
Document of The World Bank · CURRENCY EQUIVALENTS (Exchange Rate Effective April 30, 2008)...
65
Document of The World Bank Report No: ICR0000668 IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-46290 IDA-35370 JPN-53117) ON A LOAN IN THE AMOUNT OF US$63.2 MILLION AND A CREDIT IN THE AMOUNT OF SDR 31.4 MILLION (US$40 MILLION EQUIVALENT) TO THE REPUBLIC OF INDONESIA FOR A SECOND PROVINCIAL HEALTH PROJECT June 27, 2008 Health, Nutrition and Population Sector Unit Human Development Department East Asia and Pacific Region Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of Document of The World Bank · CURRENCY EQUIVALENTS (Exchange Rate Effective April 30, 2008)...

Document of The World Bank
Report No: ICR0000668
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-46290 IDA-35370 JPN-53117)
ON A
LOAN IN THE AMOUNT OF US$63.2 MILLION AND A CREDIT
IN THE AMOUNT OF SDR 31.4 MILLION (US$40 MILLION EQUIVALENT)
TO THE
REPUBLIC OF INDONESIA
FOR A
SECOND PROVINCIAL HEALTH PROJECT
June 27, 2008
Health, Nutrition and Population Sector Unit Human Development Department East Asia and Pacific Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENTS
(Exchange Rate Effective April 30, 2008)
Currency Unit = Indonesian Rupiah (IDR) IDR 1.00 = US$ 0.00011
US$ 1.00 = IDR 9,234
FISCAL YEAR Government of Indonesia January 1 – December 31
ABBREVIATIONS AND ACRONYMS
ADB Asian Development Bank JPS-BK Social Safety Net, Health Component
Askeskin Health Insurance for the Poor Kanwil Kesehatan
Ministry of Health Provincial Office
Bappeda Regional Development Planning Agency KPKN Treasure Office Bappenas National Development Planning Agency MOF Ministry of Finance BLU General Service Unit MOH Ministry of Health BPKP Central Audit Bureau MOHA Ministry of Home Affairs BPS Central Bureau of Statistics NGO Non Government Organization CAS Country Assistance Strategy OECD Organization for Economic
Cooperation and Development CPCU Central Project Coordination Unit PCAR Procurement Capacity Assessment
Report Dinas Kesehatan
Local Government Health Department PCIU Provincial Central Implementation Unit
DIPA Development Budgets Allocations PHP Provincial Health Project DIU District Implementation Units PHPB Provincial Health Promotion Board DPRD District Assembly PMM Project Management Manual GOI Government of Indonesia RU Research Unit HIS Health Information System SK Decree IDA International Development Association TA Technical Assistance IG Inspectorate General TF Task Force JHC Joint Health Council TRT Technical Review Team
Vice President: James W. Adams
Country Director: Joachim von Amsberg Sector Manager: Fadia M. Saadah
Project Team Leader: Puti Marzoeki ICR Team Leader: Puti Marzoeki
INDONESIA The Second Provincial Health Project
CONTENTS
Data Sheet A. Basic Information B. Key Dates C. Ratings Summary D. Sector and Theme Codes E. Bank Staff F. Results Framework Analysis G. Ratings of Project Performance in ISRs H. Restructuring I. Disbursement Graph
1. Project Context, Development Objectives and Design............................................... 12. Key Factors Affecting Implementation and Outcomes .............................................. 53. Assessment of Outcomes .......................................................................................... 124. Assessment of Risk to Development Outcome......................................................... 205. Assessment of Bank and Borrower Performance ..................................................... 216. Lessons Learned ....................................................................................................... 267. Comments on Issues Raised by Borrower/Implementing Agencies/Partners .......... 27Annex 1. Project Costs and Financing.......................................................................... 30Annex 2. Outputs by Component ................................................................................. 31Annex 3. Economic and Financial Analysis................................................................. 36Annex 4. Bank Lending and Implementation Support/Supervision Processes ............ 37Annex 5. Beneficiary Survey Results ........................................................................... 39Annex 6. Stakeholder Workshop Report and Results................................................... 40Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR..................... 41Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders....................... 48Annex 9. List of Supporting Documents ...................................................................... 49Map IBRD 36234.......................................................................................................... 50
i
A. Basic Information Country: Indonesia Project Name:
ID-PROVINCIAL HEALTH II
Project ID: P049539 L/C/TF Number(s): IBRD-46290,IDA-35370,TF-53117
ICR Date: 06/27/2008 ICR Type: Core ICR Lending Instrument: SIL Borrower: GOI Original Total Commitment:
USD 103.2M Disbursed Amount: USD 57.0M
Environmental Category: C Implementing Agencies: Ministry of Health Cofinanciers and Other External Partners: B. Key Dates
Process Date Process Original Date Revised / Actual Date(s)
Concept Review: 12/21/2000 Effectiveness: 04/24/2002 04/24/2002 Appraisal: 04/18/2001 Restructuring(s): Approval: 06/26/2001 Mid-term Review: 10/15/2005 01/11/2006 Closing: 06/30/2007 06/30/2007 C. Ratings Summary C.1 Performance Rating by ICR Outcomes: Unsatisfactory Risk to Development Outcome: Substantial Bank Performance: Moderately Unsatisfactory Borrower Performance: Unsatisfactory
C.2 Detailed Ratings of Bank and Borrower Performance (by ICR) Bank Ratings Borrower Ratings
Quality at Entry: Moderately Satisfactory Government: Moderately Unsatisfactory
Quality of Supervision: Moderately Unsatisfactory
Implementing Agency/Agencies: Unsatisfactory
Overall Bank Performance:
Moderately Unsatisfactory
Overall Borrower Performance: Unsatisfactory
ii
C.3 Quality at Entry and Implementation Performance Indicators Implementation
Performance Indicators QAG Assessments (if any) Rating
Potential Problem Project at any time (Yes/No):
Yes Quality at Entry (QEA):
None
Problem Project at any time (Yes/No):
Yes Quality of Supervision (QSA):
None
DO rating before Closing/Inactive status:
Moderately Unsatisfactory
D. Sector and Theme Codes
Original Actual Sector Code (as % of total Bank financing) Central government administration 3 3 Compulsory health finance 2 2 Health 91 91 Sub-national government administration 4 4
Theme Code (Primary/Secondary) Decentralization Primary Primary Health system performance Primary Primary Other communicable diseases Primary Primary Participation and civic engagement Secondary Secondary Rural services and infrastructure Primary Primary E. Bank Staff
Positions At ICR At Approval Vice President: James W. Adams Jemal-ud-din Kassum Country Director: Joachim von Amsberg Mark Baird Sector Manager: Fadia M. Saadah Maureen Law Project Team Leader: Puti Marzoeki Samuel S. Lieberman ICR Team Leader: Puti Marzoeki ICR Primary Author: Aparnaa Somanathan F. Results Framework Analysis Project Development Objectives (from Project Appraisal Document) The project's goals are, first, to bring about effective health sector decentralization in the provinces of North Sumatera, West Java, and Banten. The challenge is to initiate key

iii
sector reforms and put health financing on a firm footing, while protecting health services which are essential for the poor and the public at large during a period of government restructuring. The second objective is to help the Ministry of Health carry out its role in a decentralized system. These responsibilities encompass providing sectoral vision and leadership, analysis and policy follow up of the health needs of the poor and risks to the public at large, advocacy of best practices and standards, and support for local initiative. Revised Project Development Objectives (as approved by original approving authority) (a) PDO Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 : Changes in organization structure, health financing mechanisms, service delivery arrangements and workforce policies.
Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO is too broad. See intermediate outcome indicators 1-9
Indicator 2 : Implementation of effective, locally relevant curative service delivery and financing arrangements.
Value quantitative or Qualitative)
Districts applied historical planning and budgeting
Four rounds of annual district grants prepared following evidence based planning principles
Three rounds of annual district grants prepared following evidence based
Date achieved 04/24/2002 06/30/2007 06/30/2007 Comments (incl. % achievement)
There was only 3 rounds of district grants because of delayed project effectiveness
Indicator 3 : Implementation of effective, locally grounded public health service provision and financing arrangements.
Value quantitative or Qualitative)
Districts applied historical planning and budgeting
Four rounds of annual district grants prepared following evidence based planning principles
Three rounds of annual district grants prepared following evidence based planning principles
Date achieved 04/24/2002 06/30/2007 06/30/2007 Comments There was only 3 rounds of district grants because of delayed project

iv
(incl. % achievement)
effectiveness
Indicator 4 : Increased awareness within GOI and among the public of health issues/risks/solutions.
Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO is too borad. See Intermediate Outcome Indicator 12
Indicator 5 : Indications of enhanced commitment at the province and district levels including financing of priority programs, and basic services/drugs for the poor, and inclusion of health indicators in the DAU formula.
Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO is too broad. See intermediate outcome indicator 16
Indicator 6 : Effective partnership arrangements with districts, provinces, and NGOs. Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO is too broad. See intermediate outcome indicator 16
Indicator 7 : Enhanced effectiveness of communicable disease surveillance. Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO is too broad. See intermediate outcome indicator 13, 14
Indicator 8 : Enhanced food and drug inspection systems and public accountability. Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
See Intermediate Outcome Indicator 17
v
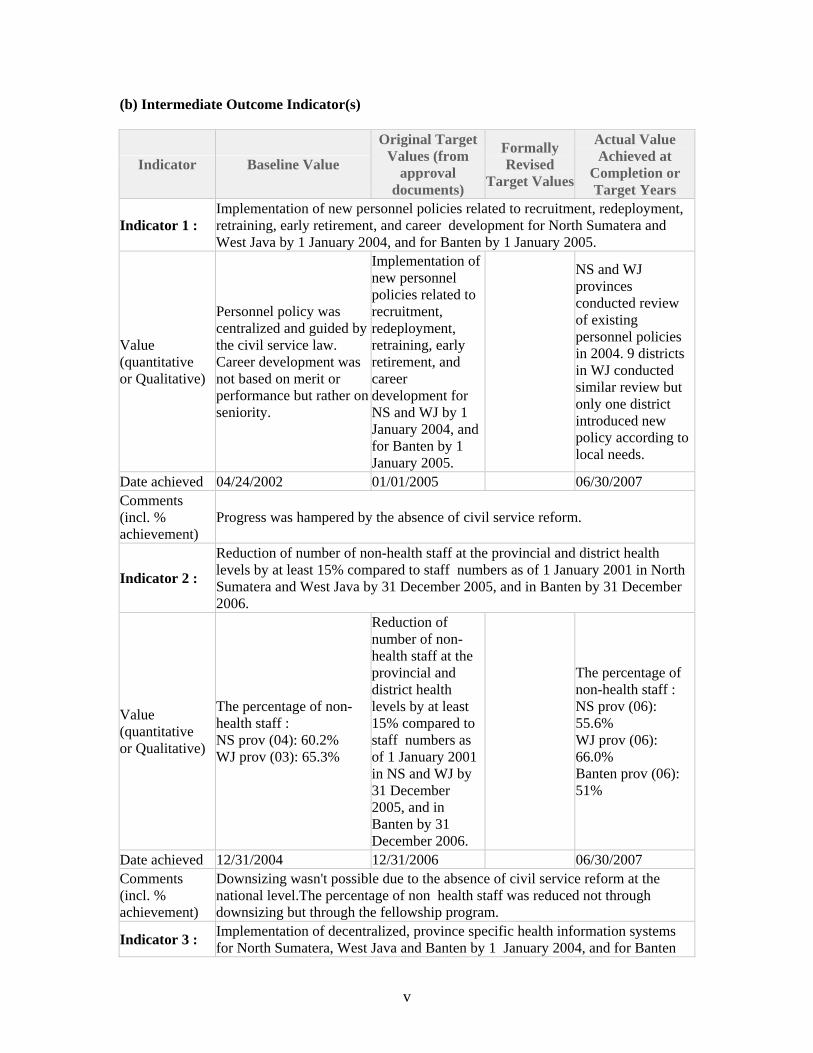
(b) Intermediate Outcome Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised
Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 : Implementation of new personnel policies related to recruitment, redeployment, retraining, early retirement, and career development for North Sumatera and West Java by 1 January 2004, and for Banten by 1 January 2005.
Value (quantitative or Qualitative)
Personnel policy was centralized and guided by the civil service law. Career development was not based on merit or performance but rather on seniority.
Implementation of new personnel policies related to recruitment, redeployment, retraining, early retirement, and career development for NS and WJ by 1 January 2004, and for Banten by 1 January 2005.
NS and WJ provinces conducted review of existing personnel policies in 2004. 9 districts in WJ conducted similar review but only one district introduced new policy according to local needs.
Date achieved 04/24/2002 01/01/2005 06/30/2007 Comments (incl. % achievement)
Progress was hampered by the absence of civil service reform.
Indicator 2 :
Reduction of number of non-health staff at the provincial and district health levels by at least 15% compared to staff numbers as of 1 January 2001 in North Sumatera and West Java by 31 December 2005, and in Banten by 31 December 2006.
Value (quantitative or Qualitative)
The percentage of non-health staff : NS prov (04): 60.2% WJ prov (03): 65.3%
Reduction of number of non-health staff at the provincial and district health levels by at least 15% compared to staff numbers as of 1 January 2001 in NS and WJ by 31 December 2005, and in Banten by 31 December 2006.
The percentage of non-health staff : NS prov (06): 55.6% WJ prov (06): 66.0% Banten prov (06): 51%
Date achieved 12/31/2004 12/31/2006 06/30/2007 Comments (incl. % achievement)
Downsizing wasn't possible due to the absence of civil service reform at the national level.The percentage of non health staff was reduced not through downsizing but through the fellowship program.
Indicator 3 : Implementation of decentralized, province specific health information systems for North Sumatera, West Java and Banten by 1 January 2004, and for Banten

