
Division of Infectious and Tropical Diseases Hepatology Outpatient Unit University of Pavia-IRCCS...
82
Division of Infectious and Tropical Diseases Hepatology Outpatient Unit University of Pavia-IRCCS San Matteo Raffaele Bruno Overview sulla nuove terapie dell'epatite HCV correlata
-
Upload
derek-robbins -
Category
Documents
-
view
214 -
download
0
Transcript of Division of Infectious and Tropical Diseases Hepatology Outpatient Unit University of Pavia-IRCCS...

Division of Infectious and Tropical Diseases Hepatology Outpatient Unit
University of Pavia-IRCCS San Matteo
Raffaele Bruno
Overview sulla nuove terapie dell'epatite HCV correlata

HCV Genome and Protein Synthesis
(Penin F, Dubuisson J, Rey FA, Moradpour D, Pawlotsky JM. Hepatology 2004;39:5-19)

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

HCV Life Cycle

Infectedhepatocytes
Non-infectedhepatocytes
HCV Kinetics

Infectedhepatocytes
production
Non-infectedhepatocytes
HCV Kinetics

Infectedhepatocytes
production de novo infection
Non-infectedhepatocytes
HCV Kinetics

Infectedhepatocytes
production de novo infection
Non-infectedhepatocytes
HCV Kinetics

Infectedhepatocytes
production de novo infection
Non-infectedhepatocytes
Infected celldeath
HCV Kinetics

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
HCV Kinetics

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
HCV Kinetics

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Infectedhepatocytes
Peripheral blood(“viral load”)
production de novo infection
Non-infectedhepatocytes
Infected celldeath
Treatment Targets

Potential Targets of New Hepatitis C Antivirals
capsid
NS3 Protease domain
NS5B RNA-dependentRNA polymerase
C E1 E2 p7 NS2 NS3 NS4A NS4B NS5A NS5B
NS3 Helicase domain
NS3 Bifunctionalprotease / helicase
© 2002 JG McHutchison, DUMC
envelope protease/helicase polymerase

New Compounds - Agenda
• NM283 Valopicitabine (Idenix)• SCH 503034 (Schering Plough)• VX-950 (Vertex)• Albuferon (HGS)• Viramidine (Valeant)• CPG10101

Early Clearance of HCV RNA with Valopicitabine (NM283) plus Peg-Interferon in Treatment-Naïve Patients with HCV-
1 infection: First Results from a Phase IIb Trial
D Dieterich, E Lawitz, T Nguyen, Z Younes, J Santoro,N Gitlin, D McEniry, R Chasen, J Goff, S Knox,
K Kleber, B Belanger K, N Brown and the Valopicitabine 006 Study Group
EASL Annual Meeting April 29, 2006EASL Annual Meeting April 29, 2006Vienna, AustriaVienna, Austria

O
OHVal-O
CH3
N
NH
NH2
O
HO
Valopicitabine (NM283)2’-C-methylcytidine-3’-O-L-valine ester
Valopicitabine (NM283)First Nucleoside-Type HCV Pol Inhibitor
• NS5b polymerase inhibitor– Ribonucleoside; cytidine
analogue – NM107-triphosphate inhibits viral
polymerase by viral RNA chain termination
• Oral agent– Valyl ester pro-drug provides high
oral bioavailability– Plasma half life (4-6 hrs) &
intracellular half life (15 hrs) support once daily dosing

Key Eligibility CriteriaValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
• 18-65 years of age, male or female• HCV genotype 1• Treatment Naïve
– no previous antiviral therapy for HCV• Baseline
– HCV RNA ≥5 log10 IU/mL– ALT >1.0 x ULN and <5 x ULN
• Compensated liver disease• Candidate for interferon therapy

400→800 mgNM283 QD
peg-IFNα + 800 mg NM283 Follow-up
200 mgNM283 QD
peg-IFNα + 200 mg NM283 Follow-up
800 mgNM283 QD
peg-IFNα + 800 mg NM283 Follow-up
peg-IFNα + 800 mg NM283 Follow-up
peg-IFNα + 800 mg NM283 Follow-upNo Treatment peg-IFNα only
Baseline Week 1 Week 4 Week 48 Week 72
A
E
B
C
D
Initial Study DesignValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients

Baseline ParametersValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
A B C D E
Number (n=173) 34 34 34 36 35
Gender (% Male) 53 53 50 64 51
Age (mean years) 45 48 48 50 47
Mean HCV RNA (log10 IU/mL) 6.27 6.38 6.21 6.46 6.22
Mean serum ALT (U/L) 89 80 88 102 83
A Peg-IFN 180 µg QW @ D8 + NM283 400→800 mg QD @D29B NM283 200 mg QD @ D1 + Peg-IFN 180 µg QW @ D8C NM283 400→800 mg QD ramp @ D1 + Peg-IFN 180 µg QW @ D8D NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D8E NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D1
Treatment Group

HCV RNA Reduction to Week 4 Valopicitabine (NM283) plus peg-IFN vs. pegIFN alone
peg-IFNαinitiated in arms A-D
Mean log10
Reductionin HCV RNA from
Baseline(IU/mL)
A Peg-IFN 180 µg QW @ D8 + NM283 400→800 mg QD @D29 (n= 34)B NM283 200 mg QD @ D1 + Peg-IFN 180 µg QW @ D8 (n= 34)C NM283 400→800 mg QD ramp @ D1 + Peg-IFN 180 µg QW @ D8 (n= 34)D NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D8 (n= 36)E NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D1 (n= 35)
Week 4
All NM283+pegIFN arms with greater antiviralefficacy than pegIFN alone, at Week 4
-1.87
-2.92-3.12
-3.67-3.18
-5
-4
-3
-2
-1
0
1
0 2 4 6 8 10 12
Weeks

Convergence of HCV RNA Reductions by Week 12Valopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
-3.93 log10
-3.99 log10 -4.27 log10
-4.32 log10 -4.46 log10
peg-IFNαinitiated in arms A-D
No peg-IFNα alonearm after Week 4
Mean log10
Reductionin HCV RNA from
Baseline(IU/mL)
A Peg-IFN 180 µg QW @ D8 + NM283 400→800 mg QD @D29 (n= 30)B NM283 200 mg QD @ D1 + Peg-IFN 180 µg QW @ D8 (n= 31)C NM283 400→800 mg QD ramp @ D1 + Peg-IFN 180 µg QW @ D8 (n= 31)D NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D8 (n= 30)E NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D1 (n= 31)
Week 12 (partial data)
NM283 started for Group A
B: 87%E: 81%
A: 87%
C: 94% D: 90%
EVR (%)
-5
-4
-3
-2
-1
0
1
0 2 4 6 8 10 12
Weeks

Evidence for Antiviral Synergy: NM283 + pegIFNPredicted and Observed Viral Load Reductions, Week 4
peg-IFNαinitiated
200 mg valopicitabine 800 mg valopicitabine
Predicted
Observed
0 5 10 15 20 25 30
Study Day
Ch
an
ge
fro
m B
as
elin
e in
HC
V R
NA
log
10
-4
-3
-2
-1
0
NM283 Mono (001)
Peg-IFN Mono (006)283+Peg-IFN (Hyp. Add.)
283+Peg-IFN (Obs 006)
0 5 10 15 20 25 30
Study Day
Ch
an
ge
fro
m B
as
elin
e in
HC
V R
NA
log
10
-4
-3
-2
-1
0

A Peg-IFN 180 µg QW @ D8 + NM283 400→800 mg QD @D29B NM283 200 mg QD @ D1 + Peg-IFN 180 µg QW @ D8C NM283 400→800 mg QD ramp @ D1 + Peg-IFN 180 µg QW @ D8D NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D8E NM283 800 mg QD @ D1 + Peg-IFN 180 µg QW @ D1
Percent of Patients with HCV RNA PCR NegativeValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
6045 48
6752
61 62 6072
50
0
10
20
30
40
50
60
70
80
90
Week 12 Week 16
PercentOf
Patients
Solid Bars: < 600 IU/mL (Amplicor detection limit)Stippled Bars: < 20 IU/mL (Taqman detection limit)
70 7165 67
77 7673
8377 80

