Dispatches (Winter 2004)
16
1999 Nobel Peace Prize Laureate Updates Remembering Rwanda Letters from Liberia Nepal: A Hospital at the Top of the World The Mechanics of Malnutrition FTAA: Trading Away Health MSF in Canada Canadians on Mission IN THIS ISSUE 1 4 6 8 10 12 14 16 The 1994 Rwandan genocide was a horrific event resulting in the deaths of some 800,000 Tutsis and moderate Hutus. As years go by, articles continue to diminish the estimated number of dead, as if the world is trying to forget this period of history that came so soon after it said "never again" with the Holocaust. Médecins Sans Frontières worked in Rwanda before, during and after the genocide and its brutality has personally affected all of the expatriates that worked in the troubled "Great Lakes" region of Central Africa. This April marks the 10th anniversary of the start of the genocide and I would like to take the opportunity to remember one MSF Rwandan staff member who was among many that perished that year because they were considered "inyenzi", the Kinyarwanda word for "cockroaches", by the extremist Hutus. (continued, on page 2) Dispatches Vol. 6, Ed.1 MSF CANADA NEWSLETTER REMEMBERING RWANDA
-
Upload
doctors-without-borders-medecins-sans-frontieres-msf-canada -
Category
Documents
-
view
228 -
download
2
description
Dispatches is the English-language newsletter of Doctors Without Borders / Médecins Sans Frontières (MSF) Canada.
Transcript of Dispatches (Winter 2004)
1 9 9 9 N o b e l P e a c e P r i z e L a u r e a t e
Updates
Remembering Rwanda
Letters fromLiberia
Nepal: A Hospitalat the Top ofthe World
The Mechanicsof Malnutrition
FTAA: TradingAway Health
MSF in Canada
Canadians on Mission
IN THIS ISSUE
1
4
6
8
10
12
14
16The 1994 Rwandan genocide was a horrificevent resulting in the deaths of some800,000 Tutsis and moderate Hutus. Asyears go by, articles continue to diminish theestimated number of dead, as if the world istrying to forget this period of history thatcame so soon after it said "never again" withthe Holocaust. Médecins Sans Frontièresworked in Rwanda before, during and afterthe genocide and its brutality has personally
affected all of the expatriates that worked inthe troubled "Great Lakes" region of CentralA f r i c a . T h i s A p r i l m a r k s t h e 1 0 t hanniversary of the start of the genocide andI would like to take the opportunity toremember one MSF Rwandan staff memberwho was among many that perished that yearbecause they were considered "inyenzi",the Kinyarwanda word for "cockroaches",by the extremist Hutus. (continued, on page 2)
DispatchesVol. 6, Ed.1
M S F C A N A D A N E W S L E T T E R
REMEMBERING RWANDA
9908_Dispatch Eng 1/22/04 2:17 PM Page 1

Dispatches Vol. 6, Ed.1
In the spring of 1992, I was preparing for my first visitto MSF projects in the field. This was my opportunityto see field workers in action, together with their localcounterparts, in addressing the health needs ofpopulations in danger. I was to visit Pierre LaPlante, anurse from Vancouver working in the tiny centralAfrican nation of Rwanda where war had left thousandsof people from the area bordering Uganda subsisting in"internally displaced camps". Pierre requested that Ibring him a number of items, including a Timex watch.
Rwanda’s lush beauty lived up to its tourism slogan,“pays des mille collines” or country of a thousandhills. I went to the Kigali office and met the team,and I remember meeting many Tutsi staff includingJean Nyiligira and his wife Odette (who also workedfor MSF) and their five children. Jean was Pierre'sdriver and over the next week touring around thenortheast of the country, I would learn that he wasmuch more than a chauffeur. Jean was fluent in threelanguages and a fully trained mechanic. The MSF
driver plays other roles: helping to keep the expatriatesafe by reading an often complex security situation;and act ing as a t ranslator, without which mostinternat ional MSF workers would be unable tofunction. While MSF sends some 3000 internationalworkers to over 80 countries each year, it is the workof another 15,000 national staff that makes theorganization effective in the field. It was remarkableto watch soft-spoken Jean walk through camps of tensof thousands of people - mostly Hutus displaced by aTutsi rebel incursion - and ensure that Pierre was ableto address basic health concerns for these people.
