Document 5c PRIMARY CARE TRANSFORMATION FUND 2016… Pc co-co - 16 june 2016... · PRIMARY CARE...
72
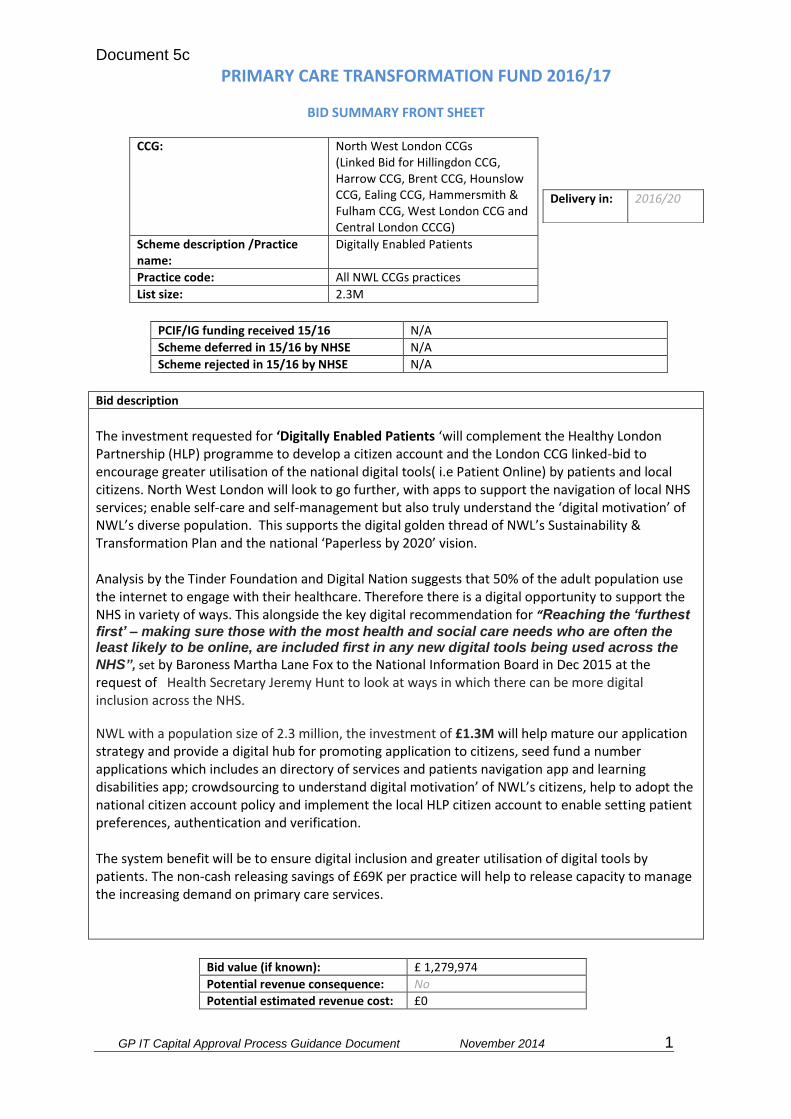
Document 5c GP IT Capital Approval Process Guidance Document November 2014 1 PRIMARY CARE TRANSFORMATION FUND 2016/17 BID SUMMARY FRONT SHEET CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG) Scheme description /Practice name: Digitally Enabled Patients Practice code: All NWL CCGs practices List size: 2.3M PCIF/IG funding received 15/16 N/A Scheme deferred in 15/16 by NHSE N/A Scheme rejected in 15/16 by NHSE N/A Bid description The investment requested for ‘Digitally Enabled Patients ‘will complement the Healthy London Partnership (HLP) programme to develop a citizen account and the London CCG linked-bid to encourage greater utilisation of the national digital tools( i.e Patient Online) by patients and local citizens. North West London will look to go further, with apps to support the navigation of local NHS services; enable self-care and self-management but also truly understand the ‘digital motivation’ of NWL’s diverse population. This supports the digital golden thread of NWL’s Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. Analysis by the Tinder Foundation and Digital Nation suggests that 50% of the adult population use the internet to engage with their healthcare. Therefore there is a digital opportunity to support the NHS in variety of ways. This alongside the key digital recommendation for “Reaching the ‘furthest first’ – making sure those with the most health and social care needs who are often the least likely to be online, are included first in any new digital tools being used across the NHS”, set by Baroness Martha Lane Fox to the National Information Board in Dec 2015 at the request of Health Secretary Jeremy Hunt to look at ways in which there can be more digital inclusion across the NHS. NWL with a population size of 2.3 million, the investment of £1.3M will help mature our application strategy and provide a digital hub for promoting application to citizens, seed fund a number applications which includes an directory of services and patients navigation app and learning disabilities app; crowdsourcing to understand digital motivation’ of NWL’s citizens, help to adopt the national citizen account policy and implement the local HLP citizen account to enable setting patient preferences, authentication and verification. The system benefit will be to ensure digital inclusion and greater utilisation of digital tools by patients. The non-cash releasing savings of £69K per practice will help to release capacity to manage the increasing demand on primary care services. Bid value (if known): £ 1,279,974 Potential revenue consequence: No Potential estimated revenue cost: £0 Delivery in: 2016/20
Transcript of Document 5c PRIMARY CARE TRANSFORMATION FUND 2016… Pc co-co - 16 june 2016... · PRIMARY CARE...
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17
BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name:
Digitally Enabled Patients
Practice code: All NWL CCGs practices
List size: 2.3M
PCIF/IG funding received 15/16 N/A
Scheme deferred in 15/16 by NHSE N/A
Scheme rejected in 15/16 by NHSE N/A
Bid description
The investment requested for ‘Digitally Enabled Patients ‘will complement the Healthy London Partnership (HLP) programme to develop a citizen account and the London CCG linked-bid to encourage greater utilisation of the national digital tools( i.e Patient Online) by patients and local citizens. North West London will look to go further, with apps to support the navigation of local NHS services; enable self-care and self-management but also truly understand the ‘digital motivation’ of NWL’s diverse population. This supports the digital golden thread of NWL’s Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. Analysis by the Tinder Foundation and Digital Nation suggests that 50% of the adult population use the internet to engage with their healthcare. Therefore there is a digital opportunity to support the NHS in variety of ways. This alongside the key digital recommendation for “Reaching the ‘furthest
first’ – making sure those with the most health and social care needs who are often the least likely to be online, are included first in any new digital tools being used across the
NHS”, set by Baroness Martha Lane Fox to the National Information Board in Dec 2015 at the request of Health Secretary Jeremy Hunt to look at ways in which there can be more digital inclusion across the NHS.
NWL with a population size of 2.3 million, the investment of £1.3M will help mature our application strategy and provide a digital hub for promoting application to citizens, seed fund a number applications which includes an directory of services and patients navigation app and learning disabilities app; crowdsourcing to understand digital motivation’ of NWL’s citizens, help to adopt the national citizen account policy and implement the local HLP citizen account to enable setting patient preferences, authentication and verification. The system benefit will be to ensure digital inclusion and greater utilisation of digital tools by patients. The non-cash releasing savings of £69K per practice will help to release capacity to manage the increasing demand on primary care services.
Bid value (if known): £ 1,279,974
Potential revenue consequence: No
Potential estimated revenue cost: £0
Delivery in: 2016/20
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 2
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG √
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √
Demonstrates a process for monitoring, measuring and evaluating expected benefits.
√ Deliverable within financial years April 2016 to March 2019 (the end point for PCTF)
√
Consistent with primary care commissioning plans
√ Evidence of patient involvement and engagement across the local health economy
√
Recommended YES
Priority HIGH
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
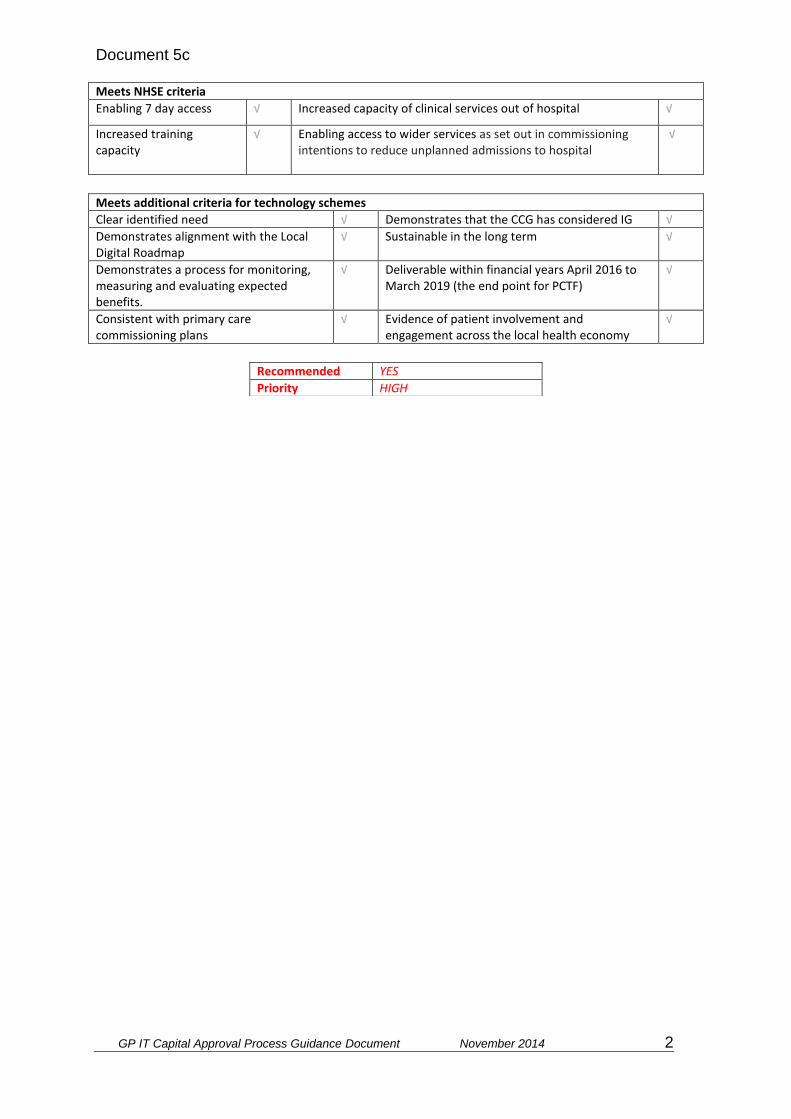
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF. :
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
No
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
No
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. No
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
No
4 This is a bid for capital to provide core technology necessary to support a GP practice move
No
5 This is a bid for capital to provide core technology to a new GP practice No
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME Digitally Enabled Patients
NAME OF THE CCG MAKING THE APPLICATION
Sponsor: Brent CCG a linked bid on behalf of North West London CCGs (Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCG)
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Bill Sturman Director of Informatics, North West London Collaboration of CCGs, Email: [email protected] Sonia Patel Digital Programme Director, North West London Collaboration of CCGs, Email: [email protected]

Document 5c
GP IT Capital Approval Process Guidance Document November 2014 4
John Keating Head of ICT Projects North West London Collaboration of CCGs, Shared ICT Service Email: [email protected] Mobile: 07766 070 628
DELIVERY PARTNER CONTACT DETAILS
North West London Collaboration of CCGs Shared ICT Service Contact details as above.
BRIEF SCHEME DESCRIPTION
Strategic Context and Purpose The investment requested for ‘Digitally Enabled Patients ‘will complement the Healthy London Partnership (HLP) programme to develop a citizen account and the London CCG linked-bid to encourage greater utilisation of the national digital tools( i.e Patient Online) by patients and local citizens. North West London will look to go further, with apps to support the navigation of local NHS services; enable self-care and self-management but also truly understand the ‘digital motivation’ of NWL’s diverse population. This supports the digital golden thread of NWL’s Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. Analysis by the Tinder Foundation and Digital Nation suggests that 50% of the adult population use the internet to engage with their healthcare. Therefore there is a digital opportunity to support the NHS in variety of ways. This alongside the key digital recommendation for “Reaching the ‘furthest first’ – making sure those with the most health and social care needs who are often the least likely to be online, are included first in any new digital tools being used across the NHS”, set by Baroness Martha Lane Fox to the National Information Board in Dec 2015 at the request of Health Secretary Jeremy Hunt to look at ways in which there can be more digital inclusion across the NHS. The CCGs within NW London have identified the need to increase digital inclusion of NWL citizens to better use of day to day technology already at their disposal to access local healthcare services, by:
1. Increasing the awareness and utilisation of online appointment booking, online repeat prescription ordering and online access to records through Patient Online and also the North West London Care Information Exchange.
It would also like to actively support:
2. Enabling patients to navigate through the NHS healthcare system through the use of informative and innovative mobile apps.
3. Enable targeting of health promotion information and campaigns through
mobile technology. All of the above underpinned by a coherent strategy for Digital Empowerment driven by citizens and patients needs. The three core objectives of the ‘Digital Empowerment’ strategy will be to:
1. Digital inclusion supporting better use of existing tools 2. Digital inclusion to support Navigation and Access to Services 3. Digital inclusion to support Self-Care and Self-Management
Objective 1: Digital inclusion supporting better use of existing tools

Document 5c
GP IT Capital Approval Process Guidance Document November 2014 5
With 66% of the adult population in the UK personally own/use a smartphone and 61% use their mobile phone to access the Internet
1 this holds a significant digital opportunity,
however the majority of patients still book appointments via the telephone and in person, with only 6.4% of patients reporting to book appointments online and 2.4% aware they can access their GP record online
2. As identified by the NHS Digital Technology Strategy
technology has the ‘power to change the relationship between patients and their GP, just as it has changed our relationship on other walks of life, such as managing our finances or shopping’
3. NWL will work the London Digital Programme to take advantage and make best
use of the resources that may be available to encourage greater utilisation of Patient Online (this bid excludes any investment for Patient Online) but an important component of NWL strategy. Alongside the national tools, in North West London the Care Information Exchange (CIE) is being launched to help enable integrated care and to increase patient engagement in the management of their health. The CIE will be accessible to patients, service users, and health and care professionals via the internet. It will draw together near real-time information such as upcoming appointments, hospital attendances, pathology and radiology results and correspondence from different health and social care organisations across North West London. The individual will control who can see certain parts of the record and will be able to add to the record themselves with information such as symptoms and outcomes. We now need to harness the full potential for the benefit of citizens and staff. This investment requested will support the engagement arm in primary care to encourage take-up. Objective 2: Digital inclusion to support Navigation and Access to Services Some of our local areas have started exploring with their patient groups ways in which to improve access to services and reduce unnecessary demand on services and pressure on front-line staff. This has generated into the following pilot project for a patient-facing app. Pilot One - Directory of Services and Patient Navigation app: A smart app to help citizens and local primary care services through effective information and service signposting to reduce demand on 111, A&E and other acute services and associated waiting times and promotion of Out of Hospital services reduces pressure on frontline services. Giving people access to the most appropriate service, instead of just booking a GP appointment by default thus cuts unnecessary GP appointment and reducing potential DNAs. The technology allows sharing of information, data and communications over a range of media platforms. It could provides a single portal / one stop shop that allows residents to access a range of health information and services. The app also has the multi-functional potential for patients, practice staff, expert patients, volunteers, third sector and more Objective 3: Digital inclusion to support Self-Care and Self-Management
1 Figures taken from Q1 2015, OFCOM, http://media.ofcom.org.uk/files/2015/facts-figures-table15.pdf
2 GP Patient Survey 2014-15, NHS England, https://www.england.nhs.uk/statistics/2015/07/02/gp-patient-
survey-2014-15/ 3 NHS England, https://www.england.nhs.uk/ourwork/pe/patient-online/