Adverse events (>6%)Valopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
A
pegIFN + 800mg NM283
wk 4(n=32)
B
200mg NM283 + pegIFN day 8
(n=31)
C
400→800mg NM283 + pegIFN
day 8(n=32)
D
800mg NM283 + pegIFN day 8
(n=36)
E
800mg NM283 + pegIFN day 1
(n=33)Total
(n=164)
Preferred Term N (%) N (%) N (%) N (%) N (%) N (%)
>1 AE 30 (93.8) 31 (100.0) 32 (100.0) 36 (100.0) 33 (100.0) 162 (98.8)
NAUSEA 17 (53.1) 19 (61.3) 25 (78.1) 30 (83.3) 27 (81.8) 118 (72.0)
VOMITING 9 (28.1) 9 (29.0) 15 (46.9) 20 (55.6) 25 (75.8) 78 (47.6)
FATIGUE 11 (34.4) 11 (35.5) 11 (34.4) 9 (25.0) 13 (39.4) 55 (33.5)
DIARRHEA 6 (18.8) 9 (29.0) 10 (31.3) 16 (44.4) 12 (36.4) 53 (32.3)
FLU-LIKE ILLNESS 13 (40.6) 6 (19.4) 6 (18.8) 7 (19.4) 7 (21.2) 39 (23.8)
HEADACHE 8 (25.0) 4 (12.9) 10 (31.3) 7 (19.4) 9 (27.3) 38 (23.2)
DEPRESSION 6 (18.8) 3 (9.7) 2 (6.3) 3 (8.3) 4 (12.1) 18 (11.0)
INJECTION SITE ERYTHEMA
4 (12.5) 5 (16.1) 1 (3.1) 4 (11.1) 4 (12.1) 18 (11.0)
INSOMNIA 8 (25.0) 3 (9.7) 1 (3.1) 1 (2.8) 5 (15.2) 18 (11.0)
RIGORS 3 (9.4) 5 (16.1) 0 5 (13.9) 2 (6.1) 15 (9.1)
ABDO PAIN 2 (6.3) 0 1 (3.1) 7 (19.4) 2 (6.1) 12 (7.3)
ANOREXIA 2 (6.3) 0 3 (9.4) 5 (13.9) 1 (3.0) 11 (6.7)
NEUTROPENIA 2 (6.3) 2 (6.5) 2 (6.3) 4 (11.1) 1 (3.0) 11 (6.7)
DIZZINESS 3 (9.4) 1 (3.2) 1 (3.1) 2 (5.6) 3 (9.1) 10 (6.1)
DYSGEUSIA 2 (6.3) 2 (6.5) 0 4 (11.1) 2 (6.1) 10 (6.1)
MYALGIA 4 (12.5) 3 (9.7) 1 (3.1) 1 (2.8) 1 (3.0) 10 (6.1)

Safety SummaryValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
• GI side effects common with initial dosing, usually mild-moderate; lessen within 1-2 weeks in 70-80% of affected patients, typically manageable with continued treatment
• 32 of 173 (18%) patients discontinued by Week 12– 24 (14%) for adverse events, mostly for GI side effects– only 2 patients in 200 mg cohort discontinued
• 8 SAEs reported by Week 12 (all in 800 mg dose groups)• 2 attributed to NM283 or NM283+pegIFN: dehydration with
renal insufficiency and pancreatitis; hyponatremia/hypokalemia
• 6 non-attributable: eye infection, flu with dehydration, CHF/diabetes, chest pain, numbness in arm/confusion, burn
– All patients recovered• Grade 3/4 lab abnormalities
– Most were attributable to peg-IFNα (WBC, ANC, platelets)– 9 patients with Grade 3/4 AST and 2 patients with Grade 3/4 lipase
elevation, all in 800 mg treatment groups