vi
by January 1, 2005.
Value (quantitative or Qualitative)
Provinces and Districts implemented centrally developed HIS known as SP2TP and S2RS which only record information from the public sector.
Implementation of decentralized, province specific health information systems for NS, WJ by 1 January 2004 and for Banten by 1 January 2005.
NS conducted review of existing HIS in 2004 and develop a blue print for an integrated HIS in 2006 but not yet implemented. WJ only prepared instruments for collecting baseline of HIS status Banten, only Tangerang district has a locally developed HIS.
Date achieved 04/24/2002 01/01/2005 06/30/2007 Comments (incl. % achievement)
Indicator 4 : Implementation of new licensing and accreditation system (for health manpower and health facilities) for North Sumatera and West Java by 1 January 2003, and for Banten by 1 January 2004.
Value (quantitative or Qualitative)
License to practice's provided by the DHO based on fulfillment of some admin criteria incl a letter of recommendation frm the local branch of prof assoc.Accreditation of hospitals' conducted by a team frm the PHO using centrally developed instrument
Implementation of new licensing and accreditation system (for health manpower and health facilities) for NS and WJ by 1 January 2003 and for Banten by 1 January 2004.
NS and WJ designed an independent Quality Council to be responsible for quality assessment of providers in 2006. WJ has drafted a regulation on this for signing by the Governor.
Date achieved 04/24/2002 01/01/2003 06/30/2007 Comments (incl. % achievement)
Indicator 5 : Implementation of at least 2 public accountability mechanisms for North Sumatera and West Java by January 1, 2003, and for Banten by 1 January 2004.
Value (quantitative or Qualitative)
Public accountability was not a popular concept, some health offices and health facilities used suggestion boxes to receive complaints A complaint resolution mechanism for the JPSBK program was available on paper.
Implementation of at least 2 public accountability mechanisms for N S and WJ January 1, 2003, and for Banten by 1 January 2004.
By 2006, Healthy District Forum (FKK) was implemented in 16 districts in NS. By 2006, 15 districts in WJ preferred to continue with the implementation of a
vii
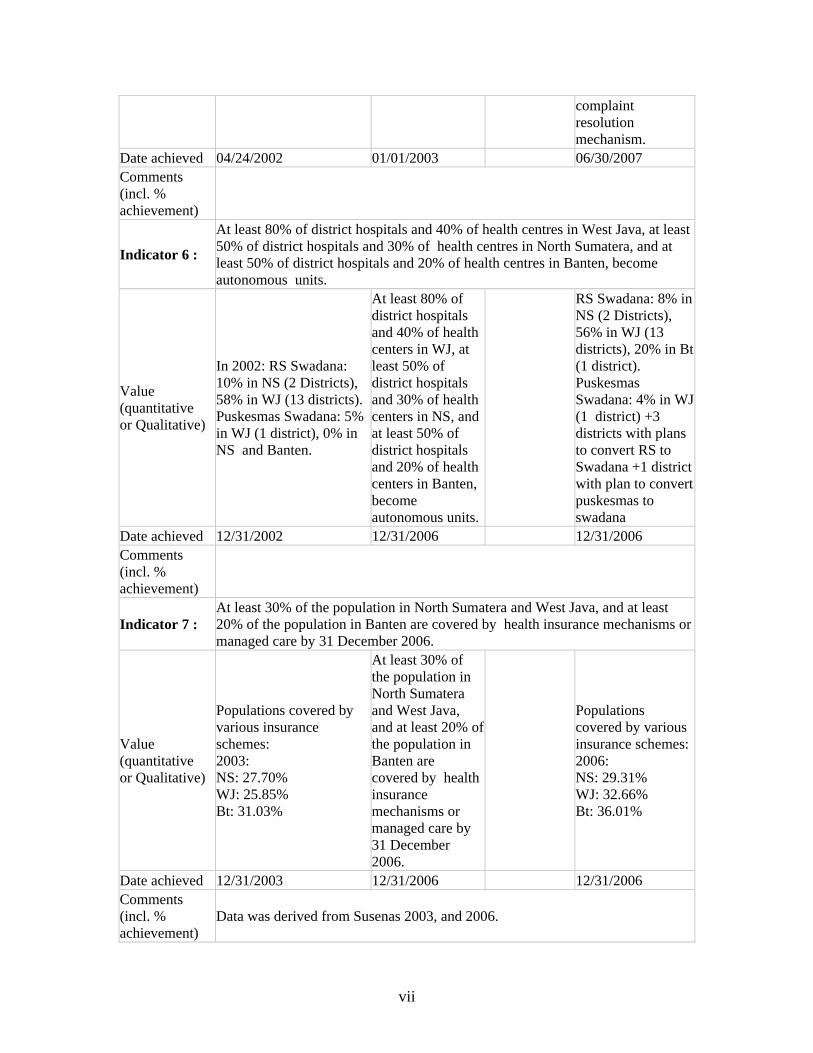
complaint resolution mechanism.
Date achieved 04/24/2002 01/01/2003 06/30/2007 Comments (incl. % achievement)
Indicator 6 :
At least 80% of district hospitals and 40% of health centres in West Java, at least 50% of district hospitals and 30% of health centres in North Sumatera, and at least 50% of district hospitals and 20% of health centres in Banten, become autonomous units.
Value (quantitative or Qualitative)
In 2002: RS Swadana: 10% in NS (2 Districts), 58% in WJ (13 districts). Puskesmas Swadana: 5% in WJ (1 district), 0% in NS and Banten.
At least 80% of district hospitals and 40% of health centers in WJ, at least 50% of district hospitals and 30% of health centers in NS, and at least 50% of district hospitals and 20% of health centers in Banten, become autonomous units.
RS Swadana: 8% in NS (2 Districts), 56% in WJ (13 districts), 20% in Bt (1 district). Puskesmas Swadana: 4% in WJ (1 district) +3 districts with plans to convert RS to Swadana +1 district with plan to convert puskesmas to swadana
Date achieved 12/31/2002 12/31/2006 12/31/2006 Comments (incl. % achievement)
Indicator 7 : At least 30% of the population in North Sumatera and West Java, and at least 20% of the population in Banten are covered by health insurance mechanisms or managed care by 31 December 2006.
Value (quantitative or Qualitative)
Populations covered by various insurance schemes: 2003: NS: 27.70% WJ: 25.85% Bt: 31.03%
At least 30% of the population in North Sumatera and West Java, and at least 20% of the population in Banten are covered by health insurance mechanisms or managed care by 31 December 2006.
Populations covered by various insurance schemes: 2006: NS: 29.31% WJ: 32.66% Bt: 36.01%
Date achieved 12/31/2003 12/31/2006 12/31/2006 Comments (incl. % achievement)
Data was derived from Susenas 2003, and 2006.
viii
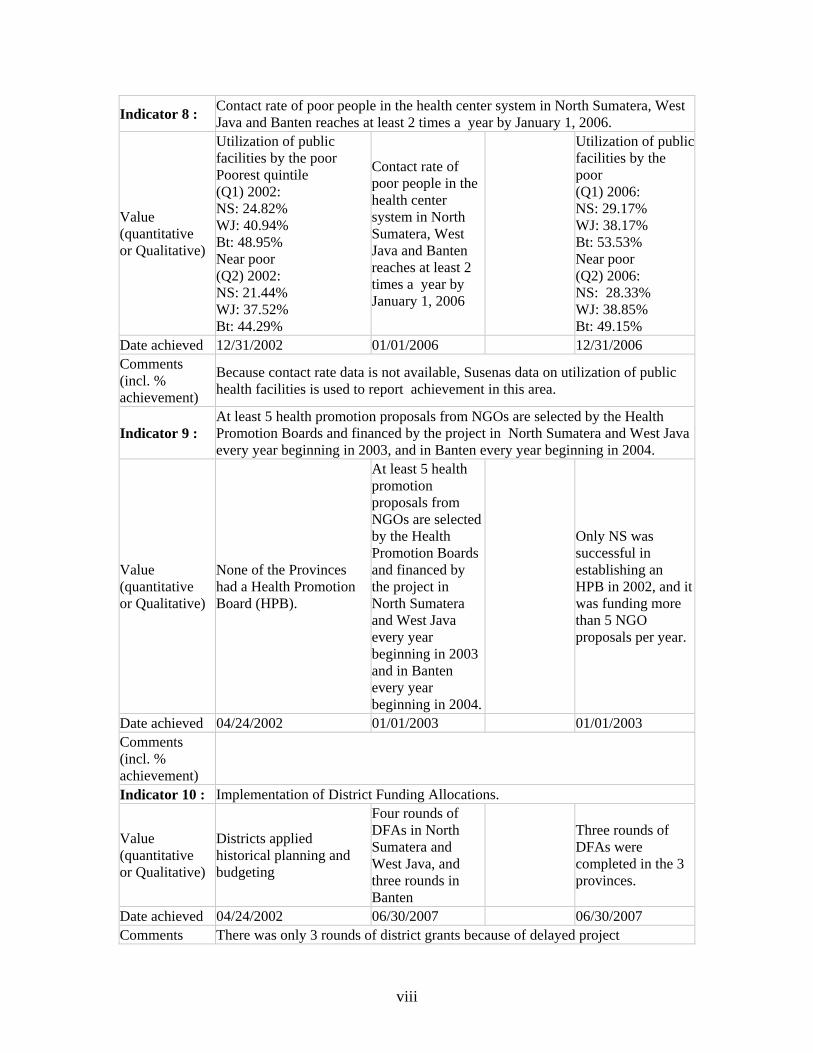
Indicator 8 : Contact rate of poor people in the health center system in North Sumatera, West Java and Banten reaches at least 2 times a year by January 1, 2006.
Value (quantitative or Qualitative)
Utilization of public facilities by the poor Poorest quintile (Q1) 2002: NS: 24.82% WJ: 40.94% Bt: 48.95% Near poor (Q2) 2002: NS: 21.44% WJ: 37.52% Bt: 44.29%
Contact rate of poor people in the health center system in North Sumatera, West Java and Banten reaches at least 2 times a year by January 1, 2006
Utilization of public facilities by the poor (Q1) 2006: NS: 29.17% WJ: 38.17% Bt: 53.53% Near poor (Q2) 2006: NS: 28.33% WJ: 38.85% Bt: 49.15%
Date achieved 12/31/2002 01/01/2006 12/31/2006 Comments (incl. % achievement)
Because contact rate data is not available, Susenas data on utilization of public health facilities is used to report achievement in this area.
Indicator 9 : At least 5 health promotion proposals from NGOs are selected by the Health Promotion Boards and financed by the project in North Sumatera and West Java every year beginning in 2003, and in Banten every year beginning in 2004.
Value (quantitative or Qualitative)
None of the Provinces had a Health Promotion Board (HPB).
At least 5 health promotion proposals from NGOs are selected by the Health Promotion Boards and financed by the project in North Sumatera and West Java every year beginning in 2003 and in Banten every year beginning in 2004.
Only NS was successful in establishing an HPB in 2002, and it was funding more than 5 NGO proposals per year.
Date achieved 04/24/2002 01/01/2003 01/01/2003 Comments (incl. % achievement)
Indicator 10 : Implementation of District Funding Allocations.
Value (quantitative or Qualitative)
Districts applied historical planning and budgeting
Four rounds of DFAs in North Sumatera and West Java, and three rounds in Banten
Three rounds of DFAs were completed in the 3 provinces.
Date achieved 04/24/2002 06/30/2007 06/30/2007 Comments There was only 3 rounds of district grants because of delayed project

ix
(incl. % achievement)
effectiveness
Indicator 11 : Health spending increases at the district level between 2001 and 2006, reaching 15% of total local government spending (or Rp.42,000 per capita in 2001 prices) by 2006.
Value (quantitative or Qualitative)
None of the districts in PHP II provinces allocated at least 15% of APBD for health.
Health spending increases at the district level between 2001 and 2006, reaching 15% of total local government spending (or Rp.42,000 per capita in 2001 prices) by 2006.
Only 3 Districts in WJ achieved the minimum 15% target in 2006.
Date achieved 04/24/2002 12/31/2006 06/30/2007 Comments (incl. % achievement)
There was no data to measure this indicator. Most districts did not have Distsrict Health Accounts
Indicator 12 : A Decentralization Unit is set up and functioning at the central level by December 31, 2001
Value (quantitative or Qualitative)
Preliminary decentralization unit
Establishment of Decentralization Unit
Establishment of Decentralization Unit
Date achieved 07/23/2001 12/31/2001 03/20/2002 Comments (incl. % achievement)
Indicator 13 : Establishment of Geographic Information System and Early Warning Outbreak Response System for communicable diseases in Banten, North SUmatera, and West java by June 30, 2004
Value (quantitative or Qualitative)
GIS and EWORS pilot in selected districts in 6 provinces
Establishment of GIS and EWORS in the 3 provinces
Achievement of MOU between the center and Head of Health Office in each district
Date achieved 04/24/2002 06/30/2004 06/30/2007 Comments (incl. % achievement)
Indicator 14 : A public health laboratory for environmental health and communicable disease control are estbalished in Jakarta and Medan by December 31, 2003
Value (quantitative or Qualitative)
An environmental health laboratory existed in Jakarta and Medan
A public health laboratory for environmental health and communicable disease control are
A public health laboratory for environmental health and communicable disease control are

x
estbalished in Jakarta and Medan
estbalished in Jakarta and Medan
Date achieved 04/24/2002 12/31/2003 06/30/2007 Comments (incl. % achievement)
Establishment of the labs was fully funded by APBN not PHP II
Indicator 15 : Sulianti Saroso hospital is functioning as a center of excellence for communicable disease case management by June 30, 2004
Value (quantitative or Qualitative)
Sulianti Saroso is an infectious disease hospital
Sulianti Saroso hospital is functioning as a center of excellence for communicable disease case management
Sulianti Saroso hospital is the center of excellence for CD case management in Indonesia
Date achieved 04/24/2002 06/30/2004 06/30/2007 Comments (incl. % achievement)
Establishment of Sulianti Saroso hospital as a center of excellence for CD case management was fully funded by APBN not PHP II
Indicator 16 : A national health grants mechanism to assist poorer districts is established and an initial set of pilot grants is evaluated by December 31, 2002
Value (quantitative or Qualitative)
No matching grant scheme
A national health grants mechanism to assist poorer districts is established and an initial set of pilot grants is evaluated
A two year NHG pilot was completed
Date achieved 04/24/2002 12/31/2002 06/30/2007 Comments (incl. % achievement)
More than 20 district proposal were financed through the NHG scheme but no formal evaluation was conducted
Indicator 17 : An enhanced inspection systems related to food and drug control is in place by December 31, 2003
Value (quantitative or Qualitative)
An enhanced inspection systems related to food and drug control is in place
A model for drug inspection system and inspector management
Date achieved 12/31/2003 06/30/2007 Comments (incl. % achievement)
Indicator 18 : A food and drug complaiant resolution mechanism is established within regional food and drug control offices by December 31, 2003
Value (quantitative or Qualitative)
A Food and drug complaiant resolution
A hotline service was established at the center for

xi
mechanism is established within regional food and drug control offices
providing response to questions on food and drug safety and quality issues
Date achieved 12/31/2003 06/30/2007 Comments (incl. % achievement)
Indicator 19 : The Research Unit under Part B.6 of the Project is established by June 30, 2002
Value (quantitative or Qualitative)
The Research Unit under Part B.6 of the Project is established
The Research Unit was established on 07/23/2003
Date achieved 06/30/2002 07/23/2003 Comments (incl. % achievement)
G. Ratings of Project Performance in ISRs
No. Date ISR Archived DO IP
Actual Disbursements (USD millions)
1 12/10/2001 Satisfactory Satisfactory 0.00 2 06/03/2002 Satisfactory Satisfactory 0.63 3 11/26/2002 Satisfactory Satisfactory 4.63 4 06/12/2003 Satisfactory Satisfactory 4.63 5 12/23/2003 Satisfactory Satisfactory 5.28 6 06/28/2004 Satisfactory Satisfactory 8.32 7 12/15/2004 Satisfactory Satisfactory 17.65 8 12/29/2004 Satisfactory Satisfactory 17.65 9 12/29/2004 Satisfactory Satisfactory 17.65
10 05/13/2005 Satisfactory Satisfactory 28.86 11 06/17/2005 Satisfactory Satisfactory 28.86 12 06/30/2005 Satisfactory Unsatisfactory 28.86 13 04/26/2006 Moderately Satisfactory Unsatisfactory 35.37
14 01/12/2007 Moderately Unsatisfactory Unsatisfactory 65.55
15 06/29/2007 Moderately Unsatisfactory Unsatisfactory 75.23
H. Restructuring (if any) Not Applicable

xii
I. Disbursement Profile
1
1. Project Context, Development Objectives and Design
1.1 Context at Appraisal The Indonesia Provincial Health Project II (PHP II) was approved by the Board on June 26, 2001, and became effective on April 24, 2002 for an original Credit amount of US$40 million equivalent and a loan of US$63.2 million. At the time PHP II was designed and appraised, a major reorganization of government involving decentralization was underway in Indonesia. These changes brought new opportunities and risks for a health sector that was overstretched in the pre-crisis period and was further disrupted during the economic crisis of the late 1990s. In North Sumatera, West Java and Banten, the project’s three focal provinces, health outcomes in the late 1990s were unsatisfactory. Utilization of government health facilities remained low and was characterized by sharp differentials across income groups. Coverage of JPS-BK, the health component of the country’s social safety program, set up in response to the economic crisis was also weak. Less than 30% of the intended beneficiaries in each of the three provinces were covered due to ineffective targeting mechanism and inflexible program guidelines and procedures. Underlying the poor performance was chronic underfunding for the health sector, exacerbated by high levels of technical and allocative inefficiency in the allocation of the scarce resources. In addition, there was weak capacity at the province and district levels for priority setting, program design and evaluation. Decentralization served to highlight these weaknesses. Province-level projects like PHP II represented a distinctive and useful component in the Government of Indonesia Ministry of Health (GOI/MOH’s) decentralization strategy. The First Provincial Health Project (PHP I), which became effective in August 2001, provided a template for tackling health decentralization within the sub-national framework. The Credit/Loan provided under PHP II was intended to support a further extension of this approach in response to decentralization. The value-added of Bank support included both content and process dimensions. Through the process of decentralization in Indonesia, the Bank emphasized the need to pay attention to the opportunities and risks inherent in decentralization. A further contribution of the Bank was its ability to include inputs from efforts to monitor decentralization issues across sectors.

