DM Medscape
1
Type 2 diabetes mellitus consists of an array of d ysfunctions characterized by hyperglycemia and resulting from the combination of resistance to insulin action, inadequate insulin secretion, and excessive or inappropriate glucagon secretion. See the image below. Simplified scheme for the pathophysiology of type 2 diabetes mellitus. See Clinical indings in !iabetes "ellitus, a Critical #mages slideshow, to help identify various cutaneous, ophthalmologic, vascular, and neurologic manifestations of !". Essential Update: New Abridged Recommendations for Primary Care Providers The $merican !iabetes $ ssociation has released condensed recommendations for Standards of "edical Care in !iabetes% $bridged for &rimary Care &roviders , highlighting recommendations most relevant to primary care. The abridged version focusses particularly on the following aspects% • &rediabetes • Self'management education • (utrition • &hysical activity • Smo)ing cessation • &sychosocial care • #mmunizations • *lycemic treatment • Therapeutic targets • !iagnosis and treatment of vascular complications • #ntensification of insulin therapy in type 2 diabetes The recommendations can be accessed at $merican !iabetes $ssociation !iabetes&ro &rofessional +esources nline, Clinical &ractice +ecommendations - 2/0. 1/ Signs and symptoms "any patients with type 2 diabetes are asymptomatic. Clinical manifestations include the following% • Classic symptoms% &olyuria, polydipsia, polyphagia, and weight loss • 3lurred vision • 4ower'extremity paresthesias • 5e ast infections 6eg, balanitis in men7 See &resentation for more detail. Diagnosis !iagnostic criteria by the $merican !iabetes $ssociation 6$!$7 include the following 12 %
Transcript of DM Medscape

7/23/2019 DM Medscape
http://slidepdf.com/reader/full/dm-medscape 1/3
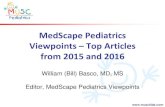
Type 2 diabetes mellitus consists of an array of dysfunctions characterized by hyperglycemia and resultingfrom the combination of resistance to insulin action, inadequate insulin secretion, and excessive orinappropriate glucagon secretion. See the image below.
Simplified scheme for the pathophysiologyof type 2 diabetes mellitus.
See Clinical indings in !iabetes "ellitus, a Critical #mages slideshow, to help identify various cutaneous,ophthalmologic, vascular, and neurologic manifestations of !".
Essential Update: New Abridged Recommendations for Primary CareProviders
The $merican !iabetes $ssociation has released condensed recommendations for Standards of "edicalCare in !iabetes% $bridged for &rimary Care &roviders, highlighting recommendations most relevant toprimary care. The abridged version focusses particularly on the following aspects%
• &rediabetes
• Self'management education
• (utrition
• &hysical activity
• Smo)ing cessation
• &sychosocial care
• #mmunizations
• *lycemic treatment
• Therapeutic targets
• !iagnosis and treatment of vascular complications
• #ntensification of insulin therapy in type 2 diabetes
The recommendations can be accessed at $merican !iabetes $ssociation !iabetes&ro &rofessional+esources nline, Clinical &ractice +ecommendations - 2/0.1/
Signs and symptoms
"any patients with type 2 diabetes are asymptomatic. Clinical manifestations include the following%
• Classic symptoms% &olyuria, polydipsia, polyphagia, and weight loss
• 3lurred vision
• 4ower'extremity paresthesias
• 5east infections 6eg, balanitis in men7
See &resentation for more detail.
Diagnosis!iagnostic criteria by the $merican !iabetes $ssociation 6$!$7 include the following 12 %

7/23/2019 DM Medscape
http://slidepdf.com/reader/full/dm-medscape 2/3
• $ fasting plasma glucose 6&*7 level of /28 mg9d4 6:. mmol947 or higher, or
• $ 2'hour plasma glucose level of 2 mg9d4 6//./ mmol947 or higher during a :0'g oral glucose
tolerance test 6*TT7, or
• $ random plasma glucose of 2 mg9d4 6//./ mmol947 or higher in a patient with classic symptoms
of hyperglycemia or hyperglycemic crisis;hether a hemoglobin $/c 6<b$/c7 level of 8.0= or higher should be a primary diagnostic criterion or an
optional criterion remains a point of controversy.
#ndications for diabetes screening in asymptomatic adults includes the following 1>, ?%
• Sustained blood pressure @/>09A mm <g
• verweight and / or more other ris) factors for diabetes 6eg, first'degree relative with diabetes, 3&
@/?9B mm <g, and <!4 >0 mg9d4 and9or triglyceride level @20 mg9d47
• $!$ recommends screening at age ?0 years in the absence of the above criteria
See ;or)up for more detail.
Management
*oals of treatment are as follows%
• "icrovascular 6ie, eye and )idney disease7 ris) reduction through control of glycemia and bloodpressure
• "acrovascular 6ie, coronary, cerebrovascular, peripheral vascular7 ris) reduction through control of
lipids and hypertension, smo)ing cessation
• "etabolic and neurologic ris) reduction through control of glycemia
+ecommendations for the treatment of type 2 diabetes mellitus from the Duropean $ssociation for theStudy of !iabetes 6D$S!7 and the $merican !iabetes $ssociation 6$!$7 place the patientEs condition,desires, abilities, and tolerances at the center of the decision'ma)ing process. 10, 8, :
The D$S!9$!$ position statement contains : )ey points%
/. #ndividualized glycemic targets and glucose'lowering therapies
2. !iet, exercise, and education as the foundation of the treatment program
>. Fse of metformin as the optimal first'line drug unless contraindicated
?. $fter metformin, the use of / or 2 additional oral or inGectable agents, with a goal of minimizingadverse effects if possible
0. Fltimately, insulin therapy alone or with other agents if needed to maintain blood glucose control
8. ;here possible, all treatment decisions should involve the patient, with a focus on patientpreferences, needs, and values
:. $ maGor focus on comprehensive cardiovascular ris) reduction
The 2/> $!$ guidelines for S"3* frequency focus on an individualEs specific situation rather thanquantifying the number of tests that should be done. The recommendations include the following 1A, B %
• &atients on intensive insulin regimens - &erform S"3* at least before meals and snac)s, as well
as occasionally after mealsH at bedtimeH before exercise and before critical tas)s 6eg, driving7H whenhypoglycemia is suspectedH and after treating hypoglycemia until normoglycemia is achieved.
• &atients using less frequent insulin inGections or noninsulin therapies - Fse S"3* results to adGust
to food inta)e, activity, or medications to reach specific treatment goalsH clinicians must not only educatethese individuals on how to interpret their S"3* data, but they should also reevaluate the ongoing needfor and frequency of S"3* at each routine visit.
$pproaches to prevention of diabetic complications include the following%
• <b$/c every >'8 months
• 5early dilated eye examinations

7/23/2019 DM Medscape
http://slidepdf.com/reader/full/dm-medscape 3/3
• $nnual microalbumin chec)s
• oot examinations at each visit
• 3lood pressure />9A mm <g, lower in diabetic nephropathy
• Statin therapy to reduce low'density lipoprotein cholesterol