) and
tests of heterogeneity were calculatedby using a random-effects model (Der-Simonian and Laird). The summary
measures were calculated on the natu-ral logarithm of the LR and then expo-nentiated to arrive at LRs. If 1 or morestudies contained zeros in their 2-by-2table, resulting in LR estimates of zeroor infinity, 0.5 was added to the countsfor all studies in that analysis. Statisti-cal analysis was conducted by using R:A Language and Environment for Sta-tisticalComputing version 2.5.0 and theMeta Contributed Package version0.8-2. R is an open-source dialect of theS language (Swas developed byAT&T)that is maintained by a core team (http://www.r-project.org). A likelihood ra-tio is the likelihood that a given test re-sult would be expected in a patientwiththe target condition comparedwith thelikelihood that the same result wouldbe expected in a patientwithout the tar-get condition.
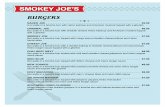
RESULTSOur search yielded 1896 citations, in-cluding 1487 citations fromMEDLINEand409 citations fromEMBASE.A totalof 164 full-text articles met initial in-clusion criteria and were retrieved forassessment. An additional 38 articleswere identified from review of the ref-erence lists of the 164 retrieved ar-ticles (FIGURE 2).
Figure 2. Study Flow Diagram
1896 References identified1487 in MEDLINE409 in EMBASE
164 Articles with potentialrelevance
40 Articles met inclusioncriteria and includedin analyses
202 Articles with potentialrelevance reviewed
1732 Excluded based on screeningof titles and abstracts
38 Articles identified fromreview of reference lists
162 Excluded based on specific criteria134 Did not meet inclusion criteria21 Only assessed test reliability7 Unable to obtain outcomes data
URINARY INCONTINENCE
2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 26, 2008Vol 299, No. 12 1449
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
We identified 40 articles for inclu-sion. Reasons for exclusion included in-ability to meet inclusion criteria (134studies), assessment of test reliabilityonly (21 studies), and inability to ob-tain outcomes data (7 studies). At-temptsweremade to contact the lead au-thors and obtain further data from thearticles thatweremissingoutcomesdata.The included studies were pub-
lished between 1980 and 2007, andranged in size from 25 to 4500 pa-tients. These studies assessed question-naires and questions, stress test, Q-tiptest, the Larsson frequency/volumechart nomogram, pad tests, and theoverall clinical assessment for diagno-sis of urinary incontinence. All the in-cluded studies enrolled only women,except for 1 study that enrolled pri-marily women (80%).
The History in DiagnosingUrinary Incontinence
Reliability. Simple questions to diag-nose stress or urge incontinence havehigh reliability (=0.8; 95% CI, 0.3-0.9).12 The percentage agreement be-tween the first and second interviewswas 90% (95%CI, 84%-95%) for all in-continence types (stress, urge, or both)among a sample of 123women aged 75years or older.
Stress Incontinence. We identified10 cohort studies that focused onwhat questions to ask when diag-nosing stress urinary incontinence(TABLE 1).6,13-21 These were questionsrelated to urinary leakage with activi-ties such as coughing, sneezing,lifting, walking, or running. Therewas significant heterogeneity amongthe studies (all P for heteroge-neity .001). Age of participantsranged from 18 to 98 years. Themajority of the studies were conductedin gynecology clinics or urodynamicunits; however, 1 study13 includednondemented nursing home residents,another study14 involved assessmentsby general practitioners, and a thirdstudy6 sampled women in the commu-nity. Despite the statistical heteroge-neity across studies, these simplequestions had clinically useful LRswith narrow CIs. The presence ofcoughing, sneezing, lifting, walking,or running as initiators of inconti-nence increased the likelihood ofstress incontinence as the cause of uri-nary leakage (summary LR, 2.2; 95%CI, 1.6-3.2), while their absencedecreased the likelihood of stressincontinence (summary LR, 0.39; 95%CI, 0.25-0.61). The LRs did notchange when 1 study that included
both stress and mixed incontinencewas excluded.13
Urge Incontinence.Ten cohort stud-ies focused on questions of urine lossassociated with urinary urgency(TABLE 2).6,13-16,19-23 The age of thewomen studied ranged from 16 to 98years. Themajority of the studies wereconducted in gynecology clinics or uro-dynamic units; however, 1 study13 in-cluded nondemented nursing homeresidents, another study14 involved as-sessments by general practitioners, andtwo other studies6,22 sampled womenfrom the community. The type of ques-tion to elicit the symptoms of urge in-continence varied slightly across thestudies. The results had slight statisti-cal heterogeneity (all P .08), but theCIs were narrow enough to infer theclinical use of the findings. An endorse-ment of an urge incontinence ques-tion, such as Do you experience sucha strong and sudden urge to void thatyou leak before reaching the toilet?,6
demonstrated that positive answers in-creased the likelihood of urge inconti-nence (summary LR, 4.2; 95% CI, 2.3-7.6). Similar to stress incontinence, theabsence of urgency symptoms de-creased the likelihood of urge inconti-nence (summary LR, 0.48; 95% CI,0.36-0.62). Excluding the 2 stud-
Table 1. Studies Assessing the Role of the History in Diagnosing Stress Incontinence
Source Study DesignSampleSize Question(s)
Likelihood Ratio(95% Confidence Interval)
Positive Negative
Kirschner-Hermanns etal,13 1998
Prospective cohort 130 Asked total of 5 incontinence questions: leaks onlywith stress, no warning
6.0 (0.11-308.9) 0.98 (0.49-1.95)
Sandvik et al,61995
Prospective cohort 236 Do you lose urine during sudden physical exertion,lifting, coughing or sneezing?