Document 5c
GP IT Capital Approval Process Guidance Document November 2014 6
There is strong evidence that increasing people’s knowledge about their condition, how to self-care (including improving diet, physical activity and symptom control), and when to use health services appropriately, will significantly save the NHS time and money. Interventions, which integrate several technologies such as online education, mobile phones and telemedicine, have shown the most potential for improving self-management. The lack of informed patients can experience unnecessary levels of preventable ill health suffer for longer than they need to, sometimes increasing distress by having to repeat their story more than once and perpetuate the time needed by care professionals when treating their condition. Therefore information technology plays an essential and rapidly expanding role in providing information between professionals involved in an individual’s care and empowering people to actively take charge of their own health, encouraging self-management and collaboration building trust in an open and transparent way and building trust ensuring citizens increase in confidence about sharing their data to improve care and health outcomes. Some of our local areas have started exploring with their patient groups ways in which to improve access to support self-care through digital empowerment. This has generated a second pilot project for a patient-facing app for patient’s learning disabilities this genuinely stretches the ambition to support true digital inclusion. Pilot Two:
The Learning Difficulties App will digitalise Health Action Plans and make these available to patients via a mobile app. This will prevent current issues created by loss of paper. It can be tailored to other priorities such as self-care and self-management of long-term conditions. The technology allows sharing of information, data and communications over a range of media platforms. Approach & Deliverables
NWL with a population size of 2.3 million, the investment of £1.3M will help mature our application strategy and provide a digital hub for promoting application to citizens, seed fund a number applications which includes an urgent care service app and learning disabilities app; crowdsourcing to understand digital motivation’ of NWL’s citizens, help to adopt the national citizen account policy and implement the local HLP citizen account to enable setting patient preferences, authentication and verification. The three core-deliverables of the funding will: Deliverable 1: Digital Empowerment Strategy Develop a collaborative strategy with patients for ‘Digital Empowerment’ that harness local innovation, development and delivery of patient online and mobile services informed by
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 7
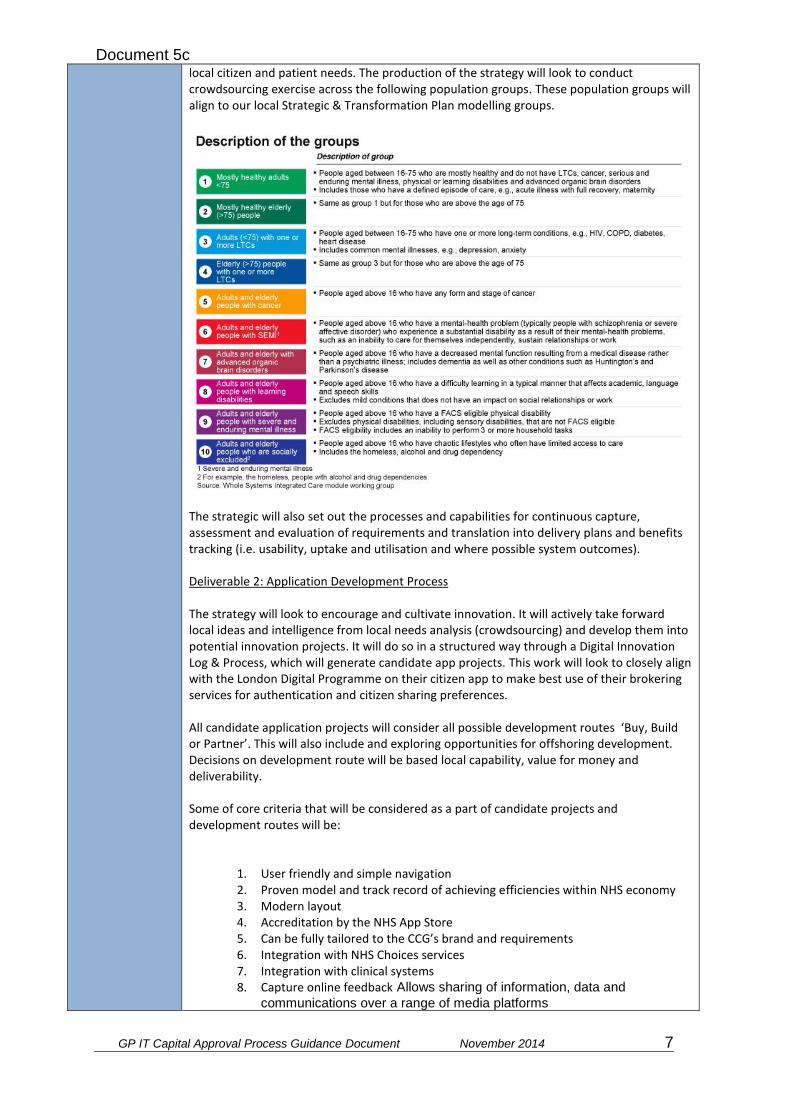
local citizen and patient needs. The production of the strategy will look to conduct crowdsourcing exercise across the following population groups. These population groups will align to our local Strategic & Transformation Plan modelling groups.
The strategic will also set out the processes and capabilities for continuous capture, assessment and evaluation of requirements and translation into delivery plans and benefits tracking (i.e. usability, uptake and utilisation and where possible system outcomes).
Deliverable 2: Application Development Process The strategy will look to encourage and cultivate innovation. It will actively take forward local ideas and intelligence from local needs analysis (crowdsourcing) and develop them into potential innovation projects. It will do so in a structured way through a Digital Innovation Log & Process, which will generate candidate app projects. This work will look to closely align with the London Digital Programme on their citizen app to make best use of their brokering services for authentication and citizen sharing preferences. All candidate application projects will consider all possible development routes ‘Buy, Build or Partner’. This will also include and exploring opportunities for offshoring development. Decisions on development route will be based local capability, value for money and deliverability. Some of core criteria that will be considered as a part of candidate projects and development routes will be:
1. User friendly and simple navigation 2. Proven model and track record of achieving efficiencies within NHS economy 3. Modern layout 4. Accreditation by the NHS App Store 5. Can be fully tailored to the CCG’s brand and requirements 6. Integration with NHS Choices services 7. Integration with clinical systems 8. Capture online feedback Allows sharing of information, data and
communications over a range of media platforms

Document 5c
GP IT Capital Approval Process Guidance Document November 2014 8
The intention is this strategy will mature over time and allow NWL through its digital hub to promote tools for its citizens and patients. Deliverable 3: Seed the fund the following Delivery of Mobile App pilots The following pilots have been generated through the draft Digital Innovation Log & Process proposed as a part of Deliverable 2: Pilot 1: Directory of Services and Patient Navigation The app will deliver functions for public and patients this will include a symptom checker; directory of local NHS services (including hours of service, distance from device and maps), journey planner, news feed (with push notifications), capture user feedback, provide a Health Wallet (to save useful contacts, appointment dates, notes). Pilot 2: Learning Disabilities The Learning Difficulties App will digitalise Health Action Plans and make these available to patients via a mobile app. This will prevent current issues created by loss of paper. It can be tailored to other priorities such as self-care and self-management of long-term conditions. Investment breakdown and resourcing
Outcomes and Benefits:
System the benefits that are envisaged from a Digital Empowerment and
structured approach to digital innovation and apps:
1. Health and Wellbeing: Promotes health and wellbeing using push notification to
mobile phones for advice and targeting health promotion and other campaigns, effective information and service signposting, removing the need for a GP appointment, and thereby freeing up time for other patients with more serious complaints
2. Managing Demand on Primary Care Service: Through online accessibility
to Primary Care enabling contact-free GP appointment booking and cancellation and online repeat prescriptions ordering
3. Scalability and sharing with London Community 4. Potential to expand to pan London and beyond and potential to develop
additional functionality and realise additional benefits through a structured
Project DigitallyEnabledPatients
SumofTotalincVAT ColumnLabels
RowLabels 16-17 17-18 18-19 19-20 GrandTotal
One-off £530,088 £518,121 £178,253 £183,601 £1,410,064
(P40)BusinessAnalyst £90,000 £90,000
(P40)BusinessAnalyst(band7)-inclaccommodationcharges,trainingandexpenses £68,110 £70,153 £72,258 £210,520
(P41)DigitalComms&EngagmentLead £90,000 £30,900 £120,900
(P41)DigitalProjectManager £101,250 £34,763 £136,013
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
Clinican(2dayspermonth) £16,200 £22,248 £22,915 £23,603 £84,966
Communicationmaterial £12,000 £12,000
Crowdsourcingactivities £36,000 £36,000
Developmentdays(inctestandreleasemgmt) £24,000 £49,440 £50,923 £52,451 £176,814
Eventsandlearningsessions £36,000 £36,000
Hosting,contentandsupport £24,000 £24,720 £25,462 £74,182
IG/LegalFees £36,000 £37,080 £73,080
LearningDisabilityAppsetupandimplementation £27,000 £27,000
OfficeServices £6,750 £2,318 £9,068
PMcosts(hardwareandsoftwaretools) £4,320 £4,320
Setupofmobileapp,websiteandcontent £240,000 £240,000
Supportandmaintenance £4,497 £9,264 £9,542 £9,828 £33,131
GrandTotal £530,088 £518,121 £178,253 £183,601 £1,410,064
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 9
approach. Some specific benefits from the pilot App projects are:
The benefits of the app are identified as: 1. Potential efficiencies
a. Reduction in demand on 111, A&E and other acute services and associated waiting times and promotion of Out of Hospital services
b. Reduces pressure on frontline services c. Giving people access to the most appropriate service, instead of just
booking a GP appointment by default d. Cuts unnecessary GP appointments e. Reduced DNAs
2. Accessibility
a. Start exploring how to digitally engage hard to reach groups. b. Provides a single portal / one stop shop that allows residents to access a
range of health information and services c. Fits patient lifestyles and digital demands d. Multi-functional tool for patients, practice staff, expert patients,
volunteers, third sector and more

Document 5c
GP IT Capital Approval Process Guidance Document November 2014 10
NON-RECCURNT INVESTEMENT (including VAT)
15/16 16/17 17/18 18/19 19/20 Total Total Capital Cost: £xk £xk £xk £xk £xk £xk
NON-CASH RELEASING SAVINGS
Net revenue impact (by financial year) 15/16 16/17 17/18 18/19 19/20 Total Net Revenue Impact £xk £xk £xk £xk £xk £xk Please provide details of the revenue/quality benefit in sufficient detail to support the calculation of the return on investment for the project.
PRIORITISATION OF PROJECTS
If submitting a number of projects for capital funding (via additional
PIDs), please state the priority of this project:
1. HIGH
PROPOSED PROCUREMENT STRATEGY
This scheme will be delivered within 16/20. The procurement process will start once NHS England approves the funding. Procurement will follow Brent’s Standard Financial Instructions and NHS procurement rules.
KEY RISKS
There is a risk: patients will not be engaged in the project The consequence would be: low uptake and utilisation of online services and apps This will be mitigated by: patient and public engagement strategy will be pivotal to the project. There will be patient and public involvement in the development of the online strategy. Existing and new communication channels can be used to promote the online and app services, such as tailoring message to GP health promotion screens. Lessons Learnt and recommendations from similar projects will be incorporated into the planning.
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 11
Organisation
Date
APPROVED BY: Head of Financial Management NHSE (London Region)
Document 5c
GP IT Capital Approval Process Guidance Document November 2014 12
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17 BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name:
Integrated Care Planning – Technical Standards
Practice code: All NWL CCGs practices
List size: 2.3M
Building condition: Technology Bid
Bid description
The investment requested for ‘Integrated Care Planning – Technical Standards ‘will complement the Healthy London Partnership programme to develop a standards based information exchange architecture to support patients and local citizens. North West London as a pioneer for Health & Social Care integration is committed to mobilising patient-centred, multidisciplinary and proactive care. NWLs experiences of over the last five years with developing integrated care model evidences that care planning is contingent on shared information. Significant expertise has been invested to-date to develop local care-planning tools for GPs. The shortcoming of the tools is the difficulty to share critical care-planning information further than the GP IT system. This genuinely hinders the ability to share with acute consultants and social care professionals. This has been due to the lack of universally accepted technical standards that can be adopted by IT system suppliers. North West London’s clinical and professional leadership propose to be an accelerator site and work with national delivery partners (PSRB, NHSE and HSCIC) to develop a professionally accepted technically standard. This will enable the next stage of digital maturity for Integrated Care planning. This investment will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. This investment of £328K will commission the PSRB; provide clinical and professional expertise; support local engagement with patients and professionals and on-board integration specialist to test and implement the standards locally. The system benefit is a PSRB endorsed technical standard for Integrated Care Planning that would help nationally other NHS organisations, pioneers and vanguards.
Bid value (if known): £328,071
Potential revenue consequence:
No
Potential estimated revenue cost:
£0
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG
√
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √
Demonstrates a process for √ Deliverable within financial years April 2016 √
cotchr
Typewritten Text
Document 5d