2
1.2 Original Project Development Objectives (PDO) and Key Indicators (as approved) The project's goals are, first, to bring about effective health sector decentralization in the provinces of North Sumatera, West Java, and Banten. The challenge is to initiate key sector reforms and put health financing on a firm footing, while protecting health services which are essential for the poor and the public at large during a period of government restructuring. The second objective is to help the Ministry of Health carry out its role in a decentralized system. These responsibilities encompass providing sectoral vision and leadership, analysis and policy follow-up of the health needs of the poor and risks to the public at large, advocacy of best practices and standards, and support for local initiatives. For the first PDO, there were three Outcome/Impact Indicators: (i) changes in organization structure, health financing mechanisms, service delivery arrangements and work force policies; (ii) implementation of effective, locally relevant curative service delivery and financing arrangements; and (iii) implementation of effective, locally grounded public health service provision and financing arrangements. For the second PDO, there were five Outcome/Impact Indicators: (i) increased awareness within GOI and among the public of health issues/risks/solutions; (ii) indications of enhanced commitment at the province and district levels including financing of priority programs, and basic services/drugs for the poor, and inclusion of health indicators in the block funding allocation (DAU) formula; (iii) effective partnership arrangements with districts and provinces and with NGOs; (iv) enhanced effectiveness of communicable disease surveillance; and (v) enhanced food and drug inspection systems and public accountability.
1.3 Revised Project Development Objectives and Key Indicators, and Reasons/Justification N/A
1.4 Main Beneficiaries The population and more specifically, poor households located in North Sumatera’s 19, West Java’s 22 and Banten’s 6 districts and municipalities were expected to benefit from the project. According to the Central Bureau of Statistics (BPS), the percentage of poor people in 1996 in North Sumatera and West Java (including Banten at the time) was around 10%, but had risen to roughly 22% in North Sumatera, 21% in West Java (excluding Banten) by early 1999 due to the economic crisis. Approximately, 2.9 million people in North Sumatera and 8 million people in West Java (including Banten) were defined as poor in 1999.

3
The poor were expected to benefit from the project through improved access to higher quality health services. Government subsidies were to be targeted more effectively by allocating project funds based on the number of poor people in each district and the rates of public facility use by the poor. Districts in turn, were to be encouraged to develop mechanisms to improve use by the poor. The population living in other provinces was expected to benefit also through strengthened disease control, improved drug and food oversight and improved mechanisms for targeting public subsidies.
1.5 Original Components Like PHP I, PHP II consisted of two components, one addressing health needs and issues in specific districts and provinces, and the second focusing on responsibilities and functions of mainly the MOH, but also a newly created food and drug control agency.
Component A – Districts and Provinces A1: Managing Decentralization (US$ 20.07 million; 2.2% of total cost) Project supported Task Forces would focus on critical institutional topics and develop recommendations for implementation in Phases 1 and 2. The work of the tasks forces would cover: (i) restructuring health organization in the provinces and districts; (ii) human resource management and development; (iii) developing new health information systems; (iv) upgrading the regulatory framework including the licensing and certification of health professionals and accreditation of health care organizations; (v) strengthening public accountability mechanisms; and (vi) intensifying health promotion. A2: Resource Mobilization (US$ 2.43 million; 0.3% of total cost) District Health Offices (DHOs) would work individually or through the task forces to explore ways of financing district health needs. This included both making the case for adequate allocations from the district health budget, and relying on user fees whenever the population had the ability to pay for treatment costs. A3: District Funding Allocations (US$ 850.44 million; 94.9% of total cost) Starting in 2003 (2004 in Banten) Credit/Bank resources would be channelled to districts through block allocations with the aim of raising government health spending to levels which are sustainable during the medium term. During negotiations, assurances were received that government health spending levels would be equal to at least Rp 42,000 per capita in 2001 prices, or 15% of total district health expenditures by the end of the project in 2006. The locally financed portion of the district budget was to be treated as counterpart funding. A4: Project Management (US$ 5.03 million; 0.6% of total cost) Project management units would be established at the province and district levels. Funds would be allocated to support consultant services, supplies and supervision.

4
Component B – The Center B1: Institutional Development (US$ 1.92 million; 0.2% of total cost) The project would assist in establishing a small, functional Decentralization Unit within MOH. B2: Strengthening Communicable Disease Control (US$ 8.57 million; 1.0% of total cost) The project would help transform the existing Directorate General (DG) for Communicable Disease Control (P2M) into a specialized central agency within MOH. To this end, PHP II would support the adaptation in West Java, North Sumatera and Banten, the development of a surveillance system already implemented in six other provinces with ADB support. B3: Ensuring Equity in Service Provision (US$ 3.48 million; 0.4% of total cost) PHP II would fund National Health Grants to reorient district health systems, provide cost-effective public health programs and co-finance catastrophic care for the poor. Funds would be directed to roughly 20 poor districts which also satisfied other criteria. B4: Assessing Health Research Needs, Capacities and Options (US$0.06 million; 0.0% of total cost) PHP II would support a broad analysis of health research requirements and options within a decentralized system. B5: Strengthening Food and Drug Control (US$ 2.01 million; 0.2% of total cost) PHP II would assist in transforming the newly created food and drug agency into a professional unit whose operations are based on scientific, risk management principles. At the time PHP II was appraised, GOI had just established an autonomous drug and food control agency (NADFC) and adjusted the roles and responsibilities of the former Directorate General of Drug of Food Control of MOH (DG POM). B6: Project Management (US$ 1.79 million; 0.2% of total cost) A coordination unit (CPCU) would be established at the central level for overall coordination of PHP II. Project funds would be used to support consultant services, office equipment and supplies, workshop, project management training and project supervision.
1.6 Revised Components N/A

5
1.7 Other Significant Changes The World Bank withheld payment under categories 3 (workshop/training) and 7 (incremental operating cost) under the project for a period of 12 months (May 2005 to May 2006) following confirmation of fraudulent practices at the central level. Based on the findings of the investigation, the World Bank declared an amount of IDR 8,673,492,880 as ineligible expenditures. Payment for both categories continued after the government fulfilled an action plan to strengthen internal financial control of the project. The CPCU was dismantled and project management responsibility was transferred to a different team as a result of this. On December 21, 2006, upon request from the Government, the World Bank cancelled a part of the loan amounting US$32 million. 2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry
Context Influencing Project Design
PHP II and the predecessor to this project, PHP I, were designed with the specific intention of assisting government in addressing the challenges faced by the health sector as a consequence of decentralization in Indonesia as mandated by Laws 22 and 25. These laws, signed in 1999, provided the statutory underpinning for Indonesia’s Big Bang decentralization of 2001. Law 22 provided the conceptual and legislative framework for decentralization, transferring planning, budgeting and implementing responsibilities to districts. Law 25 complemented Law 22 by augmenting and increasing the predictability of financing for local governments. This resulted in the district becoming the key level for policy implementation as well as formulation and also led to greatly increased resources for districts. Thus, local assemblies and district chief executives (Bupatis) assumed responsibility for managing health centers and public hospitals. Districts also took on training and regulatory functions, and became responsible for priority setting and resource allocation, together with some quality assurance and personnel management functions. The project design that emerged in the context of this process of rapid decentralization reflected several key considerations. First, because Laws 22 and 25 affected virtually every dimension of health and health care, project designers believed a sector-wide approach was essential to preserve basic health services, especially for the poor, during the period in which new systems were being established in response to rapid decentralization. This was a significant departure from previous “program-oriented” health projects. Second, the project designers believed an essential initial priority was to address the issue of the readiness of government structures to take on their expanded policy and implementation roles.
6
Thus, while supportive of the process of decentralization in health, the project, by design recognized that some of the new functions districts were being asked to take on would be problematic given the small size of their populations and lack of specialized staff. These included essential public health, health education and information functions for which districts could not capture scale and scope advantages or gains that would yield externalities. The project therefore proposed to support selected central and provincial activities chosen on the basis of the extent to which these activities would result in scale and scope economies and externalities In taking this position, the project took advantage of in the fact that Law 22 acknowledged that districts may not have the scale, depth and numbers of staff and other resources to carry out all of the health responsibilities that the central government was mandated to transfer. Building on the literature and experience with decentralization in other countries, scale, scope and externality considerations led project designers to argue that certain responsibilities previously held at the central level should be assigned to the province level. It was felt that an important contribution of the project would be to highlight functions and roles that are best handled by provinces. These include surveillance, most aspects of communicable disease control and health promotion. While most of project activities and support were directed at the provincial and district levels, the project also included a small component to support central-level agencies with the decentralization process. The project design included the establishment of a decentralization unit within central MOH to facilitate health decentralization and reform. This unit was also supposed to recommend strategies for transforming MOH internally to better respond to and prepare for decentralization, and be more responsive to customer perceptions and preferences. Project design also recognized that Law 22 had changed the hierarchal relationship between districts, provinces and central authorities. The project foresaw a need for new policy mechanisms to ensure that cross-district health concerns were addressed. This led to the recommendation that a Joint Health Council (JHC) be constituted at the provincial level, which would become a forum for raising health issues, sharing management burdens, formulating common policies and organizing advocacy efforts. Technical support to the JHC to carry out these functions was to be provided by the Technical Review Team and Task Forces that would focus on key institutional and health policy issues, as well as generate recommendations for implementation. Finally, the project adopted a management structure that fitted the decentralized structure; Project Directors at the Provincial and District levels were the local government chief executives while the Deputy Provincial Directors were the head of the province/district health office.

7
Limitations of the Overall Design The project design was in general an appropriate response to the challenges confronted at the time by a rapidly changing health sector. Project design documents reflected a strong awareness of the risks involved in proceeding with rapid decentralization in the health sector, citing approaches that had proved difficult in other country contexts. It also offered a thoughtful analysis of the functions that should be undertaken at each level of government in order to ensure that decentralization in health would contribute as much as possible to improved health outcomes, particularly for the poor. It can be argued also that if the Bank was to be helpful to the government in the then on-going process of rapid decentralization, the project had little choice but to accept considerable risk and uncertainty. The program was designed to be flexible but that also posed some challenges as noted below. A key limitation was in the design of the central-level component, which was more complex under PHP II than under PHPI, and thus placed greater demands on central-level policymakers. PHP II envisaged the establishment of the Decentralization Unit that would help achieve the institutional commitment and support needed to sustain decentralization. In reality, this proved to be ineffective in bringing about significant institutional change. Most departments did not share the vision of changing the role of the central ministry to one of primarily facilitating, monitoring, and advocating for improved provision of services at the district level. Wide-reaching central-level reforms were proposed to strengthen communicable disease surveillance, health information systems and, food and drug control. In a context where support for decentralization was weak, this proved too extensive a range of reforms for MOH to undertake at the central level. While it is acknowledged that it is not realistic to expect one operation to change this, the project was too ambitious in its expectations. A second limitation was that the project design took on a broad range of reform activities. The scope of the reform agenda was equally broad under PHP I, yet feasible to implement. The difference under PHP II was that the project was being scaled up to larger provinces with greater heterogeneity in initial conditions and institutional capacity. Given this, a more feasible approach would have been to use the project to provide a menu of reform areas, which the provinces and districts could have selected from to outline a program of reforms. Clearly articulated provincial plans would have provided guidance to the provinces, especially those with less capacity to focus their efforts and reforms, and thus achieved better results. A third limitation of project design was that it underestimated the extent to which the existing, as well as ever changing civil service regulations would constrain the project’s ability to achieve progress on the project’s human resource management agenda.

8
2.2 Implementation The innovative instruments introduced by the project at the province level (TRT, JHC, TFs, etc.) were, overall, successful and contributed to the success of the district grants component. Of these mechanisms, the Technical Review Team (TRT) was the most successful, particularly in West Java. Districts in West Java reported to the ICR team that the West Java TRT was strong and its support was quite valuable. Experience with the Joint Health Council (JHC) confirmed the need for a mechanism supporting cross-district discussion of health issues, but it proved unrealistic to expect district heads to attend regular meetings on health. Besides, the mechanism needed fine-tuning. Similarly the Task Force (TF)s proved essential to the reform process, although TF members were often side-tracked by their routine responsibilities and did not allocate enough time to moving the reform agenda forward. Short term TA proved beneficial in helping the TF focus on key issues and consider alternative policy options. The main constraints to implementation of PHP II were related to delays in and disruptions to the flow of funds, and the informal suspension sanctioned by the World Bank upon confirmation of fraudulent practices within the project at the central level. Implementation of PHP II was severely constrained by delays in the release of funds from the Ministry of Finance. The late release of funds by the Ministry of Finance each year meant that the effective implementation period for PHP II was only 6-7 months per year. For instance, the District Funding Allocation (DFA) component that started in 2004 had an effective implementation period of 23 months during the 3-year period. The informal suspension of the program further disrupted project implementation, exacerbating the effects of delayed financial transfers. Province and central level activities were the most affected, including those of the TRTs and task forces. Direct disbursement of DFAs to districts was not affected. By the time the suspension was lifted, it was too late to implement the proposed activities before the project closed. Inadequate coordination among the TFs reduced their potential impact, particularly with respect to developing a clear and coherent reform framework, although reform areas supported by the project, such as workforce, financing, regulation and information were interrelated. Moreover, there was also limited collaboration between the consultants assisting the TFs with regard to sharing information or comparing notes on reform strategies. By contrast, in Yogyakarta (PHP I), a high degree of collaboration between the TFs and their consultants was a key determinant of the superior implementation performance of this province. Technical coordination and support to provinces from the center were weak. Moreover, the management support from the CPCU at the center was disrupted. The CPCU lost credibility after it was found to engage in fraudulent practices. MOH decided to dissolve the CPCU after it the presence of fraudulent practices was confirmed, and transfer project management responsibility to PHP I CPCU. This decision improved the management performance of the CPCU significantly.