R w a n d a
Jean Nyiligira translating and mediating for Pierre LaPlante
“ Health defines a humane way of
pursuing life itself and is, without question,
the fundamental human right. "
Dr. James Orbinski, Former International
President, MSF October 1994
9908_Dispatch Eng 1/22/04 2:17 PM Page 2

The Timex watch was a gift to Jean from Pierre inappreciation of his outstanding work. Pierre describedJean as his guardian angel who had helped himnavigate some charged situations. I witnessed oneclose up. Just after nightfal l , we approached acheckpoint at the town of Byumba, hit by 18 rebelrockets just a few hours before. Despite carrying ahealth ministry off ic ial , two drunken soldiersstaggered out with a rocket-propel led grenadelauncher and a machine gun pointed at us asking for abribe. Jean negotiating with them allowed us to pass,I will never forget that night. The growing tension inKigali was palpable. I asked Jean, "What will you do ifth i s count r y exp lodes? " He ca lmly answered , " I ' l lattach myself to an expatriate and try to survive."
Less than two years later, the aircraft carry ingPresident Juvénal Habyarimana and his Burundiancounterpart was shot down and the genocide began.During those months of horror and insanity, I oftent h o u g h t a b o u t t h e s e R w a n d a n M S F w o r k e r s -especial ly Jean. There was no way of knowing whathad happened to them. Had Jean found anexpatr iate to shelter him? What had happened toOdette and the chi ldren?
In 1996, I had the chance to return to Kigali as hundredsof thousands of the Hutu refugees, sheltered in Zaire fortwo years, started to stream home. What had been a quietcity with a handful of aid organizations had now becomea gridlock of white humanitarian agency Land Cruisers. Itwas eerie to drive through streets where the Interhamwemilitias had manned checkpoints and machetedthousands to death. When I reached the MSF office, Iwas amazed to see the familiar face of Odette. Sheexplained that she and the children had found sanctuaryin the stadium and rode out the brutality. However, shewas a widow now. Jean had been caught in the streetsand never seen again.
It is strangely easy to become detached from thesuffering that surrounds you. But Jean was one of thefirst MSF workers that I had met and will occupy aspecial place in my memory. The genocide will never beabstract statistics to me. But the strangest thoughtthat I have had is, somewhere among the countlessHutus awaiting trial, one man is probably wearing aTimex watch that was given as a token of friendship buttaken after an act of indescribable terror.
Page 3
Ben Chapman,MSF Canada Board Member
“ When we got into Kigali, the airport
looked really modern, but all the glass was
broken… It was a modern looking place,
but no one around, nobody on the streets,
no cars. That was the front line, and
there was nobody there. ”
Sidne Maddison, MSF nurse part of
Dr. Orbinski’s team“In 1994, I was a doctor in Kigali, the capital of
Rwanda. I witnessed the unfolding of one of this
century’s great massacres, and I witnessed the
apathy of the international political community in its
unwillingness to respond adequately. I spoke out
with MSF as we called on the international
community including the members of the Security
Council to stop the genocide - a genocide cannot be
stopped by doctors.”
Dr. James Orbinski September 2003
Jean, Odette and 4 of their 5 children in the backyard of the MSF house in Kigali
9908_Dispatch Eng 1/22/04 2:17 PM Page 3

Dispatches Vol. 6, Ed.1
A m e r i c a s
?MEDICINES FOR ALL: STEP FORWARD, STEP BACKWARDS. TRADING AWAY HEALTH. IS THE AMERICAS NEXT?
9908_Dispatch Eng 1/22/04 2:17 PM Page 4

Still too many medicines missing from our medical kits
When MSF was created in the 1970s, our volunteer doctors lackedcertain medicines to treat patients. Today, despite medicaladvancements, not enough has changed. The cost of life-prolonginganti-retrovirals has dropped dramatically due to generic competitionyet the forgotten Chagas disease, which affects 25% of the populationin the Americas, still has no medicine to treat its chronic stage.
Along the Thai-Burma border malaria resistance is high, andinitially MSF doctors had largely ineffective anti-malarial drugs intheir medicine kits. Today, effective anti-malarials, like artemisinin-based combination therapy (ACT), exist and are in use in severalcountries. Yet, governments in countries such as Sudan and Indiarefuse to make ACT therapies for malaria the national standard. Asmedical humanitarians, it is unethical not to use medicines weknow are effective. Despite pressure not to in some countries, weuse ACT medicines and/or campaign to change protocols for use ofACT. In Burundi, where malaria epidemics are too common, thegovernment made the important national protocol change this yearbecause of MSF, NGO and national health workers’ pressure.
For treatable diseases such as HIV/AIDS, until recently, themedicines were simply out of reach for our patients because ofexorbitant prices. Today, only six percent of the 6 million people whocould benefit immediately from anti-retrovirals for HIV/AIDS havethem. It is unacceptable that people are still ‘too poor to cure’.
