Do Novel Antipsychotics Improve Cognition? A Report...
7
Richard S. E. Keefe, PhD; Anna M. Bollini, BA; and Susan G. Silva, PhD II 623 with non-schizophrenic individuals his age. In addition, his ability to categorize information, make decisions, and construct plans is poor, with scores in the bottom 10%, compared with normal individuals. Tests show that his attention and verbal memory are also substandard, with scores in the bottom 10% to 15%, compared with normal individuals. Anyone involved in Sebastian's treatment would be concerned about these cogni- tive deficits and would be inclined to ask the fol- lowing questions: To what degree do these cogni- tive deficits affect Sebastian's life? Are they a result of his other symptoms of schizophrenia, such as his negative symptoms, or are they inde- pendent, warranting a treatment regimen aimed specifically at ameliorating them? Are medica- tions available to treat these cognitive deficits? Will the improvements caused by these medica- tions be clinically meaningful? What changes can Sebastian and his physician expect? It is important to consider these questions because they concern areas that are central to the quality of life of individuals with schizophrenia. As reviewed by Green et al., 1 cognitive impair- ment in schizophrenia is strongly related to poor outcome and poor everyday functioning. Employment status is strongly related to perfor- mance on cognitive tests (5. McGurk and H. Meltzer, unpublished data, April 16, 1999). Many studies conducted during the past 40 years have addressed the question of whether typical Pharmacologic Treatments In Schizophrenia and Their Effect on Cognitive Function Do Novel Antipsychotics Improve Cognition? A Report of a Meta-Analysis 5 ebnstinn is 28 yenrs old nnd hns cllrollic scllizo- pllrellin. Five yenrs ngo lie moved from Cllile to New York City, where he becnme n tnxi driver. After n few mOlltlls, he begnn to experience nnxiety ns n reslllt of tile elmo tic traffic, 1'IIde pnssellgers, nlld lIis demnnding boss. He tried to sclledllie lIis sllifts so tllnt he cOllld nvoid working dllring the TIIsllllollrs, bllt lie still fOlllld lIimself overcome with stress. III ndditioll to lIis growing nllxiehj, Sebnstinll wns IInving problellls remelllberillg the pnssellgers' destillntions nlld plnll- lIing which rOllte wns the most time nlld distmlce effi- ciellt. Twice lIe mil throllgh red ligllts becallse he wns 1I0t pnyillg nttelltioll to his drivillg. MnllY pnssengers felt elldmlgered mId botllered by lIis circllitolls rolltes. Several complnilled to lIis employer or refllsed to pny the fnre. After 6 mOllths, Sebnstiml wns fired. He sOllgllt employmellt nt otller tnxi compnllies, bllt fOlllld tlmt lie lind tile snllle difficllities drivillg for them mId evelltllnlly gnve lip drivillg n tnxi altogether. Like many patients with schizophrenia, Sebastian has significant cognitive deficits. A neu- ropsychological testing battery suggests that his working memory, which refers to his ability to keep information in mind during brief periods of time, is poor, falling in the bottom 25%, compared Alf of the RUIl,Ors till! from tilt Dt-pnrfmcllf of Psyclrinfry alld Ddmvioral Sowers, OlLke Ullitli!rsity Mt'rlical Cellter. DllrllCllll, Nartll Carolina. Address reprint rrquests 10 Riclmrd KC:l'fl!. PliO. Box 3270, Duke U,Jivtrsify Medical DurJllJlII, NC 27710. Dr. &I'fe's n:senrdl aclivilies are s1mllsorcd by Eli Lilly ami COlli/HIllY alld Jill/SSW. He is I' ,mid cOI/SIIIlrml to Jallssell, Eli Lilly and COIII/'alIY. ami Wyeth-Ayasl.
Transcript of Do Novel Antipsychotics Improve Cognition? A Report...