Protocol Amendment: Dose ModificationValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
• Patients receiving 800 mg NM283/pegIFN will continue treatment at reduced dose, randomly assigned (1:1) to:
• 200 mg valopicitabine/peg-IFNα or• 400 mg valopicitabine/peg-IFNα
• 12 patients with HCV RNA ≥ 600 IU/mL at time of protocol amendment; all discontinued treatment
• Patients in Group B (200mg NM283/pegIFN) continue study treatment unchanged
GI tolerance issues for some patients at 800 mg/d NM283 dose level, so a dose reduction has been implemented:

Valopicitabine Development: Next StepsFirst nucleoside-type HCV polymerase inhibitor
• 200-400 mg valopicitabine doses chosen for further study in treatment-naïve patients
– Good antiviral efficacy with good safety/tolerance
– Antiviral efficacy at Week 12 comparable to higher (800 mg/d) dosing regimens
• Ribavirin / NM283 interaction study – starts 2Q2006
• Potential investigation of double and triple regimens (NM283 + pegIFN + ribavirin) in phase III clinical trials
• Global Phase III program as collaboration between Idenix and Novartis

ConclusionsValopicitabine (NM283) Phase IIb Study in Treatment Naïve Patients
• Dose-related antiviral efficacy for NM283 + pegIFN at Week 4, shows antiviral synergy
• Convergence of HCV RNA reductions during Weeks 4-16 due to good efficacy in all arms
– EVR in 87-94% of patients on NM283+pegIFN (arms B, C, D)
– 67-79% HCV RNA undetectable by Amplicor (< 600 IU/mL) by Week 12
• Vs. 38-57% <600 IU with pegIFN-2a + RBV *
– 47-66% <20 IU/mL by Taqman
• Good tolerance and antiviral effect with NM283 200 mg/d + pegIFN
* Reddy, 2004; Murphy 2006

Randomized Trial of Valopicitabine (NM283)Alone and in Combination with Peg-Interferon
vs. Retreatment with Peg-Interferon plus Ribavirin (PegIFN/RBV) in Hepatitis C Patients with Previous Non-Response to PegIFN/RBV:
Second Interim Results
N. Afdhal, C. O’Brien, E. Godofsky, M. Rodriguez-Torres,
S. Pappas, P. Pockros, E. Lawitz, N. Bzowej, V. Rustgi, M. Sulkowski, K. Sherman,I. Jacobson, G. Chao, S. Knox,
K. Pietropaolo, and N. Brown
EASL Annual Meeting April 28, 2006EASL Annual Meeting April 28, 2006Vienna, AustriaVienna, Austria

ObjectivesValopicitabine (NM283) Phase IIb Trial in Non-responders
• Compare antiviral efficacy and safety/tolerability of:• 3 different dosing regimens of valopicitabine + peg-
IFNα-2a vs. re-treatment with peg-IFNα-2a + ribavirin
• also included: valopicitabine monoRx arm
• Patient population: patients with genotype 1 chronic hepatitis C who were non-responders to pegIFNα/RBV• relapsers to pegIFN+RBV excluded

Key Eligibility CriteriaValopicitabine (NM283) Phase IIb Trial in Non-responders
• 18-65 years of age, male or female
• HCV genotype 1
• Non-responders to previous adequate treatment course• At least 12 weeks of pegIFN + RBV• At least 75% of the prescribed doses pegIFN/RBV• Failed to clear HCV RNA to non-detectable levels• Patients must have previously failed for efficacy, not safety
• Screen/Baseline • HCV RNA ≥ 105 IU/mL• ALT < 5 x ULN
• Compensated liver disease

Study DesignValopicitabine (NM283) Phase IIb Trial in Non-responders
• Multicenter (22), randomized, active control design
• HCV RNA response criteria for failure and discontinuation – reductions from baseline • Week 4 0.5 log• Week 12 1.0 log • Week 24 > 2.0 log • Primary efficacy endpoint: SVR by HCV RNA:
COBAS TaqMan™ PCR assay (20 IU/mL)