5.6 (2.9-10.5) 0.38 (0.25-0.60)
Lagro-Janssen etal,14 1991
Prospective cohort 103 Do you lose urine by spurts during coughing,sneezing, jumping or lifting?
4.8 (2.0-11.7) 0.26 (0.12-0.55)
Cundiff et al,151997
Retrospective 535 Occurrence of incontinence coincident withcoughing, sneezing, lifting, and walking
3.4 (2.1-5.4) 0.64 (0.49-0.84)
Bent et al,16 1983 Retrospective 81 Patients rate symptom of stress incontinence 2.6 (1.2-5.7) 0.08 (0.01-0.58)
Le Coutour et al,171990
Prospective cohort 154 Do you lose urinewhen coughing or runningwhen walking or with minimal effort?
1.5 (0.75-3.1) 0.20 (0.07-0.53)
Weidner et al,182001
Retrospective 950 Any stress symptoms on history 1.5 (1.2-1.8) 0.21 (0.14-0.30)
Fantl et al,19 1990 Prospective cohort 145 Symptoms of stress incontinence on history 1.5 (0.79-2.8) 0.36 (0.16-0.81)
Glezerman et al,201986
Cohort (not clear ifprospective)
105 Loss of urine during coughing, sneezing, or both 1.3 (0.41-4.3) 0.18 (0.03-1.09)
Sand et al,21 1988 Prospective cohort 218 History of urine loss associated with stress(cough, Valsalva, running, sneezing)
1.3 (0.65-2.5) 0.94 (0.63-1.41)
URINARY INCONTINENCE
1450 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
ies13,14 that included both urge andmixed incontinence did not changethese findings.A study of 4500 women examined
the relationship between overactivebladder symptoms (urinary fre-quency, urgency with or without urgeincontinence) and an urodynamic di-agnosis of detrusor overactivity (de-fined as detrusor contractions ob-served in the presence of urgency orurinary leakage during urodynamicstudies).24 Urge incontinence is con-sidered an overactive bladder symp-tom, but women can have overactivebladder symptoms without being in-continent in that they can have uri-nary frequency, urinary urgency, or bothbut always reach the toilet on time. Thepresence of overactive bladder symp-toms increases the likelihood of accu-rately diagnosing detrusor overactiv-ity (LR, 2.1; 95%CI, 1.8-2.3), althoughthe absence of symptomshas little effecton the likelihood of diagnosing detru-sor overactivity during urodynamics(LR, 0.83; 95% CI, 0.81-0.86).24
Questionnaires. There are a num-ber of questionnaires that have been de-veloped to help diagnosis the type ofurinary incontinence, and these ques-tionnaires vary in their diagnostic use-fulness (TABLE 3).25-37 Although theModified Gaudenz-Incontinence ques-tionnaire appears to increase the like-
lihood of accurately diagnosing bothstress and urge incontinence, this ques-tionnairewas designed for and has onlybeen studied among Japanese wom-en.25 The Bladder Instability Discrimi-nation Index has acceptable LRs for di-agnosing urge incontinence; however,it involves a complex calculation thatis not practical in the clinical setting.26
Similarly, the 20-item questionnaire de-veloped by Versi et al36 has acceptableLRs for diagnosing stress inconti-nence but requires computed statisti-cal analysis to determine a score.The patient-completed Question-
naire for Urinary Incontinence Diag-nosis contains 6 questions, of which 3are intended to predict stress inconti-nence and 3 are intended to predict urgeincontinence. The internal consis-tency (Cronbach ) of the items per-taining to stress and pertaining to urgeincontinence was 0.85 and 0.87, re-spectively. The test-retest reliability wasgood when measured in 79 women(67.5%) who responded to the firstmailed questionnaire (median test-retest interval, 7 days;weighted range,0.66-0.93).27 This patient-completedquestionnaire appears to increase thelikelihood of correctly diagnosing urgeincontinence (positive LR, 3.7; 95%CI,1.6-9.0; negative LR, 0.27; 95% CI,0.17-0.42), but is not as helpful in thediagnosis of stress incontinence (posi-
tive LR, 2.8; 95% CI, 1.6-4.9; negativeLR, 0.21; 95% CI, 0.12-0.37).
Accuracy of the PhysicalExamination in DiagnosingUrinary Incontinence
Performing a physical examination isarguably important for ruling out sig-nificant pathology, such as obstruc-tion, significant prolapse, and malig-nancy. We were unable to find anystudies that addressed the physical ex-amination for diagnosing the type ofurinary incontinence that met our in-clusion criteria, but there is some evi-dence supporting use of special testssuch as the stress test.Stress Test. The stress test, per-
formed while the woman is supine orstanding, involves observation for urineloss immediately on coughing or witha Valsalva maneuver. The test can beperformed before the bladder is emp-tied, after emptying the bladder, or af-ter filling of the bladder with salinethrough a catheter. Five cohort stud-ies of the stress test were identified(TABLE 4).38-42 All 5 studies were con-ducted in specialized clinics, with theage of the women ranging from 23 to92 years. Three studies (a total of 582women) involved empty-bladder su-pine stress tests.40-42 One study (41women)38 conducted the supine stresstest after the bladderwas filledwith 200
Table 2. Studies Assessing the Role of the History in Diagnosing Urge Incontinence
Source Study DesignSampleSize Question(s)
Likelihood Ratio(95% Confidence Interval)
Positive Negative
Sand et al,21 1988 Prospective cohort 218 History of urine loss associated with urgency 20.9 (5.4-80.3) 0.68 (0.37-1.24)
Sandvik et al,6 1995 Prospective cohort 236 Do you experience such a strong and sudden urgeto void that you leak before reaching the toilet?