Richard S. E. Keefe, PhD; Anna M. Bollini, BA; and Susan G. Silva, PhD
II
623
with non-schizophrenic individuals his age. Inaddition, his ability to categorize information,make decisions, and construct plans is poor, withscores in the bottom 10%, compared with normalindividuals. Tests show that his attention andverbal memory are also substandard, with scoresin the bottom 10% to 15%, compared with normalindividuals. Anyone involved in Sebastian'streatment would be concerned about these cognitive deficits and would be inclined to ask the following questions: To what degree do these cognitive deficits affect Sebastian's life? Are they aresult of his other symptoms of schizophrenia,such as his negative symptoms, or are they independent, warranting a treatment regimen aimedspecifically at ameliorating them? Are medications available to treat these cognitive deficits?Will the improvements caused by these medications be clinically meaningful? What changes canSebastian and his physician expect?
It is important to consider these questionsbecause they concern areas that are central to thequality of life of individuals with schizophrenia.As reviewed by Green et al.,1 cognitive impairment in schizophrenia is strongly related to pooroutcome and poor everyday functioning.Employment status is strongly related to performance on cognitive tests (5. McGurk and H.Meltzer, unpublished data, April 16, 1999). Manystudies conducted during the past 40 years haveaddressed the question of whether typical
Pharmacologic Treatments InSchizophrenia and Their
Effect on Cognitive Function
Do Novel AntipsychoticsImprove Cognition? A Reportof a Meta-Analysis
5ebnstinn is 28 yenrs old nnd hns cllrollic scllizopllrellin. Five yenrs ngo lie moved from Cllile toNew York City, where he becnme n tnxi driver.
After nfew mOlltlls, he begnn to experience nnxiety nsn reslllt of tile elmotic traffic, 1'IIde pnssellgers, nlld lIisdemnnding boss. He tried to sclledllie lIis sllifts so tllnthe cOllld nvoid working dllring the TIIsllllollrs, bllt liestill fOlllld lIimselfovercome with stress. III ndditioll tolIis growing nllxiehj, Sebnstinll wns IInving problelllsremelllberillg the pnssellgers' destillntions nlld plnlllIing which rOllte wns the most time nlld distmlce efficiellt. Twice lIe mil throllgh red ligllts becallse he wns1I0t pnyillg nttelltioll to his drivillg. MnllY pnssengersfelt elldmlgered mId botllered by lIis circllitolls rolltes.Several complnilled to lIis employer or refllsed to pnythe fnre. After 6 mOllths, Sebnstiml wns fired. HesOllgllt employmellt nt otller tnxi compnllies, bllt fOlllldtlmt lie lind tile snllle difficllities drivillg for them mIdevelltllnlly gnve lip drivillg n tnxi altogether.
Like many patients with schizophrenia,Sebastian has significant cognitive deficits. A neuropsychological testing battery suggests that hisworking memory, which refers to his ability tokeep information in mind during brief periods oftime, is poor, falling in the bottom 25%, compared
Alf of the RUIl,Ors till! from tilt Dt-pnrfmcllf of Psyclrinfry alld DdmvioralSowers, OlLke Ullitli!rsity Mt'rlical Cellter. DllrllCllll, Nartll Carolina. Addressreprint rrquests 10 Riclmrd KC:l'fl!. PliO. Box 3270, Duke U,Jivtrsify MedicalG~IJ'er. DurJllJlII, NC 27710.
Dr. &I'fe's n:senrdl aclivilies are s1mllsorcd by Eli Lilly ami COlli/HIllY alldJill/SSW. He is I' ,mid cOI/SIIIlrml to Jallssell, Eli Lilly and COIII/'alIY. amiWyeth-Ayasl.