400→800 mgNM283 QD
peg-IFNα + 800 mg NM283 Follow-up
400 mgNM283 QD
peg-IFNα + 400 mg NM283 Follow-up
800 mgNM283 QD
peg-IFNα + 800 mg NM283 Follow-up
peg-IFNα + 1000-1200 mg ribavirin Follow-up
Follow-up
Baseline Week 1 Week 48 Week 72
A
E
B
C
D
Initial Study DesignValopicitabine (NM283) Phase IIb Trial in Non-responders
NoTreatment
800 mg NM283 monotherapy

Current Status and Patient DispositionValopicitabine (NM283) Phase IIb Trial in Non-responders
• 190 patients randomized (fully enrolled in 2005)• 12 patients withdrew prior to receiving study medications
• 178 patients received study medications (ITT population)• 60 patients discontinued by Week 24
• 34 (19 %) failed viral response criteria at 4 or 12 weeks• 14 (8 %) discontinued for adverse events; only 1 on 400mg• 12 (7 %) withdrew consent or discontinued for other
reasons
• 118 patients past week 24
• Trial ongoing, today’s presentation: final 24 week interval analysis

Mean Reduction HCV RNA to Week 24Valopicitabine (NM283) Phase IIb Trial in Non-responders
E 2.27 logB 2.45 log
C 2.99 log
D 3.29 log
A NM283 800 mg QD (n=21) B NM283 400 mg QD + peg-IFN 180 µg QW (n=41) C NM283 400→800 mg QD ramp (1st week)→ 800 mg QD +peg-IFN 180 µg QW (n=41)D NM283 800 mg QD + peg-IFN 180 µg QW (n=41)E Ribavirin + peg-IFN 180 µg QW @ D8 (n=34)
SerumHCV RNA
(Mean Log10
ChangeFrom
Baseline)
Wks 12-24 n=7
Study Week
A 0.46 log
n = ITT Population
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0 6 12 18 24 30

Antiviral Efficacy at Week 24Valopicitabine (NM283) Phase IIb Trial in Non-responders
Treatment Group N
Mean HCV RNA (log10 IU/mL)
>2 log Reduction Number (%)
PCR –veNumber (%)
A NM283 monoRx 21 0.46 0 0 (0%)
B NM283 400 + pegIFN 41 2.45 23 (56%) 7 (17%)
C NM283 400-800 + PegIFN 41 2.99 * 30 (73%) * 5 (12%)
D NM283 800 + pegIFN 41 3.29 * 29 (71%) * 10 (24%)
E pegIFN + RBV retreatment 34 2.27 16 (47%) 6 (18%)#
* p < 0.02 vs pegIFN + RBV (comparisons of C and D to E)
#Residual viral load (median HCV RNA level) is ca. 1.8 log10 higher incontrol arm E vs. high-dose NM283 arms (C and D) at W24. Favors increasingdifference in HCV RNA clearance to non-detectable over time.

Adverse events (>10%):Valopicitabine (NM283) Phase IIb Trial in Non-responders
A: NM283 800mg(N=21)
B: NM283 400 mg+ Peg-IFN
(N=41)
C: NM283 400-800 mg
+ Peg-IFN(N=41)
D: NM283 800 mg+ Peg-IFN
(N=41)
E: RBV+ Peg-IFN
(N=34)Overall(N=178)
Preferred Term n (%) n (%) n (%) n (%) n (%) n (%)
>1 AE 20 (95.2) 41 (100.0) 41 (100.0) 41 (100.0) 34 (100.0) 177 (99.4)
NAUSEA 14 (66.7) 30 (73.2) 33 (80.5) 33 (80.5) 11 (32.4) 121 (68.0)
FATIGUE 3 (14.3) 21 (51.2) 20 (48.8) 25 (61.0) 22 (64.7) 91 (51.1)
VOMITING 10 (47.6) 20 (48.8) 21 (51.2) 32 (78.0) 3 (8.8) 86 (48.3)
DIARRHOEA 7 (33.3) 13 (31.7) 25 (61.0) 14 (34.1) 5 (14.7) 64 (36.0)
HEADACHE 2 (9.5) 16 (39.0) 15 (36.6) 12 (29.3) 9 (26.5) 54 (30.3)
DECREASED APPETITE
5 (23.8) 5 (12.2) 8 (19.5) 11 (26.8) 5 (14.7) 34 (19.1)

