Disturbances of Respiratory Function
8
Disturbances of Respiratory Function Love, bbf. Page 1 Note: This lecture is almost totally the same with all that’s written in Chapter 252: Disturbances of Respiratory Function, Harrison’s Principles of Internal Medicine 18 th Ed. Disturbances of the respiratory system are divided into: disturbances of ventilation disturbances of perfusion disturbances of gas exchange Problems with these three would cause derangement of respiratory function, because the primary function of the respiratory system is to oxygenate blood and to eliminate C0 2 , and to fulfill this function, there must be adequate perfusion, ventilation and normal diffusion of gases = O 2 and CO 2 . There are three interdependent functional components of the lungs. – the airways, the neuromuscular system and the chest wall. First, the lungs including the airways; the neuromuscular system including the muscles that would contract and relax to help you inhale or exhale; the chest wall including all that is not lung or neuromuscular system - meaning the mass of the respiratory muscles, the abdomen (especially in obese individuals), and the heart (especially if it is large). These three components have mechanical properties that relate with the lung volume, or in the case of the neuromuscular system, the volume at which it is operating, and the rate of change of its volume. VOLUME-RELATED MECHANICAL PROPERTIES – STATICS Due both to surface tension at the air-liquid interface between alveolar wall lining fluid and alveolar gas and to elastic recoil of the lung tissue itself, the lung requires passive transmural pressure to inflate, to expand, and to stay expanded. The expanding pressure is the elastic recoil pressure of the lungs. This causes increase in lung volume. The lung becomes very stiff, very hard to expand at high volume, so that relatively small volume change is accomplished even with high transpulmonary pressure. In contrast, lung is compliant at low lung volume as the graph shows. Because the lung is compliant, it is very easy to inhale or exhale, hardly any effort is needed. And at zero, there is still a normal amount of air in the lungs. This is because the small peripheral airways are tethered/helped open by the radially outward pulling of the lungs. This air intention is exaggerated in patients with obstructive airway disease resulting in the increase of the tidal volume. Chest Wall - Encloses a large volume at atmospheric pressure - Compliant at high enclosed volume & even at small negative transmural pressure - At very small lung volume in response to large negative transmural pressure, chest wall becomes stiff due to: squeezing together of ribs & intercostals muscles; diaphragm stretch; displacement of abdominal contents & straining of ligaments & body articulation
-
Upload
jason-mirasol -
Category
Documents
-
view
215 -
download
0
description
lecture on pulmonologyrespiratory functionmedicinepulmonology
Transcript of Disturbances of Respiratory Function

Disturbances of Respiratory Function
Love, bbf. Page 1
Note: This lecture is almost totally the same with all that’s written in Chapter 252: Disturbances of Respiratory Function, Harrison’s Principles of Internal Medicine 18
th Ed.
Disturbances of the respiratory system are divided into:
disturbances of ventilation
disturbances of perfusion
disturbances of gas exchange
Problems with these three would cause derangement of respiratory function, because the primary function of the respiratory system is to oxygenate blood and to eliminate C02, and to fulfill this function, there must be adequate perfusion, ventilation and normal diffusion of gases = O2 and CO2.
There are three interdependent functional components of the lungs. – the airways, the neuromuscular system and the chest wall.
First, the lungs including the airways;
the neuromuscular system including the muscles that would contract and relax to help you inhale or exhale;
the chest wall including all that is not lung or neuromuscular system - meaning the mass of the respiratory muscles, the abdomen (especially in obese individuals), and the heart (especially if it is large).
These three components have mechanical properties that relate with the lung volume, or in the case of the neuromuscular system, the volume at which it is operating, and the rate of change of its volume.
VOLUME-RELATED MECHANICAL PROPERTIES – STATICS Due both to surface tension at the air-liquid interface between alveolar wall lining fluid and alveolar gas and to elastic recoil of the lung tissue itself, the lung requires passive transmural pressure to inflate, to expand, and to stay expanded. The expanding pressure is the
elastic recoil pressure of the lungs. This causes increase in lung volume. The lung becomes very stiff, very hard to expand at high volume, so that relatively small volume change is accomplished even with high transpulmonary pressure.
In contrast, lung is compliant at low lung volume as the graph shows. Because the lung is compliant, it is very easy to inhale or exhale, hardly any effort is needed.
And at zero, there is still a normal amount of air in the lungs. This is because the small peripheral airways are tethered/helped open by the radially outward pulling of the lungs. This air intention is exaggerated in patients with obstructive airway disease resulting in the increase of the tidal volume.
Chest Wall
- Encloses a large volume at atmospheric pressure
- Compliant at high enclosed volume & even at small negative transmural pressure
- At very small lung volume in response to large negative transmural pressure, chest wall becomes stiff due to: squeezing together of ribs & intercostals muscles; diaphragm stretch; displacement of abdominal contents & straining of ligaments & body articulation