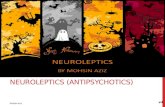
TABLE 1
'" I Methodologies of 15 Studies of the Effect of Novel Antipsychotic Medication on Cognitive Functions in Patients WithN·...Schizophrenia
BaselineNeuro- Assessment
cognitive Multiple Neura- of Neuro-
Assessment Arms With Daily cognitive cognitive/Diagnosis of (Medication Random Study Medication Test Sample Clinical
Subjects Status) Assignment Duration Doses Batteries Size Relationships
Double-blind studies (N =3)
Meyer-Lindenberg Treatment- Yes Yes Testing at Clozapine: Maze tests only 26 No
"et al./ 1997 resistant (4-day day 2, then 150-450 mg; c
schizophrenia washout) weekly for zotepine: '"c6 weeks 150-450 mg '"'"Buchanan et aJ.,8 Treatment- Yes Yes 10 weeks Clozapine: 400 mg 4 cognitive 9 subjects Yes
.,..(fluphenaziiie domains in each
..1994 (phase i) responsive (200-600); '"schizophrenia hydrochloride) haloperidol:
..group :;
'- 20 mg (10-30) "" 0<
Green et a1. /1 1997; Treatment- Yes .--Yes 4 weeks Risperidone: 6 mg; 4 domains over- 59 Yes ~
=McGurk et al.,9 1997; resistant (3- to 7-day haloperidol: 15 mg all; 2 measures c..and Kern et aL, 10 1999 schizophrenia washout per publication ~
following "3-week "'U
~ haloperidol '"~C0< stabilization) '"n'":I:
;; ~
c-< Open-iabel studies (N =12) ~~
'"n Goldberg et al.,l1 1993 Psychotic Yes No 3-24 months; (Iozapine; many 9 domains 15 No :;» disorders (conventional mean = 15 adjunctive ;;zz antipsychotic) months medications '"» '0~ Hagger et al.,12 1993 Treatment- Yes (27 drug No 6 weeks; Clozapine: 6 domains 36 Yes~
N resistant free; 5 typicals; 6 months; 363 ± 11 mg for~
schizophrenia 4 1-3 days of 1 year 6 weeks, 403 ± 208
z dozapine) mg for 6 months0 Buchanan et al.,8 Treatment- Yes No 1 year Clozapine: 3 domains 33 Yes<m 1994 (phase II) responsive (fluphenazine 200-600 mgs:~ schizophrenia hydrochloride)m~ Lee et aJ., 13 1994 Treatment- Yes Yes 6 weeks; Not available 6 domains Conven- Yes-~ responsive 6 months; tiona I =23;~
~ schizophrenia 1 year c10zapine =24
l~;Jt,,;,'<';..;.";'·';C;:r;.-~it4~.t':":~,#1"~'."::"~~~~~"'i"'~ :~:a_ ~ l;;-: _. :-'..;..:~=-,:,,:,-;-;-~ L -~'.~~,~'.'" ~ .,;-~~~ . -;::~.l:'~~_~- ~~.~ ~:;.;o:'~;~.;:...;....:.-:.::~._ ..;.,,~.~:~..,.. '_ . ""~"""., '. ,.--.o:.r..--j.·. ; ....~ ~.,~ .....I!'- .. -..:<.- ...............

~
-;".~_:'~.~r:·~;~~-: ' . - l
;."~~:;.~:i.~'~, ':'~i";'~ ~~6-~:r,U". .~,,,,,,,,,
'"'' ... I ••• ~ ~ .. - "" '''':w.::t''~.=-~-. '-" . ~-
.~ =- ~. , - - -:~'_.~~ .:;t,"T ':':-":':"':""~' '•- ~ or; ,... " . ..~- - _.,
Zahn et al.,l-I 1994 Schizophrenia Yo' No 6 weeks Fluphenazine hydro- 2 tests 25 No.~
~ (fluphenazine each phase chloride: mean = 23 hallucln-~
n hydrochloride ± 14.8 mg; c1ozapine: ations0:
or placebo) mean = 444 ± 189 mg only» --< Gallhofer et al.,1S 1996 Schizophrenia No No 7 days C1ozapine: Maze tests only 16 No~,
- 20D-400 mg; i.-n» risperidone: 4-8 mg; Iz haloperidol: 3-15 mg;z» fluphenazine hydro-r~ chloride: 6-24 mgN
Hoff et al.,16 1996~ Treatment- Yes No 12 weeks Baseline CPZ 10 domains 20 Yesresistant (conventional equivalents: ""
z schizophrenia neuroleptic) 1.418 ± 809; z0 c1ozapine: "c:< 425-900 mg.