Safety Summary to Week 24Valopicitabine (NM283) Phase IIb Trial in Non-responders
• Nausea (with/without vomiting) common with initiation of NM283 + pegIFN treatment; diarrhea is less common; usually transient or intermittent - 4 patients (3%) discontinued for GI side effects
• 24 serious adverse events (SAEs) through Week 24
• 6 reported possibly attributed to NM283 (anemia, colitis, dehydration, fatigue, pancreatitis, gram-negative bacteremia 2° to UTI)
• Sporadic elevations of amylase, lipase, AST, ALT
• rarely treatment-limiting

SCH 503034
A HCV Protease Inhibitor

SCH 503034 plus PegIntron® in G1 NR to PegIntron® ± RBV – Phase I
P1 P2 P3
A7 days SCH 503034 mono *
14 days Peg-alfa 2b mono 14 days combo
B 14 days Peg-alfa 2b mono 14 days combo7 days SCH 503034 mono *
C 14 days combo7 days SCH 503034 mono *
14 days Peg-alfa 2b mono
* dose: 200 or 400 mg, q8h
Zeuzem et al, EASL 2006, oral

PK Profile of Pegalfa 2b ± PIM
ean
HC
V
RN
A C
han
ge
(Log
10)

SCH 503034 plus Peg-alfa 2b in G1 NR to Peg-alfa 2b ± RBV – Phase I
• Results:– Mean max log10 viral load drop 2.4 and 2.9 log
for 200 and 400 mg combined with Peg-IFN alfa 2b
• 4/10 became HCV RNA negative on combination therapy with 400 mg SCH 503034
• HCV RNA reduction disappointing for a PI (mean 1.5 log highest monotherapy dose)
• No resistance reported
• q8h dosing is a challenge for patientsZeuzem et al, EASL 2006, oral

Follow-up
Follow-up
Follow-up
Follow-up
Follow-up
SCH 503034 plus PegIntron® ± RBV – Ongoing Phase II Study – Study Design
Randomi-zation
Study Weeks 480 72
CH
C,
G1,
NR
to
Peg
-IF
N +
RB
V,
n=
300
PegIntron® plus SCH 503034 100 mg q8
PegIntron® plus SCH 503034 200 mg q8
Follow-up
PegIntron® plus SCH 503034 400 mg q8
24
PegIntron® plus RBV plusSCH 503034 400 mg q8
PegIntron® plus SCH 503034 400 mg q8
PegIntron® plus RBV

VX-950
A HCV Protease Inhibitor

VX-950 Phase Ib – Study Design
Naï
ve,
G1,
n=
20
VX-950 750 mg q8h plus PEGASYS® 180 µg qw
VX-950 750 mg q8h
0 2
PEGASYS® 180 µg qw plus Placebo
Randomization Study weeks
n=8
n=8
n=4
Reesink et al, EASL 2006, oral late breaker

VX-950 – Results
5.50
44.00
11.00
00.00
1.00
2.00
3.00
4.00
5.00
6.00
Median log10 reduction of HCVRNA
Number of patients with HCV RNA<10 IU/mL
Combination therapy VX-950 PEGASYS
Reesink et al, EASL 2006, oral late breaker

VX-950 – Phase IIa – Study DesignC
HC
, G
1, n
aïve
, n
=12
VX-950§ 750 mg q8h plus PEGASYS® 180 µg plus
COPEGUS® 1000-1200 mg
Study Weeks
0 4
VX05-950-102
§ One-time loading dose 1250 mg
* Patients continue on PEGASYS®/COPEGUS®
*

VX-950 – Results
6
1112 12
23
9
12
0123456789
101112
Week 1 Week 2 Week 3 Week 4
Nu
mb
er o
f p
atie
nts
HCV RNA <30 IU/mL HCV RNA <10 IU/mL
VX05-950-102
End of