Disturbances of Respiratory Function
Love, bbf. Page 2
The chest wall differs markedly from the lungs. The lung tends to deflate, but the chest wall tends to go outwards.
Because the lung and chest wall function in mechanical series, the pressure required to displace the passive respiratory system (lungs + chest wall) at any volume is simply the sum of the elastic recoil pressure of the lungs and the transmural pressure across the chest wall. So that’s why it becomes a sigmoid curve.
There is stiffness at high lung volume and low lung volume. At high lung volume, the stiffness is caused by the stiffness of the lung, while at low lung volume, the stiffness is caused by the chest wall. The respiratory system is very compliant at the middle portion.
We have a passive resting point when the alveolar gas and the transmural pressure is zero. This is the volume at your FRC wherein the outward pull of the chest wall is equal to the inward pull of the lung. This is at the zero resting volume of the respiratory system.
The maximal pressures these sets of muscles can generate varies with the lung volume at which they operate, due to the length-tension relationship of striated muscles and the changes of the mechanical advantage as the angles of insertion change with lung volume.
The respiratory muscles are more than adequate to generate force to inhale or drive the respiratory system up to the total lung capacity (TLC) and up to the residual volume (RV). RV is the volume that remains within the lungs no matter how hard you try exhale. The excursion of the chest wall is from the TLC up to the RV. The vital capacity (VC) is the difference between the TLC and RV.
Measurement of Lung volume
Inert gas dilution test
The O2 washout test – you let the patient inhale -instead of He, give your patient pure O2. Washout all the N2 because the air that we breathe in is 98% N2. Then after several minutes of breathing pure O2, this pure O2 is diluted with N2, then check the concentration, and calculate for the RV.
Body box
Plethysmograph
**The problem with the washout test or dilution test: there may be some areas which are poorly ventilated, which cannot be measured.
Measurement of Muscle Strength
To measure the muscle strength of the neuromuscular function, request for the maximal inspiratory pressure, or maximal expiratory pressure. Try to ask patient to inhale or exhale maximally through a closed circuit/ closed mouthpiece, then measure the pressure the patient is able to generate.
Inhalation = generates a negative pressure = maximal inspiratory pressure = - 60cmH2O
At - 25cmH2O, you can already generate an effective cough.
Exhalation = positive pressure = pressure above atmospheric pressure = + 60cmH2O

Disturbances of Respiratory Function
Love, bbf. Page 3
FLOW-RELATED MECHANICAL PROPERTIES – DYNAMICS
The dynamic airflow properties of the lung substantially determine the ability to ventilate and contribute importantly to the work of breathing, and are often deranged by disease. Understanding these properties is, therefore, well worthwhile.
As with flow of any fluid (gas or liquid) in any tube, maintenance of airflow within the pulmonary airways requires a pressure gradient that falls along the direction of flow, the magnitude of which is determined by the flow rate and the frictional resistance to flow. During quiet tidal breathing, the pressure gradients driving inspiratory or expiratory flow are small owing to the very low frictional resistance of normal pulmonary airways (normally <2 cmH2O/L per second). However, during rapid exhalation, another phenomenon reduces flow below that which would have been expected, were frictional resistance is the only impediment to flow. This phenomenon is called dynamic airflow limitation, and it occurs because the bronchial airways through which air is exhaled are collapsible rather than rigid.
Airflow is constant along the airway Flow = volume / time Velocity of flow = flow summed cross-sectional area
Velocity of flow is much greater in the central airways than in the peripheral airways
During exhalation, gas leaving the alveoli must therefore gain velocity as it proceeds toward the mouth.
The maximum value of flow is related to: - Gas density - Airway cross-section & distensibility - Elastic recoil pressure of the lungs - And the frictional pressure loss to the
flow-limiting airway site.
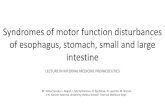
A. Normal.
B. Airflow obstruction.
C. Fixed central airway obstruction. RV, residual volume; TLC, total lung capacity. *Flow-volume loops.