13.7 (5.7-32.7) 0.46 (0.25-0.83)
Lagro-Janssenet al,14 1991
Prospective cohort 103 Do you have such a strong desire to voidthat you leak before reaching the toilet?
13.0 (3.7-45.4) 0.41 (0.16-1.03)
Cundiff et al,15 1997 Retrospective 535 Occurring with symptoms of urgency 10.5 (5.7-19.2) 0.61 (0.43-0.87)
Glezerman et al,201986
Cohort (not clear ifprospective)
105 Lost urine volume is large 3.7 (0.97-14.3) 0.51 (0.13-2.02)
Brown et al,22 2006 Prospective cohort 301 3 questions in series: leak urine most oftenwith the urge to empty the bladder
3.3 (2.1-5.2) 0.32 (0.21-0.49)
Kirschner-Hermannset al,13 1998
Prospective cohort 130 Asked total of 5 incontinence questions:no leak with stress, less than 5-min warning
2.2 (0.80-6.2) 0.80 (0.45-1.43)
Cantor and Bates,231980
Cohort (not clear ifprospective)
214 Involuntary loss of urine associated with urgency 1.6 (1.1-2.5) 0.21 (0.10-0.43)
Bent et al,16 1983 Retrospective 81 Patients rate symptoms of urge incontinence 1.6 (0.73-3.7) 0.34 (0.09-1.24)
Fantl et al,19 1990 Prospective cohort 145 Symptoms of urge incontinence on history 1.3 (0.75-2.4) 0.57 (0.26-1.24)
URINARY INCONTINENCE
2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 26, 2008Vol 299, No. 12 1451
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
mL normal saline. The final study (37women)39 looked at nonempty blad-der supine and standing stress tests inwhich the stress test was conducted ini-tiallywithout emptying the bladder andrepeated with controlled bladder fill-ing only if the initial test was negative.These studies combined suggest that apositive stress test makes stress incon-tinence much more likely (summaryLR, 3.1; 95% CI, 1.7-5.5; P for hetero-geneity=.12), while a negative test re-sult decreases the likelihood (sum-mary LR, 0.36; 95%CI, 0.21-0.60; P forheterogeneity=.13).A positive filledbladder supine
stress test result (LR, 9.4; 95% CI, 1.1-
77.7)38 may be more accurate than apositive emptybladder supine stresstest result (LR, 2.8; 95% CI, 1.3-1.5; Pfor heterogeneity= .06)40-42 for con-firming a diagnosis of stress inconti-nence. A negative filled-bladdersupine stress test is helpful for findingwomen less likely to have stressincontinence (LR, 0.07; 95% CI, 0.01-0.39),38 whereas a negative empty-bladder supine stress test is less accu-rate (LR, 0.48; 95% CI, 0.34-0.68; Pfor heterogeneity= .56).40-42 Doing amore complicated stress test that usesa step-wise approach to bladder fillingand combines supine and standingtesting does not further improve diag-
nostic accuracy for stress inconti-nence (positive LR, 3.4; 95% CI, 0.97-12.1; negative LR, 0.19; 95% CI,0.05-0.79).39
The stress test performed withcoughing appears to be a reliable test.A cohort study of 50 incontinentwomen found this to be a highly pre-cise test for both positive and nega-tive test results.43 Test-retest analysisdemonstrated that in 32 of 35women (91%), the test was positiveboth times and in 13 of 15 women(87%), it was negative both times(=0.77). We did not identify anytests of reliability when the stress testinvolved a Valsalva maneuver.
Table 3. Questionnaires Used to Diagnose Urge and Stress Incontinence
Source Questionnaire DescriptionSampleSize
Likelihood Ratio (95% Confidence Interval)
Urge Stress
Positive Negative Positive Negative
Ishiko et al,252000
ModifiedGaudenz-IncontinenceQuestionnaire
15 Questions divided intostress and urge scores forJapanese women
198 24 (11-54) 0.14 (0.06-0.36) 10.1 (4.7-21.9) 0.18 (0.12-0.27)
Contreras Ortizet al,261993
Bladder InstabilityDiscrimination Index
Mathematical model fordiagnosing bladderinstability
271 5.1 (3.6-7.2) 0.14 (0.05-0.41) NR NR
Bradley et al,272005
Questionnaire for UrinaryIncontinence Diagnosis
Score of6 is cutoff for urge;4 is cutoff for stress
117 3.7 (1.6-9.0) 0.27 (0.17-0.42) 2.8 (1.6-4.9) 0.21 (0.12-0.37)
Kujansuu andKauppila,281982
Urgency Score 10 Questions summarizedinto an urgency score
121 2.8 (1.8-4.2) 0.36 (0.22-0.59) NR NR
Basra et al,292007
The Bladder ControlSelf-AssessmentQuestionnaire
Designed for self-assessmentof overactive bladdersymptoms
293 2.3a 0.24a NR NR
Diokno et al,301990
Self-report of continencestatus
Based on answers tostandardized setof questions
166(urge)161
(stress)
1.9 (1.2-3.1) 0.51 (0.23-1.14) 3.2 (2.0-5.2) 0.40 (0.29-0.55)
FitzGerald andBrubaker,312002
Lemack andZimmern,321999
Urogenital DistressInventoryShort Form
Designed to evaluatesymptom distress
293
128
1.6 (1.1-2.4) 0.57 (0.25-1.31) 3.4 (2.1-5.6) 0.51 (0.43-0.61)
van Brummenet al,332004
Dutch version of theUrogenital DistressInventory and theIncontinence ImpactQuestionnaire
Designed to evaluatesymptom distressand life impactof incontinence
95 1.4 (1.2-1.7) 0.18 (0.03-1.25) NR NR
Haeusler etal,34 1995
Gaudenz-IncontinenceQuestionnaire
26 Questions related to stressand urge
1911 1.4a 0.68a 1.0a 0.99a
Khan et al,352004
Bristol Female LowerUrinary Tract SymptomQuestionnaire
Designed to assess urinarysymptoms
69 NR NR 5.7a 0.86a
Versi et al,361991
Computer-based score Calculated from answersto 20 questions
252 NR NR 5.0 (3.3-7.5) 0.26 (0.19-0.37)
Klovning et al,371996
Detrusor Instability Score Scored questionnaire(cut point = 5)
250 NR NR 2.6a 0.52a
Abbreviation: NR, not reported.aUnable to calculate 95% confidence interval from data available.
