DoD/PEPFAR ART Program COL Nelson Michael, M.D., Ph.D. Walter Reed Army Institute of Research U.S....
22
DoD/PEPFAR ART Program COL Nelson Michael, M.D., Ph.D. Walter Reed Army Institute of Research U.S. Military HIV Research Program Track 1.0 ART Program Meeting: Willard Intercontinental Track 1.0 ART Program Meeting: Willard Intercontinental Hotel Washington, D.C. Washington, D.C. August 11-12, 2008
-
Upload
damian-todd -
Category
Documents
-
view
216 -
download
1
Transcript of DoD/PEPFAR ART Program COL Nelson Michael, M.D., Ph.D. Walter Reed Army Institute of Research U.S....

DoD/PEPFAR ART Program
COL Nelson Michael, M.D., Ph.D.
Walter Reed Army Institute of ResearchU.S. Military HIV Research Program
Track 1.0 ART Program Meeting: Willard Intercontinental Track 1.0 ART Program Meeting: Willard Intercontinental HotelWashington, D.C.Washington, D.C.
August 11-12, 2008

DoD: A “Dual” Program
• Functions as an agency and an implementer.
• DoD HIV/AIDS Prevention Program (DHAPP), also seriving as the PEPFAR Executive Agent for DoD, and the U.S. Military HIV Research Program (USMHRP).
• DHAPP mil-mil: USMHRP mil-mil & mil-civ.
• Direct DoD PEPFAR funding in focus countries for COP FY08 ($83.3M) based on current MOA (May 2008):
• 50.2% support mil-mil programs (many reaching civ. populations)
• 49.8% for mil-civ efforts (~$41.5M COP FY08)
• Programs cover the full spectrum of PEPFAR program areas (country dependent).
• DoD provides direct TA to sites via clinical, lab and prevention experts.
• Level of in-country staffing for direct support/management varies.

DoD HIV/AIDS Programs in Africa (FY08)
Funding Sources
Red: PEPFAR Focus Country
Blue: PEPFAR Mini-Cop/Bilateral Country
Grey: DHAPP
White: No DoD Funding
USMHRP
Note: Sudan is a PEPFAR Mini-Cop country and DoD serves on PEPFAR Core Team but there is no DoD funding or presence in country.

• Maintain a low level of ex-pat/DoD technical staff with a focus on local resources for service delivery.
• Empower local leadership in determining course and approach to expansion.
• Expand clinic staff based on capacity of partner to absorb positions into annual budgets.
• Ongoing training capacity as part of the partner portfolio.
• Strengthen logistic infrastructure and capacity of local counterparts in areas of reagent and pharmaceutical supplies.
Sustainable Approach

USMHRP PEPFAR Programs
• Kenya
South Rift Valley: 2.5 million people
Kenya Department of Defense: 100K military + dependents
• Nigeria:
Nigerian Ministry of Defense: 380K active and retired military + dependents and ~1.5 million civilians
• Tanzania:
Southern Highlands: 6 million people
Tanzania Peoples Defense Forces: 120K military + dependents and ~800K civilians
• Uganda:
Kayunga District: 300K+ people
Catchment populations

Objectives of ART Activities
• Develop the local capacity to provide quality care and treatment services for HIV positive individuals, including necessary laboratory support.
• Enhance community networks through indigenous partners by linking treatment services with prevention and care.
• Increase the local capacity to support HIV treatment services by improving the technical knowledge and skills of indigenous staff and partners.

Continuum of Care in Resource Poor Settings
OVCOVC
Clinical Care &Support
Clinical Care &Support
Counseling and Testing
Counseling and Testing
PMTCTPMTCT
PreventionABC/IEC
PreventionABC/IEC
TransmissionPrevention
TransmissionPrevention
Home BasedPalliative
Care
Home BasedPalliative
Care
MTCTPlus
MTCTPlus
ARTART

Kenya DoD PEPFAR Sites
ART
TB/HIV
PMTCT

Nigeria DoD PEPFAR Sites

Tanzania DoD PEPFAR Sites

Uganda USMHRP* PEPFAR Sites
* DHAPP supports Uganda Peoples Defence Forces in country not depicted here or in ART and Care data on following slides.