GP IT Capital Approval Process Guidance Document November 2014 2
monitoring, measuring and evaluating expected benefits.
to March 2019 (the end point for PCTF)
Consistent with primary care commissioning plans
√ Evidence of patient involvement and engagement across the local health economy
√
Recommended YES
Priority HIGH
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF. :
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
No
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
No
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. No
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
No
4 This is a bid for capital to provide core technology necessary to support a GP practice move
No
5 This is a bid for capital to provide core technology to a new GP practice No
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME
Integrated Care Planning (Development and Implementation of Technical Standards)
NAME OF THE CCG MAKING THE APPLICATION
Co-Sponsor: Brent CCG a linked bid on behalf of North West London CCGs (Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCG) Co-Sponsor: Mike Part, Head of Technology, (NHS England London Region) [email protected]
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Bill Sturman Director of Informatics, North West London Collaboration of CCGs,
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 4
Email: [email protected] Sonia Patel Digital Programme Director, North West London Collaboration of CCGs, Email: [email protected] John Keating Head of ICT Projects North West London Collaboration of CCGs, Shared ICT Service Email: [email protected] Mobile: 07766 070 628
DELIVERY PARTNER CONTACT DETAILS
If relevant, please provide details of the technology delivery partner contact Munish Jokhani, clinical engagement lead transfers of care, HSCIC [email protected] Jan Hoogerwerf, Programme Manager: Health Informatics Unit, Royal College of Physicians, PRSB (Professional records Standards Body)
[email protected] John Kelly, Head of Systems Solutions, Imperial College Healthcare NHS Trust [email protected] Mike Part, Head of technology, NHS England London Region) [email protected] Mohammad Al-Ubaydli, Patient Knows Best [email protected] Nilesh Bharakhada, GP Lead Hillingdon Integrated Care Plan, [email protected] EMIS Tony Willis, GP IT Lead, Hammersmith & Fulham GP [email protected] TPP
BRIEF SCHEME DESCRIPTION
Strategic Context and Purpose
The investment requested for ‘Integrated Care Planning – Technical Standards ‘will complement the Healthy London Partnership programme to develop a standards based information exchange architecture to support patients and local citizens. North West London as a pioneer for Health & Social Care integration is committed to mobilising patient-centred, multidisciplinary and proactive care. NWLs experiences of over the last five years with developing integrated care model evidences that care planning is contingent on shared information. Significant expertise has been invested to-date to develop local care-planning tools for GPs. The shortcoming of the tools is the difficulty to share critical care-planning information further than the GP IT system. This genuinely hinders the ability to share with acute consultants and social care professionals. This has been due to the lack of universally accepted technical standards that can be adopted by IT system suppliers. North West London’s clinical and professional leadership propose to be an accelerator site and work with national delivery partners (PSRB, NHSE and HSCIC) to develop a professionally accepted technically standard. This will enable the next stage of digital maturity for Integrated Care planning. This investment will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. NWL’s strategic vision to deliver integrated joined up care for its citizens is contingent on the ability of care professionals to share information across care setting a) to enable new models of care and b) further development of multi-disciplinary teams. The investment sought shall co-develop and implement the technical standards to support shared integrated care plan. The summary of work will include understanding the care-planning user-cases for care professionals and service-users to support new care models this will include building on the work already done in NWL. In alliance
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 5
with NHS Digitals Information Standards work programme determine the technical and data requirements thus identifying the data and coding standard to create information standards for integrated care planning that specifies rules for the collection, processing, management and sharing of information to support patient care. Look to work closely with the IT system suppliers system suppliers to adopt universal technical standards to support sharing between care professionals and their patients; and advance NWL’s interoperability plans. This will also require a parallel work stream on data quality which form a part of NWL’s existing Data Quality Forum and framework. Integrated care in North West London (NWL) started in 2011 with the initiation of 2 ‘integrated Care Pilots’, in Outer NWL (Brent Harrow and Hillingdon) and Inner NWL (Central London, West London, Hounslow, Hammersmith & Fulham and Ealing), by 2012 this evolved into 4 pathways focusing on a separate population groups. Building on the success of these care pilots, the ambitious and pioneering programme Whole Systems Integrated Care (WSIC) was launched in 2013 with commitment of 31 health and social care organisations across NWL. The programme continued to focus on person-centred integrated care for NWL citizens. But considering and actively addressing the practical issues to delivering integrated care at pace and scale. This included the significant changes in the way individuals receive care in their homes and communities, and encouraging health and social care professionals to work together daily in a seamless integrated way, further supported by the continual development of new models of care, increasing the ability for care professionals to work together and improve outcomes for patients and service users in NWL by providing a more centralised personal service based on their individual needs. Phase one of the WSIC Programme co-developed a virtual toolkit (http://integration.healthiernorthwestlondon.nhs.uk/chapters) that published online NWL’s latest thinking and a series of tools to support elements of health and social integrated care and the establishment of Accountable Care Partnerships (ACPs). A core strand of the toolkit was informatics as information and the appropriate information systems were seen as crucial to inform and support decision-making and the delivery of care; sharing informed care plans between professionals, across organisational boundaries and their systems and empowering service users to self-manage supported by their care information. This work identified the following user-cases for care planning. User-cases for Service Users The work as a part of the WSIC integration toolkit identified that service-users wish to be empowered to maintain independence and to lead full lives as active participants in their communities. Changing the traditional way patients and service users’ behaviours and activities carried out by themselves, promoting the development of self-care and self-management and also how professionals support care decisions and work together towards personal care goals. Service users will need information to help them understand their progress, their options and where they can get advice.
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 6
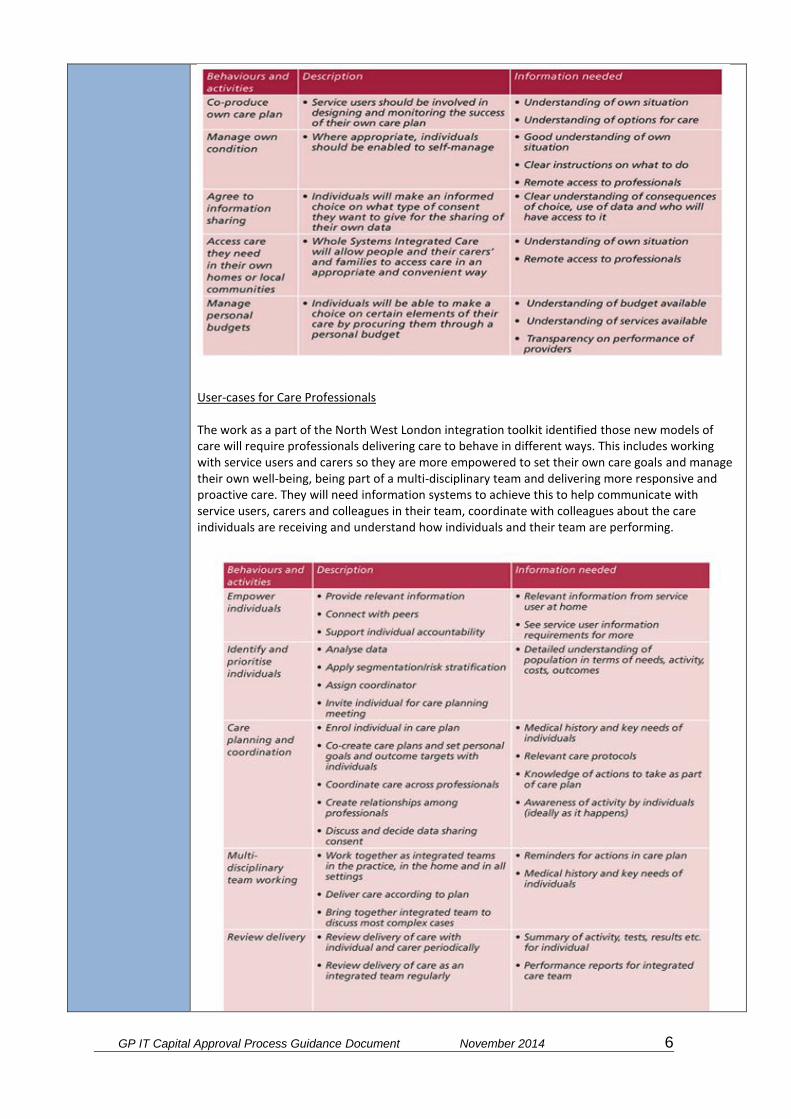
User-cases for Care Professionals The work as a part of the North West London integration toolkit identified those new models of care will require professionals delivering care to behave in different ways. This includes working with service users and carers so they are more empowered to set their own care goals and manage their own well-being, being part of a multi-disciplinary team and delivering more responsive and proactive care. They will need information systems to achieve this to help communicate with service users, carers and colleagues in their team, coordinate with colleagues about the care individuals are receiving and understand how individuals and their team are performing.
cotchr
Typewritten Text
Document 5d

GP IT Capital Approval Process Guidance Document November 2014 7
Syndication of Care-Planning User-Cases Further syndication of the user-cases was conducted as a part of a NWL-wide care planning principles and processes event on the 3
rd June 2015. This included attendance from a wide range of
care professionals and lay partners (patients) across the eight CCGs who are actively involved with their local models of care. The aim was to bring together integration experts to build on their experience and learning to develop a NWL owned shared set of standards to support the local development of early adopters' care planning. At the event a single patient viewable care plan was discussed and a vision for what a universal care plan should contain as a minimum. Patients and care professionals co-produced the agreed minimum principles and processes;
Contact information of services users’ human connections.
Diagnosis and medication.
Clear, achievable, and measurable goals, which are meaningful to the service user and owned by named people, e.g. I can walk to the shops three times a week.
Crisis plan understood by service user.
Agreed review dates.
Supporting information e.g. Carer role (formal and informal), recently bereaved
Regional and National Context In early in 2015 NHS England (London region) and London’s 32 Clinical Commissioning Groups (CCGs) launched the Healthier London Partnership (HLP) with a vision to make London the world’s healthiest global city. Part of this vision for a healthier London was the development of an standards based interoperable infrastructure that federates 32 CCG areas and their respective health and social care systems as a part of the London Health & Care Exchange (LHCE). NWL has agreed to be an accelerator site for the LHCE and will work in partnership locally and regionally organisations to establish a technical Integrated Care Planning standard, which could benefit upto 9 million citizens across London. Further enhancing the delivery of patient centred care. In February 2016, NHS England also released the ‘NHS Shared Planning Guidance’ which asked every health and care system to come together to create their own ambitious local blueprint for accelerating implementation of the Five Year Forward View. Sustainability and Transformation Plans (STPs) and the enamelling Digital Roadmaps to create multi-year, multi-organisational plans, built around the needs of local populations and their supporting health and social care organisations are being placed at the heart of the drive to create innovation and bring about a paperless, digitally engaged NHS by 2020, a goal set by the UK Digital Champion, Baroness Martha Lane Fox in
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 8
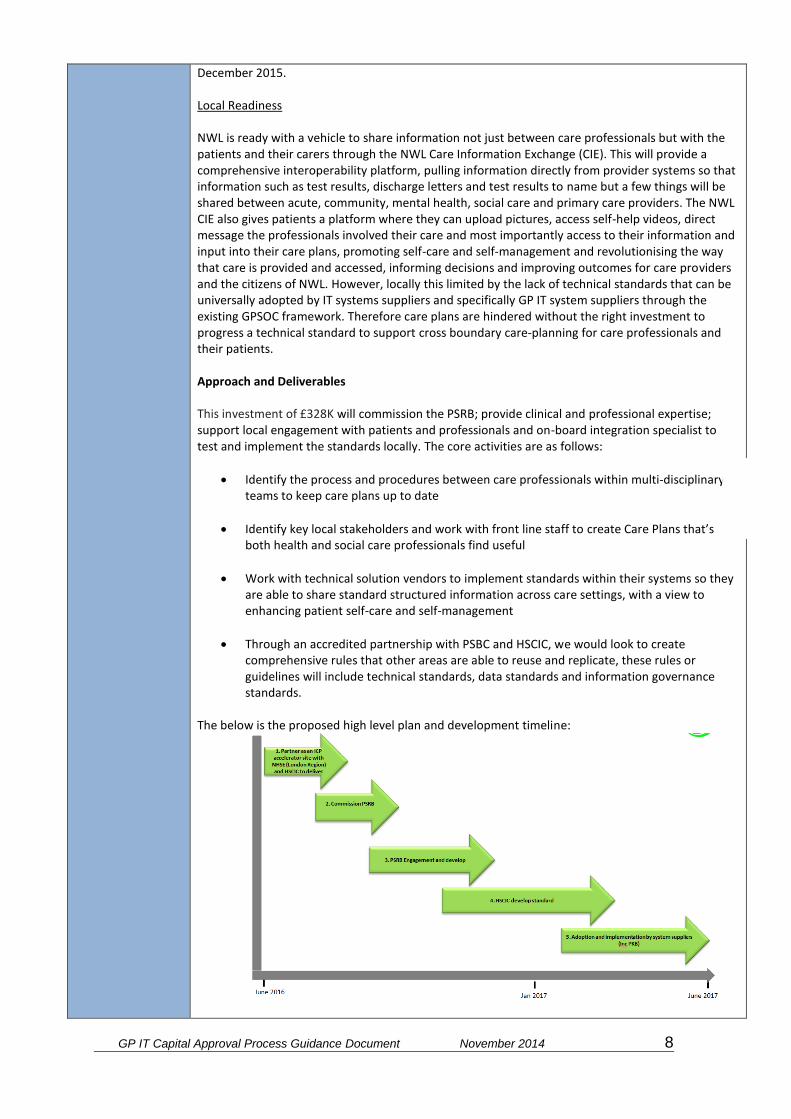
December 2015. Local Readiness NWL is ready with a vehicle to share information not just between care professionals but with the patients and their carers through the NWL Care Information Exchange (CIE). This will provide a comprehensive interoperability platform, pulling information directly from provider systems so that information such as test results, discharge letters and test results to name but a few things will be shared between acute, community, mental health, social care and primary care providers. The NWL CIE also gives patients a platform where they can upload pictures, access self-help videos, direct message the professionals involved their care and most importantly access to their information and input into their care plans, promoting self-care and self-management and revolutionising the way that care is provided and accessed, informing decisions and improving outcomes for care providers and the citizens of NWL. However, locally this limited by the lack of technical standards that can be universally adopted by IT systems suppliers and specifically GP IT system suppliers through the existing GPSOC framework. Therefore care plans are hindered without the right investment to progress a technical standard to support cross boundary care-planning for care professionals and their patients. Approach and Deliverables This investment of £328K will commission the PSRB; provide clinical and professional expertise; support local engagement with patients and professionals and on-board integration specialist to test and implement the standards locally. The core activities are as follows:
Identify the process and procedures between care professionals within multi-disciplinary teams to keep care plans up to date
Identify key local stakeholders and work with front line staff to create Care Plans that’s both health and social care professionals find useful
Work with technical solution vendors to implement standards within their systems so they are able to share standard structured information across care settings, with a view to enhancing patient self-care and self-management
Through an accredited partnership with PSBC and HSCIC, we would look to create comprehensive rules that other areas are able to reuse and replicate, these rules or guidelines will include technical standards, data standards and information governance standards.
The below is the proposed high level plan and development timeline:
cotchr
Typewritten Text
Document 5d

GP IT Capital Approval Process Guidance Document November 2014 9
Current context that NWL has two main GP Clinical Systems, EMIS in Brent, Harrow and Hillingdon and TPP (SystmOne) in Central Lodon, West London, Hammersmith & Fulham, Hounslow and Ealing. As a result we have two fairly well developed integrated care plan templates in NWL; the Hillingdon care plan which was created on EMIS GP Systems with a view to interoperability and the NWL CIE and the Community Independence Service (CIS) developed on SystmOne, hosted in the community health provider Central London Community healthcare (CLCH). We would look to bring both together to create a unified approach with support of the development of technical standards across all 8 boroughs. Therefore breaking dependency on a host system and ability to share systematically as a part of the wider interoperability agenda alongside the system-wide rollout of the NWL CIE and the Healthier London Partnership Information Exchange Platform covering all London boroughs.
Outcomes & Benefits The investment in integrated care standards and delivery effective and efficient care planning tools shall enable the:
Increase in care-planning capability. Care coordinators need the ability to create a care plan and review progress and results. The care plan will be the road map for the integrated care that the individual will receive, ensuring its appropriateness and timeliness. As part of the care planning process, access to a library of care protocols should also be available, to support decision making and ensure that the care plan being created is in line with relevant guidelines and best practices.
Develop Intervention management capability. To ensure that professionals can respond to the specific needs of individuals in a timely fashion, care teams should be alerted to relevant events. This could include alerts issued when an individual requires an intervention (e.g., vaccination reminders), based on recent events (e.g., discharge from hospital) or on a "care gap analysis”.
Develop remote monitoring capability. Self-management and empowering individuals to
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 10
make decisions about their care is an objective of supporting users to receive appropriate care in their home and, where appropriate, to self-manage by opening up patients records to them using North West London’s Care Information Exchange (CIE) and the Healthier London Partnership Information Exchange Platform (HLP IE). Providers will have the ability to monitor and share goals and objectives with and about service users remotely.
Therefore this could provide a large-scale system benefit of a PSRB endorsed technical standard for Integrated Care Planning to help nationally other NHS organisations, pioneers and vanguards.
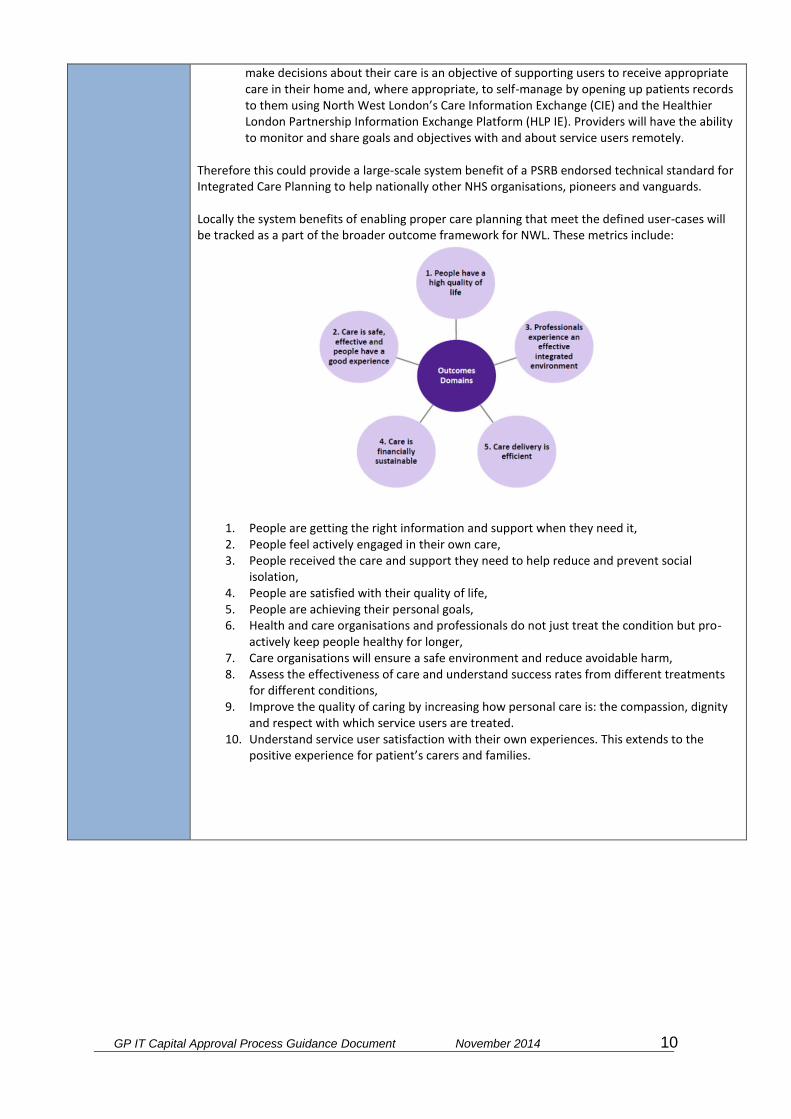
Locally the system benefits of enabling proper care planning that meet the defined user-cases will be tracked as a part of the broader outcome framework for NWL. These metrics include:
1. People are getting the right information and support when they need it, 2. People feel actively engaged in their own care, 3. People received the care and support they need to help reduce and prevent social
isolation, 4. People are satisfied with their quality of life, 5. People are achieving their personal goals, 6. Health and care organisations and professionals do not just treat the condition but pro-
actively keep people healthy for longer, 7. Care organisations will ensure a safe environment and reduce avoidable harm, 8. Assess the effectiveness of care and understand success rates from different treatments
for different conditions, 9. Improve the quality of caring by increasing how personal care is: the compassion, dignity
and respect with which service users are treated. 10. Understand service user satisfaction with their own experiences. This extends to the
positive experience for patient’s carers and families.
cotchr
Typewritten Text
Document 5d