9
Project procurement arrangements were another source of delay in implementations. Difficulties of implementing units, particularly the districts, in following the Bank’s bidding or consultant selection procedures were reported to have impeded performance. Ring-fencing the operation to the level it was designed meant that the Bank’s review processes were extensive, and contributed to delays in procurement.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization Overall, the performance indicators identified in the PAD were broad and did not lend themselves adequately to monitoring progress towards the Project Development Objectives (PDOs). However, it is acknowledged that performance indicators based on health outcomes and health care use alone would have been insufficient to track the progress of a project focused on strengthening institutions and building health systems capacity and the focus on institutional change was appropriate. Monitoring and evaluation of the project, including project baseline, midterm, and final evaluations, and the tracking and special studies related to the reform process, were the responsibility of an independent research unit (RU) hired by MOH. Although the RU was expected to report to the project director, in practice it reported to the CPCU. The absence of a counterpart in MOH that could engage in technical discussions and provide direction limited the effectiveness of the RU. Important studies, such as the tracking study was not conducted while only one special study was conducted quite late in the project. Despite this limitation, the RU developed a series of operational measures for each of the project indicators that formed the basis of the baseline evaluation. However, the RU had a different team leader with differing technical capacity for each of the baseline, midterm and final evaluations. As a result, the three evaluations were not directly comparable, rendering it difficult to systematically assess project impact. Additional studies had to be undertaken to make up for some of these limitations. The final evaluation used both quantitative (using household survey data (Susenas) and qualitative methods to measure the institutional as well as direct, health related objectives of the project. Information was collected retrospectively for different stages of the project.
Safeguard and Fiduciary Compliance
Financial Management Based on the experience of PHP I where the performance of private auditors selected by the project for conducting interim audits was poor, the Bank recommended in October 2004 that the CPCU consider the use of BPKP as an interim auditor for PHP II. However, in March 2005, anonymous information was received by the Bank regarding fraudulent practices in the CPCU of PHP II. The Bank team acted quickly and followed up with MOH on the information. With MOH agreement, the BPK (State Auditing Agency) conducted an investigative audit to confirm the allegation. When the BPK confirmed fraudulent practices within the CPCU the Bank launched a special mission to strengthen financial control of the project and an action plan was agreed upon that was to apply not only to PHP II but also to PHP I and III. The plan was to serve three purposes:

10
(a) send a strong message to all implementing units for deterrence purposes (b) strengthen financial controls with the aim of preventing future mismanagement and
fraudulent practices, and (c) determine whether fraudulent practices were limited to the two categories in question
(workshops/training and incremental costs) and by doing so, determine the full extent of financial losses.
The action plan consisted of the following areas: (a) strengthening of controls by removing financial management and procurement
management responsibilities from the Bureau of Planning to the relevant units in MOH, namely, the Bureau for Financing for financial management and the Bureau of Logistics for procurement
(b) ensuring the integrity of internal controls and capacity to detect problems by recruiting a firm to conduct internal audits of the three PHPs and, at the same time, work with the Inspectorate General’s office to strengthen internal controls within MOH
(c) determining the full extent of ineligible expenditures by expanding investigations to include more samples
(d) appointing BPK to conduct project external audit replacing BPKP (e) withholding payment for PHP II during the transition period until immediate actions
was taken, except for activities under the District Funding Allocation and selected activities at the provincial/central level that were agreed upon by the Bank and MOH.
The Bank also requested reimbursement of the ineligible expenditures under question. MOH, on the other hand, also took action by removing the implicated staff. The Midterm Review of PHP II in January 2006 concluded that while actions were taken and MOH agreed to the action plan, the implementation of some of the actions was slow. The mission rated financial management of the project as highly unsatisfactory. A subsequent mission in November 2006 found that all agreed actions to enhance financial control of the PHPs were already in place, except for the selection of a third party by the Inspectorate General (IG) to assist in conducting an internal audit while building the capacity of the IG staff in conducting audits. At the time the project was closed, this matter still had not been finalized. Thus, while the initial response of MOH to specific fraudulent practices was timely, steps to put in place agreed upon broader financial controls were not taken with the same speed or resolve. Future projects will need to reach agreement upfront on a range of financial management controls that government and the Bank feel are warranted and can be fully implemented. Close attention to the auditing function would be especially critical.

11
One notable side effect of the informal suspension was that the provinces and districts felt they were punished for the actions of others over whom they had no control. Given that critical funds were put on hold, localities complained bitterly to the ICR team they had not been able to implement project activities that they very much wanted to undertake, particularly reform pilots that they had underway. They thought it especially unfair that it was largely the center that caused this situation given their belief that in other important ways the center had not fully supported project implementation. It must also be noted that once the suspension was put in place, project momentum at the center slowed considerably. Little implementation progress, particularly with respect to restructuring of the project as proposed by the Bank, occurred after this. Procurement Procurement, particularly in PHP II, was a further weak aspect of implementation performance. Weak capacity and lack of understanding of World Bank procurement processes, mainly those of the district implementing units, were an issue and contributed to slow project disbursement. The fact that these difficulties were widespread and pervasive raises the question of whether procurement under the project should have taken place at the district level. Given the context of decentralization at the time, districts would likely have strongly resisted having procurement occur at higher levels of government although their capacity to conduct procurement according to Bank guidelines was low as reported by the procurement capacity assessment. Despite the low capacity, the Bank agreed on district level procurement but strengthened control by applying low thresholds for prior review. This decision resulted in a large volume of prior review contracts, and the Bank oversight of these contracts became extremely challenging, particularly as the 3 Provincial Health Project followed the same procurement arrangements. Despite the high workload for Bank procurement staff, the Bank could not change prior review arrangements because Bank post review exercises continued to find some procurement irregularities until the end of project implementation.
Environment The project did not result in any significant environmental impacts.
2.4 Post-Completion Operation/Next Phase At the district and province levels, the project is widely regarded as having laid the foundations for institutional change in a decentralizing environment. Specific examples of how capacity was built to undertake institutional change include: the establishment of JHCs for formulating policy; the proposal preparation process for applying for district funding grants; and, the introduction of new mechanisms to improve public accountability and health promotion through a participatory process involving civil society. In the majority of cases, the districts and provinces were successful in conceptualizing and piloting how these institutions would be established.

12
The extent to which the proposed institutional changes were implemented and sustained depended largely on existing commitment and capacity to implement reforms at the district and province levels. In North Sumatera, the Health Promotion Board was sustained because it was able to leverage local resources. At the end of the project, the JHC in West Java was integrated into the provincial level planning committee and has been expanded to include other sectors. By design, PHP II emphasized the role of the province in assisting the district to gain economies of scale by building cross-district collaboration. Although this strategy seemed incongruent with the goals of decentralization at the time, in hindsight, it is clear that it was an appropriate strategy in the context of decentralization in Indonesia. Two recent laws, Law 32/2004 and PP 38/2007 confer greater power to the provinces, reversing some of the decentralization to the districts in the earlier laws. Evidently, there are economies of scale and scope to be gained in implementing at the province level instead of the district level.
3. Assessment of Outcomes
3.1 Relevance of Objectives, Design and Implementation The project objectives, as appraised, continue to be relevant to current country priorities and overall developmental objectives. The Country Assistance Strategy (CAS) in 2004 stressed that making public sector service delivery more responsive to the needs of the poor is an important vehicle for reducing poverty and vulnerability in Indonesia. The main objective of PHP II was to bring about decentralization in a manner which protected essential health services for the poor. The 2004 CAS further articulated the need for revamping management and accountability systems to make providers more directly accountable to clients, and the need to strengthen local government accountability under a more coherent decentralization framework. Policy reforms envisaged under PHP II such as the JHCs, public accountability mechanisms and health promotion activities that involve civil society are entirely consistent with these CAS goals. The Country Partnership Strategy for 2008-2011 which was being prepared at the time the ICR was written also emphasizes the strengthening of public sector systems including institutional development to strengthen governance. PHP II objectives are also consistent with the Poverty Reduction Strategy Paper (PRSP) published in 2003 that emphasized the importance of social protection, and human capital development and capacity strengthening as critical to addressing the needs of the poor. According to policymakers, PHP II goals became increasingly relevant as decentralization progressed further and awareness about the types of institutional changes it required deepened. There was a consistent comment among district- and province-level policymakers interviewed for this ICR that PHP II became more relevant as the pace of decentralization increased. The project’s emphasis on capacity building and institutional change were instrumental in this regard.

13
PHP II goals were ahead of their time, but they were also based on overly ambitious expectations about the types of institutional change that would be feasible. Many of the reforms proposed at the district and province levels required concomitant reforms at the central level. Delays at the central level limited the ability of provinces and districts to carry out some reforms.
3.2 Achievement of Project Development Objectives The two Project Development Objectives of PHP II were defined broadly, and so were the eight PDO Indicators specified in the PAD. In view of this lack of specificity of the PDO Indicators, this ICR uses the more specific objectives of the two project components and corresponding sub-components in order to arrive at an assessment of the extent to which the two PDOs were achieved. In the sub-sections below we first assess the extent to which the project achieved the first PDO by achieving the objectives of the first component (Component A—Districts and Provinces) and its sub-components; we then assess the extent of achievement of the second PDO by reviewing the achievements in the objectives of the second component (Component B—Center) and its sub-components
(A) Support Effective Decentralization in the Provinces of Banten, North Sumatera and West Java The challenge for PHP II was to initiate key sector reforms and ensure the sustainability of health financing, while protecting health services for the poor during a period of government restructuring. It sought to meet this challenge through a series of reforms whose objectives were to: (i) manage decentralization and, (ii) improve resource mobilization for health through district funding allocations and other means. (i) Managing Decentralization
PHP II initiatives to restructure the organization and management of key health entities early in the project was envisaged as a first step to building the institutional capacity to decentralize effectively. JHCs, TRTs and TFs were established in all three provinces with the objective of formulating policies and strategies, developing new approaches and designing pilots for reforms. The extent to which these objectives were met varied across provinces, due to variations in the level of existing capacity and the flexibility in the design. West Java, that has strong capacity, for instance made most progress in terms of the restructuring, personnel, and financing agenda.

14
The PHP II objective of improving human resource management and development was more difficult to meet because decentralization did not extend authority over personnel policy to the districts. Decentralization provided a good opportunity to improve efficiency and quality of service provision by revising personnel policies and redefining human resource requirements in line with local needs. This would have been possible had districts and provinces been given the authority over civil servants at each level. In the absence of such a policy change, districts had little incentive to review human resource needs and design new policies. This is a good example of the extent to which the design of PHP II was unrealistic about the types of reform that would be feasible. The only exceptions to this were a few districts in West Java, which conducted comprehensive reviews of human resource needs and managed to work within the existing constraints to improve human resource planning and management. Implementing units at all level did use project resources to finance fellowship in various areas and various levels of education (Table 1). This will potentially improve health management and the quality of health services. Table 1: Fellowship Program 2002-2005
Location D3 S1 S2 S3
West Java Province 1069 165 190 4 North Sumatera 326 217 151 28 Banten Province 19 6 10 11 Central level 8 80 119 Total Fellowship 1422 468 470 43
Note: D3: Academy level, S1: Bachelor level, S2: Masters level, S3 Doctorate level Strengthening Health Information Systems (HIS) is key to decentralization because it is a means to ensure that the allocation of resources matches needs. While progress was made in terms of designing blueprints for a HIS, most districts continued to work with the system designed before decentralization. Typically, provinces turned to information technology (IT) consultants for technological solutions instead of attempting to reform the information system itself. Provinces and districts also indicated that they were aware that the center was developing a national HIS and did not want to invest too much in developing a local system. A key concern for the provinces and districts was that a new HIS designed by them would not mesh with the one to be developed by the center.
15
The PHP II objective of upgrading the regulatory framework in the health sector was met only partially and in only a few districts. Decentralization and the consequent reorganization of administrative roles between levels of government provided an opportunity to upgrade the regulatory framework and thus, to improve the quality of service delivery. In particular, the project proposed the introduction of more rigorous competency tests to be administered by independent boards. North Sumatera and West Java visited Yogyakarta early on to learn from the province’s successful experience in conducting the same reform under PHP I. This was followed by reviews of existing licensing and accreditation arrangements. Five districts (4 in West Java and 1 in Banten) unofficially introduced new competency tests. The more substantial reforms to the regulatory framework expected under PHP II did not take place due to uncertainty over the extent to which regulation for licensing and accreditation was under the authority of the central ministry. For instance, there was uncertainty over whether it was premature to introduce competency test at the regional level before the competence standards had been established at the national level. The PHP II objective of strengthening public accountability was partially met. North Sumatera was one of the better performers with respect to this component in that it established an independent board, the Healthy District /City Forum (FKK) to handle complaints about health services in many of the districts. At the time of the final evaluation, the FKK was functioning in 16 of the 25 districts. Other provinces were not as successful. PHP II initiatives to strengthen health promotion were also met with mixed success. A health promotion board, as proposed under PHP II was successfully institutionalized in North Sumatera, and proposals for health promotion activities from non government organizations were accepted for funding. The North Sumatera health promotion board made a strong effort to leverage other resources, which further enhanced the sustainability of this activity. West Java and Banten were much less successful in this regard. (ii) Improving Resource Mobilization through District Funding Allocations and Other means
A basic concern at the time that PHP II was designed was that health services will not be provided with adequate resources post decentralization. Thus, a second PHP II objective was to overcome limitations in the availability of discretionary public funds for health at the district level through (i) block grants known as District Funding Allocations (DFA) and local government counterpart funding and (ii) identification of other options for generating resources. PHP II also included mechanisms to address and enhance the budget planning process and the preparation of district health plans in a manner that better reflected equity issues, epidemiologic needs and local health priorities. There are two parts to whether PHP II achieved its objectives with regard to the DFAs. Did PHP II strengthen capacity for budget planning and management? And did the DFAs lead to an increase in health expenditures at the district level?

16
PHP II was successful in improving districts’ capacity to prepare district health plans that reflect local priorities and needs. The quality of the proposals submitted as part of the health plans improved significantly during the course of the project. In particular, the extent to which the proposals reflect the poverty and epidemiological context of the districts, and local priorities improved considerably. Budget planning and the preparation of the district health plans became the primary responsibility of the districts, thus building capacity in the prioritization process. Nevertheless, performance was variable across districts and was very much influenced by the capacity of the Technical Review Teams (TRTs). In all provinces, the idea to use the JHC forum for fostering scale economies was not successful, although in West Java, the role of the JHC in the distribution of the DFA to the districts was instrumental. Although in practice the JHC gave the final approval of the DFAs, the act was rather administrative rather than a result of careful deliberation of cross district needs and priorities. Budgetary allocations to the health sector did increase during the course of PHP II. The increase in government allocations to the health sector at the district level occurred in part due to increases in overall allocations to the districts. No data are available on the number of districts reaching the target of allocating 15% of their budget to the health sector, the counterpart funding level negotiated as part of PHP II. Policymakers interviewed for this ICR indicated that 15% was too high an allocation for districts. Data on health expenditures were only available for three districts (2 in West Java, 1 in Banten). Per capita spending increased in all three districts. PHP II efforts to identify other sources of financing for health did not progress beyond the assessment of options and design of pilots in some districts. Coverage through other small insurance schemes did increase in Indonesia during PHP II, but it did so in both project and non-project districts. To summarize, the first objective was to support districts and provinces in managing decentralization effectively by restructuring the organization and management of health entities, improving human resource planning, and strengthening institutional capacity. On the whole, achievement with respect to the first objective was moderately unsatisfactory. The second objective was to improve resource mobilization for health, particularly through the DFA mechanism. Achievement with respect to the second objective was moderately satisfactory as it improved planning capacity and was associated with an increase in allocations for and expenditures on health. Based on the above discussion the ICR rating for the achievement of the first PDO is Moderately Unsatisfactory.
(B) Assist MOH in Delineating and Carrying Out Its Roles in a Decentralized Health System The objective is to support MOH in providing the sectoral vision and leadership to successfully undertake decentralization in the health sector. The expected outcomes related to institutional strengthening at the central level.