...m '";: mean = 668 ± 164 ..w Zm
Stip and lussier,17 1996 Schizophrenia Yes No 8 weeks; Haloperidol: 3 domains 13 Minimal; ..~
(conventional 20-30 weeks 1 patient-40 mg; correia- '"'"~
I ..~ neuroleptic) risperidone: tions '"~
with '"1 patient-ll mg. "2 patients-1 0 mg 8PRS..'"and '"
PANSS s:total '".,scores "c:
Rossi et a1.,18 1997 Schizophrenia Yes No 4 weeks Risperidone: 2 mg 3 tests 30 Yes ...'"(1 week placebo) "'"Serper and ChOU,19 1997 Schizophrenia Yes No 4 weeks CPZ equivalents: 3 measures Atypical = 9; No z
(medication free; 827 ± 528 mg; typical ='2 .."time period ziprazidone:"N/A; z
unknown) aripiprazole: N/A.•
Galletly et al.,20 1997 Schizophrenia Yes No 6.5 ± 2.0 Clozapine: 7 domains 19 Yes(1 medication months mean = 393 ±free; 4 risperi- 182 mgdone; 14 con-ventionals)
Fujii et al./ I 1997 Treatment- Yes No 12-16 months Clozapine: 7 domains 10 Noresistant (conventional 250-900 mg.schizophrenia neuroleptics) mean:=:: 643
'" ICI'Z - elliorymlllla:.iut; BrRS - Bnef Psycll;atric Rntill8 Sea/(; l'ANSS • l'osiliVf amI Nrgative SYlldml1lr Srair; NIA - nnt ltUllil,d'/r,N
'"
__"_-"'----=-3._---,

DO NOVEL ANTIPSYCHOTICS IMPROVE COGNITION?
il
Long-term treatment withconventional antipsychoticmedications improvessymptoms, but appears tohave limited cognitivebenefits.
antipsychotics improve cognitive function inpatients with schizophrenia. Numerous literaturereviews, including a recent review of data collected during the past 9 years,' have arrived at thesame basic conclusions: long~term treatmentwith conventional antipsychotic medicationsimproves symptoms, but appears to have limitedcognitive benefits. In fact, the literature examining the cognitive effects of typical antipsychoticsprovides some of the clearest demonstrations ofthe recalcitrant nature of cognitive impairmentdespite symptom change. The results of several
Ystudies may be interpreted to suggest that typical
",ntipsychotic medications actually prevent adequate learning effects and worsen motor skills,'memory function,' and executive abilities, suchas problem solving and performance assessment.s
META-ANALYSIS METHODSThe advent of novel antipsychotics has moti
vated researchers to examine how these medications affect cognitive impairments comparedwith conventional medications. To address tmsquestion empirically, a meta-analysis was conducted including the 15 studies that, as of June30, 1998, had investigated the impact of novelantipsychotic medication on cognitive dysfunction in patients with schizophrenia.' The methodology used in each of the 15 studies is listed inTable 1. The analysis was not restricted to studiesinvestigating a particular novel antipsychoticmedication. Three of the studies were random"ized and double-blind, and 11 were open-label
626
studies. In 1 study!" the patients who receivednovel antipsychotics and a portion of the patientswho received haloperidol were assessed in adouble-blind manner; however, several of thepatients who received haloperidol were not. Oneof the open-label studies" used multiple studyarms with random assignment. The numbers ofstudies that included the various novel antipsychotics are as follows: clozapine, 11; risperidone,4; zotepine, 1; ziprazidone, 1; and aripiprazole, 1.
The 15 studies used a wide range of test measures. Some studies examined only a fe"; neurocognitive measures, whereas others conducteda more com prehensive neuropsychologicalassessment. The number of different neurocognitive tests given to subjects ranged from 1 to 13.Because of the variability in the type and thenumber of measures used to assess neurocognitive effects, test results were grouped into the following categories: (1) attention subprocesses; (2)executive function; (3) working memory; (4)learning and memory; (5) visuospatial analysis;(6) verbal fluency; (7) digit symbol substitution;and (8) fine motor function.
Each study was examined to determineimprovement in performance on a Single testafter treatment with novel antipsychotic medication compared with after conventional antipsychotic treatment (atypical vs typical) or a significant positive change in performance aftertreatment with novel antipsychotic medicationrelative to baseline. Our definition of improvement was conservative. We corrected for multiplecomparisons in each study using an experimentwise P value of less than .05, even if the studyauthors did not complete this statistical procedure. For instance, if 10 measures were reportedin a study, we assigned a significance criterion of.05 /10 ~ .005 for each measure.