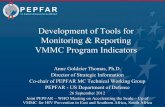
Patients Currently on ART by Country (>41K)*
0
5,000
10,000
15,000
20,000
25,000
30,000
Mar. 05 Sep. 05 Mar. 06 Sep.06 Mar.07 Sep. 07 Mar. 08
KenyaNigeriaTanzaniaUganda
To
tal
Nu
mb
er o
f P
atie
nts
* As of March 31st, 2008.
Percent pediatric cases as of March 31st, 2008 ranges from 4.4% in military programs (TPDF) to 10.2% civilian programs (SRV).

Patients Receiving Facility Based Clinical Care by Country*
0
50,000
100,000
150,000
200,000
250,000
300,000
Sep. 04 Mar. 05 Sep. 05 Mar. 06 Sep.06 Mar.07 Sep. 07 Mar. 08
Kenya
Nigeria
Tanzania
Uganda
To
tal
Nu
mb
er o
f P
atie
nts
* As of March 31st, 2008.

Clinical Outcomes
Median CD4 Counts*
Baseline CD4
CD4 at
6 months
CD4 at
12 months
CD4 at
18 months
CD4 at
24 months
Median 136 246 316 376 398
Median Difference from Baseline
- 110 180 240 262
Proportion of patients alive after 6, 12 and 24 months of ART: 1,992 out of 2,259 (88%)
Proportion of patients, who started ART, remained on ART for 1 or more years: 2,115 out of 2,580 (82%)
• Kericho District Hospital (Kenya). Cohorts of patients on treatment for period specified above (adults and peds.).• Data: Unlinked data from patient files, n = 2,190.

As of March 31st, 2008
Capacity Developed
Program
Number of palliative care outlets
Number of staff trained in provision of HIV palliative care
Number of ART outlets
Number of staff trained in provision of ART
Number of laboratories with capacity to perform 1) HIV tests and 2) CD4 tests and/or lymphocyte tests
Number of individuals trained in the provision of laboratory-related activites
Kenya 388 810 131 835 11 12Nigeria 37 172 41 208 34 86Tanzania 162 792 111 1,673 60 186Uganda 30 227 17 164 10 41Total 617 2,001 300 2,880 115 325
Treatment and Care Laboratory Infrastructure

Treatment of Common Opportunistic Infections
Infection Diagnosis Treatment Med. Supply*
Pulmonary TB Sputum/X-ray/AFB smear plus CXR - varies by country
MOH based Usually available
Cryptococcocal Meningitis CrAg** Fluconazole Erratic
Pneumocystis Carinii pneumonia Clinical symptoms CTX Adequate
Bacterial Pneumonia Clinical symptoms Antibiotics Adequate
Cutaneous fungal infections Clinical symptoms Antifungal creams and tablets
Erratic
Muco-cutaneous candidiasis Clinical symptoms Antifungal creams and tablets
Erratic
Diarrhea diseases Clinical symptoms Supportive therapy Adequate
HSV Clinical Symptoms Acyclovir Out of stock in Tanzania
Toxoplasmosis Clinical Symptoms High dose CTX Adequate
* Similar availability across countries, though some variation.** Kenya and Tanzania.

Cotrimoxazole Preventive Therapy
CTX provision varies by country and in accordance with local MOH guidance.
• Kenya HIV infected adults, adolescents and children are started on CTX after HIV diagnosis. Remain on CTX regardless of
ARV, treatment, clinical or immunological status.
HIV exposed infants are started on CTX from the age of 4-6 weeks and are only discontinued when an HIV negative status is confirmed.
Rate of uptake for qualified patients registered in the program is 90%. 10% of patients are allergic to sulphur base drugs.
• Nigeria All HIV positive, not just ART eligible initiated on CTX.
Drug availability- the drug cannot be imported and SCMS cannot purchase locally (certification issue). The Country will soon be issuing the drugs to our sites through the National Program.
• Tanzania All eligible patients for ART (CD4<200) get CTX prophylaxis.
Approximately 90% of eligible patients are provided with CTX.
• Uganda CTX given to all HIV+ patients (Dapsone given to those sensitive to CTX).
DoD procures over 80% of the CTX as govt. stock outs are common.