GP IT Capital Approval Process Guidance Document November 2014 11
NON-RECURRENT INVESTMENT (including VAT)
NON-CASH RELEASING SAVINGS
None directly identified.
PRIORITISATION OF PROJECTS
In February 2016, NHS England released the ‘NHS Shared Planning Guidance’, including the Sustainability and Transformation Plans (STPs) and the enamelling Digital Roadmaps create multi-year, multi-organisational plans, built around the needs of local populations and their supporting health and social care organisations are being placed at the heart of the drive to create innovation and bring about a paperless, digitally engaged NHS by 2020.
PROPOSED PROCUREMENT STRATEGY
This scheme will be delivered within 16/17. The procurement process will start once NHS England approves the funding. Procurement will follow Brent’s Standard Financial Instructions and NHS procurement rules.
KEY RISKS
Scheme can be given by needs to be allocated by July 2016 Initial Project Risks
I. Lack of multidisciplinary representation will mean that care plans aren’t fit fir purpose for all care settings
II. The Caldicott review will not promote sharing of information for direct care of the patients between health and social care professionals
III. National Partners will not be able to support the integrated care planning standards and there will be a slow uptake from professionals without endorsement
IV. NWL CCG areas develop their own individual care plans, with no common consistency and increasing the duplication of effort for the NHS, resulting in an increase in spend
Initial System Risks
Project IntegratedCareBids
SumofTotalincVAT ColumnLabels
RowLabels 16-17GrandTotal
One-off £328,071 £328,071
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
DevelopmentofIntegratedCareStandards £270,000 £270,000
OfficeServices £12,000 £12,000
GrandTotal £328,071 £328,071
cotchr
Typewritten Text
Document 5d
GP IT Capital Approval Process Guidance Document November 2014 12
V. Multiple touch points, patients have to repeat their stories, information is not passed on to the right care professionals
VI. Information about a patients care is lost in translation between care professionals putting patients at risk and increasing duplication of effort for tests etc
VII. Increase in re-admittance for long term conditions because there is no active way to monitor progress and for patients to self-manage
VIII. Lack of commitment from system suppliers will mean that templates will not be made available to create an integrated care plan
IX. Nationally other pioneer areas develop their own individual care plans, with no common consistency and increasing the duplication of effort for the NHS, resulting in an increase in spend
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Organisation
Date
APPROVED BY: Head of Financial Management NHSE (London Region)
cotchr
Typewritten Text
Document 5d

GP IT Capital Approval Process Guidance Document November 2014 13
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.
cotchr
Typewritten Text
Document 5d
Document 5e
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17 BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name:
Videoconferencing
Practice code: All NWL CCGs practices
List size: 2.3M
Building condition: Technology Bid
Bid description
The investment requested for ‘Videoconferencing ‘ looks to use the digital medium to help optimise clinical and professional time to deliver Professional-to-Professional video-consultations (this includes multidisciplinary meetings) and Professional to Patient video-consultations. The initiative will also look to reduce potential where appropriate, the need for residential and care home visits. NWL has been running a proof-of-concept project ‘Vircon’ to support Professional-to-Professional consultation and would look to upscale the pilot project to all GP practices across North West London. Alongside, encouraging greater use of Video-consultations for routine clinical appointment/clinics, based on pilot work with 16 Central London CCG practices. This will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. The envisaged improvement is to better use of clinical time that may have otherwise spent on travelling for physical visits with potential non-cash releasing savings of £28K per practice. There is no request for commitment to on-going costs post the funding period as this decision will be built into lifetime of the funding if the solution is found to provide the envisaged benefits.
Bid value (if known): £742,440
Potential revenue consequence:
NO
Potential estimated revenue cost:
0
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG
√
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √
Demonstrates a process for monitoring, measuring and evaluating expected benefits.
√ Deliverable within financial years April 2016 to March 2019 (the end point for PCTF)
√
Consistent with primary care √ Evidence of patient involvement and √
Delivery in:
2016/20

Document 5e
GP IT Capital Approval Process Guidance Document November 2014 2
commissioning plans engagement across the local health economy
Recommended YES
Priority HIGH
Document 5e
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF. :
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
No
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
No
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. No
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
No
4 This is a bid for capital to provide core technology necessary to support a GP practice move
No
5 This is a bid for capital to provide core technology to a new GP practice No
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME Video Conferencing
NAME OF THE CCG MAKING THE APPLICATION
Sponsor: Brent CCG on behalf of NW London CCGs (Brent, Central London, Ealing, Hammersmith & Fulham, Hillingdon, Hounslow, and West London).
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Sonia Patel Digital Programme Director Email: [email protected] John Keating Head of ICT Projects North West London Collaboration of CCGs Email: [email protected]

Document 5e
GP IT Capital Approval Process Guidance Document November 2014 4
Mobile: 07766 070 628 Bill Sturman Director of Informatics Email: [email protected]
DELIVERY PARTNER CONTACT DETAILS
North West London Collaboration of CCGs Shared ICT Service Contact details as above.
BRIEF SCHEME DESCRIPTION
Strategic Context and Purpose The CCGs within NW London have identified the need for the local population to making better use of day to day technology already at their disposal to access local healthcare services, by:
Using videoconference technology to provide easier access to clinical services for patients.
Enabling fast and secure collaboration between GP’s, commissioners and providers.
With a predicted funding gap of £30bn by 2020, there is an increased need to become more efficient in the delivery of appointment and consultations; at both the point of entry and throughout the delivery of care plans, between those involved in delivering care and with patients directly.
- In 2015 78% of adults in the UK accessed the internet at least once per day1.
- 49% of adults in the UK used the internet to look for health related information2.
- Between 1995 and 2014 the number of GP consultations grew from around 200M to 360M
3.
- The NHS Digital Technology Strategy identifies that digital technology has the ‘power to change the relationship between patients and their GP, just as it has changed our relationship on other walks of life, such as managing our finances or shopping’
4
The Scheme is to provide video conferencing to GP’s that would also be accessible to patients, secondary care staff and CCG Staff. There are a number of scenarios in which this Deliver benefits. The organisations that will benefit from this are:
Brent CCG
Harrow CCG
Hillingdon CCG
Central London CCG
West London CCG
Hammersmith and Fulham CCG
Hounslow CCG
Ealing CCG Approach & Deliverables The Scope of this project is:
To roll out a complete Video conference solution to 3550 users initially allowing 1100 concurrent connections, with the potential to scale up to 3000 concurrent connections
Delivery programme will include:
Document 5e
GP IT Capital Approval Process Guidance Document November 2014 5
1. Implementation of a consolidated modern future proof video conferencing
solution available to: a. GP’s b. Patients c. Commissioners d. Provider
2. A thorough evaluation of current solutions available tested against agreed acceptance criteria.
3. The purchase, deployment, training and handover of the selected solution. The Chosen Solutions will deliver the following functionality:
Cloud based secure video conference facility
Cloud based secure audio conference facility
A single place to search for contacts
Screen sharing
Document sharing
Benefits & Outcomes The Benefits of Video conference are identified as:
1. Face to face consultation without the need to travel. 2. Collaboration
a. Between i. Clinician – CCG ii. Clinician to clinician iii. GP to MDT
3. Efficiencies a. Reduced requirements to travel for
i. GP’s ii. Immobile patients iii. Care home staff and residents
b. Reduced pressure on practice staff 4. Scalability
a. The proposed solution is available nationwide
1http://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/bulletins/internetaccesshouseholdsandindividuals/2015-08-06 2http://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/bulletins/internetaccesshouseholdsandindividuals/2015-08-06 3 https://www.england.nhs.uk/wp-content/uploads/2013/09/igp-cta-evid.pdf | http://www.rcgp.org.uk/policy/rcgp-policy-areas/~/media/Files/Policy/A-Z-policy/2015/RCGP-Patient-safety-implications-of-general-practice-workload-July-2015.ashx 4 NHS England, https://www.england.nhs.uk/ourwork/pe/patient-online/

Document 5e
GP IT Capital Approval Process Guidance Document November 2014 6
NON-RECURRENT INVESTMENT
POTENTIAL NON-CASH RELEASING SAVINGS
PRIORITISATION OF PROJECTS
1- HIGH
PROPOSED PROCUREMENT STRATEGY
The procurement process will start once NHS England approves the funding. Procurement will follow Brent’s Standard Financial Instructions and NHS procurement rules.
KEY RISKS
There is a risk: GP practices will not be engaged in the project The consequence would be: low uptake and utilisation of video conferencing This will be mitigated by: Clinical technology engagement will be pivotal to the project. There will be CCG and clinical leads, super users / champions and MDT groups involved in the delivery of the project. There will be awareness and engagement sessions and campaigns. Existing and new communication channels can be used to promote videoconferencing.
Project Videoconferencing
SumofTotalincVAT ColumnLabels
RowLabels 16-17 17-18 18-19 19-20 GrandTotal
One-off £421,856 £207,188 £57,536 £55,860 £742,440
(P42)ProjectManager £101,250 £69,525 £170,775
(P43)TechnicalEngineer(band5/6) £94,875 £94,875
(P44-P55)2xTrainers-halfdayperpracticeandcorporatedaysplussupport(band5) £75,000 £77,250 £152,250
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
Meetingroomsetup £19,200 £19,200
OfficeServices £9,000 £6,180 £15,180
Perperpermonth£1.03 £26,327 £26,327
Perperpermonth£1.06(inc3%annualuplift) £54,233 £54,233
Perperpermonth£1.09(inc3%annualuplift) £57,536 £57,536
Perperpermonth£1.13(inc3%annualuplift) £55,860 £55,860
PMcosts(hardwareandsoftwaretools) £5,760 £5,760
ReadinessAssessment £3,000 £3,000
WebCamswithbuiltinmics £41,372 £41,372
GrandTotal £421,856 £207,188 £57,536 £55,860 £742,440
Project Description BenefitType BenefitOccurrence UnitCost Numberofunits TotalRunRate BenefitsProfile
16-17
BenefitsProfile
17-18
BenefitsProfile
18-19
Benefits
Profile
19-20
TotalBenefits PerPractice
Videoconferencing AverageoneGPsessionperweekpercarehome.300carehomes.15,600
visitsperyear.Singlesessioncostis£400.Onesessionsavedpermonth(25%)
AnnualRecurrent £400.00 3900 £1,560,000 £0 £390,000 £780,000 £1,560,000 £2,730,000 £6,825
Videoconferencing MDT1hourperweeksaved,60,000hoursperyearofGPtime £44.17 60000 £2,650,200 £662,550 £2,650,200 £2,650,200 £2,650,200 £8,613,150 £21,533
Total £4,210,200 £11,343,150

Document 5e
GP IT Capital Approval Process Guidance Document November 2014 7
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Organisation
Date
APPROVED BY: Head of Financial Management NHSE (London Region)
Document 5e
GP IT Capital Approval Process Guidance Document November 2014 8
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.
Document 5f
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17
BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name:
Integrated telecoms and patient management systems
Practice code: All NWL CCGs practices
List size: 2.3M
Building condition: Technology Bid
Bid description
The investment for £7.3M is to apply similar tools and techniques commonly used in a variety of marketing and other service industries using a combination of software, hardware and telephony solutions to enable a personalised and integrated patient centric offering which promotes, supports and informs health and wellbeing, and provides rich intelligence data back to the service providers and commissioners in order to improve services and communication. GP practices across the CCG will be offered this suite of solutions. Access to these will be to all registered patients. However, depending on the acuity, comorbidity and long-term conditions of the patient different combinations will be used. For instance, citizens at high risk of diabetes could be sent regular motivational videos to encourage adherence to goals agreed with their primary care team, whereas patients with COPD could be provided with instructional videos on correct inhaler technique and pulmonary exercises. The beneficiaries will be the patient, the carer and the GP practice staff. The patient experience will improve through access to primary care services by personalised interaction. Non-cash releasing savings £5K per practice releasing capacity to manage with increasing demand on services. There is no request for commitment to on-going costs post the funding period as this decision will be built into lifetime of the funding if the solution is found to provide the envisaged benefits.
Bid value (if known): £7,363,328
Potential revenue consequence: No
Potential estimated revenue cost: 0
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG √
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √
Demonstrates a process for monitoring, measuring and evaluating expected benefits.
√ Deliverable within financial years April 2016 to March 2019 (the end point for PCTF)
√
Delivery in: 2016/20

Document 5f
GP IT Capital Approval Process Guidance Document November 2014 2
Consistent with primary care commissioning plans
√ Evidence of patient involvement and engagement across the local health economy
√
Recommended YES
Priority HIGH