The cognitive domains in which each investigator reported improvement with novel antipsychotic treatment are displayed in Table 2, alongwith the improved cognitive domains resultingfrom'our multiple comparison analysis. After wecorrected for multiple comparisons, 9 of the 15studies demonstrated significant neurocognitiveimprovement on at least 1 test measure followingtreatment with novel antipsychotic medicationcompared with conventional antipsychotics.
PSYCHIATRIC ANNALS 29:11/NOVEMBER 1999
.,

TABLE 2
DO NOVEL ANTIPSYCHOTICS IMPRDVE COGNITION?
TotalIQ
627
RESULTS OF THE META-ANALYSISThe meta-analysis of the 15 studies indicated
that there was a significant effect of novelantipsychotics compared with typical antipsychotics in their ability to improve cognitive functioning (chi-square ~ 62.41, P ~ .0004). The effectof novel antipsychotic medication on specificdomains of cognitive function was also examinedby combining all studies that reported data foreach domain. Corrections were not made for multiple comparisons because this would have
them using the published means and standarddeviations. In one case. we contacted the authorsto obtain unpublished means and standard deviations.
Rossi et al.,18 1997 X X . X·Serper and Chou, 19 X
1997
Galletly et al.,2' '997 X X X XFujii et al.,21 1997 X X·
Meta-Analysis Results of Impaired Cognitive Functions in 15 5tudiesAtten· Exec- Work- Learn- Vlsuo- DIgital Fine
tlon utlve Ing log and spatial Verbal Symbol MotorSubpro- Func- Mem- Mem- Anal- Flu- Substl- Func-
Study cesses tlon ory ory ysls ency tutlon lion
Meyer-Lindenberg X Xet a1./ 1997
Buchanan et al} X· X·1994 (phase I)
Green et al.,l X· X X1997; McGurk etal.,9 1997; andKern et al.,10 1999
Goldberg et a1.,111993
Hagger et al.,l2 1993 X X X· X·Buchanan et aL,8 X X X·
1994 (pha,e II)
lee et aI., Il 1994 X· X X· X·Zahn et al.,14 1994 XGallhofer et al.,15 X· X·
1996
Hoff et al.,16 1996 X XStip and Lussier,17 X·
1996
x - ill~'('$tiglllf}r rl7H1f,nlllt'''UC'Ogllilil.-oc illl/II'IJI>nIltJltS.
'NtuTDC'OgtriliT.'t improrvnltlllS Qjkr ",r"diD" jur rllllltil'l, rvm/rari50l15.
PSYCHIATRIC ANNALS 29:11/NOVEMBER 1999
STATISTICAL PROCEDUREThe statistical meta-analytic procedures used
to examine the results of these studies aredescribed in detail by Keefe et al." Briefly, Fisher'smethod for combining P values was used. It provides a summary of the statistical significance ofthe results and a test of the null hypothesis thatthere is no difference between the effects of novelantipsychotics and conventional antipsychotics.When a given study included multiple test measures, the average P value for that study was usedin the statistical procedure. If multiple test measures were included in a single domain of cognitive functioning, the average P value for thatdomain was used in the statistical procedure.When P values were not available, we calculated

DO NOVEL ANTI PSYCHOTICS IMPROVE COGNITIDN?
111'1
,
'I,II'i
required setting a variable P value for eachdomain. Meta-analyses indicated significantimprovement with novel antipsychDtics in eachof the aforementioned categories: attentiDn, executive functions, working memory, visuospatialanalysis, verbal fluency, digit symbDI substitution, and fine mDtDr functions.'
Despite a conservative statistical approach ofcorrecting the results of eacll study for the number of statistical comparisons made, the metaanalysis strongly suggests that novel antipsychotics, when compared with conventionalantipsychotics, improve cognitive functions inpatients with schizophrenia. The measures thatrespDnded the most strongly to novel antipsychotics were verbal fluency, digit symbDl substitution, fine motor functions, and executivefunctions. Attention subprocesses were alsorespDnsive. Learning and memory functionswere the least respDnsive.