Monumental Doha Declaration:"Medicines for All"
In 1999, MSF launched the "Access to Essential MedicinesCampaign" – one goal was to examine how trade laws andintellectual property (IP) can ease or block access to medicines.We continuously refer to the landmark Doha Declaration in 2001at the World Trade Organization (WTO) meeting. In Qatar, 142WTO countries agreed they needed to protect public health overprivate commercial interests, and increase trade law flexibilities tohelp poor countries get the medicines they need. The declarationaffirmed a country’s sovereign right to decide what measures totake to override patents when necessary to protect public health.
Trading away healthSince the historic Doha Declaration, MSF has sadly observeddeveloped countries’ efforts to undermine Doha, slowlyintroducing bilateral and regional trade laws that introduce morestringent patent protection than at the WTO level. Access toaffordable medicines comes in part from flexibilities in trade laws.
The Free Trade Area of the Americas (FTAA), a proposed regionaltrade agreement between 34 countries in the WesternHemisphere, including all of North, Central and South America,
and the Caribbean, except Cuba concerns MSF. If implemented asplanned in 2005, it will be the largest "free trade zone" in the worldcovering more than 800 million people with the most stringentintellectual property provisions globally. Draft intellectual propertyprovisions within the FTAA Agreement threaten the positive pricingcompetition for affordable generic drug production.
MSF calls upon countries of the Americas to exclude intellectualproperty provisions from the FTAA Agreement altogether. Webelieve that the tougher intellectual property rules proposed in theFTAA Agreement will be bad for the health of the people in theAmericas and around the world.
Canada says it will "not go beyond Doha" in the FTAA, meaningthat they will not allow a regional trade agreement that imposesstricter intellectual property provisions that what Canada agreedto at the international level. MSF donors, advocacy and outreachgroups signed a petition urging regional governments, includingCanada, to maintain their commitment and be consistentnationally, regionally and internationally about patient rights overcommercial interests. For diseases know no borders either. Atthe 8th FTAA ministerial meeting in November 2003 in Miami,MSF met with trade negotiators and NGOs from the Americas.Latin American negotiators supported the MSF position butemphasized that they are negotiating under heavy pressure fromthe United States, implying that IP provisions could be includeddespite best efforts to exclude them. MSF will continue topressure governments in the Americas to avoid IP provisions inthe FTAA. A third FTAA draft is available for public viewing athttp://www.ictsd.org/issarea/Americas/FTAA_ministerial/miami/FTAADraft_Text_191103.pdf
Page 5
"Don’t trade away health with the FTAA.
Drugs should not be treated like any other
commodity… This will mean life or death for
people in Latin America." – Dr. Luis Villa,
MSF Head of Mission, Guatemala.
There are 1.9 million people living with
HIV/AIDS in Latin America and the
Caribbean, according to the World Health
Organization– the second most-affected
region in the world after Sub-Saharan Africa.
Carol Devine,
Access to Essential Medicines Campaign Liaison, MSF Canada?
9908_Dispatch Eng 1/22/04 2:17 PM Page 5
Dispatches Vol. 6,Ed.1
F i e l d L e t t e r
LETTERS FROM
LIBERIA
9908_Dispatch Eng 1/22/04 2:18 PM Page 6

Page 7
September 7, 2003
As I expected, the immediate surrounding is much calmer thanwhat’s on the news. The plane [is] piloted by three seeminglyinebriated pilots. The young chap seated next to me works forsome sort of supplier to NGOs, making money out of thehumanitarian crisis. Here in Liberia we landed. No problem. Thewelcome committee at the airport consisted of 16 trucks ofsoldiers (about 500 of them) with AK47s. That did not worry meexcept I don’t like the sight of the weapons…
The ex-pats’ quarters are actually the previous hospital, so ourrooms are large - some of them face the ocean. From the littlebalcony of the office, you can see the ocean with three Americanwar ships. Now and then, you have this low flying helicopter,gunships patrolling the area showing that they are in control.
September 14, 2003
I have already been here for more than a week and the workloadis quite overwhelming. Today is really the first opportunity I havehad, to sit down and write something, which is important as Ifear I am rapidly becoming desensitised to life around me…
The hospital was looted but it is still functioning even though thelocal hospital staff has not been paid for two years. The local medicalschool has been closed for more than a year, however, there is a 3rdyear medical student, called Fallah, day in day out, he came to theoperating room, offering to carry the patients and scrub for theoperations. [He] does everything from cleaning the floor to suturingthe wound. He then goes home and reads up about everything he hasseen. It is so easy to let go and feel despair in these circumstances,and yet, he refuses to give up. To me, this is truly inspirational!