Document 5f
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF. :
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure.
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
4 This is a bid for capital to provide core technology necessary to support a GP practice move
5 This is a bid for capital to provide core technology to a new GP practice
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME Development of self care and patient management systems
NAME OF THE CCG MAKING THE APPLICATION
Sponsor: Brent CCG a linked bid on behalf of North West London CCGs (Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCG)
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Bill Sturman Director of Informatics, North West London Collaboration of CCGs, Email: [email protected] Sonia Patel Digital Programme Director, North West London Collaboration of CCGs, Email: [email protected]
Document 5f
GP IT Capital Approval Process Guidance Document November 2014 4
John Keating Head of ICT Projects North West London Collaboration of CCGs, Shared ICT Service Email: [email protected] Mobile: 07766 070 628
DELIVERY PARTNER CONTACT DETAILS
North West London Collaboration of CCGs Shared ICT Service Contact details as above.
BRIEF SCHEME DESCRIPTION
Strategic Context and Purpose GP practices experience some of the highest patient foot fall in the NHS and offer a similarly high volume and diversity of transactional services for their patients. Efficient and effective access to primary care continues to be one of the most challenging areas in the NHS. Whilst there have been some efforts to establish online services at GP practices, there has been minimal take up and awareness by patients. This may in part be due to the complexity of the GP record and the need to break this down into digestable elements of information. At the same time, people with long-term conditions use:
52% of all GP appointments
65% of all outpatient appointments
72% of all inpatient bed days Nearly 70% of NHS spending on primary care and hospital care supports people with long-term conditions. The UK economy stands to lose roughly £16 billion over the next 10 years through premature deaths due to heart disease, stroke and diabetes. There is strong evidence that supported self-management helps to increase people’s knowledge about their condition, how to self-care (including improving diet, physical activity and symptom control), and when to use health services appropriately. Interventions which integrate several technologies such as online education, mobile phones and telemedicine have shown the most potential for improving self-management. Furthermore, through initiatives such as the National Diabetes Prevention Programme, there is an identified need to target health and wellbeing messages to specific at risk segments of the population. Targeted messaging, personalised communication and the ability to automatically recognise and triage the patient or carer from their initial contact allow opportunities for more sophisticated and effective interactions. We cannot assume that a “one size fits all” approach is any more appropriate or effective for health and wellbeing messaging than it is for any other form of marketing. Messaging can be tailored according to both specific clinical data available within the patient record and publicly available health and wellness geodemographic data. The purpose of this proposal is to apply similar tools and techniques commonly used in a variety of marketing and other service industries using a combination of software, hardware and telephony solutions to enable a personalised and integrated patient centric offering which promotes, supports and informs health and wellbeing, and provides rich intelligence data back to the service providers and commissioners in order to improve services and communication. Whilst different aspects of these solutions have been intermittently used in some practices, there are no examples of a comprehensive and integrated approach that brings a set of tools together and presents it as one solution.
Document 5f
GP IT Capital Approval Process Guidance Document November 2014 5
Approach & Deliverables The solutions that will be deployed in this project will use a combination of channels of communication as appropriate for the patient:
Telephone – managing inbound and outbound calls both for landlines and mobile numbers.
Email – using a range of solutions for personalised, targeted and timely email messages.
SMS – implementing text messaging solutions that are more economical, better integrated in the workflow of practices, and used more extensively to prompt actions and reminders.
Online –through video content, online services, websites, and smartphone apps that allow the patient to manage their health and wellbeing more effectively and interact more successfully with other services.
GP practices across the CCG will be offered this suite of solutions. Access to these will be to all registered patients. However, depending on the acuity, comorbidity and long term conditions of the patient different combinations will be used. For instance, citizens at high risk of diabetes could be sent regular motivational videos to encourage adherence to goals agreed with their primary care team, whereas patients with COPD could be provided with instructional videos on correct inhaler technique and pulmonary exercises. The project will be implemented across multiple years in 4 phases:
1. Design and specification – developing the model and integration plan between the technologies and target patient segments. Includes sourcing and/or design of educational and motivational content.
2. Pilot – to test the design and trial the solutions and implementation plans. 3. Procurement – carry out a procurement for the final solution, selecting a
delivery organisation that can implement the solution 4. Deployment – taking a phased approach to implementing the final solution.
Outcomes and Benefits The beneficiaries will be the patient, the carer and the GP practice staff. The patient experience will improve through access to primary care services by personalised interactions, examples will include:
1. By recognising the callers telephone number and integrating with their record the caller can be automatically targeted to the most appropriate member of staff or fast tracked depending on their medical condition.
2. By linking telephony with the clinical information system the patient’s record can be more quickly retrieved and automated actions triggered in terms of follow up questions, actions and record completeness.
3. By using healthcare CRM (customer relationship management) software, it will be possible to target messaging to specific segments of the population and automate delivery tracking and follow up messaging. This will allow promotion of relevant health and wellness services, and delivery of educational information such as support for weight loss, diabetes management or smoking cessation to target demographics or clinical segments. Furthermore, proactive communications between patients visits will encourage adherence to goals that a patient has identified, provide coaching on healthy behaviours or promote medications compliance.

Document 5f
GP IT Capital Approval Process Guidance Document November 2014 6
The GP practice will experience examples such as:
1. Automated triage and streaming of patient calls based on their need rather than the sequence and frequency of their calls or contacts.
2. Automation of high volume, low added value functions freeing up administrative and clinical staff capacity ranging from call handling to follow up and patient monitoring.
3. Easier to use automated tools that will better integrate with existing clinical information systems and manage patients with higher need and more frequent interventions.
4. Targeting messaging and content delivery (e.g. motivational videos or self-management education) to specific population groups including citizens at high risk of diabetes or patients with frequent COPD exacerbations.
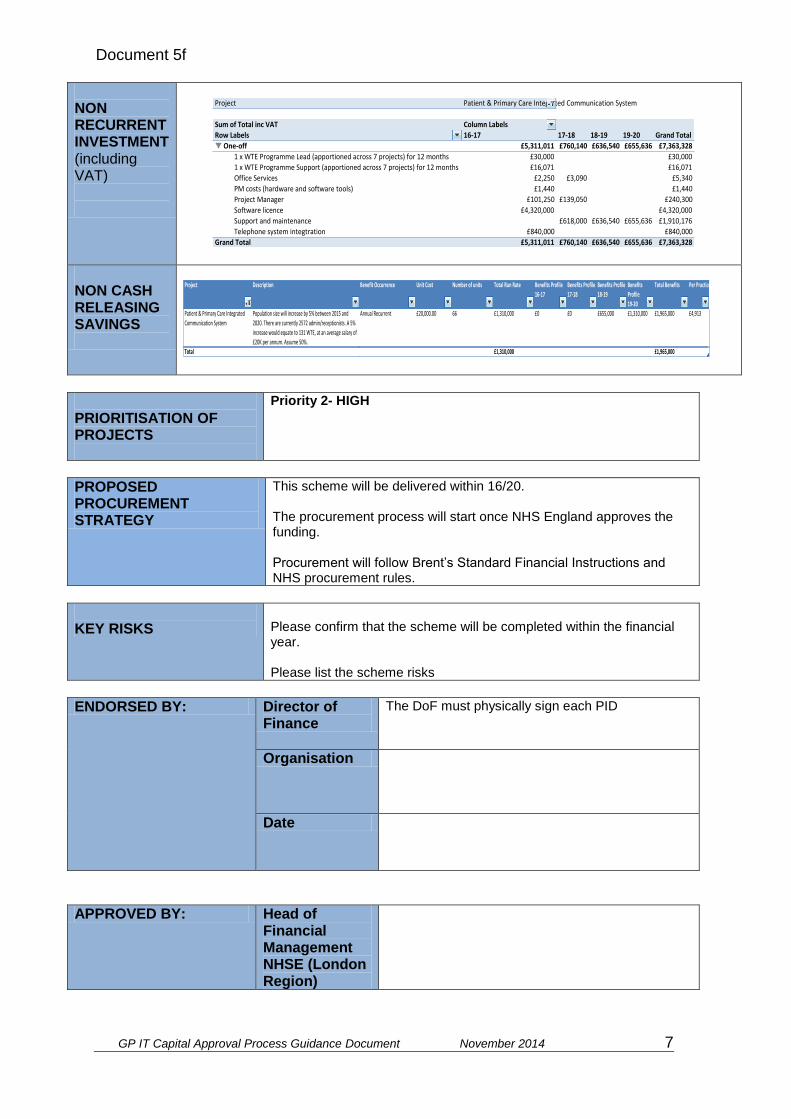
Document 5f
GP IT Capital Approval Process Guidance Document November 2014 7
NON RECURRENT INVESTMENT (including VAT)
NON CASH RELEASING SAVINGS
PRIORITISATION OF PROJECTS
Priority 2- HIGH
PROPOSED PROCUREMENT STRATEGY
This scheme will be delivered within 16/20. The procurement process will start once NHS England approves the funding. Procurement will follow Brent’s Standard Financial Instructions and NHS procurement rules.
KEY RISKS
Please confirm that the scheme will be completed within the financial year. Please list the scheme risks
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Organisation
Date
APPROVED BY: Head of Financial Management NHSE (London Region)
Project Patient&PrimaryCareIntegratedCommunicationSystem
SumofTotalincVAT ColumnLabels
RowLabels 16-17 17-18 18-19 19-20 GrandTotal
One-off £5,311,011 £760,140 £636,540 £655,636 £7,363,328
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
OfficeServices £2,250 £3,090 £5,340
PMcosts(hardwareandsoftwaretools) £1,440 £1,440
ProjectManager £101,250 £139,050 £240,300
Softwarelicence £4,320,000 £4,320,000
Supportandmaintenance £618,000 £636,540 £655,636 £1,910,176
Telephonesystemintegtration £840,000 £840,000
GrandTotal £5,311,011 £760,140 £636,540 £655,636 £7,363,328
Project Description BenefitOccurrence UnitCost Numberofunits TotalRunRate BenefitsProfile
16-17
BenefitsProfile
17-18
BenefitsProfile
18-19
Benefits
Profile
19-20
TotalBenefits PerPractice
Patient&PrimaryCareIntegrated
CommunicationSystem
Populationsizewillincreaseby5%between2015and
2020.Therearecurrently2572admin/receptionists.A5%
increasewouldequateto131WTE,atanaveragesalaryof
£20Kperannum.Assume50%.
AnnualRecurrent £20,000.00 66 £1,310,000 £0 £0 £655,000 £1,310,000 £1,965,000 £4,913
Total £1,310,000 £1,965,000

Document 5f
GP IT Capital Approval Process Guidance Document November 2014 8
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.
Document 5g
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17
BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name: Care Homes
Practice code: All NWL CCGs practices
List size: 2.3M
Building condition: Technology Bid
Delivery in: 2016/20
Bid description
The investment requested for ‘Care Homes’ is to improve the digital maturity between primary care and care homes through the use technology to provide a structured and pro-active approach to care, complemented by mobile working for Primary care; access to relevant GP System (for care homes); remote video consultation between care home residents and GP. NWL are keen to take forward some of the early learning’s and work from Care Homes Vanguards such as Sutton Homes of Care and Airedale & Partners. The funding will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. The funding sought £222K will initiate a pilot project to fund 16 care homes through an Expression of Interest process to develop systems, process and information governance for digital communication and information; provide terminals/equipment to support video consultations and make available clinical software and training to qualified staff to access patients records. Potential benefits are prevention in avoidable non-elective admissions due conditions such as UTI s, falls and pressure sores and a decrease in Out of Hours GP services (capacity that can be released for other activity). The exact cash or non-cash releasing savings are difficult to identify and the project will look to develop and evaluation framework to capture the true benefits. There is no request for commitment to on-going costs post the funding period as this decision will be built into lifetime of the funding if the solution is found to provide the envisaged benefits.
Bid value (if known): £221,867
Potential revenue consequence: NO
Potential estimated revenue cost: 0
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG √
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √

Document 5g
GP IT Capital Approval Process Guidance Document November 2014 2
Demonstrates a process for monitoring, measuring and evaluating expected benefits.
√ Deliverable within financial years April 2016 to March 2019 (the end point for PCTF)
√
Consistent with primary care commissioning plans
√ Evidence of patient involvement and engagement across the local health economy
√
Recommended YES
Priority MEDIUM

Document 5g
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF. :
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
No
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
No
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. No
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
No
4 This is a bid for capital to provide core technology necessary to support a GP practice move
No
5 This is a bid for capital to provide core technology to a new GP practice No
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME Care Home Pilots
NAME OF THE CCG MAKING THE APPLICATION
Sponsor: Brent CCG on behalf of NW London CCGs (Brent, Central London, Ealing, Hammersmith & Fulham, Hillingdon, Hounslow, and West London).
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Sonia Patel Digital Programme Director Email: [email protected] John Keating Head of ICT Projects North West London Collaboration of CCGs
Document 5g
GP IT Capital Approval Process Guidance Document November 2014 4
Email: [email protected] Mobile: 07766 070 628 Bill Sturman Director of Informatics Email: [email protected]
DELIVERY PARTNER CONTACT DETAILS
North West London Collaboration of CCGs Shared ICT Service Contact details as above.
BRIEF SCHEME DESCRIPTION
Strategic Context and Purpose
In North West London (NWL), we have a strategic vision to deliver new models of care which enable joined up, integrated care for our 2.3 million population, keeping people well for longer in their homes by care professionals to work together in multi-disciplinary teams. With shrinking budgets and a rapidly aging population these new models of care and multi-disciplinary teams working across NWL will need to harness to new digital revolution and use technology to help the most vulnerable. With an aging population care homes do and will continue to play an integral part of new models of care. An estimated 380,000 people live in approximately 17,000 nursing or residential homes in England alone, 95% of the residents inhabiting them are over 65. There are around three times as many adults in care homes as in general hospital beds. For the foreseeable future people will continue to live in care homes and the demand is due to increase as the population ages. Recent studies have shown that proactive medical review and more responsive support for care home residents can reduce emergency hospital admissions in general and that repeated hospital admissions make little difference to residents’ outcomes. The following key issues facing primary care in nursing homes have been highlighted;
• Issues with staffing ratios, training and management – Nursing home staff training and the use of agency staff have been flagged as issues. Issues included an overly risk averse approach leading to more inappropriate calls out to LAS or GPs but also a failure to properly identify problems.
• Complex care requirements – care of nursing home residents is complex and beyond the remit of the core GMS/PMS services. Visits to nursing homes also require more time for GPs, which must be scheduled around other appointments.
• Administrative burden on top of visits – there is a lot more work required from General Practice on top of nursing home visits. In particular, administrative tasks associated with prescription requests from nursing homes require a significant amount of work.
• Uneven distribution of patients – nursing home residents are not evenly distributed across practices, resulting in a higher burden for some practices. Consideration is required with regards to patient choice over their GP.
• Uncertainty on the main point contact for primary care – nursing homes have residents from multiple practices, which may be a barrier to improving the GP/nursing home relationship. Some homes note the difficulty in getting GPs to visit their patients in nursing homes.
• Limited continuity of care – GPs are seeing other practices’ patients • Avoidable admissions – Best practice nationally suggests that there is often
overreliance upon LAS and potentially avoidable acute admissions (see North Staffordshire’s findings on acute activity
• Higher weekend LAS calls – this is despite the CCG already commissioning weekend cover – see Appendix 3 for further LAS and CCG LES data.
• Limited communication on admissions –NWL Hospitals conducted a nursing home mortality review which noted the limited communication between hospital, nursing homes and GPs during acute admission

Document 5g
GP IT Capital Approval Process Guidance Document November 2014 5
• No clear expectation on level of GP care required – there is currently no national guidance on the level of additional primary care required in nursing homes above GMS/PMS services.
• Some patients may ‘fall through the gaps’ – high patient turnover and respite patients can result in patients being missed by GPs covering the home and by the patient’s GP.
Therefore nursing and residential homes would directly benefit from remote access secure video to the GP practices allowing consultations with nurses and GPs both in and out of normal hours – for everything from cuts and bumps to diabetes management to the onset of confusion. We predict that emergency admissions from these homes, based on the work already being done by NWL CCG’s (2012/2013), we predict that by promoting tele-health into care homes, it will reduced the need for GP appointments by about 35%, acute admissions by 32% and A&E attendances by up to 40%. Care homes are under increasing pressure to offer a range of care and support services to those in their care, systems and innovations can help staff from carrying out their tasks and improve on the health and well-being of their residents. They place a central role in plugging the intermediate care gap, staff have the valuable knowledge and skills and do work closely with local primary care providers, however there is more to be done in connecting up primary and social care and proactive care to keep residents well for longer and out of hospitals. Care homes residents which are often with complex needs and conditions, about two thirds of care home residents are immobile or need assistance therefore should be among the first to benefit from a major new drive to modernise how the NHS delivers care. Technology can allow residents to self-manage and empower them where possible to become more engaged with their care, it can also help care homes to take a more holistic view of the delivery of care, increasing preventative care and identify those that are most at risk.
Approach and Deliverables Expression of Interest Initiate the process of identifying pilots through an Expression of Interest. Local CCGs and Primary Care GP IT Professionals will set the Expression of Interest criteria which likely to include details around CQC registration, patient safety, clinical quality, relationship with local primary care providers and level of investment from the care home to ensure a successful pilot. The group overseeing the Expression of Interest process will also develop the evaluation criteria for the pilot sites. The proposal is to support at least 16 care homes this equates to approximately 2 care homes per CCG. The successful care home will be required to sign a Memorandum of Understanding (MOU) that outlines its commitment as pilot site. Pilot Site Implementation Plan The pilot sites will look in phases to implement the following with their primary care providers:
Phase 1: Co-design and co-develop pathways between primary care and care homes supported by digital communication, systems, processes this would include establishing the appropriate clinical protocols and governance, workforce training programme plan, information governance (inc RA access for personnel) and evaluation framework.
Phase 2: Provide equipment, set-up and implement systems for: o Mobile working for primary care professionals o Provide the agreed care homes staff with access to EMIS/Systmone o Remote video consultation between care home residents and GP; o Potential remote access to resident health data through tele-health; and use of
tele-care.
Phase 3: Deliver a robust education and training programme for staff, through an
Document 5g
GP IT Capital Approval Process Guidance Document November 2014 6
online education and training platform and bespoke courses (via the CIE or Vitrucare TBC)
Phase 4: Mobilise the new agreed pathways with new digital kit and processes.
Phase 5: Track and monitor progress over the funding period and conduct a thorough evaluation at the end of the pilot to understand the benefits.
Outcomes and Benefits
The changes described has the potential to support the whole health and social care system and benefit of local people living in care homes and assisted living as well as their relatives / unpaid carers and the local. The system benefits are likely to include:
1. Fewer A&E presentations of preventable attendances due to Enhanced Primary and Community Care and prevention management training put in place
2. Lower hospital admissions due to enhanced training to allow for earlier detection and management of the deteriorating resident
3. Enhanced Primary and Community Care interventions, allowing for early treatment and management of condition before they reach the stage of requiring hospital admissions
4. Reduced number of ambulance call outs as care staff will have increased confidence in their ability to recognise the deteriorating resident, allowing for earlier treatment and management.
5. Increase in digital capability of Care Co-ordinators and residents will enable them to actively support self-care and self-management once discharge back to the care home
6. Improve ability of care staff and patients to use technology to manage more complex conditions and treatment
7. Create a sustainable model for other health and social care systems to further integrate their care services to provide joined up care
8. Improved resident, carer and staff experience The quantitative metrics that will be tracked over the course of the pilot
9. Avoidable conditions such as UTIs, Falls and Pressure sores 10. Decrease in A+E attendances 11. Decrease in Non Elective Admissions 12. Decrease in Out of Hours GP services (capacity released for other activity)
Reference from quick guide NHS England