CONCLUSIONBecause Df the limited number of studies
included in the meta-analysis, it is difficult tocDnclusively determine the pattern of cognitiveimprovements tllat can be expected with any specific novel antipsychotic treatment. There is, hDwever, preliminary support for the notion that verbal fluency, attention, and motor speed improvewith clozapine. It has been shown that risperidone has beneficial effects on verbal workingmemory, selective attention and alertness, I andexecutive functions." A study cDnducted by Rossiet al.18 suggests that negative symptoms correlatewith performance on tl,e Wisconsin Card SortingTest before and after treatment Witll risperidone,implying that cognitive deficits and negativesymptoms have a common substrate targeted byrisperidone. Data published since our metaanalysis was completed suggest that quetiapinemay have beneficial effects Dn attention,'2 shortterm memory, and explicit memDry.23 Asreviewed by Meltzer and McGurk," preliminarydata suggest that olanzapine also has beneficialeffects on a variety of cognitive functions.
NDne of the 15 studies met all of the recentlydeveloped standards for the assessment of cognitive change in schizophrenia.' Only 3 Df the 15studies used dDuble-blind methDdDlogy and the
628
impact of the various rater biases inherent toopen-label studies of patients with schizophrenia,described recently in tl,e Veterans' Administration collaborative study of clozapine," may bestrong. However, tl,ese 15 studies serve an impDrtant function-tlley suppDrt tl,e relatively recentnotion that cognitive deficits can be improved inpatients with schizDphrenia. As a result Df theseinitial studies, several large-scale comprehensiveinvestigations of the effect of novel antipsycl10ticson cognitive impairment in schizophrenia arecurrently under way. The results of these studieswlIl be of great interest because the possibility ofimproved cognitive funCtions in individuals witllschizDphrenia will help to further enhance theirquality Df life.
REFERENCES1. Green MF, Marshall BD, Wirshing we Jr, et aL Does
risperidone improve working memory in treatment-resistant schizophrenia? Alii JPsychiatry. 1997i154:799-804.
2. Blyler CR, Gold JM. Cognitive effects of typical antipsychotic treatment: another look. In: Sharma T, Harvey PO,cds. Coglli/ive Deficits ill Sc1lizoplmmirl. Oxford: OxfordUniversity Press. In press.
3. Keefe RSE, Gold JM. Comparing pharmacologic strategies of improving cognition. In: Keefe RSE, ed. ImprovillgCogllifive FUIICtiOl1 in Sc/lizopllrclIin. London: Science Press.In press.
4. Stip E. Memory impairment in schizophrenia: perspectives from psychopathology and pharmacotherapy. Call JPsyc1linlnJ.1996;41(suppI2):27S-345.
5. Perelti CS, Danion JM, Kauffmann-Muller F, Grange 0,Patat A, Rosenzweig P. Effects of haloperidol and amisul~
pride on molar and cognitive skiU learning in healthy volunteers. Psyclloplmrmncology (Bcrl). 1997;131:329-338.
6. Keefe RSE, Silva SG, Perkins DO, Lieberman JA. Theeffects of atypical antipsychotic drugs on neurocognitiveimpairment in schizophrenia: a review and meta-analysis. Schizopllr Bull. 1999;25:201-222..
7. Meyer-Lindenberg A, Gruppe H, Bauer U, Lis S, Krieger5, Gallhofer B. Improvement of cognitive function inschizophrenic patients receiving dozapine or zotepine:results from a double-blind study. PlwrmacopsydJiatry.·1997;30:35-42.
8. Buchanan RW, Holstein e, Brier A. The comparative efficacy and long-term effect of c10zapine treahnent on neuropsychological test performance. Bioi Psyc/tiatry.1994;6:717-725.
9. McGurk 5R, Green ME Wirshing we, el al. The effects ofrisperidone vs haloperidol on cognitive functioning in
. treahnent-resistant schizophrenia: the trial making lest.eNS Spectrums. 1997;2:60-64.