URINARY INCONTINENCE
1452 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
Q-Tip Test.Two relevant studiesmetthe inclusioncriteria.44,45One study45wasa retrospective study that used a cutoffangle of 20 and involved 138 women(90with stress incontinenceand48with-out stress incontinence) primarily agedin their 50s attending an urogynecol-ogyclinic.The secondstudy44was a case-control studywith 79 cases and 36 con-trols and a cutoff angle of 35 fromhorizontalwith straining. Thesewomenranged in age from 32 to 74 years andwere recruited fromanurodynamic unit(cases) or gynecology clinic (controls).Based on these 2 studies, a positive
Q-tip test does not contribute to the di-agnosis of stress urinary incontinencewith an LR of 1.38 (95% CI, 0.91-2.09), although a normal test result de-creases the likelihood of stress incon-tinence (LR, 0.41; 95% CI, 0.22-0.76).There was no significant heteroge-neity between the studies (all P .29),but the reproducibility of the Q-tip testhas not been reported. It is not clear ifa goniometer was used to measure theangle change in these studies. Cur-rently, urinary incontinence experts pri-marily use the Q-tip test as part of theevaluation for incontinence surgery orin the setting of research studies.1
Pad Test. Only 1 study10 in whichurodynamics test results were com-pared with home pad test results metour inclusion criteria. The compari-son included 62 patients with an uro-dynamic diagnosis of stress inconti-nence and 43 with no urodynamicabnormality. A positive pad test in-creases the likelihood of an inconti-nence problem (LR, 3.3; 95% CI, 2.0-5.4). A negative pad test makes anincontinence problemmuch less likely(LR, 0.11; 95% CI, 0.05-0.27). Given
that patients with other types of incon-tinence were not included in this study,it can be concluded that the pad testconfirms an incontinence problem, butits role in distinguishing the type of in-continence cannot be commented on.Larsson Frequency/Volume Chart
Nomogram. Larsson et al46 comparedthe readings of a 48-hour urine fre-quency/volume chart to the urody-namic diagnoses of urge or stress in-continence. Study participants recordedthe number of times they urinated over48 hours, and recorded the volume ofeachmicturition. These data were usedto develop the Larsson chart.A subsequent retrospective study of
216patients found that theoptimumcut-off point for diagnosing urge inconti-nence was at a probability of 0.6 on theLarsson chart (sensitivity, 52%; specific-ity, 70%;positiveLR,1.7).47Acutoffpointof 0.3 probabilitywas optimum for iden-tifyingwomen less likely tohaveurge in-continence (sensitivity, 66%; specificity,65%; negative LR, 0.53), indicating thatthe chart is not an accurate method fordiagnosing urge incontinence.Postvoid Residual Urine Volume.
Postvoid residual urine volumes aremeasured, either with a bladder scan-
ner or through in-and-out catheteriza-tion, to help diagnose urinary reten-tion. A postvoid residual urine volumeof more than 100 mL is considered in-adequate bladder emptying. No stud-ies of postvoid urine volume measure-ment as a test for determining urinaryincontinence typemet the inclusion cri-teria. However, this is a test com-monly used in clinical practice whenoverflow urinary incontinence is sus-pected. It is also an important test forolder women with urge incontinencebecause of their increased risk of hav-ing detrusor hyperactivity with im-paired contractility.48 These women areat increased risk of developing uri-nary retention and overflow inconti-nence when treated with anticholiner-gic medications.
Accuracy of the OverallClinical Assessment
Four studies assessed the accuracy ofthe clinical diagnosis of stress urinaryincontinence, established using a sys-tematic approach to the assessmentand confirmed with reference stan-dards that included urodynamic stud-ies (TABLE 5).49-52 The first study49
involved 863 consecutive women
Table 4. Stress Test for Diagnosing Stress Incontinence
SourceTrue-Positive
RateFalse-Positive
Rate
PositiveLikelihood Ratio(95% Confidence
Interval)StudyWeighta
Hsu et al,38 1999 29/31 1/10 9.4 (1.1-77.7) 7
Kadar,39 1988 18/21 4/16 3.4 (0.97-12.1) 15
Lobel and Sand,40 1996 121/249 3/55 8.9 (2.7-29.1) 16
McLennan and Bent,41 1998 34/43 51/136 2.1 (1.2-3.7) 34
Walter et al,42 2004 20/28 28/71 1.8 (0.88-3.7) 28
Summary 3.1 (1.7-5.5)aStudy weight as a percentage of the total, representing the proportional contribution of each study to the summary.