Document 5g
GP IT Capital Approval Process Guidance Document November 2014 7
NON RECURRENT INVESTMENT (including VAT)
NON CASH RELEASING SAVINGS
The evaluation framework will determine the potential savings through measuring over time the suggested indicators:
1. Avoidable conditions such as UTIs, Falls and Pressure sores 2. Decrease in A+E attendances 3. Decrease in Non Elective Admissions 4. Decrease in Out of Hours GP services (capacity released for other
activity)
PRIORITISATION OF PROJECTS
MEDIUM
PROPOSED PROCUREMENT STRATEGY
This scheme will be delivered within 2016-2020. The procurement process will start once NHS England approves the
funding. Procurement will follow Brent’s Standard Financial Instructions and
NHS procurement rules.
KEY RISKS
Care homes potential fail our patients with lack of appropriate information.
Call GP time to make physical visits is unsustainable with increasing demand on primary care.
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Organisation
Date
Project CareHomes
SumofTotalincVAT ColumnLabels
RowLabels 16-17 17-18 18-19 19-20 GrandTotal
One-off £151,945 £22,622 £23,300 £23,999 £221,867
(P52)TechnicalProjectManager £67,500 £67,500
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
4Gcard £2,160 £4,450 £4,583 £4,721 £15,913
BroadbandLine £5,760 £11,866 £12,222 £12,588 £42,435
EMISAnywhereDevice(2perCCG) £11,520 £11,520
EMISAnywhereSupport £3,024 £3,115 £3,208 £9,347
Laptops £14,400 £14,400
N3VPNtokens £1,593 £3,283 £3,381 £3,482 £11,740
OfficeServices £1,500 £1,500
PMcosts(hardwareandsoftwaretools) £1,440 £1,440
GrandTotal £151,945 £22,622 £23,300 £23,999 £221,867
Document 5g
GP IT Capital Approval Process Guidance Document November 2014 8
APPROVED BY: Head of Financial Management NHSE (London Region)
Document 5g
GP IT Capital Approval Process Guidance Document November 2014 9
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.

Document 5h
GP IT Capital Approval Process Guidance Document November 2014 1
PRIMARY CARE TRANSFORMATION FUND 2016/17
BID SUMMARY FRONT SHEET
CCG: North West London CCGs (Linked Bid for Hillingdon CCG, Harrow CCG, Brent CCG, Hounslow CCG, Ealing CCG, Hammersmith & Fulham CCG, West London CCG and Central London CCCG)
Scheme description /Practice name: New Models of Primary Care
Practice code: All NWL CCGs practices
List size: 2.3M
Building condition: Technology Bid
Within a mile of a hub: YES/NO N/A
Delivery in: 2016/20
PCIF/IG funding received 15/16 N/A
Scheme deferred in 15/16 by NHSE N/A
Scheme rejected in 15/16 by NHSE N/A
Bid description
The investment requested for ‘New Models of Primary Care’ will enable the mobilisation and delivery of new out-of-hospital services as a part GP Federation Development. This includes IT design and specification for infrastructure, system applications and delivery of critical business intelligence (to understand population health needs, support delivery of virtual/integrated care wards). This funding will provide a stepping-stone for GP Federations to actively support and participate in local development of their Accountable Care Organisations. The funding will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. The benefits will support the early stages of the new organisational forms and functions to help future operating model and requirements for NWL primary care. There is no request for commitment to on-going costs post the funding period as this decision will be built into lifetime of the funding if the solution is found to provide the envisaged benefits.
Bid value (if known): £8,528,485
Potential revenue consequence: NO
Potential estimated revenue cost: 0
Meets NHSE criteria
Enabling 7 day access √ Increased capacity of clinical services out of hospital √
Increased training capacity
√ Enabling access to wider services as set out in commissioning intentions to reduce unplanned admissions to hospital
√
Meets additional criteria for technology schemes
Clear identified need √ Demonstrates that the CCG has considered IG √
Demonstrates alignment with the Local Digital Roadmap
√ Sustainable in the long term √
Demonstrates a process for monitoring, measuring and evaluating expected benefits.
√ Deliverable within financial years April 2016 to March 2019 (the end point for PCTF)
√

Document 5h
GP IT Capital Approval Process Guidance Document November 2014 2
Consistent with primary care commissioning plans
√ Evidence of patient involvement and engagement across the local health economy
√
Recommended YES
Priority HIGH
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 3
NHS England (London Region): Capital investments in digital technology
Project Initiation Document – 2016/17
This PID should be completed by any organisation wishing to submit a technology related bid against the NHSE London regional capital allocation in 2016/17. CCGs should complete a separate PID for each scheme. Consolidated bids from multiple CCGs for GPIT will not be accepted. Please note: PIDs should be completed for all planned schemes including GPIT, PMCFand PCTF.
Purpose of Bid (select one) Yes/No
1 This is a bid to replace ‘core’ GPIT infrastructure. (max of 20-25% in any single year).
No
2 This is a bid to enhance ‘core’ GPIT infrastructure. The investment will result in reduced ongoing operating costs.
No
3 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. No
4 This is a bid to replace ‘core’ CCG or CSU technology infrastructure. The investment will result in reduced ongoing operating costs.
No
4 This is a bid for capital to provide core technology necessary to support a GP practice move
No
5 This is a bid for capital to provide core technology to a new GP practice No
6 This is a bid for capital to ’provide new and additional ‘capabilities’ that will transform’ the way in which care is delivered to patients
Yes
TITLE OF SCHEME New Models of Primary Care
NAME OF THE CCG MAKING THE APPLICATION
Sponsor: Brent CCG on behalf of NW London CCGs (Brent, Central London, Ealing, Hammersmith & Fulham, Hillingdon, Hounslow, and West London).
CONTACT DETAILS
Sue Hardy Head of Strategic Estates Development Email: [email protected] Mobile: 07957 298481 Bill Sturman Director of Informatics Email: [email protected] Sonia Patel Digital Programme Director Email: [email protected]
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 4
John Keating Head of ICT Projects North West London Collaboration of CCGs Email: [email protected] Mobile: 07766 070 628 Mobile: 07766 070 628
DELIVERY PARTNER CONTACT DETAILS
North West London Collaboration of CCGs Shared ICT Service Contact details as above.
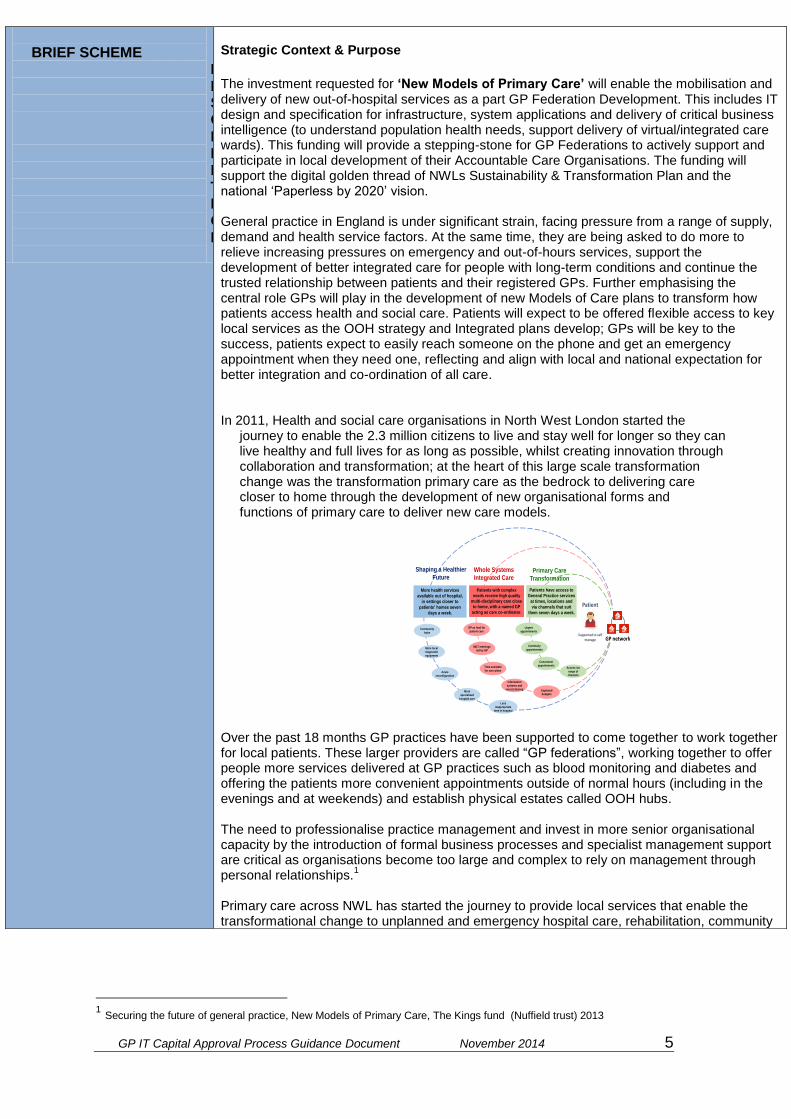
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 5
1 Securing the future of general practice, New Models of Primary Care, The Kings fund (Nuffield trust) 2013
BRIEF SCHEME
DESCRIPTION
Strategic Context & Purpose
The investment requested for ‘New Models of Primary Care’ will enable the mobilisation and delivery of new out-of-hospital services as a part GP Federation Development. This includes IT design and specification for infrastructure, system applications and delivery of critical business intelligence (to understand population health needs, support delivery of virtual/integrated care wards). This funding will provide a stepping-stone for GP Federations to actively support and participate in local development of their Accountable Care Organisations. The funding will support the digital golden thread of NWLs Sustainability & Transformation Plan and the national ‘Paperless by 2020’ vision. General practice in England is under significant strain, facing pressure from a range of supply, demand and health service factors. At the same time, they are being asked to do more to relieve increasing pressures on emergency and out-of-hours services, support the development of better integrated care for people with long-term conditions and continue the trusted relationship between patients and their registered GPs. Further emphasising the central role GPs will play in the development of new Models of Care plans to transform how patients access health and social care. Patients will expect to be offered flexible access to key local services as the OOH strategy and Integrated plans develop; GPs will be key to the success, patients expect to easily reach someone on the phone and get an emergency appointment when they need one, reflecting and align with local and national expectation for better integration and co-ordination of all care. In 2011, Health and social care organisations in North West London started the
journey to enable the 2.3 million citizens to live and stay well for longer so they can live healthy and full lives for as long as possible, whilst creating innovation through collaboration and transformation; at the heart of this large scale transformation change was the transformation primary care as the bedrock to delivering care closer to home through the development of new organisational forms and functions of primary care to deliver new care models.
Over the past 18 months GP practices have been supported to come together to work together for local patients. These larger providers are called “GP federations”, working together to offer people more services delivered at GP practices such as blood monitoring and diabetes and offering the patients more convenient appointments outside of normal hours (including in the evenings and at weekends) and establish physical estates called OOH hubs. The need to professionalise practice management and invest in more senior organisational capacity by the introduction of formal business processes and specialist management support are critical as organisations become too large and complex to rely on management through personal relationships.
1
Primary care across NWL has started the journey to provide local services that enable the transformational change to unplanned and emergency hospital care, rehabilitation, community
Shaping a Healthier
FutureWhole Systems
Integrated CarePrimary Care
Transformation
More health services
available out of hospital,
in settings closer to
patients’ homes seven
days a week.
Patients with complex
needs receive high quality
multi-disciplinary care close
to home, with a named GP
acting as care co-ordinator.
Patients have access to
General Practice services
at times, locations and
via channels that suit
them seven days a week.
Patient
MDT meetings
led by GP
Community
hubs
GP as lead for
patient care
Time available
for care plans
Information
systems and
record sharing Capitated
budgets
Supported to self manage
More local
diagnostic
equipment
More
specialised
hospital care
Acute
reconfiguration
Less
inappropriate
time in hospital
++
++++
GP network
Access via
range of
channels
Urgent
appointments
Convenient
appointments
Continuity
appointments
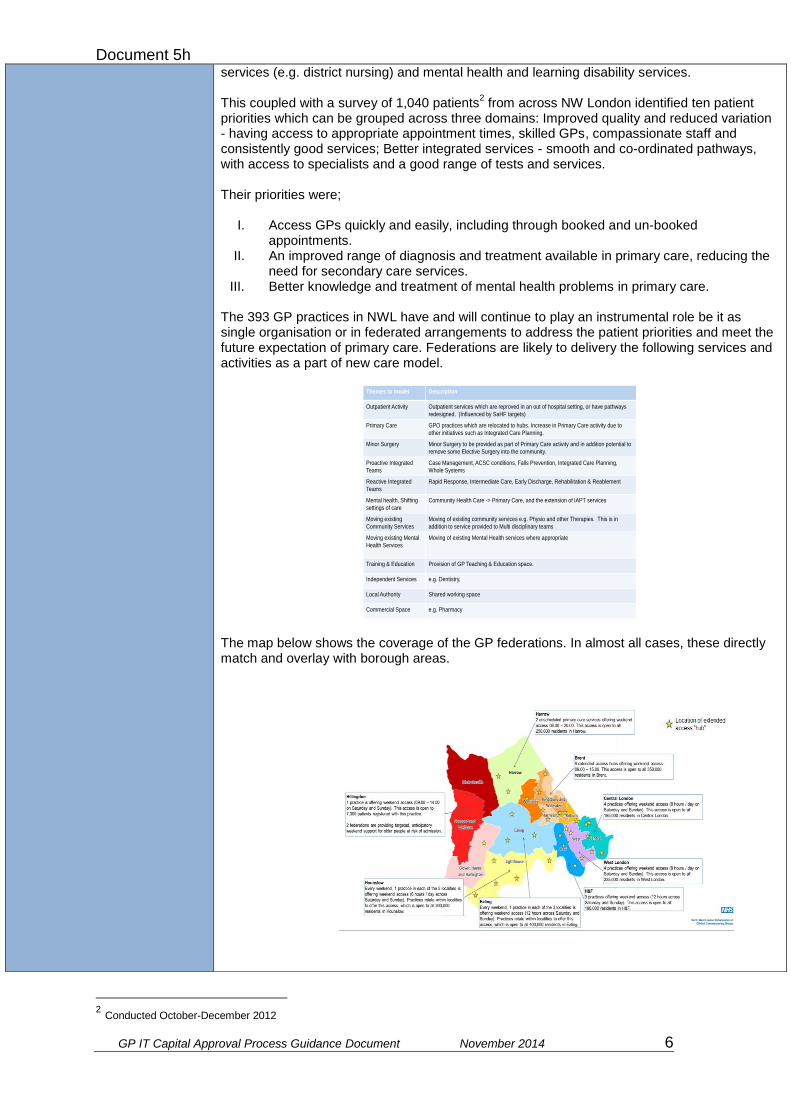
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 6
2 Conducted October-December 2012
services (e.g. district nursing) and mental health and learning disability services. This coupled with a survey of 1,040 patients
2 from across NW London identified ten patient
priorities which can be grouped across three domains: Improved quality and reduced variation - having access to appropriate appointment times, skilled GPs, compassionate staff and consistently good services; Better integrated services - smooth and co-ordinated pathways, with access to specialists and a good range of tests and services. Their priorities were;
I. Access GPs quickly and easily, including through booked and un-booked appointments.
II. An improved range of diagnosis and treatment available in primary care, reducing the need for secondary care services.
III. Better knowledge and treatment of mental health problems in primary care. The 393 GP practices in NWL have and will continue to play an instrumental role be it as single organisation or in federated arrangements to address the patient priorities and meet the future expectation of primary care. Federations are likely to delivery the following services and activities as a part of new care model.
The map below shows the coverage of the GP federations. In almost all cases, these directly match and overlay with borough areas.
Themes to model Description
Outpatient Activity Outpatient services which are reproved in an out of hospital setting, or have pathways
redesigned. (Influenced by SaHF targets)
Primary Care GPO practices which are relocated to hubs. Increase in Primary Care activity due to
other initiatives such as Integrated Care Planning.
Minor Surgery Minor Surgery to be provided as part of Primary Care activity and in addition potential to
remove some Elective Surgery into the community.
Proactive Integrated
Teams
Case Management, ACSC conditions, Falls Prevention, Integrated Care Planning,
Whole Systems
Reactive Integrated
Teams
Rapid Response, Intermediate Care, Early Discharge, Rehabilitation & Reablement
Mental health, Shifting
settings of care
Community Health Care -> Primary Care, and the extension of IAPT services
Moving existing
Community Services
Moving of existing community services e.g. Physio and other Therapies. This is in
addition to service provided to Multi disciplinary teams
Moving existing Mental
Health Services
Moving of existing Mental Health services where appropriate
Training & Education Provision of GP Teaching & Education space.
Independent Services e.g. Dentistry,
Local Authority Shared working space
Commercial Space e.g. Pharmacy