Disturbances of Respiratory Function
Love, bbf. Page 4
The maximum expiratory flow is relatively elevated when considered in relation to lung volume. Conversely, in emphysema, lung recoil pressure is reduced, which is a principal mechanism by which maximal expiratory flows fall.
The Bernoulli effect also acts during inspiration, but the more negative pleural pressures during inspiration lower the pressure outside of airways, thereby increasing transmural pressure and promoting airway expansion. Thus, inspiratory airflow limitation seldom occurs due to diffuse pulmonary airway disease. Conversely, extrathoracic airway narrowing (as due to a tracheal adenoma or post-tracheostomy stricture) can lead to inspiratory airflow limitation
Ex. Comparison of the plastic straws we use for drinking - the hard, strong one (in fastfoods/restaus) - the soft, pliant one (in softdrinks)
*When you inhale very deeply, the soft straw will compress and collapse, thus air/fluid is more difficult to flow through
Work of Breathing Normal state – minimal ↑ - ↑ need of ventilation (↑ metabolism / metabolic acidosis) ↑ in mechanical load ( stiffness of the lung /chest wall/airway resistant)
The work required of the respiratory muscles is minimal. However, the work of breathing can increase considerably, due either to requirement for substantially increased ventilation, an abnormally increased mechanical load, or both. The rate of ventilation is primarily set by the need to eliminate carbon dioxide.
Work of breathing also increases when disease reduces the compliance of the respiratory system or increases the resistance to airflow. The former occurs commonly in diseases of the lung parenchyma (interstitial processes or fibrosis, alveolar filling diseases such as pulmonary edema or pneumonia, or substantial lung resection), and the latter occurs in obstructive airways diseases such as asthma, chronic bronchitis, emphysema, and cystic fibrosis.
Sometimes, even in patients with obstructive lung disease, there would be added stiffness to the lung, not because of the airway resistance, but there would be added work of breathing due to the thickening of the lung. Because in patients with obstructive lung disease, they may develop dynamic hyperinflation.
When you inhale, the flow is better.
Ex. When you inhale, let’s say 500, then you exhale 400. You retain 100 because of the flow limitation site. Even if you haven’t exhaled all the air you inhaled, the lung will already retain more air and build your residual volume.
Adequacy of Ventilation
Minute volume = amount of air that moves in and out of the lungs in one minute
Tidal volume = amount of air that you inhale or exhale during tidal breathing. This is made up of dead space ventilation and alveolar ventilation. Alveolar ventilation is more important as this is the one that would participate in your gas exchange.
Minute ventilation (VE) = VT x RR Tidal volume (VT) = VD + VA
- Dead space ventilation Alveolar ventilation – participate in gas exchange

Disturbances of Respiratory Function
Love, bbf. Page 5
REMEMBER! PA02 = FI02 x (P bar – PH20) – PAC02 / R CO2 is used to know whether your patient has adequate ventilation or not. Why CO2?
- Because we hardly inhale CO2 20.9% = O2 78% = N2 1% = all other gases including CO2 ↑CO2 in the body – inadequate ventilation
CO2 is a waste product. It is the amount of metabolism that our body has.We blow off CO2. We do not inhale it. If there is a build-up of CO2 in the body, there isn’t enough ventilation. If this is not the cause of inadequate ventilation, it means the body has produced excessive amounts of CO2.
PaCO2 - Determined by CO2 production &
alveolar ventilation PaCO2 = vCO2 / VA
If you have increased CO2 production, you have increased CO2 in the blood. It is directly proportional. On the other hand, it is inversely proportional to the alveolar ventilation.
Gas Exchange
Diffusion - Diffusion membrane surface area &
thickness
Gas exchange involves diffusion. Diffusion is affected by the surface area. The larger the surface area, and the thinner the membrane, the better the diffusion.
- Diffusion coefficient of the gas/substance in the lung diffusion is usually “perfusion dependent”
- “diffusion dependent” on in high altitude, maximal exercise or interstitial lung disease (some)
O2 and CO2 have good diffusion coefficients. There is no problem on the transport of these gases through the alveolar surface membrane. The problem on gas exchange is with perfusion. The lung has a very big surface area – as big as a football field. Problems with perfusion affect problems of oxygen levels in blood.
In patients with shunt, there is perfusion, but no ventilation. There is blood flow, but no ventilation.
For the blood to be completely saturated with O2 as it passes through the pulmonary circulation, it only needs 1/3 of the 0.75%. So even when you exercise, the blood flow through pulmonary circulation is cut short.
The diffusion problem will only occur if you have problems with the surface - if it is destroyed or is very thick.