17
The Decentralization Unit, a key component of central level reforms contributed only in a limited manner to performing the following tasks: coordinate efforts at MOH, clarify the decentralization strategy and develop tools for strengthening decentralization of the health sector. Its most significant contribution was perhaps the formulation of the Obligatory Functions and Minimum Service Standards for Health. It also provided some assistance to the districts in developing district health plans/proposals for funding through the DFA. Progress was hindered because MOH appeared uncommitted to the idea of reforming the Ministry in line with a decentralized system. Moreover, the unit was essentially an ad-hoc unit within MOH with limited experience and leverage to lead the reform process. The PHP II objective of strengthening communicable disease control was not met, and essentially no activity took place under the subcomponent after project midterm review. Failure to meet this goal reflects poorly on the project because of the importance of a strong communicable disease control in a decentralized system, particularly as evidence suggests that disease surveillance system has broken down with decentralization. During implementation, MOH was keen to replicate the system developed under an ADB financed project, mainly in relation to the use of information technology for strengthening surveillance. However, very little was done in terms of assessing the impact of decentralization on surveillance and on building collaboration with the provinces and districts to maintain a functioning surveillance system. Implementation of other interventions was equally limited. Important studies and assessments failed to take place because of lack of follow up on the Bank’s recommendations with respect to the quality of the terms of reference. Although the project allocated several million US Dollars for procurement of equipment to strengthen both the CDC laboratories and the infectious disease hospital, no package was procured because the team in charge of procurement in CDC claimed they did not have the capacity to follow Bank guidelines, exposing them to the risk of misprocurement. By midterm review, only 1% of the amount allocated for this subcomponent had been disbursed. The piloting of the National Health Grants (NHG) mechanism under PHP II achieved good results during its two year implementation. The NHG was designed to assist poorer districts and provide them with incentives to implement MOH priority programs. Districts that requested support from NHG had to show their commitment by indicating the amount of counterpart funding they will contribute to implement the NHG financed activities. Project experience showed there was significant demand from the districts for these grants, more than 20 district proposals were financed under the scheme. During its implementation, the NHG program was managed by the CPCU with little involvement from MOH main units. The scheme however, was discontinued after the project’s mid term review because MOH chose not to adopt the approach despite quite positive response from the districts.
18
The PHP II objective of strengthening food and drug control was achieved partially through staff training and provision of consultants for strengthening particular aspects of the system such as drug inspection. Many National Agency for Drug and Food Control (NADFC) staff were sent for short term as well as long term overseas training. An international consultant was also hired to assist in developing NADFC to become a learning organization. Unfortunately, disagreements between the local and international consultants undermined performance and eventually led to the contract being terminated. Based on the above, the ICR rating for the achievement of the second PDO is Unsatisfactory.
3.3 Efficiency No net present value or rate of economic return was calculated for this ICR since accurate estimates of the impact are not available for such estimation. At the time of preparation, benefit-cost ratios were estimated for the project. The main benefit was to be an improvement in health status (number of life-years saved) that would result from improvements in allocative efficiency in spending, improved access to health services and greater quality of health services. The minimum-benefit scenario needed to justify PHP II investments was estimated as a 2.5% increase in coverage of services. Although data are not available to measure the impact of PHP II on coverage, the decline in health care utilization in the household surveys indicates that PHP II had little or no impact. In short, the minimum-benefit scenario was not achieved.
3.4 Justification of Overall Outcome Rating ICR Rating: Unsatisfactory Project objectives and project design were largely appropriate to the challenges brought upon by decentralization in health, but during implementation it became clear that the design was too ambitious, particularly for large provinces with great heterogeneity in institutional capacity like West Java and North Sumatera. The achievement of the first PDO in all 3 Provinces was moderately unsatisfactory. The provinces discussed and planned a number of key sector reforms, but implementation was limited by both capacity and fiduciary issues and the late release of funds. Achievement of the second PDO is unsatisfactory although achievement of the objective of some component like the Strengthening of Food and Drug Control was moderately satisfactory. The MOH has begun to perform new roles since decentralization, but has for the most part not chosen to do it in ways envisioned by the project. There was little implementation under the Strengthening Communicable Disease Control component.

19
The overall outcome rating for the PDO is Unsatisfactory because many of the project’s objectives were largely not achieved and any progress that was made was not sustained. Moreover, the project did not achieve any significant improvement in health care utilization or outcomes.
3.5 Overarching Themes, Other Outcomes and Impacts (a) Poverty Impacts, Gender Aspects, and Social Development Improving service delivery outcomes for the poor was a major sector-related goal for PHP II. However, the available data from evaluation of the project do not permit careful assessment of the extent to which the project was associated with changes in health care use and health outcomes for the poor. The National Socioeconomic Survey (Susenas), showed increased utilization of public facilities in 2006 compared to 2002 for the poorest and near poor income quintiles in all provinces, except for utilization by the poor in West Java province (Table 2). Similar trends were seen for non-project provinces making it difficult to distinguish the project impact from other, contemporaneous improvements in health care use. Table 2: Utilization of public facilities by the poorest and near poor income quintiles North Sumatera West Java Banten 2002 2006 2002 2006 2002 2006 Poor 24.8% 29.2% 40.9% 38.9 49% 53.5% Near Poor 21.4% 28.3% 37.5% 38.9% 44.3% 49.2%
(b) Institutional Change/Strengthening Institutional reform and strengthening were key components of PHP II. As already discussed in previous sections, PHP II had mixed results. Although actual changes with regard to human resource development, HIS, regulatory framework etc in project provinces were limited, the project was successful in laying the foundations for institutional change and strengthening in the context of a decentralized health sector. Some of the institutional changes initiated under PHP II such as the JHC, TRT and health promotion boards have been sustained albeit with varying success. The JHC has been included in the MOH decentralization strategy document which was released as a ministerial decree. In West Java, the JHC has been integrated into the province level planning committee and has been expanded to include other sectors. In North Sumatera, the Health Promotion Board is sustained and the independent board for public accountability (FKK) continues to function in some districts. There was much less institutional change in Banten, but this is hardly surprising given the project was a late starter in the province, in addition to being hampered by the delays in financing that affected other projects.

20
(c) Other Unintended Outcomes and Impacts (positive or negative) N/A
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops N/A
4. Assessment of Risk to Development Outcome ICR Rating: Substantial District and province level governments’ commitment to institutionalizing the reforms introduced under PHP II is high. There is broad agreement among sub-national level policymakers that, given time and resources to follow through with the reforms, substantial impact on health sector outcomes would have been achieved. However, the following issues pose risks to sustained implementation of these reforms: Financial: Funding for PHP II initiated activities such as JHCs and the health promotion board ended when the project was closed. Meanwhile, delays in the release of funds continue to have a disruptive effect on province and district level activities. Economic: Current, relatively high rates of economic growth have created more fiscal space for investing in the health sector. There is potential for districts wanting to sustain or strengthen reforms initiated under PHP II by lobbying their respective governments for larger allocations. Technical: Follow up investments or government programs need investment in better monitoring and evaluation capacity. Institutional: The establishment of the JHCs was an important initiative to formulate policy across districts and take advantage of province level economics of scale and scope. Although JHCs have been fully integrated into the government process and expanded to include other sectors in one province, it is not clear if they will be sustained in others. Social: Stakeholder support for PHP II has generally been high. In West Java for instance, civil society representatives belonged to the JHC. In North Sumatera, NGOs participated in the health promotion boards. These stakeholders continue to be an important source of support for sustaining PHP II reforms, where possible. Political: Law 32 and PP 38 endorse the PHP vision that the province should have a stronger role in decentralization.

21
5. Assessment of Bank and Borrower Performance
5.1 Bank Performance (a) Bank Performance in Ensuring Quality at Entry ICR Rating: Moderately Satisfactory The Project was a follow on operation to the PHP I which was reviewed by QAG before the Bank agreed to move on to PHP II. QAG rated the QAE for PHP I as “Satisfactory”. As discussed below, the strategic relevance and approach, technical, economic and financial aspects of PHP II were satisfactory. Implementation arrangements were moderately satisfactory and reflected the Bank’s and Borrowers’ assessment of feasibility at appraisal. Bank inputs and processes, assessment of risk and fiduciary aspects were also moderately satisfactory; key shortcomings are described below. The overall rating for Bank Performance in Ensuring Quality at Entry is therefore rated Moderately Satisfactory. Strategic Relevance and Approach
The objectives of PHP II were consistent with country and sector priorities at the time of preparation, and continue to be relevant. The design of the project emphasized improving service delivery for the poor, and attempted to strengthen mechanisms for doing so at the central and local levels. The institutional strengthening approach taken by PHP II was necessary given that the Bank’s underlying goal was to support decentralization in the health sector. The scope of reforms expected in the project was too broad, particularly at the central-level, given the political and institutional context in which they were to be implemented. In such a context, it would have been better to set priorities for what reforms should be undertaken and in what sequence. The technical, economic and financial aspects of PHP II were relatively sound. The project correctly assessed that the institutions and processes which underpinned technical quality would be weakened after decentralization and sought to introduce safeguards. Design elements such as the TRTs, TFs, the components to strengthen communicable disease control and surveillance and an independent monitoring and evaluation outfit are examples of such safeguards.

22
Bank Inputs and Processes
The project was a repeater operation and as such prepared within a 12 month period. It is not clear that more time spent on project preparation would have ensured that provinces and districts were ready for implementation. The level of government involvement in project preparation may not have been as extensive as it could have, in part due to the short preparation period. As is often the case with projects that push the reform envelope, PHP II was designed in close cooperation with the more progressive government counterparts. It is acknowledged that broad-based government support, particularly central government support, would have been difficult to achieve for a strong reform-oriented project such as this. Implementation Arrangements and M&E
The groundwork for many of the key institutional features was laid prior to implementation. The effectiveness of key executive agencies was reviewed during project preparation. Prior to negotiation, TORs for key positions such as the PCIUs, DIUs and CPCU were prepared, and fund channelling mechanisms identified. Given the complexity of the project, the heterogeneity in initial capacity across provinces and considerable needs for technical assistance, the project implementers in the districts and provinces felt that more intensive technical support should have been provided. This applied to both the implementation of the project components as well as procurement and financing arrangements. Clearly, the demands for technical assistance were more significant than anticipated at appraisal. As already discussed, indicators chosen to measure progress towards PDO’s were numerous and most were not amenable to precise and regular measurement and did not reflect the institutional strengthening and capacity building goals of the project. The implementation of M&E was also weak. Assessment of Risk
PHP II correctly identifies relevant risks but could have done more in terms of risk mitigation measures. For instance, the risk of central GOI commitment to decentralization not being sustained is rated as Substantially High. It was expected that the ongoing reorganization and reform within MOH, such as the setting up of the Decentralization Unit, changes in internal structure and skill mix and work culture would foster support and commitment to decentralization. This did not materialize.

23
Fiduciary Aspects
The dilemma for the Bank at the design stage was how to ensure proper procurement oversight in a situation when significant decision-making powers were being turned over to districts. The Bank team did not anticipate at preparation that reducing the threshold for World Bank prior review would result in a high volume of procurement transactions given the large number of districts involved in the project, making Bank oversight of the process challenging in light of finite supervision resources. In retrospect, the Bank could have argued to have control of procurement at a higher level or have different design of procurement methods.
(b) Quality of Supervision ICR Rating: Moderately Unsatisfactory As discussed below, the Bank’s focus on development impact during implementation, and the supervision of fiduciary and safeguard aspects was satisfactory. However, the adequacy of supervision inputs and processes, and the candour and quality of performance reporting was largely unsatisfactory, except towards the end of the project. The Bank’s role in ensuring adequate transition arrangements was minimal. The Quality of Supervision is therefore rated Moderately Unsatisfactory. Focus on Development Impact
Bank supervision of the project remained focused on the development impact of the project, while assessing progress towards institutional strengthening objectives. Progress towards institutional objectives such as the implementation of the district planning process was assessed in terms of their ability to address the needs of the poor. Adequacy of Supervision Inputs and Quality of Performance Ratings
Project supervision missions were carried out regularly and were comprehensive in covering all the many different aspects of the project. Supervision missions also took advantage of the high level of similarity between the three PHPs to do joint supervision. Supervision missions for PHP I and II and later, PHP III were held jointly, which offered several benefits to GOI. It reduced the burden on GOI from having to participate in three separate missions. It enabled GOI to look across the provinces, make comparisons and learn how provinces with different capacity dealt with the same issues or problems. Wrap-up meetings were attended by GOI counterparts from all three projects, which further encouraged sharing of lessons learnt. It also forced the provinces to learn from each other, as they often participated in supervision visits to other provinces. Finally, it was possible to pool supervision resources across three projects and share consultants and experts.

24
A weakness of the Bank was the failure to recognise and respond to two critical constraints to implementation early in the project: first, the scope of reforms was too broad given the scale and heterogeneity of PHP II provinces; second, the complexity of these reforms required closer, more intensive technical support than anticipated at appraisal. Notwithstanding delays in the transfer of funds, addressing these constraints early in the project may have improved the chances of implementation once the flow of funds resumed. A proposal to restructure the project was made at the time of the MTR. While this proposal reflects great insight into sectoral needs at the time, as well as institutional constraints and opportunities, it came too late. The “informal” suspension of the project before the MTR contributed to MOH reluctance to restructure the project. In the case of the DFA, the Bank did recognise the lack of technical capacity at the district level and actively intervened in reviewing the proposals to ensure quality. However, the demands of such intensive technical support posed a heavy burden on the supervision team’s resources, and further delayed implementation. . Another weakness of the Bank was a high propensity to overlook the poor performance by the central government, in an attempt to maintain momentum at the district and province levels. As funding delays virtually drew the project to a halt, it was increasingly apparent that central government agencies were resisting project implementation. The ISR’s noted this problem, but continued to rate the project as Satisfactory1. This rating was justified by the limited progress at the district and province levels, but is questionable given the poor performance at central level. The Aide Memoires do however contain more candid assessments of performance, perhaps because they benefited from the comparison with other PHP’s. However, Bank supervision of PHP II is to be commended for the proactive manner in which it dealt with the allegations of corruption and sought to restructure the project. Supervision during the last two years of the project was characterised by candid assessments of performance, and strong efforts to sustain progress made at the district and province levels. Supervision of Fiduciary and Safeguard Policies
Weaknesses in fiduciary arrangements put in place by the Bank are reflected in the following: (i) protracted procurement process as a lot of time was required to ensure that the procurement documents met Bank requirements and (ii) the finding of irregularities during procurement and financial management post review.
1 For 3.5 years and 11 ISR’s, when disbursements were minimal and the lack of commitment from the central government increasingly apparent, Satisfactory ratings were continuously recorded for both PDO and IP. While the Task Team recognized these constraints, it was also aware that commitment for reforms was high at the district and province levels. The Task Team argued that downgrading the ratings of the project at the time would have undermined the high level of momentum for reform that had been built up at the district and province levels.