17 September, 2003
I will be leaving Monrovia in just over a week. Amazing! In a way,I am getting very good experience. On the other hand, the healthcare here is very basic. People are dropping dead like flies andyet, we don’t know what they die of. There is no basicbiochemical test, there is no microbiological test, the x-ray isworking but produces very, very poor quality film. You simplydon’t know what you are treating…
I was doing all the emergency surgeries yesterday. It was like afactory. You can’t plan any elective cases if you are alone. It isfire fighting. Things just crash through the operating theatre door.
18 September, 2003
Today, the patient [Dr.] Juanita operated on last night, died.Nobody knows what went wrong. We waited for Steve for a while,as Steve was finishing his work at around 6 o'clock. It turnedthat he had been treating an 8-year-old girl who had beenrepeatedly raped. Poor child. How utterly disgusting!
Dr. Wei Cheng shares his experiences in Monrovia, capital of Liberia,with excerpts from e-mails written to his wife - Karin Moorhouse
Dr. Wei Cheng, a paediatric surgeon, was
sent on an emergency mission for three
weeks to L iber ia . He i s cur ren t l y in
Toronto, Ontario working as a medical
researcher for The Hospital for Sick Children.
9908_Dispatch Eng 1/22/04 2:18 PM Page 7

“ Broken equipment, obsolete surgicalequipment were piled up in many rooms.
We had to get rid of all that. ”
Dispatches Vol. 6, Ed.1
N e p a l
9908_Dispatch Eng 1/22/04 2:18 PM Page 8

N e s t l e d i n t h e v a l l e y a t t h e f o o t o f t h e N e p a l e s e m o u n t a i n s , t h e R u k u m H o s p i t a l w a s
i n g r e a t n e e d o f m a j o r l o g i s t i c a l a n d m e d i c a l s u p p o r t . K a t h r y n R o b e r t s , a y o u n g
p a e d i a t r i c i a n , s p o k e t o u s a b o u t t h e t i m e s h e s p e n t i n a p r o j e c t o n t o p o f t h e w o r l d .
"It was my first mission with MSF," smiles Dr. Roberts, ayoung doctor who spent five months at the Rukum Hospitalin Rukum, Nepal. In the western part of the country, in aregion between the government zone and the mountainscontrolled by the Maoist guerrillas, the Rukum district ishome to approximately 200,000 people. "It’s a rural regiondotted with highly isolated villages. Often patients mustwalk for two days to get to a hospital." Another particularity:at the foot of the Himalayas the diseases are not the sameas in the tropical regions. "We’re lucky; we’re too high up forthe mosquitoes so there is no malaria. However, we had totreat many cases of pneumonia in children."
Ambulances on the backs of men
In this very steep landscape, falls are common. A young boywas brought to the hospital after falling from a tree, andthen onto rocks—a total fall of eight metres. Transported onthe back of a man in a large basket, the child had lost a lotof blood by the time he reached the hospital. "He hadcompletely broken his nose and had a hole in his palate. Hehad to be stabilized before we could rush him to a modernhospital in Kathmandu, the capital," Dr. Roberts recounts. Afew weeks later, the child returned, fully healed. "I saw hismother, his three little sisters and him, in their best clothes,really happy, really appreciative. I believe that this will beone of my fondest memories."
No glass panes at 1,800 metres
"Along with medical activities, logistics helped uscompletely renovate the hospital, which first needed athorough cleaning. Broken equipment, obsolete surgicalequipment were piled up in many rooms. We had to get ridof all that," Dr. Roberts explained. Her team went aheadwith more daunting work. "We had to put glass in thewindows. Until our arrival, there were only wooden shutters.Can you imagine winter at 1,800 metres? You had the
choice of either freezing or staying in the dark. When you’resick, neither of these solutions are really acceptable." Other,more costly work carried out was restoration of thepharmacy to its original condition as well as the X-raymachine. Then the cleaning teams had to be trained torespect basic hygiene rules needed in the hospital.
During her five months in the field, Dr. Roberts sawmany changes including political ones. "I arrived onJanuary 30, 2003, the day the cease-fire was signedbetween the Nepalese government and Maoist rebels.The military situation remained calm until I left at theend of June, when new tensions arose." With therenewed political problems, MSF decided to wait a littlelonger before determining which dispensaries, in themountains around Rukum, needed the most medical andlogistical help. That is the next objective of the newMSF team in Nepal despite the growing tensionsbetween the government and the rebels. As for Dr.Roberts, she is now hard at work in Sierra Leone.