Document 5h
GP IT Capital Approval Process Guidance Document November 2014 7
Alongside federated arrangements the development of ‘hubs’ in each CCG will look to facilitate the delivery of new localised services based on local population need. The functions of the hubs are broadly to:
Manage the increased demand that cannot be met by the existing GP estate.
Provide an appropriate and flexible base from which those delivering services key to the new model of care can work - e.g. care navigators and co-ordination teams
Provide space for equipment and services moving into out of hospital settings - e.g. diagnostic equipment, space for consultant clinics, space for planned care procedures, accessible space for patient and carer education and self-care support programmes.
Considering new primary care organisational forms to deliver variety of services in new estates ‘hubs’ with new teams as a part of new care models and potentially emerging Accountable Care Organisations. Its important the digital and technology enablers and infrastructure support the future of primary care. Whilst primary care should make best use of the infrastructure already procured as part of the continual development of GP’s and their central role as being the coordinators of integrated health and social care working. However, there is much needed investment in helping local primary care to:
Understand their population health and needs
Understand digital requirements of new organsitional forms and estates to deliver care services
Understand digital opportunities to deliver care in different ways
Develop new information governance structures and process for digital sharing In NWL is the last few months there have been a surge of activity to support the above emerging requirements from Federations. However this requires a structured and managed arrangement to address local needs.
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 8
Approach and Deliverables:
There are broadly three work stream that will run concurrently to support the digital agenda for New Models of Primary Care:
Work stream 1: Smarter intelligence to support care delivery and population health
Gather, collate and assemble primary care intelligence to support local service planning for primary care.
Provide dashboard to support managing patient population as a part of federated arrangements
Provide dashboards to support better utilisation of local and national digital tools.
Provide local intelligence support to help with federation and hub development.
Create an infrastructure to support future provision of minimum datasets for new services to commissioners
Work stream 2: Local consultancy and strategic advice for Primary Care
Actively participate in the strategic discussions of the federations and networks to provide strategic advice to support their planning and future decision-making.
Support federations with developing the right enterprise and solution architecture for new operating models.
Support the development of any associated business case planning
Work with regional and national teams to support local areas to raise questions/issues
Design future information governance models with federations and hubs to support new ways of working and digital sharing
Workstream 3: Direct support to enable mobilisation of new models of care.
Delivery functionality based on existing clinical systems to support delivery of new services (i.e templates, protocols, referral wizards).
Provide data quality support to new services and federations to support constituent practices.
Develop required information sharing agreements to support federated working.
Short-term provide infrastructure to support hub mobilisation.
Benefits & Outcomes The benefits will support the early stages of the new organisational forms and functions to help future operating model and requirements for NWL primary care and are linked as enablers to the Primary Care Five Year Forward View.

Document 5h
GP IT Capital Approval Process Guidance Document November 2014 9
NON RECURRENT INVESTMENT (including VAT)
POTENTIAL NON CASH RELEASING SAVINGS
Enabling transformation of primary care.
PRIORITISATION OF PROJECTS
Realise the benefits of Digital CQUINs through ensuring readiness in
primary care
Improve patient safety
Improve productivity and efficiency with general practice
PROPOSED PROCUREMENT STRATEGY
This scheme will be delivered within 16/20. The procurement process will start once NHS England approves the funding. Procurement will follow Brent’s Standard Financial Instructions and NHS procurement rules.
KEY RISKS
Without investment to support the change, the challenge of an aging population and a shrinking budget will place unsustainable pressure on our health and social services. NWL CCGs want to reverse adverse health trends and reduce health inequalities. Shifting the balance of care away from the acute sector and moving care closer to home will help achieve this. It will also help professionals improve the way
Project NewModelsofPrimaryCare
SumofTotalincVAT ColumnLabels
RowLabels 16-17 17-18 18-19 19-20 GrandTotal
One-off £2,737,285 £2,004,255 £1,485,982 £1,618,491 £7,846,012
(P35)DevelopmentManager(band8A)-inclaccommodationcharges,trainingandexpenses £75,668 £77,938 £80,276 £233,881
(P35)ICTHubandNetworkDevelopmentLead/PM £101,250 £34,763 £136,013
(P36)BusinessAnalyst £78,750 £27,038 £105,788
(P37-P38)TemplateDesignandDeveloper £135,000 £46,350 £181,350
(P37-P39)Additional3xClincialSystemsDevelopers(band7)-inclaccommodationcharges,trainingandexpenses £272,439 £280,612 £289,030 £842,081
(P39)SystmOne/EMISSpecialist £78,750 £27,038 £105,788
(P46)Architect £123,750 £42,488 £166,238
(P47)BusinessAnalyst £78,750 £27,038 £105,788
(P48)SystmOne/EMISSpecialist £78,750 £27,038 £105,788
(P49-P51)SystemAnalytics&Reporting £202,500 £69,525 £272,025
1xWTEProgrammeLead(apportionedacross7projects)for12months £30,000 £30,000
1xWTEProgrammeSupport(apportionedacross7projects)for12months £16,071 £16,071
2xSeniorAnalyst(band8A) £145,879 £148,851 £153,316 £448,046
3rdpartydevelopmentandsupport £276,000 £284,280 £55,286 £146,404 £761,970
AnalystSupport(band5) £46,756 £48,159 £49,604 £144,519
ContractManager(band8A) £72,940 £74,425 £75,128 £222,493
DataAnalyst £223,767 £223,767
InformationSystemAdministrator £31,737 £31,737
InformationSystrmProgrammeManager £122,880 £122,880
DeploymentLead £174,262 £174,262
Deploymentsupport £39,423 £39,423
EMISEnterpriseSearch&Reports £21,734 £34,884 £35,931 £37,009 £129,558
GPDataExtractionService £144,000 £148,320 £152,770 £157,353 £602,442
Hostingandsupport £360,000 £370,800 £381,924 £393,382 £1,506,106
IGAdvice £14,400 £14,400
Legalfees £37,147 £19,131 £56,278
OfficeServices £24,750 £8,498 £33,248
PMcosts(hardwareandsoftwaretools) £15,840 £15,840
PRIMIStools £44,400 £91,464 £94,208 £97,034 £327,106
ProductManager(band8C) £27,561 £85,165 £87,720 £90,351 £290,797
ServiceDeskSupport(band5) £46,756 £48,159 £49,604 £144,519
Servicesupport £68,188 £68,188
PCAnalyticsLead £77,944 £77,944
PCFinanceLead £77,944 £77,944
PCProjectSupportOfficer £31,737 £31,737
GrandTotal £2,737,285 £2,004,255 £1,485,982 £1,618,491 £7,846,012
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 10
complex and long term conditions are managed.
ENDORSED BY: Director of Finance
The DoF must physically sign each PID
Organisation
Date
APPROVED BY: Head of Financial Management NHSE (London Region)
Document 5h
GP IT Capital Approval Process Guidance Document November 2014 11
For Official Use Only
INVESTMENT PANEL DECISION (For NHS England SS&T P&I Regional Investment Panel use)
Please document the decision made and provide supporting reasons for approving or rejecting the scheme. Please demonstrate where appropriate that acceptance of the scheme is a fair investment to support equitable and consistent progress towards standards and strategic system deployment within the region. Please document that all capital rules and any associated local governance arrangements have been adhered to.
For Official Use Only
FINAL CENTRAL SS&T P&I DIRECTORATE ASSURANCE (For NHS England Central SS&T P&I Assurance Group use)
Please document that the NHS England Central SST P&I Assurance Group is assured that the scheme is aligned with operational and strategic objectives, capital rules, and any constraints itemised within the GP IT operating model.
Provide supporting main reasons for approving or rejecting the scheme.
For Official Use Only
NHS ENGLAND CHIEF FINANCIAL OFFICER APPROVAL (For NHS England Finance PAU team use)
Please document whether approval given by Chief Financial Officer.
Cover Sheet: Primary care co-commissioning joint committees
Date Thursday, 16 June 2016
Presenter Emma Taylor (Collaboration Governance Manager, North West Collaboration of CCGs)
Authors Christopher Cotton (Primary care transformation lead, North West Collaboration of CCGs)
Emma Taylor (Collaboration Governance Manager, North West Collaboration of CCGs)
Ben Westmancott (Director of Compliance, CWHHE CCGs)
Responsible Directors Rob Larkman (SRO for Primary care transformation, North West London Collaboration of CCGs)
Matthew Hannant (Acting Director of Strategy and Transformation, North West Collaboration of CCGs)
Liz Wise (Director of Primary Care Commissioning, NHS England (London))
Clinical Lead Dr Amol Kelshiker and Dr Ruth O’Hare (NWL clinical co-leads for primary care transformation)
Confidential Yes ☐ No Items are only confidential if this is in the public interest
The Joint Committees are asked to:
endorse the revised co-commissioning terms of reference, for approval by the CCGs’ governing bodies.
Summary of purpose and scope of report
The current terms of reference contain a provision for them to be revisited after six months of operation. They were approved by governing bodies in November 2015 and this current co-commissioning meeting in common is the first one following this six-month mark.
The changes proposed in this paper do not fundamentally change the operation of the NWL joint committees, whether meeting locally or in common. Rather, they reflect:
the CCGs’ experience of running the co-commissioning local meetings and meetings in common;
new national guidance on the management of conflicts of interest; and
advice received by Capstix (legal advisors) on how to make the terms of reference more robust.
The changes proposed by the CCGs’ governance leads and the secretariat for the meeting in common have been circulated twice for comment to all members of the eight NWL joint committees as well as their non-voting advisors. The version attached here reflects the comments received back.
This draft will, if endorsed by the joint committees, then proceed for approval by the CCGs’ governing bodies. The secretariat and CCGs’ governance teams recognise that some localisation might take place at this stage, as in November 2015.
Paper title Primary care co-commissioning governance
Paper number 6
Quality & Safety/ Patient Engagement/ Impact on patient services:
Co-commissioning determines how primary care medical services are delivered in North West London. Functioning terms of reference underpin effective and transparent decision-making, which in turn support the joint committees’ ability to make decisions in the best interests of local people.
The terms of reference continue to state the commitment of the CCGs and NHS England to reflecting the voice of local patients in the work of the joint committees.
Finance, resources and QIPP
The changes to the existing terms of reference seek do not have a material impact on finance or QIPP. It is possible that the additional provisions surrounding conflicts of interests will require more involvement from the lay committee chairs and CCG governance teams, but this will be in line with the impact of new national guidance on conflict of interest management over the rest of the CCGs’ activities.
Equality / Human Rights / Privacy impact analysis
No analysis has been undertaken for this report.
Risk Mitigating actions
The equitable functioning of co-commissioning across NWL requires each joint committee to possess standard terms of reference – with the risk that the proposed revisions might not be accepted by all joint committees and then all governing bodies.
The proposed revisions have been formulated by the CCGs and NHS England.
Supporting documents
Document 6a: Primary care co-commissioning: joint committee with NHS England, proposed revised terms of reference
Governance and reporting
(list committees, groups, and any other bodies that have discussed this paper)
The changes proposed by the CCGs’ governance leads and the secretariat for the meeting in common have been circulated twice for comment to all members of the eight NWL joint committees as well as their non-voting advisors. The version attached here reflects the comments received back.

