
DISORDERS AND TREATMENT Review Session 10. What is Abnormal? Common characteristics 1) It is...
41
DISORDERS AND TREATMENT Review Session 10
-
Upload
alison-morton -
Category
Documents
-
view
215 -
download
1
Transcript of DISORDERS AND TREATMENT Review Session 10. What is Abnormal? Common characteristics 1) It is...
DISORDERS AND TREATMENT
Review Session 10
What is Abnormal?
Common characteristics 1) It is maladaptive (harmful) and
disturbing to the individual Agoraphobia- afraid of public places do unable
to leave home 2) It is disturbing to others
Zoophilia- sexually aroused by animals 3) It is unusual; based on culture!
Seeing visions 4) It is irrational
Depressed when your family moves- rational

The DSM-IV
Insane-not a medical term but a legal term

Causes by Perspective

Categories of Disorders
6 Categories Anxiety Somatoform Dissociative Mood/Affective Schizophrenic personality

Anxiety Disorders- Phobias
Specific Phobia Intense unwarranted fear of a situation or
object Claustrophobia, Arachnophobia, etc.
Agoraphobia a fear of open, public spaces
Social Phobia fear of embarrassing oneself in public
Contact with the feared object or situation results in anxiety
Anxiety Disorders
Generalized Anxiety Disorder (GAD) Constant, low level anxiety Constantly feels nervous and our of sorts
Panic Disorder Acute episodes of intense anxiety without
any provocation Often suffer anxiety due to anticipating
the attacks
Anxiety Disorders
Obsessive-Compulsive Disorder (OCD) Persistent, unwanted thoughts- obsessions Feeling the need to engage in a particular
action- compulsions Obsessions result in anxiety that is reduced
when the compulsive behavior is performed Post-Traumatic Stress Disorder (PTSD)
Flashbacks or nightmares following a person’s involvement in or observation of an extremely troubled event (wars, disasters, etc.)
Memories cause anxiety

Causes of Anxiety Disorders

Somatoform Disorders
A person manifests a psychological problem through a physiological symptom Physical problem without a physical cause
Hypochondriasis Frequent physical complaints with no medical
cause May believe minor problems are severe physical
illness Conversion Disorder
Report a severe physical problem such as paralysis or blindness with no physical reason

Causes of Somatoform Disorders

Dissociative Disorders
Involve a disruption in conscious processes Psychogenic Amnesia
When a person cannot remember things for no physiological reason
Psychogenic Fugue Not only have psychogenic amnesia but also find
themselves in an unfamiliar environment Dissociative Identity Disorder (Multiple
Personalities) A person has several personalities rather than one
integrated personality Personalities may have different ages, sexes Commonly have a history of sexual abuse or
childhood trauma

Causes of Dissociative Disorders

Mood or Affective Disorders
Major Depression Most common Remain unhappy for more than two weeks
with no clear reason Loss of appetite, fatigue, sleep changes,
feeling worthless Seasonal Affective Disorder (SAD)
Only depressed during certain types of year Use of phototherapy

Mood or Affective Disorders
Bipolar Disorder Manic Depression- involves both depressed
and manic episodes Depressed- depression symptoms Manic- feelings of high energy
Some have a heightened sense of confidence and power, others just feel anxious and irritable
Usually engage in risky behavior
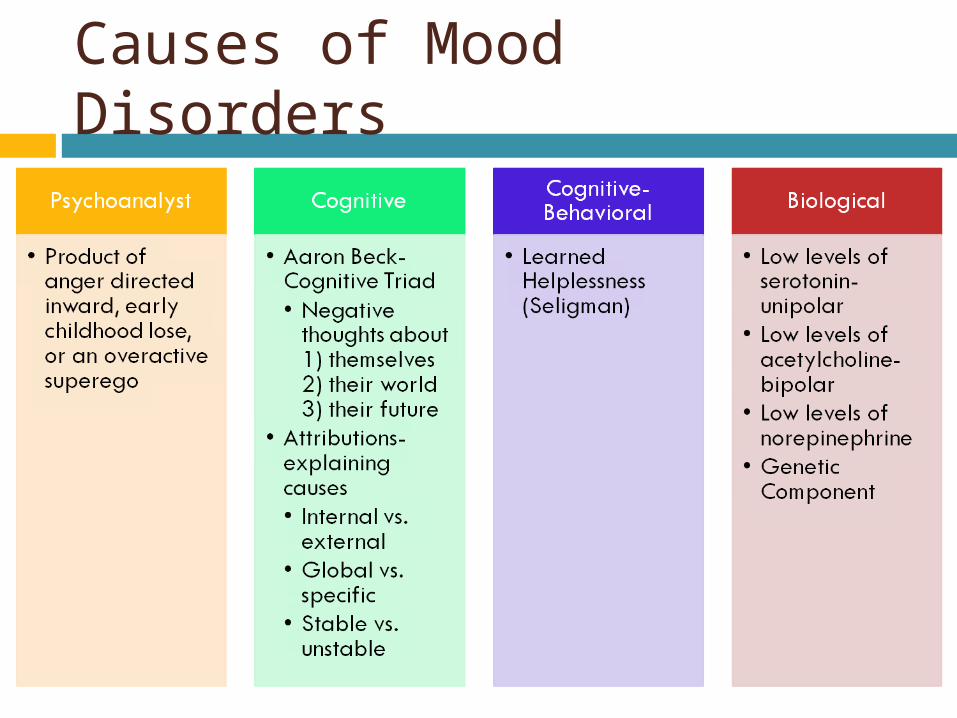
Causes of Mood Disorders