Table 5. Overall Clinical Assessment for Diagnosing Stress Incontinence
SourceTrue-Positive
RateTrue-Negative
RatePositive Likelihood Ratio(95% Confidence Interval)
StudyWeighta
Negative Likelihood Ratio(95% Confidence Interval)
StudyWeighta
Carey et al,49 1997 308/569 263/294 5.1 (3.5-7.6) 31 0.51 (0.41-0.64) 24
De Muylder et al,50 1992 228/242 108/166 2.7 (1.9-3.8) 34 0.09 (0.05-0.16) 22
Wall et al,51 1994 37/42 27/35 3.9 (1.6-9.4) 12 0.15 (0.05-0.44) 18
Diokno et al,52 1999 47/52 40/49 4.9 (2.2-11.1) 14 0.12 (0.04-0.32) 19
Diokno et al,52 1999 14/18 18/27 2.3 (0.83-6.5) 10 0.33 (0.10-1.15) 17
Summary 3.7 (2.6-5.2) 0.20 (0.08-0.51)aStudy weight as a percentage of the total, representing the proportional contribution of each study to the summary likelihood ratio.
URINARY INCONTINENCE
2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 26, 2008Vol 299, No. 12 1453
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
referred to an urogynecology clinicwhere they underwent a detailed his-tory using a standardized question-naire, physical examination, and stresstest. The second study50 enrolled 408women aged 18 to 78 years, who pre-sented with urinary incontinence to agynecologist or urologist during a29-month period. These womenunderwent a standardized history,physical examination, and postvoidresidual urine measurement; the officediagnosis was based on the presentingsymptom complexes. The thirdstudy51 involved a retrospective chartreview of 77 women who had pre-sented to an urogynecology cliniccomplaining of urinary incontinence.The clinic evaluation included historytaking, physical examination, postvoidresidual urine measurement followingvoiding into a urine flow meter, stresstest during and after filling of the blad-der to capacity using a catheter, andevaluation for leakage associated witha strong sense of urgency, while listen-ing to running water or splashinghands in a basin of warm water, whenthe bladder was filled to capacity. Theclinic diagnosis was based primarilyon the results of these later 2 tests.The fourth study52 involved the sepa-rate assessment of 2 different groupsof women (101 and 45) at a conti-nence clinic, using the same assess-ment methods. The assessmentincluded medical history; completionof a modified version of the validatedMedical, Epidemiologic, and SocialAspects of Aging (MESA) UrinaryIncontinence questionnaire; andfocused physical examination, includ-ing pelvic examination, stress test, andpostvoid residual urine measurement.There appears to be value in doing a
systematic evaluation to help diag-nose stress incontinence (positive LR,3.7; 95% CI, 2.6-5.2; P for heteroge-neity=.14; negative LR, 0.20; 95% CI,0.08-0.51; P for heterogeneity .001)(Table 5).49-52 In the 2 studies that evalu-ated urge incontinence,50,51 a compre-hensive clinical assessment is less help-ful in confirming a diagnosis (positiveLR, 2.2; 95%CI, 0.55-8.7; P for hetero-
geneity=.01; negative LR, 0.63; 95%CI,0.34-1.17; P for heterogeneity=.13).Another cohort study,53 involving 50
women aged 65 years or older, exam-ined the role of simplified diagnostictests (history, physical examination,postvoid residual measurement, stresstest, and other simple bladder fillingtests using a catheter) conducted by anurse practitioner in conjunction witha clinical algorithm.The objective of thealgorithmand simplified testswas to di-agnose reversible causes of inconti-nence, to identify patients who shouldbe referred to a specialist for furtherevaluation, and to appropriately pre-scribe medical therapy without theneed for urodynamic testing. Based onthese data, a standardized approachused by a nurse practitioner providesresults that may help confirm (posi-tive LR, 4.6; 95% CI, 1.7-12.6) or ex-clude (negative LR, 0.11; 95%CI, 0.04-0.33) a diagnosis of urge incontinenceamong older women.
