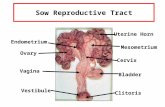
Role of Vangl2 in Female Reproductive Tract Development, 2008
Upload
rhoda-morrisCategory
view
223download
4
Disorders of the Female Reproductive
Tract (4)Infectious
Inflammatory
Structural

I. Infections of Reproductive Tract – Simple Vaginitis (Etiology) Common vaginal infection
T. vaginalis (staph or strep) Candidiasis albicans (vaginal yeast infection) Gardnerella bacillus
Inflammation of the vagina Exam of vagina shows
Bubbly or foamy exudate (T. vaginalis ) Thick cheese-like exudate (Candidiasis albicans) Bacterial vaginitis produces a malodorous milk-like
discharge

Simple Vaginitis (S/sx; Dx Tests) Vaginal exudate curd-like; yellow, white or
grayish-white Accompanied by pruritis, burning & edema
Visual exam C/S of organism Bimanual exam

Simple Vaginitis (Med Mgmt) Goals:
Cure the infection Prevent infection Prevent complications Prevent infection of partner(s)
Douching Vaginal suppositories

Simple Vaginitis (NI/Education) Application of heat Sitz bath No frequent douching Educate re: how to insert vaginal creams,
ointments, suppository Abstain from sexual intercourse until OK’d
by MD

B. Senile (Atrophic) Vaginitis Occurs in post-menopausal women as they
age Cause: levels of estrogen Leading to: atrophy of vulva & vagina Exudate causes: pruritis, edema & skin
irritation Rx: Estrogen, vaginal troche, ointments

C. PID (Pelvic Inflammatory Disease) – Etiology
PID is any acute, subacute, recurrent or chronic infection: Cervicitis Endometriosis Salpingitis Oophoritis
Causative organisms: Gonorrhea, Strep, Staph, Clamydia

C. PID – Etiology (con’t) Can occur following any procedure which
causes irritation, alteration or destruction of cervical mucus allowing bacteria to enter the uterine cavity
Some examples: F/C insertion, bx curette, pelvic surgery, sex, infection during pregnancy
Pelvic exams become extremely painful

C. PID – Etiology (con’t) Very serious condition May cause adhesions & sterility Those having more than 1 partner are @
risk for PID

C. PID – (S/sx) Hyperthermia Chills Severe abdominal pain N/V **Malodorous purulent vaginal exudate**

C. PID – (Dx Tests) Gram stain of exudate from endocervix,
urethra, rectum C/S to ID the organism Laparoscopy Vaginal ultrasound to ID abscesses Leukocyte count & ESR to confirm
presence of infection

C. PID – Med Mgmt Goal
Control & eradicate infection Prevent it from spreading to other body parts
Treatment Systemic antibiotics

C. PID – NI Follow medical plan of treatment Monitor VS & progress Encourage fluids to prevent dehydration Palliative measures for comfort
Personal hygiene & warm douches **Position in Fowler’s position**

C. PID – Education Contact MD for low-grade fever or purulent
vaginal drainage Understand the significance of PID Being compliant Good handwashing technique Avoid tampons Change peripads @ least q4h & prn

C. PID – Education (con’t) Clean clothing Sexual partner needs to be examined Painful intercourse with PID diagnosis No sex until OK’d by MD

D. Toxic Shock Syndrome (TSS) Etiology
An acute bacterial infection in menstruating women
Caused by Staph aureus Using super absorbent tampons left in
place too long Bacteria proliferate & release toxins into the
blood stream

D. TSS – Etiology (con’t) Women @ greatest risk
Inserting tampons with fingers Those with chronic vaginal infections Women with genital herpes
Sometimes occurs in non-menstruating women

D. TSS – S/sx Flu-like sx X 24 h Temp of 102 F (day 2-4 of menses) Vomiting Diarrhea Myalgia BP S/sx of onset of septic shock

D. TSS – S/sx (con’t) Sore throat HA **Red macular palmar or diffuse rash
followed by desquamation of skin, hands, feet may develop**
urinary output BUN

D. TSS – S/sx (con’t) Disorientation
Dehydration Release of toxins
Pulmonary edema Why? Inflammation of mucous membranes Why?

D. TSS – Dx Tests No definitive tests Cervical-vaginal cultures out S. aureus Leukocytosis Thrombocytopenia ( platelet count) BUN, bilirubin, ALT, AST, CPK Blood, urine & throat cultures, prn

D. TSS – Med Mgmt Treatment depends on severity Anti-bx therapy IV therapy Labs to evaluate for
Electrolyte imbalance Renal involvement Liver dysfunction

D. TSS – NI If hospitalized:
Bed rest Antibiotics
Close monitoring for: VS F&E status Respiratory compromise

D. TSS – Education DO NOT use super-absorbent tampons Use tampons with inserter only Alternate tampons with pads Use pads @ night Change pads or tampons q4h Good hand hygiene & perform frequently If sudden high fever w/ diarrhea & nausea, notify
MD immediately

II. Structural AbnormalitiesA. Endometriosis – Etiology
Definition: endometrial tissue appears outside the uterus (See Figure 12-10 AHN)
Can be found anywhere Reproductive organs Abdominal cavity
Possible spread via lymphatic system

Endometriosis – S/sx Lower & pelvic pain; w/ or w/o rectal pain Unilateral or bilateral pain; may radiate down legs More acute during menses May be familial Late childbearers Pregnancy may cure as it interrupts cycle Infertility is a complication

Endometriosis – Dx
Laparoscopy with bx of lesions Regular pelvic exams to monitor
progression
What else do you want to monitor ?