Page 9
Laurence Hughes
RUKUM: A HOSPITAL AT THE TOP OF THE WORLD
In April 2003, MSF initiated a second program,
in Nepal’s Jumla district, to address
psycho-social health and basic health care
needs for the 100,000 people living in the
northwestern district, where health care is of
poor quality and often unaffordable. Many
people in the region were traumatized in
November 2002 by the battle in Jumla town,
when 10,000 Maoist rebels attacked the city
and killed approximately 400 people.
9908_Dispatch Eng 1/22/04 2:18 PM Page 9

Dispatches Vol. 6, Ed.1
A n g o l a
THE MECHANICSOF
MALNUTRITION
9908_Dispatch Eng 1/22/04 2:19 PM Page 10

How Can You Die of Hunger?
Malnourished, undernourished, dying of hunger - theseexpressions are far from our daily reality. A strict diet ora day of fasting are the only experiences to which wecan relate when we try to understand what these wordsreally mean, but it’s only a poor approximation.
What Happens in the Body
This vicious circle begins when there is not enough ornothing to eat. Lack of food means a major loss of energy,leading to immense fatigue. Little by little, the personbecomes apathetic, wanting less and less contact with theoutside world. He no longer has the strength to move, talkor even eat. Moreover, this deprivation causes the stomachto waste away and lose its ability to accept large quantitiesof food. All hunger regulatory mechanisms such as hungerpangs, or, conversely, the feeling of fullness, which arecontrolled by gastric volume, will wane. The person is nolonger hungry or thirsty. Malnourished children are soweak that they no longer want something to drink and areconsequently very dehydrated.
Suffering and Weakness
Although the extreme weakness brought on by malnutritionentails inhibited desire and apathy, it does nothing to dull thesuffering. Children—and adults—suffer with every move, sincetheir muscles have withered. This pain is also due to the factthat the skin is cracking from extreme tissue dehydration.These people, ever more fragile from malnutrition, cantherefore catch all sorts of diseases, which results in furthersuffering. For example, it is common for yeast to developalong the esophagus. Swallowing becomes a painful feat,likened to eating a lemon with a mouth full of ulcers.
Renutrition: A Medical Issue
Feeding a malnourished child must be done very carefullysince, if not done correctly, the child could die. Theobjective is to feed the body in small amounts, but ingest asmany calories as possible, since the shrunken stomachcannot take much. Malnutrition makes the entire humanbody fragile: digestive system, kidneys, liver, heart… Thebody must be gradually returned to its normal level offunctioning. Feeding a child in this situation too much ortoo quickly can overload already fragile systems, causing thebody to shut down, such as with a heart attack. As well, thechild should be immediately rehydrated, treated formalnutrition-induced opportunistic disease and vaccinated.
Immediate Results
Supplementary feeding centres treat moderatelymalnourished children, whereas therapeutic feedingcentres take care of severely malnourished children.
"A child almost immediately starts putting back on weightthere. They quickly return to life and start playing and singingas though nothing had happened. It’s like magic!" explains aphysician who has worked at several nutritional centres.
Page 11
Forms of Malnutrition
The two main forms o f malnut r i t ion -
Marasmus and Kwashiorkor - are equally
dangerous, painful and fatal.
Marasmus: People suffering from Marasmus
are extremely thin. Without nutr i t ion,
required to maintain vital functions, such
as respiration and cardiac activity, the body
must take energy from the reserves in the
muscles and fat. This especially affects
children since their muscle and fat mass is
far lower than that of an adult.
Kwash io rko r : Peop le su f fe r ing f rom
Kwashiorkor are swollen from oedema. In
this case, the body uses its own resources
to control all its functions, especially cellu-
lar homeostasis. Water, from the cells,
moves into the body resulting in oedema or
pockets of water. The skin of those affected
is extremely dehydrated, cracks under
pressure and forms characteristic ulcers.
It is not known why certain regions are
more prone to Kwashiorkor and others to
Marasmus. In Angola, Kwashiorkor is the
predominate form of malnutrition.
9908_Dispatch Eng 1/22/04 2:19 PM Page 11

ARJAN STILL ALIVE 16 MONTHSAFTER ABDUCTION
U p d a t e s
Dispatches Vol. 6, Ed.1
Arjan Erkel, MSF head of mission in Dagestan was kidnapped August 12, 2002. Russian
authorities last provided proof that Arjan is still alive to the MSF on July 30, 2003. Dr.
Morten Rostrup, MSF International Council President urged the European Parliament to
call on the Russian authorities to step up efforts in finding Arjan and to hold the Russian
President Vladimir Putin accountable for securing his safe release after more than a year
of "unbearable captivity." Arjan Erkel is today the only foreign humanitarian worker hostage
in the Caucasus. Independent humanitarian efforts are stymied in this unstable and
insecure region, which has suffered through more than a decade of conflict, making it
difficult to deliver effective assistance to the thousands who need it. Several Canadian and
American authors have joined our petition to release Arjan, including John Irving, Margaret
Atwood, Michael Ondaatje, Graeme Gibson, Karen Connelly, Ronald Wright, and many others.