Limitations
Given the controversy around the roleof urodynamics in diagnosing urinaryincontinence, we chose to include stud-ies that used urodynamic studies, ex-pert opinion, or both as the referencestandard for diagnosis. This definitionof the reference standard best reflectscurrent clinical practice, in which a de-finitive diagnosis is determined by anexpert with or without the aid of uro-dynamic findings. Using the clinical ex-amination, with or without additionaltests, to make a definitive diagnosis isnot unique to urinary incontinence, butalso occurs in the diagnosis of arthri-tis, dementia, and Parkinson disease.However, including expert opinion asthe reference standardmight raise con-cern of incorporation bias.Of the40 includedstudies, 6 included
expert opinion within the referencestandard.6,22,27,29,37,50 Two of these stud-ies6,22 compared the diagnostic accu-racy of questions asked by a nursewitha comprehensive assessment by anexpert (gynecologist, urogynecolo-gist, orurologist) blinded to theanswersof the questions. In the 1 study,6 the
experts assessment included urody-namics. Excluding these 2 studies fromthe meta-analysis did not change theconclusions regarding the role of ques-tions in diagnosing urge incontinence(new summary positive LR, 3.8; 95%CI, 1.8-7.8; new summary negative LR,0.52;95%CI,0.39-0.71)or stress incon-tinence (newsummarypositiveLR, 2.0;95% CI, 1.4-2.7; new summary nega-tiveLR, 0.38; 95%CI, 0.23-0.64).Threeother studies compared results of stan-dardized questionnaires (2 question-naires were completed by patients27,29
and 1 questionnaire was completed bya specialized nurse37) with an assess-ment by an expert (including urody-namics in 2 studies27,37) blinded to thequestionnaire results. TheLRs for thesequestionnaires were comparable withother questionnaires examined. Thesixth study50 involved the overall clini-cal assessment in diagnosing stressincontinence. This study compared theoverall clinical assessment to the over-all clinical assessmentwith urodynam-ics, where the expert making the diag-nosis based on just the overall clinicalassessment did not have access to theurodynamic results. Excluding thisstudy from the meta-analysis did notimpact the value of the overall clinicalassessment in diagnosing stress incon-tinence (newsummarypositiveLR, 3.7;95% CI, 2.3-6.0; new summary nega-tive LR, 0.20; 95% CI, 0.05-0.73).Therefore, we do not feel that includ-ing these 6 studies within this reviewresulted in biased conclusions.The data for the overall clinical ex-
amination were all from studies of pa-tients evaluated by specialists, suggest-ing possible uncertainty as to whetherthe resultswould generalize to an evalu-ation performed by a primary care phy-sician. Although each specialist physi-cian might have performed a slightlydifferent examination, the overall clini-cal assessment is understandable in thatit involves a focused history, physicalexamination, and simple specializedtests. A study with a nurse practi-tioner doing a similar clinical assess-ment had results comparable with thatof the specialists. Therefore, it is rea-
URINARY INCONTINENCE
1454 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
sonable to assume that the results couldbe replicated in a generalists office.
SCENARIO RESOLUTIONOn review of symptoms, the patient re-ports urine loss in association with ur-gency and on 1 occasion she lost urinewhen coughing. Her physical exami-nation is unremarkable. A filled-bladder stress test is negative for urineleakage. Her postvoid residual urinevolume is 30 mL, which is within thenormal range of 100mLor less. Her uri-nalysis has no abnormal findings.Her pretest probability for urge in-
continence is approximately 67% (pre-test odds=0.67/[1-0.67]=2.0),while herpretest probability for isolated stress in-continence is approximately 25% (pre-test odds=0.25/[1-0.25]=0.3). Her his-tory supports a diagnosis of urgeincontinence (positive LR, 4.2), givinga posttest probability of 89% (posttestodds=2.04.2=8.4).Hernegative filled-bladder stress test decreases her prob-ability of stress incontinence (negativeLR, 0.07), with a posttest probability of2% (posttest odds=0.30.07=0.02).Basedon the assessment, shehasurge in-continence. All the appropriate treat-ment options cannowbediscussedwiththis patient.
THE BOTTOM LINEWhen evaluating a woman with uri-nary incontinence, a systematic ap-proach that includes a history, physi-cal examination, and stress testincreases the likelihood of correctlyclassifying the type of incontinence (forstress: positive LR, 3.7; negative LR,0.20; and for urge: positive LR, 2.2;negative LR, 0.63). The most helpfulcomponent of the assessment for de-termining the presence of urge incon-tinence is a history of urine loss asso-ciated with urinary urgency (positiveLR, 4.2).A stress test (preferably a filled-
bladder stress test) may be helpful fordiagnosing stress incontinence (filled-bladder stress test: positive LR, 9.4;negative LR, 0.07). For primary carephysicians unable to perform stress testsin their office, it would be reasonable
to refer patients for further evaluationwhen a diagnosis is needed with morecertainty.Measurement of the postvoidresidual urine volume detects incom-plete bladder emptying, but no datasupport using this in women for sepa-rating out incontinence type.Author Contributions:Dr Holroyd-Leduc had full ac-cess to all of the data in the study and takes respon-sibility for the integrity of the data and the accuracyof the data analysis.Studyconceptanddesign:Holroyd-Leduc,Tannenbaum,Straus.Acquisition of data: Holroyd-Leduc, Straus.Analysis and interpretation of data: Holroyd-Leduc,Tannenbaum, Thorpe, Straus.Drafting of the manuscript: Holroyd-Leduc, Straus.Critical revision of the manuscript for important in-tellectual content: Tannenbaum, Thorpe, Straus.Statistical analysis: Thorpe, Straus.Administrative, technical, or material support:Holroyd-Leduc, Straus.Study supervision: Tannenbaum, Straus.Financial Disclosures: Dr Tannenbaum reports hav-ing consulted for Astellas, Oryx, and Triton Pharma-ceuticals. No other authors reported any financial dis-closures.Additional Contributions:CathleenColon-Emeric,MD,and Joanne T. Piscitelli,MD (DukeUniversity, Durham,North Carolina), provided advice on earlier versionsof the article. Drs Colon-Emeric and Piscitelli did notreceive any compensation for their contribution.