Malaria Prevention
• Kenya Malaria is the 2nd highest cause of morbidity (14 - 20% of out patient visits). Education on malaria prevention done at every military unit, Medical Reserve Station, ANC and ART clinics (military
and public). All military troops are provided with insect side treated mosquito nets. Pregnant women in malaria zones are provided with Intermittent Preventive Treatment using Sulphadoxine
Pyimethamine (PMI and other sources).
• Nigeria Limited to bed-nets and no presence of PMI in country.
• Tanzania Patients on ART are provided with antimalarial treatment in the CTC and provided health education on malaria
prevention.
Bed nets are provided to both children and pregnant women through ANC and CTC (linkage with PMI).
• Uganda All HIV+ patients receive malaria education at HIV clinic.
All HIV+ patients receive insecticide treated bed nets and early diagnosis and/or treatment for malaria as part of basic preventive care package (distribution between 95-100% of all patients via trained treatment club members - PLH).
Newly diagnosed HIV+ mothers receive preventive treatment.

Current and Future Directions
• Expanding services to lower level facilities and addressing HR/task shifting.
• Continue to transition technical capacity to partners and move towards more of a management role.
• Improve Early Infant Diagnosis (EID) and microbiology diagnostic capabilities.
• Continue to develop local partners capacity to evaluate their own services focusing on improving quality.
• Take more advantage and expand upon PHE opportunities and research experience to work with partners to:
Evaluate best methods of service delivery and how to expand. Address aspects of long term treatment and treatment failure.

Integrated Care, Treatment and Research
WHO
The Emergency Plan
The Global Fund
The World Bank
HIV Care and Treatment
HIV Research
DoD/HHS/NIH/CDC
Global HIV Vaccine Enterprise
IAVI/HVTN
WHO/UNAIDS
ANRS/MRC/EU/EC
Private Industry
Academia
Provides a comprehensive community-based platform to
support ethical research
Informs best practices and practical solutions in resource limited
settings for care and treatment

Enhancing ART ProgramsPublic Health Evaluation Initiatives
Current PHE activities or those to be submitted:
• Kenya
FY07 CLADE Study FY08 PMTCT, Pending FY09 Care and Treatment, Pending
• Tanzania
FY08 Early Mortality, Pending Pre-ART, Pending
• Uganda
FY08 Early Mortality, Pending PMTCT, Pending Facility Based AIDS Care, Pending

CLADE: Clinic-based ART & Diagnostic Evaluation A Public Health Evaluation of Routine vs. Viral Load Guided ART in ART Clinics in Rural Kenya
1:1
RoutineCare
VL GuidedCare
Primary Endpoints:1. Viral Failure2. Cost-Effectiveness
Eligibility:• > 18 y/o • CD4 < 200, or • TB/HIV with CD4 <350• No prior ART• Identified by clinic staff as eligible to begin ART
18 mo Ministry of Health follow-up
Secondary Endpoints:1. Combined clinical
outcome (AIDSprogression asdefined by 2 new WHO III or 1 newWHO IV event)
2. Death3. Hospitalization4. OIs5. Adherence6. Lost-to-follow-up7. Viral resistance in
treatment failuresand all viral failuresat the final study visit
8. Feasibility of VLmonitoring
9. Costs of VL monitoring10. GCP adherence
Baseline:• Clinical exam• Routine Labs• WHO staging• CD4, Arm-B Viral Load (VL)• Resistance testing (population based, random n=200)
Routine Care:• F/u q6mo with CD4s+WHO Staging or prnViral Load Guided Care:• F/u q6mo with VL, CD4, WHO Staging or prn
n=840
6-12 mo enrollment
24-30 mo study follow-up per participant (~ 1900 pt-years)
Primary Analyses:1. Chi Square/Fishers Exact tests and hazards analyses for VL endpoint2. Cost-effectiveness based upon viral success and variable costs 3. Routine descriptive statistics based upon metrics of feasibility, GCP, and comparative secondary endpoints
As of July 29, 2008