Disturbances of Respiratory Function
Love, bbf. Page 6
Measurement of gas exchange
- Diffusion capacity (DLCO) - Pulse oximetry - Arterial blood gas (ABG)
ABG Able to determine the blood:
- pH
- PaCO2 – (N)= 35-45
- PaO2 – (N) = 80-100 - Bicarbonate level – (N) = 24 (+/-) 2 - Hgb O2 saturation
*unit: mmHg/TORR
Serial ABG – measures the partial pressures of O2 and CO2. ABG – get from artery – bright red, not maroon (vein)
The effectiveness of gas exchange can be assessed by measuring the partial pressures of oxygen and carbon dioxide in a sample of blood obtained by arterial puncture.
The oxygen content of blood (CaO2) depends upon arterial saturation (%O2Sat), which is set by PaO2, pH, and PaCO2 according to the oxyhemoglobin dissociation curve; CaO2 can also be measured by oximetry:
CaO2 (ml/dl) = 1.34 (ml/dl/kg) x Hgb (g) x O2 sat + 0.003 (ml/dl/mmHg) x PaO2 (mmHg) Pulse Oximetry
Pulse oximeter – used to determine the oxygen saturation of the blood. Patients who are critically ill need monitoring of their oxygen levels. This can be placed on the earlobe, fingertips, as a patch.
- Continuous monitoring of O2 saturation - Cannot use to predict PaO2 - Cannot determine PaCO2
False low O2 saturation: - Hypotensive - Cold tip of finger
*If you request for a complete PFT, you should include a diffusion study. Diffusion study
DLCO - Single breath diffusing capacity - Uses small amount of CO2 (10 sec
breath hold) - Diffusion increase in increased surfaced
area available for diffusion, amount of hgb within the capillaries & inversely related to the thickness of alveolar membrane
- DLCO maybe increased in: o acute CHF, asthma,
polycythemia & pulmonary hemorrhage
- Diffusion decreases in: 1. Thickened/destroyed alveolar
membrane (pulmonary fibrosis, emphysema)
2. Problem in pulmonary vasculature (pulmonary hypertension)
3. Reduced alveolar capillary hemoglobin (anemia)
Diffusion is very efficient in the respiratory system. There is hardly any problem with diffusion.
Primary function of the lung: to oxygenate the blood and eliminate CO2
Needed for lung to function normally: - Normal perfusion - Normal ventilation - Normal diffusion

Disturbances of Respiratory Function
Love, bbf. Page 7
Causes of Arterial Hypoxemia
- Low inspired O2 tension = O2 tension is less than air inhaled ( < 20.9 or 21%.) This is true in high altitudes. Ex. Riding airplanes = O2 tension decreases
- Alveolar hypoventilation PaCO2 – reflects ventilation
↓ CO2 in blood = excessive ventilation ↑ CO2 in blood = lack ventilation
- V/Q mismatch
slight increase in ventilation – lack of oxygen Tx: increase O2 to improve condition
- Shunt blood does not come in contact with O2 no chance to improve
- Diffusion defect (the respiratory system has very good diffusing capacity so this is not considered)
Computation
- A – alveolar - a – arterial - P bar – barometric pressure - R – respiratory quotient (metabolism of
whatever you eat) - FiO2 – fraction of inhaled O2
PAO2 = 0.21 x (760 - 47) – 40 / 0.8 = 0.21 x 713 – 50 = 149.52 – 50 = 99.52 PAO2 = 0.21 x (760 – 47) – 60 / 0.8 = 0.21 x 713 – 75 = 149.52 – 75 = 74.52
Clinical Correlations
Ventilatory Restriction Due to Increased Elastic Recoil - Idiopathic Pulmonary Fibrosis
- ↓ TLC, FRC & RV - ↓ FEV1 - Normal/above normal FEV1/FVC - Normal airway resistance - Marked reduction of DLCO - Hypoxemia - Flow/volume loop like a miniature
normal loop
Ventilatory Restriction Due to Chest Wall Abnormality - Moderate Obesity
- ↓ FRC - Normal TLC & RV - Mild hypoxemia - Normal flow/volume curve - Normal DLCO

Disturbances of Respiratory Function
Love, bbf. Page 8
Ventilatory Restriction Due to Reduced Muscle Strength - Myasthenia Gravis
- Normal FRC - ↓ TLC & ↑ RV - Reduced FEV1 - Normal airway resistance & DLCO - Normal oxygenation unless weakness is
severe Airflow Obstruction Due to Decreased Airway Diameter - Acute Asthma
- Scooped flow-volume loop - Normal TLC - Elevated FRC & RV - Elevated airway resistance - Mild hypoxemia - Normal or mildly ↑ DLCO -
Airflow Obstruction Due to Decreased Elastic Recoil - Severe Emphysema
- Severe emphysema - ↑ lung volume - ↓ FVC & FEV1 - Airway resistance normal in pure
emphysema - Scooped flow-volume loop - ↓ DLCO