INTERNAL MEDICINE - Isehara...INTERNAL MEDICINE - Isehara ... ...

Division of General Internal Medicine Hypertension Impact Project
September 21, 2017
Integrated Network Summit
Presented by: Mark Earnest, MD, PhDLauren Drake, Wagner Schorr-Ratzlaff MD, Huong Lam MD, Laurence Williams MD, Mary McCord MD, Hillary Chrastil
MHA, Mary Kozloski, Carmen L. Lewis MD, MPH

Background
• Goal: To achieve 70% hypertension control across both our General Internal Medicine practices.
• Strategy: Five evidence-based domains with 1-3 strategies each
• Setting• Anschutz Internal Medicine ~ 4,700
• Lowry Internal Medicine ~ 2,400


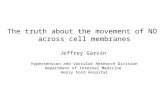
Results

33%
63%
67%
37%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
February, 2016 June, 2017
Anschutz Internal Medicine
Providers with 70% Control or Greater
Providers with Less than 70% Control
27%
88%
73%
12%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
February, 2016 June, 2017
Lowry Internal Medicine
Providers with 70% Control or Greater
Providers with Less than 70% Control

EDUCATION
Patient Education Materials Quarterly BP Measurement Technique Trainings
• Medical Assistants (MAs) participate in ongoing educational sessions
• Includes:• Overview of BP• Cuff sizing• Patient positioning• Automatic BP machines• Manual readings

Previous outreach criteria:• Patients age 18-59
• Last BP > 140/90
• Average of the last 3 BP Readings > 150/90
• Last PCP visit 6 months ago or longer
Expanded outreach criteria:
• Patients age 18-59
• Last BP >140/90
• Average of the last 3 BP readings > 140/90
• Last PCP visit 3 months ago or longer
269
504
280
95
0
100
200
300
400
500
600
700
Lowry (n=549) Anschutz (n=599)
Outreach Results
Attempted Resulted in Visit
OUTREACH

Anschutz
• Pharmacy
• Recheck & review
• Encourage Self-monitoring
Lowry
• Physician paired with a trained RN
• Collaborate & manage complex hypertensive patients
• RN provides education & support via telephone / MHC
• Recheck & review
AHA HBP Algorithm Including:• Patient education• Medication titration• Lifestyle modifications
TREATMENT &
COUNSELING

SELF MONITORING
No Co-Pay BP Checks Home BP Checks
• Encouraged self-monitoring as part of treatment via the MD/ RN HTN clinic and the Pharmacy HTN clinic
Summary n %Total # no-charge BP Checks 94# Unique patients 84BP =< 140/90 57 60.6%Escalated to RN 32 34.0%Escalated to MD 2 2.1%Sent to ED 1 1.1%

CURRENT FACULTY # Pat
ients
age
18<=
59
# w
ith B
P <= 1
40/90
# pts
unco
ntrolle
d#
additi
onal co
ntro
lled p
ts to
mee
t goal
% <
= 140
/90
Goal
Johnson, Michelle 20 16 4 - 80.00% 70.00%
Jordan, Michael 87 69 18 - 79.31% 70.00%
Doe, Jane 12 9 3 - 75.00% 70.00%
Test, Doctor 33 24 9 - 72.73% 70.00%
Lee, NP 11 8 3 - 72.73% 70.00%
Green, Mario 57 41 16 - 71.93% 70.00%
Red, Allison 14 10 4 - 71.43% 70.00%
ALL 796 538 258 20 67.59% 70.00%
Diaz, Director 77 52 25 2 67.53% 70.00%
Day, Dean 91 61 30 3 67.03% 70.00%
Physician, Miss 24 15 9 2 62.50% 70.00%
RESIDENTS 144 88 56 13 61.11% 70.00%
Last, First 61 37 24 6 60.66% 70.00%
Name, Name 12 6 6 3 50.00% 70.00%
AUDIT & FEEDBACK
LOWRY IM OP TEST, DOCTOR NO TEST, PATIENT 888888 53 12/11/2015 06/16/2015 152 96 132
LOWRY IM OP TEST, DOCTOR YES JOHNSON, TEST 222222 62 6/24/2015 09/09/2014 133 80 144
LOWRY IM OP TEST, DOCTOR YES DOE, JANE 131313 68 6/17/2015 06/17/2015 138 75 143
# Patients with HTN: 3
# Patients with last BP <= 140/90 2
% Patients with last BP <= 140/90 66.67%
Last Practice Visit
Last
PCP
Visit
Last
BP
Systolic
Last
BP
Diastolic
Average
BP
SystolicDepartment Provider
BP <
140/90
Patient
Name
MRN Age

AUDIT & FEEDBACK
54.55%
50.89%51.72%
57.63%56.14%
52.78%
57.02%54.10%
61.11%
68.24%
71.71%
56.39%
60.33%58.90%
57.96%
62.62%
56.02%
52.17%53.61%
59.73%
61.75%
66.07%
40.00%
45.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
Feb-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Oct-16 Dec-16 Feb-17 Apr-17 Jun '17
Resident Hypertension Control (Ages 18-59)
LOWRY RESIDENTS ANSCHUTZ RESIDENTS

Uncontrolled Patients: A Deep Dive
144, 83%
29, 17%
Hypertensive Patients with Uncontrolled BP (N=173)
Uncontrolled patients who are NOT actionable
Uncontrolled patients who are actionable and may benefit from anintervention
47, 33%
35, 24%
28, 19%
14, 10%
13, 9%
4, 3%
2, 1%1, 1%
Reasons Patients Were Not Actionable (N = 144)
BP is adequately controlled in Primary Care/ home measurement
Patient did not follow up
Provider is actively intervening on patient. (lifestyle modifications or med titration)
Following PCP's most recent intervention, BP is now controlled
Medication non-adherence
Other medical issues have taken priority
No longer a patient with this provider/ clinic
Patient refused intervention

In Summary
• Push individualized bi-monthly data to providers
• Focused work with residents
• Patient education materials
• Training for MAs
• Outreach
• AHA HBP Algorithm
• No co-pay BP checks
• Home BP monitoring

Lessons Learned
• Pursue improvement in multiple domains
• Monitoring the multiple data streams used to support hypertension improvement is key for improvement work
• Accurate panel attribution is imperative
• Pushing actionable patient-level data is a meaningful exercise

Future Applications for Population Health
Providers receive
actionable patient-level
data
DashboardAutomated process
to push data

Discussion