Document 6a
1
Primary care co-commissioning: joint committee with NHS England
Proposed revised terms of reference – June 2016
Preamble
The CCG has formed a primary care co-commissioning committee jointly with NHS England,
according to these terms of reference, which is known as the ‘joint committee’.
The CCG’s joint committee will meet regularly to discuss and take decisions on local primary care
issues.
The other seven CCGs in North West London have formed the equivalent joint committees with NHS
England.
In addition to meeting locally, where there are common strategic issues to be discussed across North
West London in cases where a shared approach would be beneficial, the eight joint committees are
able to meet in common, instead of holding eight separate meetings. A ‘meeting in common’
effectively means that all eight joint committees will meet at the same time and place, to the same
agenda, and be presided over by a lay chair for the purpose of managing the meeting. It is important
to note that each CCG’s joint committee retains individual decision-making authority when meeting in
common. This means that the joint committees will take decisions separately, based on their own
relevant considerations. No CCG can bind another.
The eight North West London CCGs whose joint committees will form the meeting in common are:
Central London CCG, West London CCG, Hammersmith and Fulham CCG, Hounslow CCG, and
Ealing CCG (together the CWHHE Collaborative of CCGs) and Brent CCG, Harrow CCG, and
Hillingdon CCG (together, the BHH Federation of CCGs).
At all times, the CCG and NHS England are committed to ensuring that the public voice is reflected in
the decisions taken through primary care co-commissioning. This is enabled firstly through the
membership of the joint committee and secondly through the intrinsic approach taken to the
development of key areas of business to be dealt with, as per the NHS operating framework which
requires public and patient engagement.
Terms of reference
The National Health Service Act 2006 (as amended) (“NHS Act”) provides, at section 13Z, that NHS
England’s functions may be exercised jointly with a CCG, and that functions exercised jointly in
accordance with that section may be exercised by a Joint Committee of NHS England and the CCG.
Section 13Z of the NHS Act further provides that arrangements made under that section may be on
such terms and conditions as may be agreed between NHS England and the CCG.
Purpose The CCG has entered into joint arrangements known as ‘primary care co-
commissioning’, with NHS England, which are designed to enable the CCG to
better influence the development of local primary care.
Primary care co-commissioning will enable the CCG to ensure that primary care
acts as a driver for ambitious plans to transform the local health and care
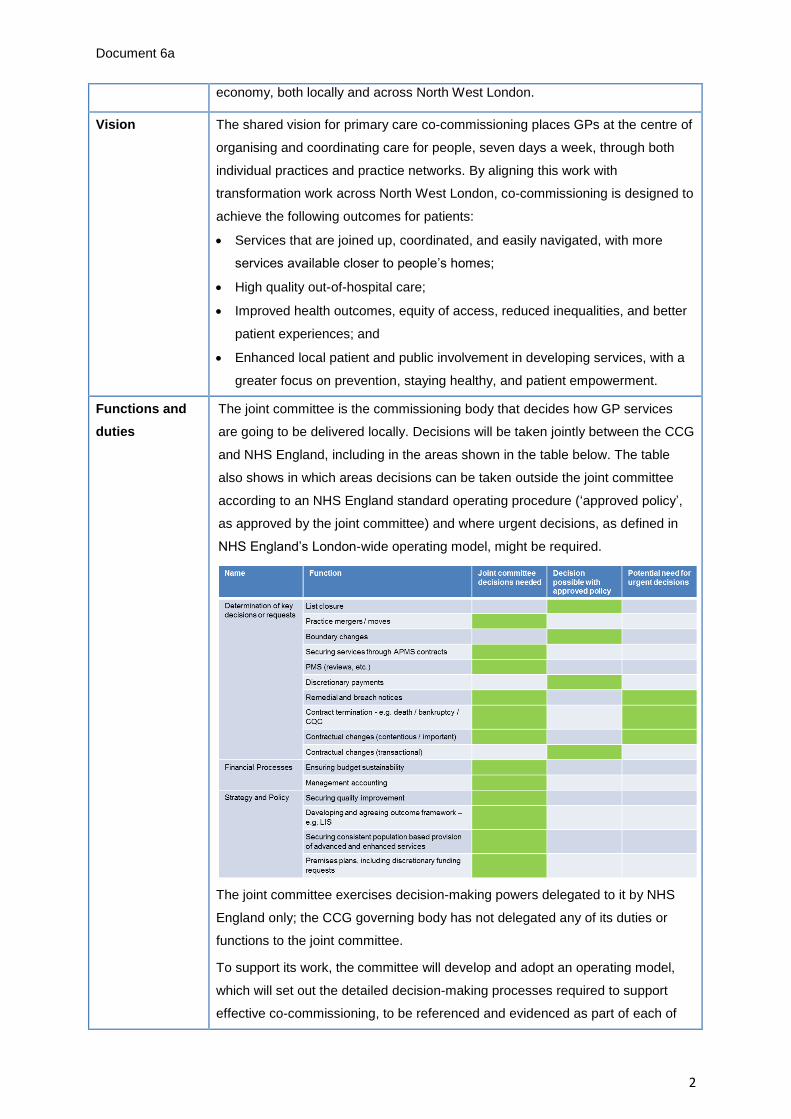
Document 6a
2
economy, both locally and across North West London.
Vision The shared vision for primary care co-commissioning places GPs at the centre of
organising and coordinating care for people, seven days a week, through both
individual practices and practice networks. By aligning this work with
transformation work across North West London, co-commissioning is designed to
achieve the following outcomes for patients:
Services that are joined up, coordinated, and easily navigated, with more
services available closer to people’s homes;
High quality out-of-hospital care;
Improved health outcomes, equity of access, reduced inequalities, and better
patient experiences; and
Enhanced local patient and public involvement in developing services, with a
greater focus on prevention, staying healthy, and patient empowerment.
Functions and
duties
The joint committee is the commissioning body that decides how GP services
are going to be delivered locally. Decisions will be taken jointly between the CCG
and NHS England, including in the areas shown in the table below. The table
also shows in which areas decisions can be taken outside the joint committee
according to an NHS England standard operating procedure (‘approved policy’,
as approved by the joint committee) and where urgent decisions, as defined in
NHS England’s London-wide operating model, might be required.
The joint committee exercises decision-making powers delegated to it by NHS
England only; the CCG governing body has not delegated any of its duties or
functions to the joint committee.
To support its work, the committee will develop and adopt an operating model,
which will set out the detailed decision-making processes required to support
effective co-commissioning, to be referenced and evidenced as part of each of

Document 6a
3
the relevant business areas dealt with at the meetings. The table above is taken
from NHS England’s London-wide operating model.
Joint committees’ meeting in common
The NWL CCGs have agreed that decisions on issues affecting more than one
CCG will be taken at the meeting in common. These will relate mostly to
longer-term strategic issues relevant across NWL. These issues will be
identified by the NWL CCGs’ staff and NHS England, who will co-ordinate the
business to be dealt with at the local meetings and the meetings in common.
Local meetings will also be able to pass decisions up to the meeting in common
where they consider this to be appropriate.
The following additional detail has been agreed by the North West London CCGs
with NHS England and Londonwide LMCs:
The joint committees will review and agree the framework by which
contract and contract performance management will be undertaken. A
memorandum of understanding between the joint committee, performance
directorate and contracting team will make explicit the duties and
responsibilities of all parties in contract and performance management.
NHS England will conduct routine contract management of GMS, PMS
and APMS contracts as before, together with offering and monitoring
delivery of Directed Enhanced Services. Where issues are identified, this
will include liaison with practices, development of appropriate action or
improvement plans, and then monitoring delivery of these plans. The joint
committee will receive aggregate reports on this routine contract and
performance management.
Where necessary, the NHS England contracting team will prepare and
present papers with recommendations to the joint committee for individual
practice sanction for non-delivery of its contractual obligations. This
includes making the case for a sanction (with the gathering of appropriate
data), plus liaison with the provider and representative organisations.
These individual cases might be considered in private session. GP
members of the joint committee will not normally be part of the decision-
making process about individual contracts.*
The joint committee will have no part in individual practitioner performance
management, revalidation and appraisal processes relating to being
included on the National Performers List.
The joint committee will be required to implement NHS England policy (for
instance, the PMS review and MPIG redistribution) and also to action
national changes to contracts negotiated with the GPC. The joint
committee is also empowered to undertake additional work required to
meet the needs of their local populations. This includes designing local

Document 6a
4
incentive schemes as an alternative to QOF, designing new extended
scope services (locally commissioned services), and enhancing locally
agreed contract terms to deliver the out-of-hospital agenda.
CCGs’ involvement with contract and performance management through
co-commissioning is aligned with their existing roles, given their statutory
duty to support NHS England to improve the quality of primary care.
LMCs will be fully consulted on all aspects of these developments.
* Further information on the management of conflicts of interest is below.
Membership The joint committee comprises the following voting members:
CCG non-audit lay member (also the joint committee lay chair);
CCG lay audit committee chair;
CCG chair;
CCG additional GP;
CCG accountable officer;
CCG managing director / chief operating officer;
CCG chief financial officer or deputy chief financial officer;
CCG secondary care governing body member;
CCG nurse governing body member;
NHS England director of primary care commissioning (London);
NHS England director of commissioning and operations (NW London);
NHS England Head of primary care (NW London);
NHS England assistant medical director (London); and
NHS England medical director (NW London).
Committee members may nominate a suitable deputy when necessary. All
deputies should be fully briefed and the secretariat informed of any agreement to
deputise so that quoracy (see below) can be maintained. Deputies exercise the
voting rights of those for whom they are deputising.
The deputy chair of the audit committee (or in exceptional circumstances,
another lay member from the CCG) may deputise for the lay audit committee
chair and may represent more than one CCG.
No person can act in more than one role on the joint committee, meaning that
each deputy needs to be an additional person from outside the joint committee
membership.
Governing body papers detailing joint committee decisions will list the members
and deputies present.
Document 6a
5
The chair Joint committee meeting (local only)
The CCG’s non-audit lay member (or
deputy) will chair local meetings of the
joint committee.
Joint committees’ meeting in common
The eight joint committees shall elect
two non-audit lay (i.e. non-clinical, non-
executive) co-chairs to preside over
alternate meetings in common. One
co-chair will be from the CWHHE
Collaborative of CCGs and one from
the BHH Federation of CCGS. These
roles do not possess any voting rights
in respect of the meeting in common;
when the joint committees are meeting
in this format, the chair of each joint
committee retains the same degree of
authority as when the joint committees
meet locally.
Each of the joint committee’s non-lay
audit chairs will be eligible to put
themselves forward for the role of co-
chair of the meeting in common.
Voting The committee will aim to make decisions by consensus wherever possible.
Where this is not achieved, a voting method will be used. The voting power of
each individual present will be weighted so that each party (CCG and NHS
England) possesses 50% of total voting power.
In cases where a vote has not determined an outright decision, the lay joint
committee chair will have a second vote.
Subsequent to the final vote being carried by the committee and recorded by the
secretariat, NHS England retains the right to exercise an overriding casting vote
in respect of functions within its statutory obligations. (The CCG has not
delegated any of its statutory functions to the joint committee.)
At the meetings in common, the eight joint committees will resolve into their
individual committees to vote. The process outlined above then applies to each
joint committee.
The numbers of weighted votes shall be recorded and announced by the
secretariat.
Quorum The joint committee can take decisions with a quorum of:
one lay member;
one CCG officer;
one NHS England officer;
one GP; and
Document 6a
6
a second clinician.
At least two permanent (i.e. not deputy) members shall be present.
If all clinicians present are conflicted and thus precluded from voting, the quoracy
requirement for a GP and second clinician will be suspended for the relevant
decision(s).
Joint committees’ meeting in common
For the purpose of the joint committees’ meetings in common, the same person
may be counted towards the quorum for more than one CCG joint committee but
cannot count more than once for an individual joint committee.
Non-voting
advisors
At all times, non-voting advisors have full speaking rights. They will receive
papers at the same time as joint committee members.
The joint committee may call additional experts to attend on an ad hoc basis.
Health and Wellbeing Board
The Health and Wellbeing Board is entitled to send a representative to all
meetings of the joint committee to act as a non-voting advisor.
Healthwatch
The Healthwatch committee is entitled to send a representative to all meetings of
the joint committee to act as a non-voting advisor.
Joint committee local meetings
The joint committee is able to appoint
any number of non-voting advisors to
inform discussions at its local
meetings. The joint committee will
determine which, if any, of these
advisors should attend parts of local
joint committee meetings otherwise
reserved for voting members only.
The LMC is invited to send a
representative to each joint committee
meeting.
Joint committees’ meeting in common
Healthwatch
The eight NWL Healthwatch
committees are invited to elect two
representatives (one from the CWHHE
boroughs and one from the BHH
boroughs) to attend the joint
committees’ meeting in common as
non-voting advisors. This is proposed
as an alternative to representation from
each local Healthwatch committee.
Londonwide Local Medical
Committees (LLMCs) Londonwide
LMCs is invited to nominate two
representatives to attend the joint
committees’ meeting in common as
non-voting advisers, representing GPs
as providers and performers (GP
status) and bringing local and clinical
expertise to discussions.

Document 6a
7
The LLMCs’ non-voting advisors are
invited to attend parts of the meetings
in common otherwise reserved only for
voting members, though the joint
committees do reserve the right to
reserve time solely for voting members
when required.
Strategy and Transformation
The Director of Strategy and
Transformation from the NWL
Collaboration of CCGs, or their
nominated representative, is a non-
voting advisor to the joint committees’
meetings in common.
The CWHHE CCGs’ Director of
Compliance and the BHH CGGs’ Head
of Governance, or their nominated
representatives, are non-voting
advisors to the joint committees’
meetings in common.
Frequency of
meetings
Joint committee meeting (local only)
The joint committee will meet monthly,
or as required.
Joint committees’ meeting in common
The joint committees will meet in
common quarterly, or as required.
Operation of the
joint committee
The secretariat function for the joint committee will be provided by:
the North West London CCGs’ shared staff for the joint committees’
meetings in common; and
the CCG staff for the joint committee’s local meetings.
In both cases, the secretariat is responsible for giving notice of meetings and
distributing an agenda and supporting papers to each member and non-voting
advisor no later than seven days before any meeting. The secretariat will also:
circulate the minutes of the joint committee; and
present these minutes to NHS England and the CCG.
Joint committee meeting (local only)
When the chair of the joint committee
deems it necessary, in light of urgent
circumstances, to call a meeting at short
notice, at least forty-eight hours’ notice
shall be given, unless a quorum of
Joint committees’ meeting in common
When the co-chairs of the meeting of
the joint committees in common
deems it necessary, together with the
respective chairs of the joint
committees, in light of urgent
Document 6a
8
members agree that earlier is
acceptable.
circumstances, to call a meeting at
short notice, at least forty-eight hours’
notice shall be given, unless a
quorum of members in each joint
committee agree that earlier is
acceptable.
Public input
into, and
transparency of,
decision-
making
The joint committee will demonstrate its transparency to local people, as well as
the CCG and NHS England, by:
meeting in public, both when meeting locally and when meeting in common;
including representation from Healthwatch, the Health and Wellbeing Board,
and LLMCs;
publishing its papers;
publishing these terms of reference;
publishing minutes for the CCG and the public domain;
publishing any joint strategies agreed; and
complying with NHSE guidance and with generally accepted principles of
good governance.
Information regarding the work of the joint committee will be made available to
the public through the CCG website.
Members of the public will be able to observe all of the joint committee’s
meetings (both local meetings and meetings in common) and to submit in
advance of each meeting questions related to the agenda items, which will be
addressed during proceedings. Members of the public do not have speaking
rights at meetings of the joint committees, which are meetings in public rather
than public meetings.
The Joint Committee may resolve to exclude the public from a meeting that is
open to the public (whether during the whole or part of the proceedings)
whenever publicity would be prejudicial to the public interest by reason of the
confidential nature of the business to be transacted or for other special reasons
stated in the resolution and arising from the nature of that business or of the
proceedings or for any other reason permitted by the Public Bodies (Admission to
Meetings) Act 1960 as amended or succeeded from time to time. The joint
committee may also reserve part of its meetings (both local meetings and
meetings and in common) for voting members only.
Managing
conflicts of
interest
The joint committee will manage conflicts of interest through its lay/executive
majority and appointment of a lay chair.
All members will provide an entry for the CCG’s register of interests.
Any additional declarations relevant to agenda items will be made during
meetings.

Document 6a
9
The lay chair and secretariat shall, as part of developing meeting agendas,
monitor potential conflicts of interests and agree an appropriate strategy for
handing any conflicts identified. They will seek the advice of the governance lead
and then (pending confirmation of new NHS England guidance) the conflict of
interest guardian where appropriate. The CCG’s primary care management lead
will also offer advice as required, as the agenda and papers are developed.
Members of the joint committee are required to inform the chair and secretariat of
all potential conflicts of interest, real and perceived, at the earliest opportunity.
All members shall act in accordance with their own organisation’s conflict of
interest policy and code of conduct.
Terms of
reference review
These terms of reference will be formally reviewed by NHS England and the
CCG after three months of operation and then in April of each year, following the
year in which the joint committee is created, in order for any necessary changes
to be made. They may be amended by mutual agreement between the parties at
any time to reflect changes in circumstances.
There will be no move to delegated co-commissioning without the explicit
approval of the CCG’s member practices.
Self-evaluation
of the joint
committee and
its meeting in
common with
other joint
committees
The joint committee shall, at least annually, review its own performance and
membership. This review will reflect experience of the joint committee in fulfilling
its functions and the wider experience of NHS England and the CCG in co-
commissioning.
Process for
reaching
agreement
All parties are committed to working together in a collaborative way.
Where decisions are required, agreement shall be reached by demonstrable
consensus of all non-conflicted members.
In the event that the non-conflicted voting members are unable to reach a clear
consensus at the end of discussion, the decision shall be reached by an open
vote. The process for this is described above.
At all times, the CCG will act in accordance with the terms of its constitution and
NHS England will act in accordance with the terms of its establishment.
No decision outcome shall impede any organisation in the fulfilment of its
statutory duties.
Withdrawal from
joint co-
commissioning
Withdrawal from co-commissioning may be through mutual agreement between
the CCG and NHS England, with six months’ notice given to all parties.