9908_Dispatch Eng 1/22/04 2:19 PM Page 12
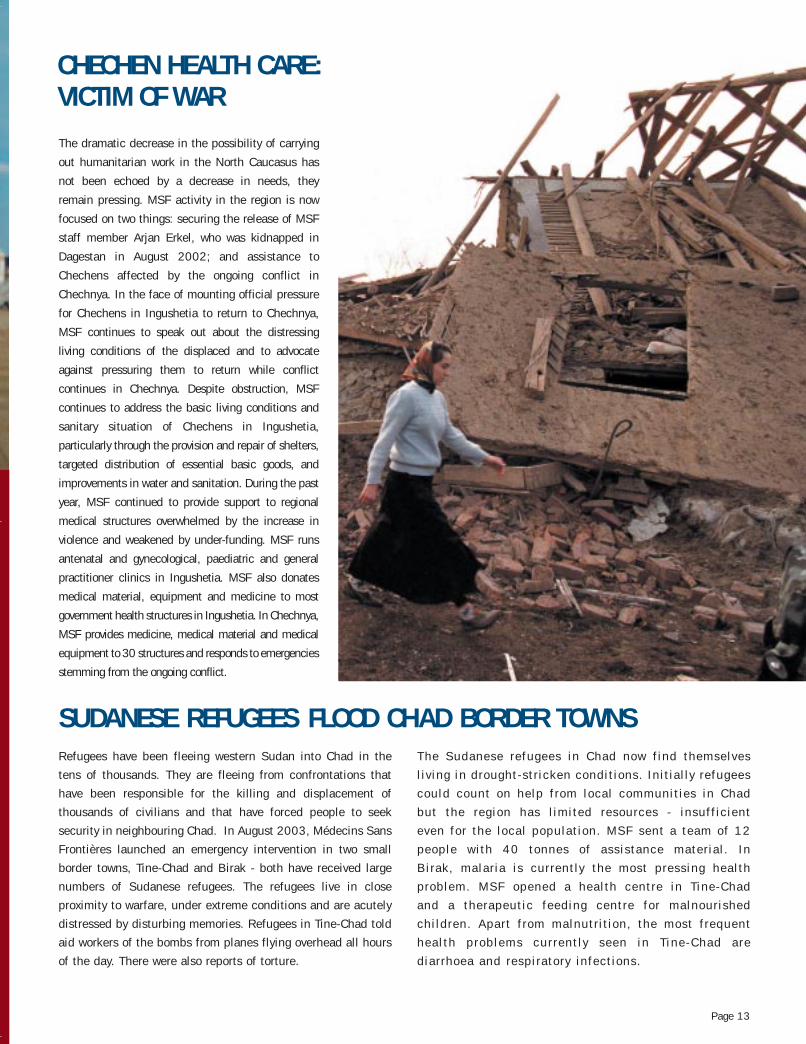
The dramatic decrease in the possibility of carrying
out humanitarian work in the North Caucasus has
not been echoed by a decrease in needs, they
remain pressing. MSF activity in the region is now
focused on two things: securing the release of MSF
staff member Arjan Erkel, who was kidnapped in
Dagestan in August 2002; and assistance to
Chechens affected by the ongoing conflict in
Chechnya. In the face of mounting official pressure
for Chechens in Ingushetia to return to Chechnya,
MSF continues to speak out about the distressing
living conditions of the displaced and to advocate
against pressuring them to return while conflict
continues in Chechnya. Despite obstruction, MSF
continues to address the basic living conditions and
sanitary situation of Chechens in Ingushetia,
particularly through the provision and repair of shelters,
targeted distribution of essential basic goods, and
improvements in water and sanitation. During the past
year, MSF continued to provide support to regional
medical structures overwhelmed by the increase in
violence and weakened by under-funding. MSF runs
antenatal and gynecological, paediatric and general
practitioner clinics in Ingushetia. MSF also donates
medical material, equipment and medicine to most
government health structures in Ingushetia. In Chechnya,
MSF provides medicine, medical material and medical
equipment to 30 structures and responds to emergencies
stemming from the ongoing conflict.
Refugees have been fleeing western Sudan into Chad in the
tens of thousands. They are fleeing from confrontations that
have been responsible for the killing and displacement of
thousands of civilians and that have forced people to seek
security in neighbouring Chad. In August 2003, Médecins Sans
Frontières launched an emergency intervention in two small
border towns, Tine-Chad and Birak - both have received large
numbers of Sudanese refugees. The refugees live in close
proximity to warfare, under extreme conditions and are acutely
distressed by disturbing memories. Refugees in Tine-Chad told
aid workers of the bombs from planes flying overhead all hours
of the day. There were also reports of torture.