25
As indicated earlier, the Bank took prompt action when evidence of fraudulent practices appeared in the project. A high-level mission was mounted to address these concerns and a strong Action Plan agreed upon with GOI to ensure that future such practices would not occur in any of the three PHP projects. In the end, most but not all of the actions of the Plan were put into effect. While the Bank’s response to fraudulent practices was certainly necessary and also appropriate, there is no question that the secondary effects of these actions were substantial. As noted elsewhere, provinces and districts far removed from the corruption that took place at the center felt they paid an unfair price for the mistakes of others. They were eager to get on with pilots and other activities on which they had worked hard up to the point when the evidence of corruption at the center became available. When the informal suspension came into effect, resources for provinces and other forms of support suddenly dried up (except for the DFAs). This raises the question of whether a more nuanced approach on the Bank’s part might have been possible that would not have so discouraged the many local project parties who were not part of the fraudulent practices and whose primary concern was to utilize project resources in order to achieve the project’s objectives.
(c) Justification of Rating for Overall Bank Performance ICR Rating: Moderately Unsatisfactory Bank Performance in Ensuring Quality at Entry was rated Moderately Satisfactory, while Quality of Supervision was rated Moderately Unsatisfactory. Given the Unsatisfactory rating for Outcomes, Overall Bank Performance is rated Moderately Unsatisfactory.
5.2 Borrower Performance (a) Government Performance ICR Rating: Moderately Unsatisfactory Arguably, there was enthusiasm and good support for the project among various government agencies during preparation and appraisal or the Bank presumably would not have proceeded with the project. However, over time this support lessened and took on a different character, particularly with changes in the key personnel responsible for the project in MOH. The obvious turning point was the revelation of fraudulent practices in the CPCU. Once that had occurred, the project’s momentum, which was not strong to begin with, virtually came to an end. Activities in the central component largely stalled. Progress at the province and district was limited as well because the flow of funds and other resources was interrupted.
26
As with PHP I, the overall enabling environment provided by central government had significant shortcomings. Most important among these was lateness of disbursement of DFA funds and confusion over precise allocation of authorities among government levels. This made it very difficult to achieve certain project objectives. The government’s response to the evidence of corruption was initially prompt and strong. It was slow, however, to put in place the complete range of actions agreed upon. There also did not appear to be interest in MOH or other agencies for a concerted effort to turn the project around by embarking on new set of actions and activities. Instead, an easier path was taken, namely to let the remaining time in the project run out while recognizing that the project’s achievements would be quite limited. (b) Implementing Agency or Agencies Performance ICR Rating: Unsatisfactory
Central MOH. Perhaps the most important failing of the project was the fact that MOH took only minimal steps to facilitate the broad health decentralization agenda that the project had articulated in the PAD. Provinces and districts repeatedly told the ICR team that they not only did not feel they were supported by the center but argued that in some cases central MOH actions made it very difficult for them to achieve project objectives locally. Provincial and District Project Entities. Here the picture is more mixed. Some provinces and districts, e.g., West Java, made many efforts to implement project activities in accordance with their understanding of project objectives. In other provinces, commitment and achievements were more mixed. (c) Justification of Rating for Overall Borrower Performance
ICR Rating: Unsatisfactory
Taken all considerations into account, the ICR team reluctantly judges the borrower performance as unsatisfactory. The project simply did not achieve most of its key objectives.
6. Lessons Learned This ICR argues that the Bank had little choice but to respond in a supportive way to the government’s decentralization initiatives, particularly in light of anticipated positive as well as negative consequences in health. The experience of the Provincial Health projects suggests, however, several lessons that emerged from this experience.
27
(a) Providing Bank funding for decentralized activities entails considerable risk to project success in a situation where lower level entities, in this case primarily districts, do not have clear indications of what specific functions they can or cannot undertake, particularly if these functions are not set forth in legislation. Some districts, like Subang in West Java were successful in developing local workforce and financing policies because of the dynamic and resourceful leadership, and the willingness to mobilize required technical assistance either from the province level or from consultants.
(b) Projects will meet difficulties if authority is decentralized without provision of
specific standards for implementing these authorities. One of the major frustrations of provinces and districts was being given authority in the laws for undertaking general functions that could be used to foster reforms but then not having the ability to set standards for ensuring that these functions could be properly performed. Nevertheless, North Sumatera and West Java had some progress in their reform efforts by learning from and adopting some of the reform ideas developed by the Yogyakarta Province, although administrative problems prevented the provinces from achieving more results. This is made possible by the good cross learning environment established between PHP I and II.
(c) A related issue has to do with the fact that where localities have weak capacity to
implement decentralized activities, providing extensive technical guidance and advice is critical. There are a number of modes for supplying such advice—technical expert panels, etc. Provincial and district project participants consistently argued that while they supported the project objectives for health reform neither the central ministry or the Bank supplied enough specific operational guidance on how to achieve the specific reforms advocated by the project, e.g., in the area of restructuring of health organizations or how to increase public accountability. They expressed appreciation for the advice received from the Bank during supervision missions but held the view that this simply was not as extensive and frequent as needed.
(d) In situations of great institutional change and turbulence, reform oriented projects
should set priorities for which reforms should be taken in what sequence. Attempting to implement too wide a scope of reforms at the same time places a large burden on project implementers operating in situations of great uncertainty. If the Bank is also well out in front of the client in terms of the how well the client understands the proposed reforms and how they can be best addressed, the implementation difficulties are only compounded.
7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners (a) Borrower/Implementing Agencies
- A five year project is too short for large system changes envisioned by the project.

28
- Performance indicators were too ambitious and difficult to achieve. It would be better to use proxy indicators. Several indicators, such as those related with personnel reform, were impossible to achieve by the regions in the absence of civil service reform.
- The length of the preparation phase (Phase I) was too short to produce meaningful outputs, particularly when the center and the regions were still struggling to get the project going.
- Implementation of the District Grants is considered as an innovative way to build capacity of the districts in planning and budgeting.
- The role of the JHC was only limited to approval of district proposal rather than the expected larger role of developing province level health policies. Limited involvement of the Bupatis (Head of the District) in JHC assemblies was seen as the main reason for ineffectiveness of the JHC.
- The TRT is considered successful in improving the capacity of districts/cities in developing annual proposals
- North Sumatera has an advantage from the closeness of the University of North Sumatera in Medan. The province also has strong collaboration with NGOs through the Health Promotion Board. West Java’s strength is in its TRT that provided districts with good quality assistance in developing their annual proposals. As a new Province, the capacity of Banten is weak, and Tangerang district is the only district that showed progress during project implementation particularly in development of its health information system
- The output of the CDC component was limited due to problems in complying with World Bank procurement guidelines
- Districts were responsive towards the National Health Grants program but the process for obtaining the grant was too complex
- Advocacy of local government is key for project sustainability in order to build political commitment for more resources for health
- Informal suspension by the Bank of categories 3 and 7 following the confirmation of fraudulent practices at the central level resulted in implementation vacuum at the 3 levels.
- Contradiction between the Bank’s procurement guidelines and the Government’s Keppres 18 was the source of confusion to the implementing units, although the use of procurement plans was considered as a useful tool for monitoring procurement activities. Moreover, procurement activities were often delayed because of delays in developing procurement plans, changes among procurement committee members and their insufficient knowledge of Bank procurement guidelines, weak capacity in TOR development, and lengthy process in obtaining Bank no objection letter ,
29
- World Bank requirements sometimes caused delays in execution of procurement, for example the requirement to conduct a feasibility study prior to construction of a new facility, or requirement to reach consensus on performance indicators prior to buying computers for developing the health information system
- Project Management Reports (PMR) was a useful tool for project monitoring. On the other hand, multiple audit activities were considered too many and time consuming. Moreover, the auditors do not always have the same perception when interpreting Bank regulations.
- Disbursement of project funds was very much influenced by procedures and regulations from MOF that often resulted in delays in budget release.
- It is better to have June 31 rather than December 31 for project closing date to ensure availability of Government funding for conducting activities between the closing date and the closing of accounts.
(b) Cofinanciers N/A (c) Other Partners and Stakeholders N/A
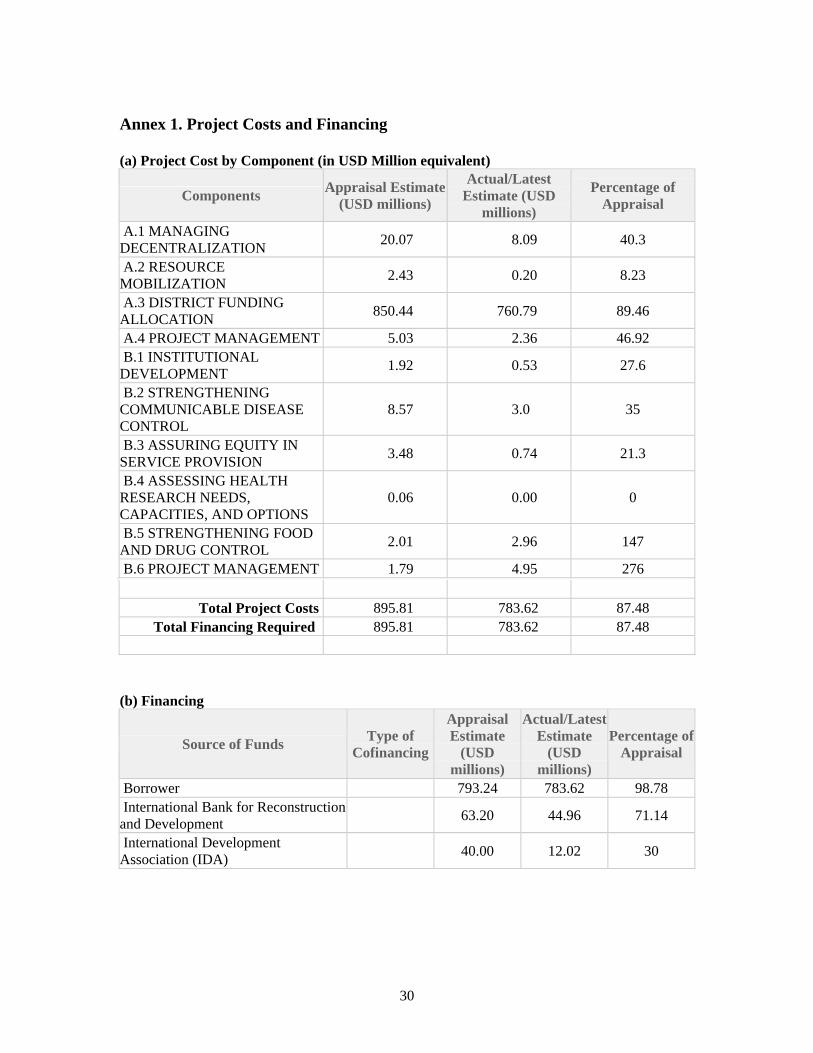
30
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in USD Million equivalent)
Components Appraisal Estimate (USD millions)
Actual/Latest Estimate (USD
millions)
Percentage of Appraisal
A.1 MANAGING DECENTRALIZATION 20.07 8.09 40.3
A.2 RESOURCE MOBILIZATION 2.43 0.20 8.23
A.3 DISTRICT FUNDING ALLOCATION 850.44 760.79 89.46
A.4 PROJECT MANAGEMENT 5.03 2.36 46.92 B.1 INSTITUTIONAL DEVELOPMENT 1.92 0.53 27.6
B.2 STRENGTHENING COMMUNICABLE DISEASE CONTROL
8.57 3.0 35
B.3 ASSURING EQUITY IN SERVICE PROVISION 3.48 0.74 21.3
B.4 ASSESSING HEALTH RESEARCH NEEDS, CAPACITIES, AND OPTIONS
0.06 0.00 0
B.5 STRENGTHENING FOOD AND DRUG CONTROL 2.01 2.96 147
B.6 PROJECT MANAGEMENT 1.79 4.95 276
Total Project Costs 895.81 783.62 87.48
Total Financing Required 895.81 783.62 87.48
(b) Financing
Source of Funds Type of Cofinancing
Appraisal Estimate
(USD millions)
Actual/Latest Estimate
(USD millions)
Percentage of Appraisal
Borrower 793.24 783.62 98.78 International Bank for Reconstruction and Development 63.20 44.96 71.14
International Development Association (IDA) 40.00 12.02 30

31
Annex 2. Outputs by Component Progress on implementation of project components is rated Unsatisfactory because none of the project’s objectives were fully achieved; any progress that was made towards building institutional capacity at the province and district level was rarely sustained. The only exception is the DFA component, where there was some evidence of capacity building. In all other components, the relevant government agencies did not progress beyond conceptualizing the institutional reforms that were required and designing pilots. It is acknowledged that much of the poor performance is related to issues that were beyond the control of the project such as civil service regulations and frequent changes to financial regulations that led to the delayed release of funds. However, these risks were not sufficiently anticipated at preparation and little was done to mitigate them before or during implementation. At the same time, it is recognized that it is beyond the control of the project to intervene in Ministry of Finance decisions. Monitoring and evaluation for the project was extremely weak, making it impossible to measure the impact of the project on either institutional capacity building or on sector related outcomes. The Key Performance Indicators identified at project appraisal (Annex 1 of the PAD) were replaced by a set of more operational measures of performance at implementation. This set of measures was used for the Baseline and Midterm Evaluations. For the Final Evaluation, the measures were modified again. The Final Evaluation collected information retrospectively in order to provide comparable data throughout the course of the project. The measures used to evaluate performance at the Final Evaluation are summarized below against each of the original project development indicators Table 1: Component A – Districts and Provinces Component Original Project
Development Indicator 2002 2004 2006
(1) Managing Decentralization
JHCs, TFs, TRTs established for policy coordination and technical inputs
Not evaluated explicitly. WJ: JHC mechanism functioned effectively and was institutionalized. The JHC reached a consensus on the criteria for distributing DFA resources to participating districts. The TRT was instrumental for developing district planning capacity including by preparing district planning tools. NS: using a JHC task force consisted of non government health experts to communicate the JHC’s views on health direction with the districts. The TRT had significant teething problems because of limited commitment from provincial program staff, but during the second half of the project there was more ownership of the process that improve the quality of interaction with the districts.
Restructuring health organization in the provinces and districts
Development of autonomous health units
WJ: 56% of hospitals became “swadana” (has the authority to retain and use fees), while only Subang

32
district has “swadana” Puskesmas. NS: conducted an assessment in 3 districts on the possibility to convert hospitals and Puskesmas into a “swadana” unit. As a part of the assessment, a consultant conducted ability and willingness to pay survey. Main constraint for achieving this output was getting the endorsement from the parliament and confusion about the future of “swadana” as MOH was in the process of introducing the BLU (General Public Services Entity) concept.
Number of health staff consistent with organization function and workload. Staff career development and quality improvement plan available
NS: At the province level, conducted review of human resource needs in 2004 and 2006, but no new personnel policies implemented. At the district level, none conducted review or introduced new policies WJ: TF on human resources commissioned a review of existing policies at province and district level. PHP II was to be used to move forward the development of new personnel policies, including a trial in 3 districts. Suspension was imposed before implementation began. When suspension was lifted, there was too little time to implement. TF also socialized all districts in the principles of personnel planning. 9 districts carried out review of personnel policy, 1 district (Subang) indicated capacity develop and revise personnel policy to meet changing local needs. B: No review conducted or new policies implemented at the province or district levels.
Effective manpower information system
Not evaluated explicitly. See progress on HIS component below
Reduce non-health staff by 15% or more
All provinces approached this objective by sending non-health staff for further training rather than by introducing downsizing policy. NS: At province level, non-health staff reduced by at least 15%. At district level, no district introduced an explicit policy to reduce non-health staff, or succeeded in reducing by 15% or more. WJ: At province level, non-health staff reduced by 15% or more but health staff also reduced by 17%. At district level, 4 districts experienced a reduction of 15% or more. B: Time series data not available. From 2004 to 2006, % of non-health staff remained unchanged.
Human resource management and development
Upgrade the regulatory framework for licensing and accreditation of health professionals
NS: TF for Regulatory Framework prepared draft proposal for a Quality Council, a competency based mechanism for assessing the quality of health professionals. Project suspended before proposal

33
could be submitted and implemented. WJ: TF for Regulatory Framework proposed an independent board. 3 districts use competency tests, due to initiatives by local chapter of the relevant professional bodies B: Local staff associations of midwives and nurses have advocated competency based testing.
Recording and reporting system for public and private services
Strengthened health information system Data and information for
annual planning
WB requested consensus development among the PHP provinces for developing a province specific HIS. Some workshops were conducted, but they were much influenced by MOH direction for adopting a MOH developed integrated HIS. NS: At province level, conducted review of existing HIS and designed blueprint for HIS. No implementation of province-specific HIS. WJ: TOR for conducting an assessment of HIS current status was approved but was not implemented. A consultant developed an HIS blue print. No implementation of province-specific HIS. B: No review or implementation.
Strengthened public accountability
Public accountability mechanisms: independent boards with accompanying complaints resolution mechanisms
NS and WJ conducted assessment. WJ produced a booklet on public accountability.
NS:14 districts WJ:10 districts B:5 districts
NS:16 districts WJ:15 districts B:5 districts
Health promotion board established
NS: Yes WJ: No B: No
NS: Yes WJ: No B: Yes
NS: Yes WJ: No B: Yes
Strengthened health promotion activities At least 5 health
promotion proposals from NGOs funded each year
NS: No WJ: No B: No
NS: Yes WJ: No B: No
NS: Yes WJ: No B: No
(2) Resource Mobilization
Increase of health per capita spending from local government resources
See (3) on District Funding Allocations below
Percentage of health centers and hospitals as public enterprises/ autonomous units:
See also (1) Managing Decentralization, restructuring organization, the establishment of “swadana” units
% of hospitals NS: 10% WJ: 58% B: -
NS: 8% WJ: 58% B: 0%
NS: 8% WJ: 56% B: 20%
Strengthened mechanisms aimed at sustainable local funding
% of health centers NS: 0% NS: 0% NS: 0%