Endometriosis – Medical Mgmt High dose antiovulatory Rx Why? Synthetic androgens (Danazol) to stop
proliferation of endometrium & prevent ovulation
Surgery Laparoscopy Lasers for vaporization Hysterectomy

Endometriosis – NI
Reinforce MD orders & explanation Regular checkups important Report abnormal vaginal bleeding Encourage venting Pain-relieving techniques Verbalizing sexual dysfunction – infertility &
painful intercourse

B. Vaginal Fistula – Etiology Fistula – abnormal opening between 2
organs Caused by ulcerating process d/t:
CA Radiation Pregnancy causes weakness Surgical interventions

Vaginal Fistula – Etiology (con’t)
Types of fistulas & the 2 organs involved
Urethrovaginal –urethra & vagina Vesicovaginal – bladder & vagina Rectovaginal – rectum & vagina

Vaginal Fistula – S/sx Identified by type of exudate & odor (urine
or feces) Bladder infection is present Vesicovaginal constant trickle of urine
into vagina Rectovaginal feces & flatus enter the
vagina

Vaginal Fistula – Dx Tests Methylene blue instillation into the bladder IVP Cystoscopy Pelvic exam

Vaginal Fistula – Med Mgmt Vitamin C (ascorbic acid) Diet in Pro Surgery depends on type of fistula
A&P repair (discussed later) May require diversion, urinary or fecal

Vaginal Fistula – NI Sitz baths Deodorizing douches Peripads Protective undergarments F/C for surgical information Protect skin integrity Sexual dysfunction issues

C. Relaxed Pelvic Muscles
Displaced uterus Usually congenital or d/t childbirth Backward displacement
Retroversion – cervix normal; uterine body pointed toward sacrum
Retroflexion – uterine body is on vagina

Displaced Uterus (con’t) S/sx: backache, muscle strain, leukorrheal
discharge, pelvic area heaviness, tires easily
Treatment: Pessary Uterine suspension

Uterine Prolapse (See Figure 12-12) – Etiology
1st degree – prolapse of the uterus through pelvic floor & vaginal outlet
2nd degree – cervix protrudes through vaginal interoitus
3rd degree – entire uterus protrudes through the interoitus (procidentia)

Uterine Prolapse – Etiology (con’t)
Contributing factors OB trauma Overstretching of the uterine musculature Coughing Straining Heavy lifting

Uterine Prolapse – S/sx c/o feeling “something coming down/out” Dyspareunia (dragging/heavy feeling in
pelvis) Backache B & B problems, prn cystocele or rectocele Stress incontinence 2nd or 3rd, protruding cervix & vaginal wall
subject to constant irritation

Uterine Prolapse – Med Mgmt
Surgery Vaginal hysterectomy with A&P of the vagina &
fascia AKA anteroposterior colporrhapy (suturing of the
vagina)
If surgery contraindicated, a pessary is used to correct the prolapse (not intended for long periods of time)

Uterine Prolapse – NI
F/U appointments with MD to check for Irritation
If worn too long may cause Erosion Fistulas Vaginal CA

Cystocele & Rectocele – Etiology Supporting musculature for uterus &
perineum overstretched & weakened by Childbearing Multiple births Cervical tears
Can cause displacement of organs/tissues Relaxation of bladder muscles causes a
displacement of bladder

Cystocele & Rectocele – S/sxCystocele
Urgency, frequency & incontinence
Fatigue Pelvic pressure Incomplete bladder
emptying UTI
Rectocele Relaxation of rectal-
supporting muscles Constipation Rectal pressure Heaviness Hemorrhoids

Cystocele & Rectocele – Med Mgmt
Surgical correction of cystocele & rectocele AKA
A&P repair A P colporrhapy

Cystocele & Rectocele – NI Pre-op/post-op teaching Cathartic, then cleansing enemas ‘til clear Cleansing vaginal douche Liquid diet 48 hr before surgery Routine post-op NI F/C Early ambulation No sex X 6 weeks

D. Benign Uterine Tumors – Etiology (fibroids)
Most common benign tumors (AKA fibroids) Pressure from enlarging mass Dysmenorrhea Abnormal uterine bleeding Menorrhagia w/ menses Backache Constipation Urinary symptoms

Fibroids – Dx Tests Pregnancy test D&C Laparoscopy Ultrasonography Hysterectomy Myomectomy

Fibroids – Med Mgmt Depends on
Severity of sx & patient age How near to menopause If additional children are desired
Myomectomy during childbearing years Hysterectomy if severe or obstruction or
close to menopause

Fibroids – NI Pre-&-post-op NI for hysterectomy Reinforce MD’s orders Pelvic exams @ regular intervals Rx: SE, uses, how to take Menorrhagia – diet in Fe-rich foods;
FeSO4
Rarely malignant