The Sudanese refugees in Chad now find themselves
living in drought-stricken conditions. Initially refugees
could count on help from local communities in Chad
but the region has limited resources - insufficient
even for the local population. MSF sent a team of 12
people with 40 tonnes of assistance material. In
Birak, malaria is currently the most pressing health
problem. MSF opened a health centre in Tine-Chad
and a therapeutic feeding centre for malnourished
children. Apart from malnutrition, the most frequent
health problems currently seen in Tine-Chad are
diarrhoea and respiratory infections.
Page 13
SUDANESE REFUGEES FLOOD CHAD BORDER TOWNS
CHECHEN HEALTH CARE: VICTIM OF WAR
9908_Dispatch Eng 1/22/04 2:19 PM Page 13
M S F C a n a d a N e w s
Dispatches Vol. 6, Ed.1
1. ‘ The Right of First Refusal ’ provision:This provision gives a patented pharmaceutical companythe right to take over contracts initially negotiated by ageneric pharmaceutical company with a developingcountry government. This deal would secure a lowerprice on a particular medicine for the developing countrybut would soon discourage generic manufacturers fromnegotiating future contracts because the patent-holderscould repeatedly block the generic manufacturer. Thisflaw is the most serious and could undo all otherpositive aspects of the proposed amendment. Thedramatic drop in medication prices, due to genericcompetition, has been vital in saving lives.
2. Limited list of pharmaceutical products:The bill includes a list of Canadian patented medicinesthat can be produced as generics. MSF is concerned aboutthis limited list of medicines because no system currentlyexists to update the list efficiently. Therefore a medicinerequired to treat an infectious disease affecting people in adeveloping country but is not included on this list, may notbe produced generically in Canada.
3. A limited list of countries allowed toimport generic medicines:
Bill C-56 has a list of countries recognized by the UnitedNations as "least-developed countries" that may benefitfrom generic medicines from Canada. However otherdeveloping countries not on this list (such as Viet Nam,Turkmenistan) cannot import generic pharmaceuticals fromCanada, even though they express a clear need for them.
4. Non-governmental representatives are not allowed to buy generic medicines:
Currently, Bi l l C-56 only al lows a government of adeveloping country - or an agent of that government- to enter into a contract with a Canadian genericmanufacturer. Non-governmental organizat ions, l ikeMSF, a re no t ' agen ts ' o f gove rnment and a retherefore not, by def init ion, permitted to contractgeneric companies to import generic medicines. ForMSF, this means that we must st i l l re ly on the wi l lof governments to obtain much needed cheapergeneric medicines.
Bill C-56 has gone for further committee review and should be passed as law, with corrections, with Prime Minister Paul Martinin office. This should produce a bill that would truly benefit those who need it most: our patients in developing countries.
In September 2003, Stephen Lewis, the UN Special Envoy to Afr ica for HIV/AIDS, asked the Canadiangovernment to show global leadership by introducing legislation to al low the production of generic medicinesfor HIV/AIDS. Though Bil l C-56 has not been passed there remain four serious f laws. These include:
BILL C-56: A “WAIT AND SEE” ACT?
Isabelle Jeanson
MSF staff stage “street hockey” theatre to raise public awareness of Bill C-56.
9908_Dispatch Eng 1/22/04 2:19 PM Page 14

In November 2003, MSF Canada had 137 volunteers out in the
field, surpassing the 2002 year-end total of 116. Though con-
siderably beyond forecasted numbers, the increase can be attrib-
uted to the growing number of emergencies worldwide. Most
Canadian field volunteers were posted to the Middle East and
Africa - regions with acute emergencies like the crisis in Iraq and
chronic emergencies such as the famine situation in Ethiopia.
Our field volunteers are often bilingual and able to get
to the field quickly. Many go to fill management roles
in the field and French speakers are needed especially
in West and Central Africa: Democratic Republic of
Congo, Ivory Coast, Burundi and Congo Brazzaville.
MSF Canada has shifted its structure and focused more on
recruitment from coast to coast. This was achieved by reorganiz-
ing the human resources department and refocusing recruitment
efforts. The bumper year of field volunteers included the most
first mission volunteers from all over Canada - divided equally
between Western and Central Canada regions and Quebec. MSF
is becoming active in the wider medical community – medical
schools, professional conferences – to recruit more doctors.