10. Kern R5, Green MF, Marshall BD Jr, et al. Risperidone vs.haloperidol on reaction time, manual dexterity, andmotor learning in treatment-resistant schizophrenicpatients. Bioi Psychiatry. 1999;44:726-732.
11. Goldberg TE, Greenberg RD, Griffin 5J, et al. The effect ofdozapine on cognition and psychiatric symptoms in
PSYCHIATRIC ANNALS 29:11/NOVEMBER 1999

DO NOVEL ANTIPSYCIIOTICS IMPROVE COGNITION?
II ;1
1./'! I. I
II::, .
! 'I
:11
:1
I'i i, ,
'II i, I
II f. II .
II
629
symploms and cognitive deficit in schizophrenia: an openstudy. Acta Psycltiatr SCUllrl. 1997;95:40-43.
19. Serper MR, Chou JCY. Novel neuroleptics improve allentiona I functioning in schizophrenic patienls: ziprazidoneand aripiprazole. CNS Speclrums. 1997;2:56-59.
20. Gillletly CA, Clark Rc. McFarlane Ac. Weber DL. Therelationship between changes in symptom ratings, neuropsychological test performance, and quality of life inschizophrenic patients treated with c1ozapine. PsyclliatryRes. 1997;72:161-166.
21. Fujii OEM, Ahmed J, Jokumsen M, Compion JM. Theeffects of c10zapine on cognitive functioning in treatmentresistant schizophrenic patients. / Nel/ropsycllintry eli"NCflrosci.1997;9:240-245.
22. Sax KW, StTakowski SM, Keck PE Jr. Attentional improvement following quetiapine fumarate treatment in schizophrenia. ScllizolJlIr Res. 1998;33:151-155.
23. Stip E, Lussier I, Babai M, Fabian IL, Link C. Seroquel andcognitive improvement in pLltienls with schizophrenia.Bioi Psychiatry. 1996;40:434-435. Letter.
24. Meltzer HY, McGurk SR. The effect of c1ozapine, risperidone, and olanzapine on cognitive funcHon in schizophrenia. ScliizopJIr BI/fl. 1999;25:233-255.
25. Rosenheck R, Cramer J, Xu W, et al. A comparison ofc10zapine and haloperidol in hospitalized patients withrefractory schizophrenia: Department of Veterans' AffairsCooperative Study Group on Clozapine in RefractorySchizophrenia. N Engl JMerl. 1997;337:809·815.
. L ...
,
patients wilh Sdlizophrenia. BrJ PSlJcbjatry. 1993i162:4348.
12. Hagger C, Buckley P, Kenny JT, Friedman L, Ubogy D,Meltzer HY. Improvement in cognitive functions and psychiatric symptoms in treatment-refractory schizophrenicpatients receiving c1ozapine. BioI Psychiatry. 1993;34:702712.
13. Lee MA, Thompson PA, Meltzer HY. Effects of clozapineon cognitive function in schizophrenia. JClill PS.'lc11intry.1994;55(suppI8):82-87.
14. Zahn TP, Pickar D, Haier RJ. Effects of c1ozapine,fluphenazine, and placebo on reaction time measures ofattention and sensory dominance in schizophrenia.Schizopllr Res. 1994;13:133-144.
15. Gallhofer B, Bauer U, Lis 5, Krieger 5, Gruppe H.Cognitive dysfunction in schizophrenia: comparison oftreatment with atypical antipsychotic agents and conventional neuroleptic drugs. Ellr NellropsyclJOplmrmncoI.1996;6(suppI2):13-20.
16. Hoff AL, Filushnan WQ, Wieneke M, et al. The effects ofc10zapine on symptom reduction, neurocognitive function, ilnd clinical management in treLlhnent-refractorystate hospital schizophrenic inpatients. Neuropsyc1JopJUlrmncology.1996;15:361-369.
17. Stip E, Lussier I. The effect of risperidone on cognition inpatients with schizophrenia. Cnll J Psychiatry. 1996;41(supp12):35-40. .
18. Rossi A. Mancini F, Stratta P, et aL Risperidone, negative
PSYCHIATRIC ANNALS 29:11/NOVEMBER 1999
I