34
WJ: 5% B: 0%
WJ: 4% B: 0%
WJ: 4% B: 0%
Health financing innovations.
WJ developed a concept for Free Delivery (Jakesiba) program, in which the Government pays for the poor, while non poor provide co-financing. But the pilot was not conducted because there was not enough time.
Percentage of health insurance participants (total insurance coverage among population).
2001 NS: 17.5% WJ: 16.4% B: 20.3%
2003 NS: 18.4% WJ: 17.7% B: 18.0%
2005 NS: 19.0% WJ: 20.2% B: 20.7%
(3) District Funding Allocations
Coverage of priority public health programs Skilled birth delivery.
NS: 81% WJ: 48% B: 52.7%
NS: 81.2% WJ: 55.6% B: 55.5%
NS: 82.7% WJ: 58% B: 59.4%
Contact rate of poor people at health facilities: % of the poorest quintile that used puskesmas.
Utilization of public facilities by the poor Poorest quintile (Q1) 2002: NS: 24.82% WJ: 40.94% Bt: 48.95% Near poor (Q2) 2002: NS: 21.44% WJ: 37.52% Bt: 44.29%
Utilization of public facilities by the poor (Q1) 2006: NS: 29.17% WJ: 38.17% Bt: 53.53% Near poor (Q2) 2006: NS: 28.33% WJ: 38.85% Bt: 49.15%
Table 2: Component B – Centre Component Original Project
Development Indicator 2002 2004 2006
(1) Institutional Development
Strengthened roles and functions of central MOH
Established functional central Decentralization Unit.
DU established DU led the preparation of a decree on decentralization policies and strategies in Jan 2003 and formulation of SPM.
Technical assistance to provinces and districts.
The DU trained a group of MOH staff to become the so called “paratroopers”. They work with provinces and districts based on demand. Some districts use the paratroopers’ services to assist in DFA development.
(2) Strengthening Communicable Disease Control
Disease surveillance and
Establishment of province, district and
Heads of Dinas Kesehatan in project provinces and districts signed an MOU with the DG of CDC to
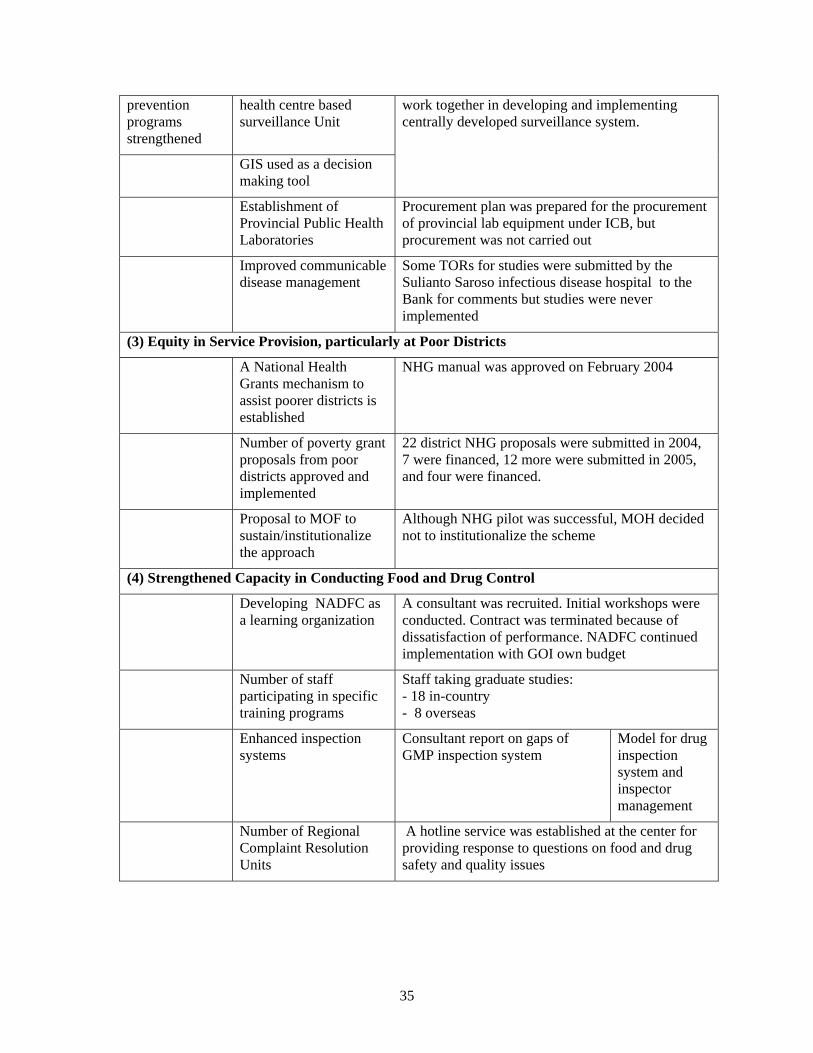
35
prevention programs strengthened
health centre based surveillance Unit
GIS used as a decision making tool
work together in developing and implementing centrally developed surveillance system.
Establishment of Provincial Public Health Laboratories
Procurement plan was prepared for the procurement of provincial lab equipment under ICB, but procurement was not carried out
Improved communicable disease management
Some TORs for studies were submitted by the Sulianto Saroso infectious disease hospital to the Bank for comments but studies were never implemented
(3) Equity in Service Provision, particularly at Poor Districts
A National Health Grants mechanism to assist poorer districts is established
NHG manual was approved on February 2004
Number of poverty grant proposals from poor districts approved and implemented
22 district NHG proposals were submitted in 2004, 7 were financed, 12 more were submitted in 2005, and four were financed.
Proposal to MOF to sustain/institutionalize the approach
Although NHG pilot was successful, MOH decided not to institutionalize the scheme
(4) Strengthened Capacity in Conducting Food and Drug Control
Developing NADFC as a learning organization
A consultant was recruited. Initial workshops were conducted. Contract was terminated because of dissatisfaction of performance. NADFC continued implementation with GOI own budget
Number of staff participating in specific training programs
Staff taking graduate studies: - 18 in-country - 8 overseas
Enhanced inspection systems
Consultant report on gaps of GMP inspection system
Model for drug inspection system and inspector management
Number of Regional Complaint Resolution Units
A hotline service was established at the center for providing response to questions on food and drug safety and quality issues
36
Annex 3. Economic and Financial Analysis Not Applicable
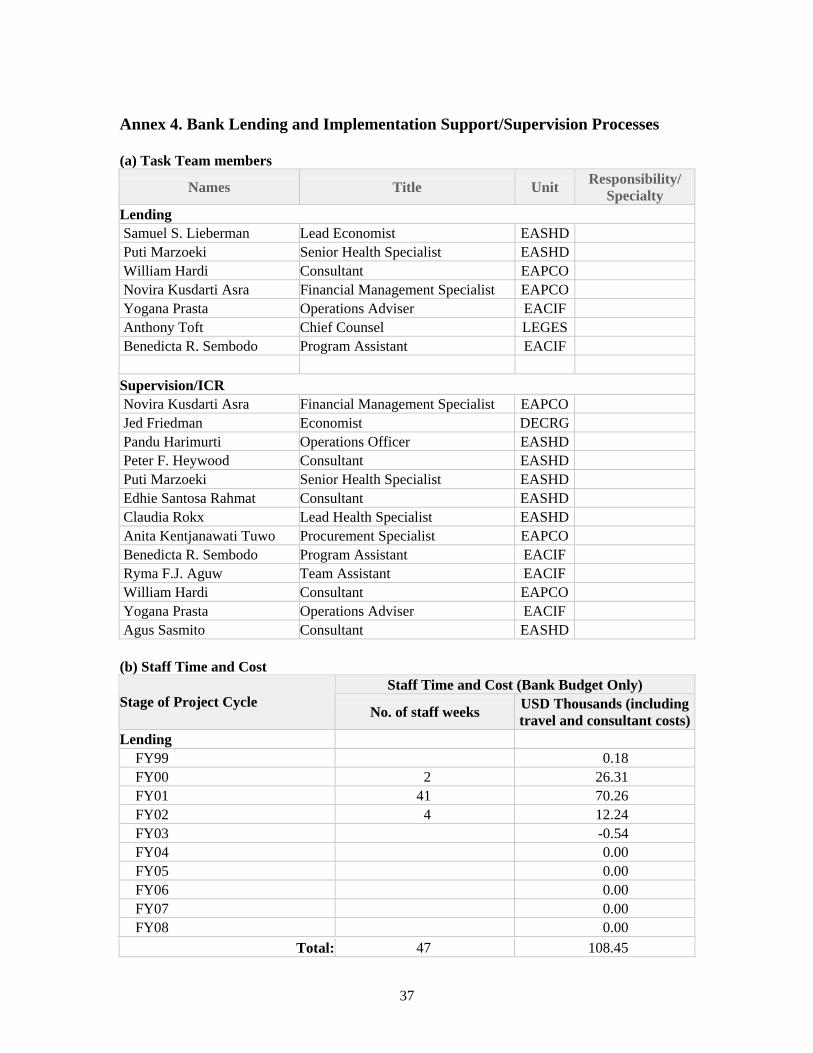
37
Annex 4. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit Responsibility/ Specialty
Lending Samuel S. Lieberman Lead Economist EASHD Puti Marzoeki Senior Health Specialist EASHD William Hardi Consultant EAPCO Novira Kusdarti Asra Financial Management Specialist EAPCO Yogana Prasta Operations Adviser EACIF Anthony Toft Chief Counsel LEGES Benedicta R. Sembodo Program Assistant EACIF
Supervision/ICR Novira Kusdarti Asra Financial Management Specialist EAPCO Jed Friedman Economist DECRG Pandu Harimurti Operations Officer EASHD Peter F. Heywood Consultant EASHD Puti Marzoeki Senior Health Specialist EASHD Edhie Santosa Rahmat Consultant EASHD Claudia Rokx Lead Health Specialist EASHD Anita Kentjanawati Tuwo Procurement Specialist EAPCO Benedicta R. Sembodo Program Assistant EACIF Ryma F.J. Aguw Team Assistant EACIF William Hardi Consultant EAPCO Yogana Prasta Operations Adviser EACIF Agus Sasmito Consultant EASHD
(b) Staff Time and Cost Staff Time and Cost (Bank Budget Only)
Stage of Project Cycle No. of staff weeks USD Thousands (including
travel and consultant costs)Lending
FY99 0.18 FY00 2 26.31 FY01 41 70.26 FY02 4 12.24 FY03 -0.54 FY04 0.00 FY05 0.00 FY06 0.00 FY07 0.00 FY08 0.00
Total: 47 108.45
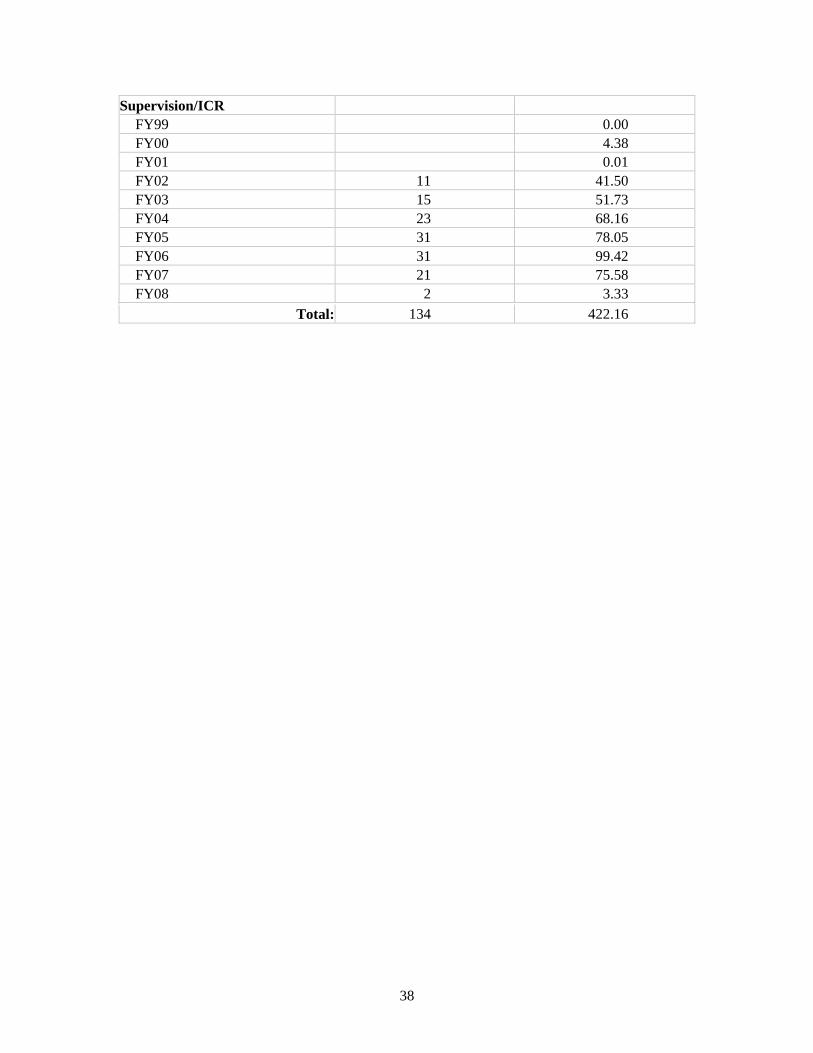
38
Supervision/ICR FY99 0.00 FY00 4.38 FY01 0.01 FY02 11 41.50 FY03 15 51.73 FY04 23 68.16 FY05 31 78.05 FY06 31 99.42 FY07 21 75.58 FY08 2 3.33
Total: 134 422.16

39
Annex 5. Beneficiary Survey Results Not Conducted

40
Annex 6. Stakeholder Workshop Report and Results Not Conducted
41
Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR General Provincial Health Project I (PHP I) is a project implementing decentralization in two provinces and followed up by PHP II. PHP II started on April 2002 and finished at 30 June 2007. PHP II is implemented at: Provinces North Sumatera, Banten, West Java and Central. Generally activities implemented in PHP II are “Health Sector Reform” activities in all aspects.
In following up changes due to the emerging of the new laws, a lot of preparations should be done, among others: institutions, human resource and other resources, and supporting regulations. Usually the above changes are beyond the capacity of the Ministry of Health. This means that we should prepare to overcome potential problems that may appear.
The implementation of PHP I and PHP II is very close, so that no meaningful PHP I experiences could be used as lessons learned for PHP II.
The expansion of new districts and province (Banten) often caused personnel transfer or mutation, limited quantity and quality of personnel, a long process to obtain No Objection Letter from the Bank, the availability of budget always late, all of these influenced the smoothness of implementation of PHP II.
During the life of PHP II, the Bank discovers “fraudulent and corruption practices” at component B6, at the central level. This caused suspension approximately one year for activities in category 3 and category 7. Suspend that applied for central and province has influenced to all project implementation activities. Further, this also influenced the implementation of the District Funding Allocation (=DFA, the amount of DFA is about 65 % of the total loan).
Project Design 1. Similar as PHP I, PHP II is a project developed to change a health system, from a centralistic
character to a decentralistic one. For this change, innovative activities were required in relation with capacity building, planning and health expenditure, improving accessibility and quality of health service delivery, etc. This change needs to be supported by a consistent central policy, which do not often change, including the human resources (tour of duty, tour of area, etc.).
2. A five-year period is too short to realize this relatively big system change. We consider the
Performance Indicators as too ambitious and difficult to be achieved. Proxy-indicators would be better. Besides that, several indicators related to human resource were impossible to be achieved by the region because it was related to “human resource law” as an umbrella law for civil servants.
3. PHP II consists of two phases, Preparation phase (24 April 2002–31 December 2003) and
Operational phase (1 January 2004–30 June 2007). Preparation phase is considered necessary. The 20 months period of preparation phase was considered not enough to yield outputs as planned in the PAD. During the Preparation phase, at the Central level, activities were mostly focused to furnish necessary documents for implementing “foreign loan project” such as:

42
a. Circulation Letter from Directorate General of Budget (released on 23 July 2002), b. Legal Opinion from Department of Justice (released on 12 December 2002), c. Establishment of Implementing Unit such as:
- Decentralization Unit, - Implementing Unit at Directorate General of CDC, - Implementing Unit at Central Research and Development in Health, - Implementing Unit at Food and Drug Control Body (Badan POM)
d. Similar activities occurred at the regions, developing new organizations such as: JHC (Joint Health Council), TRT (Technical Review Team), PHPB (Provincial Health Promotion Board), Task Forces, etc. Task Forces should come up with outputs as planned. However the outputs are developed at the Operational phase, simultaneously with the implementation.
4. Implementation of District Funding Allocation (DFA) is an innovative capacity building in the “comprehensive health planning and budgeting”. Districts and cities develop Plans of Action tailored to their needs in the form of proposals, complete with budget and its source. Districts and cities develop a Master Plan (a five-year period plan) and a one-year plan based on their Master Plan. This prove to enhance personnel’s ability to develop a comprehensive health plan for their districts/cities.
5. The objective of establishing Joint Health Council (JHC) at the province is for dealing with
health issues and development of health policies in the region. We assume that JHC’s members, who are consisted of Bupati/Major, Professional organization, NGOs, cannot function well as it is hoped. JHC only provides proposal approval submitted by the Districts/Cities.
6. The objective of establishing Technical Review Team (TRT) at the province level is for
assisting District/Cities in proposal development and reviewing it. TRT is considered successful in conducting its role, even though at the beginning there are rejections from the Districts/Cities with various reasons such as: inability to keep company, guidance for proposal development was not clear. However as time goes on, the role of TRT was well-accepted by the Districts/Cities. There was a significant capacity improvement of district’s planners.
Project Components There are five components at provincial and three at central level. Those components are considered important to support health sector reform which was really required in the decentralization era (Organization, planning, health information, health financing, regulation, public accountability reforms, etc.).
Component 3: Assuring Equity in Service Provision. Under this component is NHG (National Health Grant), managed by the central level. NHG is an activity where regions are interested. A lot of NHG proposals submitted by the Provinces and Districts/Cities with various topics and innovative. While other subcomponents: Assessing Health Research Needs; Capacities and Options; have no activities at all since the beginning of the project. Output of Project Component a. Output at Province/District/City

43
Decentralization is executed based on Law 22/1999, which was then revised to Law 32/2004. For the implementer, Decentralization is a new issue. This is even more if it is linked to Health Sector Reform. - North Sumatera Province, with its 25 Districts and Cities, is considered having human
resources with better ability. To anticipate the JHC weakness, the Provincial Health Office took initiative by mobilizing retired personnel to facilitate the provinces, appeared to help project implementation running well. University of North Sumatera has experts who assist Provincial/District/City health office for developing decentralization concepts that could be applied. Beside that, the Provincial Health Office also worked together with NGO in developing health promotion activities.
- West Java Province: The human resources capacity at Provincial Health Office is good
enough in developing and implementing the project. The output of TRT at the province level is very supportive to the Districts and Cities in developing proposals. Task Forces also showed similar performance.
- Banten Province: Banten is a new province with many problems such as human resource, in term of quantity and quality; at the province as well as at the districts and cities. Tangerang district showed significant results, among others in developing Health Information System and almost all districts and cities showed good proposals writing for “funding allocation”.
b. Output at Central Level
Organization change from “Ministry of Health and Social Welfare” to “Ministry of Health” brought forth mutation of personnel several times at central level. Time is required for the new personnel to make adjustment and fully understand in managing the project comprehensively. - Component of Strengthening of Communicable Disease Control
Planning for this component was not done well, so that the output was not sufficient. Planning has been done for the development of Sulianti Saroso Hospital as a center of excellence for infectious diseases could not be realized because difficulties in the procurement process. The Bank insisted the need of a consultant to conduct a feasibility study of the advantage of the equipment procured and also the civil work. In fact a procurement officer should be assigned to assist the procurement process. However until the end of the project, this activity was never realized.
- Component of Strengthening Food and Drug Control
PHP II helped seriously the transformation of Directorate General of Food and Drug Control to become a “Professional Unit” in its functions. Various activities related to human resource capacity building such as training of the Inspection system for the inspector/auditor was done. Other training was: Strengthening of Public Accountability, fellowships for S-I and S-II abroad and domestic, technical assistance by consultants, etc.
- National Health Grant (Component 3)
For the purpose of implementing NHG, PHP II has developed guidelines: its objectives, activities that could be supported, its mechanism, reporting and monitoring system that should be followed for NHG activities. Many proposals submitted by the Districts/Cities. However the implementation was not simple. The administrative procedures were complicated and lengthy. Monitoring and evaluation of technical issues is much easier

44
compared to monitoring and evaluation of administrative aspects and finance. (Monitoring and evaluation should be done by the secretariat at central level). Budget that always overdue, influenced NHG implementation. Sometime amendment of the contract between project and regional implementer should be done. .
c. Fellowship There was a clear benefit in capacity building for health personnel at the province/district/city/central through D-III, S-I, S-II and S-III educations. This covered PHP II provinces as well as outside PHP II provinces.
d. Project Sustainability and Key Lessons Learned
- To increase involvement and sense of belonging of the local government (To gain budget
allocation) as well as the central MOH, PHP I and PHP II collaborating with “Center for Management of Health Service” (PMPK), Gajah Mada University, organized a seminar, discussing activities considered as “Best Practices”.
- There should be a continuous advocative approach toward the local government including the local parliament in order to assure political commitment, so that implementation budget will be there.
- After the project ends, to maintain technical competence of the districts and provinces, Ministry of Health must continue to provide technical assistance.
Project Management The establishment of Project Secretariat at the Central level, Province and all Districts/Cities was very helpful in the smoothness of project implementation: - In facilitating all project activities conducted by Technical Unit/Task Force at the Ministry of
Health, Provincial/District/City Health Offices.
- In conducting project administration according to “loan agreement” such as: planning, procurement of goods/consultant, finance and monitoring project. Good coordination and cooperation in the project secretariat is very helpful in the smoothness of the project.
- In managing inter-sectoral financing administration such as with the Ministry of Finance for replenishment and reimbursement of the budget.
At the early 2005, World Bank discovered fraudulent practices at the central level that caused suspension for category 3 and 7 (World Bank’s letter dated 19 May 2005). In response to the suspension, Inspector General conducted investigation, followed by the State Auditor (request of the Bank). Suspension of category 3 and 7 is related to project implementation. Since suspension was also applied to the Province level, practically all project activities could not be conducted at all levels. To prevent the recurrence of similar practices, the World Bank requested Inspectorate General to conduct internal audit all foreign-loan projects that was never be done previously.
45
Comments on the World Bank a. Procurement
- The project is obliged to develop a “Procurement Plan” yearly, which must be approved by the Bank. The plan contains district’s need. The Procurement Plan is very useful as assessment tool for yearly needs and for the monitoring the procurement activities.
• Yearly procurement activities are always late/out of schedule, due to: • Procurement plan developments are behind schedule. • Procurement Committee members change every year. • Insufficient knowledge of the Committee regarding the Bank’s rules.
- The time needed by the Bank to issue the NOL.
- Procurement of Computers to support the Health Information System is far too late in procurement. Procurement was just implemented in 2007. This is because procurement may be done only after the performance indicators are approved by central.
b. Project Management Report (PMR)
During 2002 – 2005, PHP II was not careful enough in developing the Project Management Report (PMR). As a consequence there were differences between un-audited PMR and audited PMR until 2004. The auditor (BPKP) never provided statements regarding these differences in their audit report, with a consequence the project management never made correction of the PMR. So far PHP II management paid no attention to this difference.
As a result of the above, the following issues occurred: - There was difference of 2005 early balance between un-audit PMR and audit PMR as it
was reported by BPK (state auditor) for fiscal year 2005.
- There was a big backlog in the “letter of payment authorization”
- There was a big expenditure in the “bridging account” (State Treasurer). These issues have been overcome by the new management.
c. Audit
- In line with the Loan Agreement, the project audit consists of:
• General Audit by BPKP, conducted each year: March–June • Ex Post Review, each year conducted by different auditors, appointed by the Bank:
April – June • Interim Audit, for district / cities twice yearly March and October. • Technical Audit, the Loan Agreement mention as twice yearly. The project considers
once a year to be sufficient: September–November. - The different audits, going through the same documents, executed at nearly the same
time/period, make it difficult for the implementers.
- Very often they have different perception regarding the Bank’s regulation. The guideline, a reference for the implementation of the project needs to be clear, free from possible mis/multiple perceptions by every component, especially the auditors.

46
d. Performance Indicator
- Time target set in the Performance Indicator is too short, since changing the system (which is the goal of the project) cannot be achieved in such a short time. There should have been a preparation time for the regions, especially the manpower. Implementation time needs to be longer.
- Other indicators not able to be fulfilled by the regions are those contradictory with the existing Law. For example: reducing number of personnel, early retirement, recruitment, etc.
e. Closing Date
We suggest that the closing date of the next projects will not be at 31 December, but 30 June. The reason of this suggestion is because of: the project faces difficulties in conducting activities between closing date and closing account. The activities are among others: to finish up the administration: replenishment, reimbursement, writing final project report, follow up of audit/investigation report. These activities require certain budget. The budget is liquefied after DIPA issuance, and very often DIPA issuance is late.
Comments on the Ministry of Finance Loan disbursement is very much depended upon budget withdrawal. In reality implementation is very often behind the schedule. This is due to: a. Project implementation was behind schedule, due to error of DIPA software (mistake was at
the budget proportion of GOI). Software revision is required and this takes time.
b. The different perception with the KPKN / KPPN managers in Lampung and Jogjakarta in translating the Circular Letter from Directorate General of Budget regarding the implementation of District Grant caused a delay in money withdrawal for Districts/Cities.
c. Transition of the new rule of “Unified Budget” system needs time.
d. The establishment of “travel efficiency budget” policy in the amount of 70 % on August 2007. At the beginning it also applied for “Foreign Loan and Grant” (PHLN). The budget efficiency policy was repealed at the early November 2007, and the dispensation to use the money was approved at the late November 2007.
Comments on the Ministry of Health There was no matching budget available at the beginning of the project. The changes of project management line (which in the beginning under Secretariat General) were moved to “main unit” (Directorate General of Community Health). This influenced budgeting mechanism (Changes of Working Unit/SATKER), and required a long time to settle. Revision process must wait the Regional and Central DIPA compilation. It could not be processed separately. Difficulties in recruiting “Working Unit Staff” and members for the Procurement Committee. Project results, especially best practices, need to be well documented and disseminated so that other provinces can learn.
47
For the 7 years (84 months) working plan, in reality only implemented 54 months (64 %). Conclusion a. Decentralization in the autonomy era is not only delegation of authority or financial
distribution between central and region. Further more, how decentralization could improve services to the community. As a consequence many things should be anticipated, especially technical provider in the field.
b. In reality, the human resource in the provinces and districts are not yet prepared to implement
the programs decentralized by the MOH, so that capacity building is required to achieve the development objectives of PHP I.
c. Managerial skill and good communication are very important to manage a project. d. To obtain local government support after the project closing, political commitment is required
through continuous policy dialogue. e. After the project closes, the local governments are still required to further expand the
technical support from MOH.

48
Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders Not Available

49
Annex 9. List of Supporting Documents Project Appraisal Document Credit/Loan Agreement Implementation Status Reports (ISRs) Aide Memoires Project Baseline, Midterm, and Final Evaluation Reports

Puncak Jaya(5030 m)
Obi
Ceram
Buru
SULAWESISUMATERA
Bali
KALIMANTAN
Raba
Pematangsiantar
Sorong
Timika
FakfakAmahai
PaluJambi
Mataram
BandungSurabaya
Semarang
Palembang
Pekanbaru
Palangkaraya
Bandar Lampung
Serang
IRIAN JAYA(PAPUA)
19
21
22
26
29
20
23
25
24
2827
30
32
31
33
12
11
13
1415
8
67
3
54
2
1
16
17 18
10
9
PAPU
AN
EW G
UIN
EA
A U S T R A L I A
THAILAND
MYANMAR
19
21
22
26
29
20
23
25
24
2827
30
32
31
33
12
11
13
1415
8
67
3
54
2
1
16
17 18
10
9
Balikpapan
Parepare
Baubau
Tarakan
Raba
Ende
Waingapu
Pematangsiantar
Sorong
Merauke
Timika
FakfakAmahai
Palu
Ambon
Gorontalo
Jambi
Medan
Kupang
Padang
Manado
Mataram
Bandung
Kendari
Denpasar
Surabaya
Semarang
Bengkulu
Jayapura
Palembang
SamarindaPontianak
Pekanbaru
Yogyakarta
Banda Aceh
Bandjarmasin
PalangkarayaPangkalpinang
Makassar
Ternate
Bandar Lampung
Serang
Manokwari
Mamuju
Tanjungpinang
JAKARTA
PAPU
AN
EW G
UIN
EA
A U S T R A L I A
SINGAPORE
VIETNAM
THAILAND
MYANMAR
TIMOR-LESTE
BRUNEI
PHILIPPINES
MA L A Y
SI
A
CelebesSea
Java Sea BandaSea
Arafura Sea
SuluSea
PACIFIC OCEAN
I N D I A N O C E A N
IRIAN JAYA(PAPUA)
AruIs.
KaiIs.
TanimbarIs.
Halmahera
Biak
Yapen
Morotai
Misool
Waigeo
Peleng Obi
Muna
Ceram
Buru
SULAWESI Sula Is.
Timor
FloresAlor
WetarMoa
Babar
Sumba
SumbawaLombokJAWA
NatunaBesar
Belitung
Madura
SUMATERABangka
Lingga
Nias
Siberut
Enggano
Simeulue
TalaudIs.
Bali
KALIMANTAN
Men t a w
a i I s .
Puncak Jaya(5030 m)
0°
5°
5°
10°
10°
15°
0°
5°
10°
15°
15°
10°
95° 100° 105°
115° 120° 125°
95° 100° 105° 110° 115° 120° 125°
130° 135° 140°
135° 140°
INDONESIA
NANGGROE ACEH DARUSSALAMSUMATERA UTARARIAUSUMATERA BARATJAMBIBENGKULUSUMATERA SELATANLAMPUNGBANGKA-BELITUNGBANTEND.K.I. JAKARTA
123456789
1011
PROVINCES:
1213141516171819202122
JAWA BARATJAWA TENGAHD.I. YOGYAKARTAJAWA TIMURBALINUSA TENGGARA BARATNUSA TENGGARA TIMURRIAU KEPULAUANKALIMANTAN BARATKALIMANTAN TENGAHKALIMANTAN SELATAN
KALIMANTAN TIMURSULAWESI UTARAGORONTALOSULAWESI TENGAHSULAWESI BARATSULAWESI SELATANSULAWESI TENGGARAMALUKU UTARAMALUKUIRIAN JAYA BARATPAPUA (IRIAN JAYA)
2324252627282930313233
IBRD 36234
JUN
E 2008
INDONESIASECOND PROVINCIAL
HEALTH PROJECTPROJECT PROVINCES
SELECTED CITIES AND TOWNS
PROVINCE CAPITALS
NATIONAL CAPITAL
MAIN ROADS
RAILROADS
PROVINCE BOUNDARIES
INTERNATIONAL BOUNDARIES
This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other information shown on this map do not imply, on the part of The World Bank Group, any judgment on the legal status of any territory, or any endorsement or acceptance of such boundaries.
0 200
0 100 200 300 400 Miles
400 Kilometers


