Paramedical recruiting for lab technicians, mid-wives, and
nurses also continues but medical specialists in HIV, TB and
infectious diseases are desperately needed. Also, mental health
specialists need to be recruited to treat the people affected by
wars, the people who end up being victims of violence and abuse.
Reshmi Kutty
2003 - A RECRUITMENT SUCCESS STORY
MSF recently published Civilians Under Fire, a collection ofarticles that looks introspectively and self-critically at MSF’soperations during 1998 to 2000, an acute phase of the civil warthat devastated the Republic of Congo (better known as Congo-Brazzaville). The publication sheds light on some of theimportant ethical, medical and practical considerations thatarise when organizations such as MSF make the decision toprovide assistance to victims of rape, a category of victims thatis often overlooked by humanitarian organizations.
The writers also ask the question: "What is an effectivehumanitarian aid operation?" answered by an exploration of thequality of aid, its complexities and its vital importance for peopleaffected by conflict and crisis. Civilians, more than soldiers orguerrilla fighters, bore the overwhelming brunt of the death toll,loss and suffering. The acts of violence against them—rangingfrom forced displacement to summary executions, rape, looting,denial of food, and use as "human shields"— were boundless. Thisbook describes how MSF teams were faced with a medical andnutritional emergency of staggering proportions and how theinternational media paid little notice to the catastrophe when thestruggle for political power was playing itself out alonggeographical and ethnic lines and control over the civilianpopulation became a central objective.
CIVILIANS UNDER FIREMSF examines its actions in Congo-Brazzaville
Page 15
M S F R e a d s
9908_Dispatch Eng 1/22/04 2:20 PM Page 15
DispatchesMédecins Sans Frontières/
Doctors Without Borders
720 Spadina Avenue, Suite 402Toronto, Ontario, M5S 2T9
Tel: 416.964.0619Fax:416.963.8707
www.msf.ca
Editors:Reshmi Kutty
Dominique Desrochers
Editorial Director:Tommi Laulajainen
Contributors: Ben Chapman, Carol Devine, Laurence
Hughes, Isabelle Jeanson, Reshmi Kutty
Circulation: 65,000Design: One Company
Printing: Warren's Imaging andDryography
Winter 2004
Photo Credits: Remco Bohle, Alain Frilet, Roger Job, Olivier Jobard/SIPA Press, Jim Lavery, Jehad Nga/Corbis, John Reardon, Andrew Schechtman, Stephan Vanfleteren
CANADIANS ON MISSIONAfghanistanAlexandra ConseilAnu SharmaDavid CroftJudy McConneryKathleen BochslerMike FarkAngolaDanielle MorinGabriela PahlHélène PoliquinPhilippe BlackburnBangladeshViolet BaronBurundiBruce LampardChristopher CarterClaude TrépanierClive StraussDominique ProteauErin CulleyFrancine BelisleJason PeatKyra AbbottMichelle MilneYves CantinChadAndré FortinCaroline TourignyClea KahnDolores Ladouceur
Patrice RichardPhilipe MougeotRandy BarehamCongo-BrazzavilleClaudette ChayerFrédéric BeaudoinJennifer WeteringsLindsay BrysonSerena KasparianTammy HinscheDemocratic Republicof CongoDavid TuHeather ThomsonJosée PepinJulienne TurcottePatricia SimpsonReine LebelSophie-G. GagnonThomas KelleyEthiopiaAnders LonnqvistCheryl McDermidIsabelle AubryMichel PlouffeRik NagelkerkeSelig WilanskyGuineaMichel ParadisIndiaJames SquierIranYvan Marquis
Ivory CoastAlain CalameJangh Bhadur RaiJon SoehlJulia PuttergillVanessa Van SchoorJordanTheo MurphyKenyaChristina CepuchDenis GuzziFrançoise GoutierLiberiaJ-Sébastien MatteMarie SkinniderMaya HarariSylvain GroulxMauritaniaMarisa CutroneMyanmar (Burma)Stephanie FaubertPaul MathersNepalRobert ParkerNigeriaJoanne LiuNicole FultonNorth SudanLia CopelandPakistanPatrick Robitaille
Palestinian TerritoriesLynne ChobotarRussiaBen ReentovichÉric TremblaySierra LeoneDarryl StellmachKevin CoppockSomaliaJody ThomasMario FortinNicola WoolleySharon JanzenSylvain DeslippesSouth SudanDavid MichalskiJanice KopinakMarie-H. MayrandNancy DaleSteve DennisTiffany MooreSri LankaAdam ChildsBree LenzDoug Kittle
Current MSF Missions
ISSN 1484-9372
9908_Dispatch Eng 1/22/04 2:20 PM Page 16