REFERENCES
1. Staskin D, Hilton P, Emmanuel A, et al. Chapter 9:initial assessment of incontinence. In: Abrams P, Cor-dozo L, Khoury S, Wein A, eds. Incontinence. Vol 1.Plymouth, MA: Health Publication Ltd; 2005.2. Thom D. Variation in estimates of urinary incon-tinence prevalence in the community: effects of dif-ferences in definition, population characteristics,and study type. J Am Geriatr Soc. 1998;46(4):473-480.3. Holroyd-Leduc JM, Straus SE.Management of uri-nary incontinence in women: clinical applications.JAMA. 2004;291(8):996-999.4. Holroyd-Leduc JM, Straus SE.Management of uri-nary incontinence in women: scientific review. JAMA.2004;291(8):986-995.5. Abrams P, Andersson KE, Brubaker L, et al. Rec-ommendations of the International Scientific Com-mittee: evaluation and treatment of urinary inconti-nence, pelvic organ prolapse and faecal incontinence.In: Abrams P, Cardozo L, Khoury S, Wein A, eds. In-continence. Vol 2. Plymouth, MA: Health Publica-tion Ltd; 2005.6. Sandvik H, Hunskaar S, Vanvik A, Bratt H, SeimA, Hermstad R. Diagnostic classification of female uri-nary incontinence: an epidemiological survey cor-rected for validity. J Clin Epidemiol. 1995;48(3):339-343.7. AmericanCollegeofObstetricians andGynecologists.Urinary incontinence inwomen.ObstetGynecol. 2005;105(6):1533-1545.8. Crystle CD, Charme LS, Copeland WE. Q-tip testin stress urinary incontinence.Obstet Gynecol. 1971;38(2):313-315.9. Walsh LP, Zimmern PE, Pope N, Shariat SF. Com-parison of the Q-tip test and voiding cystourethro-gram to assess urethral hypermobility among womenenrolled in a randomized clinical trial of surgery forstress urinary incontinence. J Urol. 2006;176(2):646-649.10. Versi E, Orrego G, Hardy E, Seddon G, Smith P,
Anand D. Evaluation of the home pad test in the in-vestigation of female urinary incontinence. Br J Ob-stet Gynaecol. 1996;103(2):162-167.11. Fantl JA, Newman DK, Colling J. Urinary Incon-tinence in Adults: Acute and Chronic Management.Rockville, MD: Agency for Healthcare Research andQuality; 1996. AHCPR Publication 96-0682.12. Rohr G, Christensen K, Ulstrup K, Kragstrup J. Re-producibility and validity of simple questions to iden-tify urinary incontinence in elderly women. Acta Ob-stet Gynecol Scand. 2004;83(10):969-972.13. Kirschner-Hermanns R, Scherr PA, Branch LG,Wetle T, Resnick NM. Accuracy of survey questionsfor geriatric urinary incontinence. J Urol. 1998;159(6):1903-1908.14. Lagro-Janssen AL, Debruyne FM, van Weel C.Value of the patients case history in diagnosing uri-nary incontinence in general practice. Br J Urol. 1991;67(6):569-572.15. Cundiff GW, Harris RL, Coates KW, Bump RC.Clinical predictors of urinary incontinence in women.Am J Obstet Gynecol. 1997;177(2):262-266.16. Bent AE, Richardson DA, Ostergard DR. Diagno-sis of lower urinary tract disorders in postmenopausalpatients. Am J Obstet Gynecol. 1983;145(2):218-222.17. Le Coutour X, Jung-Faerber S, Klein P, RenaudR. Female urinary incontinence: comparative value ofhistory and urodynamic investigations. Eur J ObstetGynecol Reprod Biol. 1990;37(3):279-286.18. Weidner AC, Myers ER, Visco AG, Cundiff GW,Bump RC.Which women with stress incontinence re-quire urodynamic evaluation? Am J Obstet Gynecol.2001;184(2):20-27.19. Fantl JA, Wyman JF, McClish DK, Bump RC. Uri-nary incontinence in community-dwellingwomen: clini-cal, urodynamic, and severity characteristics.Am JOb-stet Gynecol. 1990;162(4):946-951.20. Glezerman M, Glasner M, Rikover M, Tauber E,Bar-Ziv J, Insler V. Evaluation of reliability of historyin women complaining of urinary stress incontinence.Eur J Obstet Gynecol Reprod Biol. 1986;21(3):159-164.21. Sand PK, Hill RC, Ostergard DR. Incontinence his-tory as a predictor of detrusor stability.Obstet Gynecol.1988;71(2):257-260.22. Brown JS, Bradley CS, Subak LL, et al. The sen-sitivity and specificity of a simple test to distinguishbetween urge and stress urinary incontinence.Ann In-tern Med. 2006;144(10):715-723.23. Cantor TJ, Bates CP. A comparative study of symp-toms and objective urodynamic findings in 214 in-continent women. Br J Obstet Gynaecol. 1980;87(10):889-892.24. DigesuGA,Khullar V, Cardozo L, Salvatore S.Over-active bladder symptoms: do we need urodynamics?Neurourol Urodyn. 2003;22(2):105-108.25. Ishiko O, Hirai K, Sumi T, Nishimura S, Ogita S.The urinary incontinence score in the diagnosis of fe-male urinary incontinence. Int JGynaecolObstet. 2000;68(2):131-137.26. Contreras Ortiz O, Lombardo RJ, Pellicari A. Non-invasive diagnosis of bladder instability using the Blad-der Instability Discriminant Index (BIDI). ZentralblGynakol. 1993;115(10):446-449.27. Bradley CS, Rovner ES, MorganMA, et al. A newquestionnaire for urinary incontinence diagnosis inwomen: development and testing. Am J ObstetGynecol. 2005;192(1):66-73.28. Kujansuu E, Kauppila A. Scored urological his-tory and urethrocystometry in the differential diag-nosis of female urinary incontinence. Ann ChirGynaecol. 1982;71(4):197-202.29. Basra R, Artibani W, Cardozo L, et al. Design andvalidation of a new screening instrument for lower uri-nary tract dysfunction: the Bladder Control Self-Assessment Questionnaire (B-SAQ). Eur Urol. 2007;52(1):230-237.