VX-950 in Naïve G1– Phase II – Study Design – Expected Start May 2006
Study Weeks 480
Placebo plus PEGASYS® plus COPEGUS®
VX-950 750 mg q8h plus PEGASYS® plus
COPEGUS®
VX-950 750 mg q8h plus PEGASYS®
VX-950 750 mg q8h plus PEGASYS® plus
COPEGUS®
CH
C,
naï
ve,
G1,
n=
320
2412
VX-05-950-104
PEGASYS® plus COPEGUS®

VX-950 – Summary
• Highest antiviral activity (4log drop) of an antiviral in monotherapy
• In triple combo all patients HCV RNA negative (<10 IU/mL) by week 4
• VX-950 has potential to significantly shorten treatment duration in combination therapy
• Q8h dosing is an issue
• High resistance in monotherapy– Not seen in phase 2a combo

New Long Acting IFNs
Albuferon

Albuferon Characteristics
• IFN alfa-2 fused with human serum albumin
• higher efficacy not expected
• better convenience because of less frequent dosing
• currently in phase II
• possible launch 2010
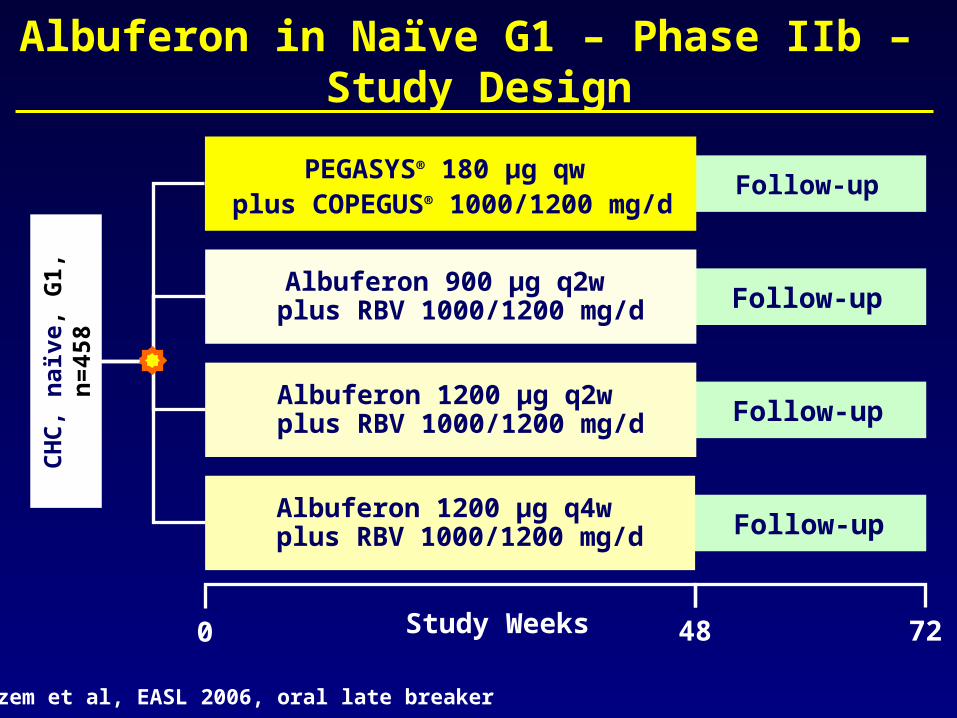
Albuferon in Naïve G1 – Phase IIb – Study Design
Study Weeks 480 72
CH
C,
naï
ve,
G1,
n=
458
Follow-upPEGASYS® 180 µg qw
plus COPEGUS® 1000/1200 mg/d
Zeuzem et al, EASL 2006, oral late breaker
Follow-upAlbuferon 900 µg q2w
plus RBV 1000/1200 mg/d
Follow-upAlbuferon 1200 µg q2w
plus RBV 1000/1200 mg/d
Follow-upAlbuferon 1200 µg q4w
plus RBV 1000/1200 mg/d

Albuferon in Naïve G1 – Week 12 Results
Zeuzem et al, EASL 2006, oral late breaker
Albuferon
PEGASYS® + RBV
(n=114)
900 µg q2w + RBV
(n=110)
1200 µg q2w + RBV
(n=118)
1200 µg q4w + RBV
(n=116)
EVR (≥2 log drop)
85.7% (96/112)
80.4% (90/112)
87.5% (91/104)
73.4% (80/109)
HCV RNA negative at week 12
62.5% (70/112)
66.1% (74/112)
74.0% (77/104)
52.3% (57/109)