URINARY INCONTINENCE
2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 26, 2008Vol 299, No. 12 1455
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015
-
30. Diokno AC, Normolle DP, BrownMB, Herzog AR.Urodynamic tests for female geriatric urinaryincontinence. Urology. 1990;36(5):431-439.31. FitzGerald MP, Brubaker L. Urinary incontinencesymptom scores and urodynamic diagnoses. Neuro-urol Urodyn. 2002;21(1):30-35.32. Lemack GE, Zimmern PE. Predictability of urody-namic findings based on the Urogenital Distress In-ventory-6 questionnaire. Urology. 1999;54(3):461-466.33. van Brummen HJ, Heintz AP, van der Vaart CH.The association between overactive bladder symp-toms and objective parameters from bladder diary andfilling cystometry. Neurourol Urodyn. 2004;23(1):38-42.34. Haeusler G, Hanzal E, Joura E, Sam C, Koelbl H.Differential diagnosis of detrusor instability and stress-incontinence by patient history: the Gaudenz-Incontinence-Questionnaire revisited.ActaObstet Gy-necol Scand. 1995;74(8):635-637.35. Khan MS, Chaliha C, Leskova L, Khullar V. Therelationship between urinary symptom question-naires and urodynamic diagnoses: an analysis of twomethods of questionnaire administration.BJOG. 2004;111(5):468-474.36. Versi E, Cardozo L, Anand D, Cooper D. Symp-toms analysis for the diagnosis of genuine stressincontinence. Br J Obstet Gynaecol. 1991;98(8):815-819.37. Klovning A, Hunskaar S, Eriksen BC. Validity of ascored urological history in detecting detrusor insta-
bility in female urinary incontinence. Acta Obstet Gy-necol Scand. 1996;75(10):941-945.38. Hsu TH, Rackley RR, Appell RA. The supine stresstest: a simplemethod to detect intrinsic urethral sphinc-ter dysfunction. J Urol. 1999;162(2):460-463.39. Kadar N. The value of bladder filling in the clini-cal detection of urine loss and selection of patients forurodynamic testing. Br J Obstet Gynaecol. 1988;95(7):698-704.40. Lobel RW, Sand PK. The empty supine stress testas a predictor of intrinsic urethral sphincter dysfunction.Obstet Gynecol. 1996;88(1):128-132.41. McLennanMT, Bent AE. Supine empty stress testas a predictor of low valsalva leak point pressure.Neu-rourol Urodyn. 1998;17(2):121-127.42. Walter AJ, Thornton JA, Steele AC. Further char-acterization of the supine empty stress test forpredicting low valsalva leak point pressures. IntUrogynecol J Pelvic Floor Dysfunct. 2004;15(5):298-301.43. Swift SE, Yoon EA. Test-retest reliability of thecough stress test in the evaluation of urinaryincontinence. Obstet Gynecol. 1999;94(1):99-102.44. Bergman A, McCarthy TA, Ballard CA, Yanai J.Role of the Q-tip test in evaluating stress urinaryincontinence. J Reprod Med. 1987;32(4):273-275.45. Bai SW, Lee JW, Shin JS, Park JH, Kim SK, ParkKH. The predictive values of various parameters in thediagnosis of stress urinary incontinence. Yonsei MedJ. 2004;45(2):287-292.46. Larsson G, Blixy C, Janson G, Victor A. The fre-
quency/volume chart as a differential diagnostic toolin female urinary incontinence. Int Urogynecol J. 1994;5:273-277.47. Tincello DG, Richmond DH. The Larsson fre-quency/volume chart is not a substitute for cystom-etry in the investigation of women with urinaryincontinence. Int Urogynecol J Pelvic Floor Dysfunct.1998;9(6):391-396.48. Resnick NM, Yalla SV. Detrusor hyperactivity withimpaired contractile function: an unrecognized butcommon cause of incontinence in elderly patients.JAMA. 1987;257(22):3076-3081.49. Carey MP, Dwyer PL, Glenning PP. The sign ofstress incontinence: should we believe what we see?Aust N Z J Obstet Gynaecol. 1997;37(4):436-439.50. De Muylder X, Claes H, Neven P, De Jaegher K.Usefulness of urodynamic investigations in femaleincontinence. Eur JObstet Gynecol Reprod Biol. 1992;44(3):205-208.51. Wall LL, Wiskind AK, Taylor PA. Simple bladderfilling with a cough stress test compared with sub-tracted cystometry for the diagnosis of urinaryincontinence. Am J Obstet Gynecol. 1994;171(6):1472-1477.52. Diokno AC, Dimaculangan RR, Lim EU, SteinertBW. Office based criteria for predicting type II stressincontinencewithout further evaluation studies. J Urol.1999;161(4):1263-1267.53. Ouslander J, Staskin D, Orzeck S, Blaustein J, RazS. Diagnostic tests for geriatric incontinence.World JUrol. 1986;4:16-21.
Education should have two objects: first, to give defi-nite knowledge, reading and writing, language andmathematics, and so on; second, to create those men-tal habits which will enable people to acquire knowl-edge and form sound judgments for themselves.Bertrand Russell (1872-1970)
URINARY INCONTINENCE
1456 JAMA, March 26, 2008Vol 299, No. 12 (Reprinted) 2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Georgian Court University User on 02/24/2015