Viramidine
A Ribavirin Prodrug

VISER 1 – Phase III, Pivotal Study – Study Design
Follow-upPegIntron®
plus Viramidine 1200 mg/d
Study Weeks
0 48 72
Follow-upPegIntron®
plus RBV 1000/1200 mg/d
CH
C, n
aïv
e, n
=9
70
* Treatment duration according to genotype: G2/3 24 weeks, G1/4 48 weeks
24 *

VISER 1 – Efficacy Results
Viramidine Ribavirin
SVR * (ITT analysis) 38% 52%
Anemia rate (Hb <10 g/dL) 5% 24% p<0.0001
* Percent of patients with HCV RNA <39 IU/mL
Press release, 21.03.2006

VISER 1 – Viramidine * Weight-Based Analysis
Viramidine dose n SVR § Anemia ‡
≤18 mg/kg 323 47% 4.3%
19-22 mg/kg 82 66% 2.4%
≥23 mg/kg 16 81% 12.5%
* Fixed dose of Viramidine averaged ~15 mg/kg, based on mean weight for the study population
§ HCV RNA <39 IU/mL, per protocol analysis‡ Hb <10 g/dL
Press release, 21.03.2006

VISER 2
• Identical study design to VISER 1 but PEGASYS® instead of PegIntron®
• Results available in Q3/2006

CPG 10101

Phase Ib Trial with CPG 10101
• CPG 10101 is a synthetic oligonucleotide and selective TollLikeReceptor9 agonist which enhances the ability of dendritic cells to activate killer T cells against invaders. Actilon appears to stimulate TLR9 in a different way resulting in significantly stronger activation of interferon-α production by the plasmacytoid dendritic cells.

Phase Ib Trial with CPG 10101
• Dose escalation study (doses 0.25 to 20 mg once or twice weekly for 4 weeks), randomized, placebo-controlled
• Patient population: 60 CHC patients (predominantly G1 who failed previous therapy)
• Results:– CPG 10101 was well tolerated– ≥1 log 10 reduction was seen in all patients
receiving ≥ 1 mg– Patients showed a dose-dependent increase in
markers of immune activation and associated decreases in HCV RNA levels
McHutchison et al, EASL 2006, oral

CPG 10101 plus PegIntron® ± RBV in G1 Relapsers – Study Design
Randomization Study Weeks480 72
CH
C,
G1,
rel
apse
rs t
o
PE
G-I
FN
+ R
BV
, n
=74
Follow-upPegIntron® 1.5 µg/kg/wk plus RBV 800-1400 mg/d
Follow-upPegIntron® 1.5 µg/kg/wk plus RBV
800-1400 mg/d plus CPG 0.2 mg/kg/wk
Follow-upPegIntron® 1.5 µg/kg/wk plus CPG 0.2 mg/kg/wk
Follow-upCPG 0.2 mg/kg/wk
plus RBV 800-1400 mg/d
Follow-upCPG 0.2 mg/kg/wk

CPG 10101 plus PegIntron® ± RBV in G1 Relapsers – Week 12 Results
• Conclusion:Preliminary data indicate a greater proportion of patients achieving EVR received CPG + PEG + RBV than PEG + RBV and suggest that CPG + PEG may represent a therapeutic alternative to PEG + RBV
PEG + RBV
CPG + RBV + CPG
CPG + PEG
CPG + RBV
CPG
HCV RNA (Mean log10 decrease) a 2.19 3.26 2.15 1.41 0.1 *
EVR at week 12 b 57% 86% 57% 21% 0%* p<0.001 vs PEG + RBV, a at week 12, b no definition provided
McHutchison et al, EASL 2006, oral late breaker

Summary
• Antiviral compounds are expected to change HCV treatment significantly by– increasing SVR rates– shortening treatment duration– Until now Peg seems to be the backbone of
HCV therapy in the future.


