Schizophrenic Disorders
Tends to strike people as young adults Disordered, distorted thinking often demonstrated
through delusions and hallucinations Delusions- beliefs that have no basis in reality
Delusions of persecution- believing people are out to get you
Delusions of grandeur- belief that you enjoy greater power and influence than you do
Hallucinations- perceptions in the absence of any sensory stimulation
Schizophrenics DO NOT have split personalities Positive Symptoms- excesses of behavior Negative Symptoms- correspond to deficits of
behavior

Types of Schizophrenia

Causes of Schizophrenic Disorders
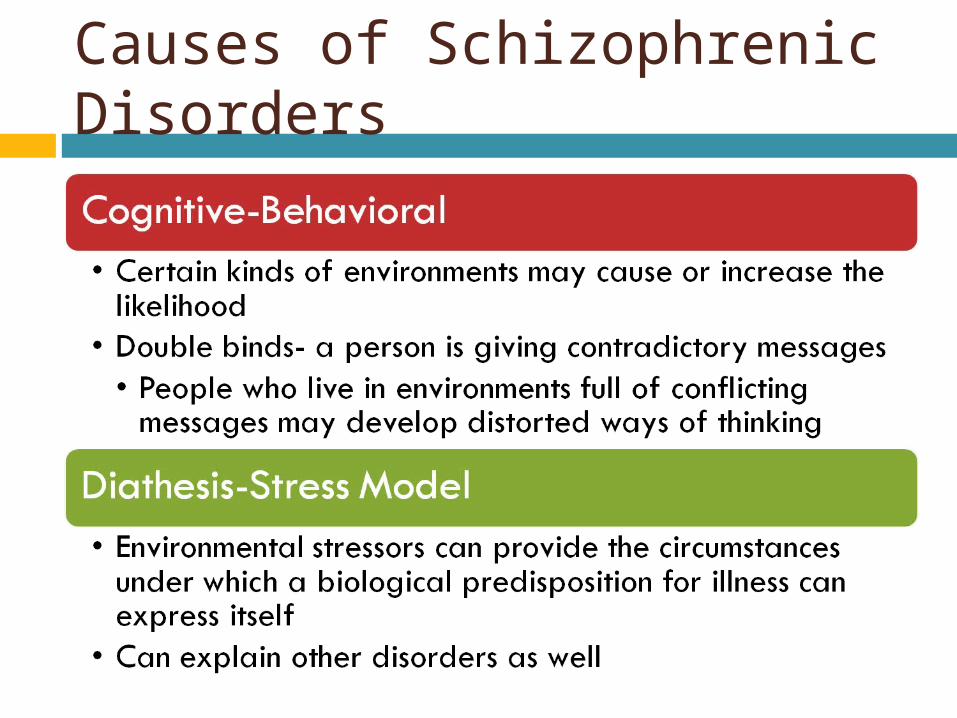
Causes of Schizophrenic Disorders

Personality Disorders
Generally less serious Well-established, maladaptive ways, of
behaving Antisocial Personality Disorder- have
little regard for other people’s feelings (often criminals)
Dependent Personality D/o- depend too much on others
Histrionic Personality Disorder- overly dramatic

Other Psychological Disorders Paraphilias/Psychosexual Disorders-
sexual attraction to an object, person, or activity not usually seen as sexual
Eating Disorders- Anorexia and Bulimia
Substance Abuse Disorder Autism- atypical social development ADHD

The Rosenhan Study (1978)
David Rosenhan and his associates sought admission to mental hospitals, claiming that they had been hearing voices; all were admitted as suffering from schizophrenia At that time, they ceased reporting any
unusual symptoms and behaved as usual None were exposed, all leftwith the diagnosis
of schizophrenia in remission Should people who were once diagnosed
carry it the rest of their lives? To what extent are disorders the product of
the environment? What is the level of institutional care
available of the imposters could go undetected for weeks?

Types of Therapy- Generally Effective
Psychoanalytic Therapy
Cause of disorders in unconscious conflicts; must identify the underlying cause
Symptom substitution- happens in other types of therapy when the underlying problem is not addressed; person will have a new psychological problem
Hypnosis- an altered state of consciousness where people are less likely to repress troubling thoughts

Psychoanalytic Theory
Free Association- saying whatever comes to mind, we cannot constantly sensor everything we say
Dream Analysis- the ego’s defenses are relaxed during sleep Manifest content- what a patient reports
about their dream Latent content- the hidden
content revealed by interpretive work

Psychoanalytic Theory
Resistance- disagreeing with their therapist’s interpretations Strongly voiced- close to getting at the
actual problem Transference- having strong feelings
toward their therapist Love, hate, etc.
Psychodynamic- after Freud (Adler, Horney etc.)

Humanistic Theory
Focuses on helping people understand and accept themselves and strive to self-actualize
People are innately good and possess free will- capable of controlling their own destinies (opposite of determinism)
Carl Rogers (Client Centered Therapy) The therapist provides the patient with
unconditional positive regard (support no matter what)
Essential to healthy development

Humanistic Therapy
Non-directive- do not tell client what to do, but seek to help clients choose the best course of action for themselves Active listening- clarify feelings for client-
(“So what I’m hearing you say is…”) Gestalt Therapy (Perls)- encourage client
to get in touch with their whole selves Body position, minute actions Stress importance of the present

Behavioral Therapy
Counterconditioning- a kind of classical conditioning in which an unpleasant conditioned response is replaced with a pleasant one Give Bentley a treat when he is put in his cage
Systematic Desensitization- teaching the client to replace the feelings of anxiety with relaxation Teach the client to relax Create an anxiety hierarchy- rank ordered list of
what the client fears and tackle each one

Behavioral Therapy
Flooding- address the most frightening scenario first to realize fears are irrational
Modeling- learning by observing the behavior of others
Aversive conditioning- pairing a habit one wishes to break with an unpleasant stimulus
Token Economy- identify desired behaviors and reward them for tokens that can be exchanged
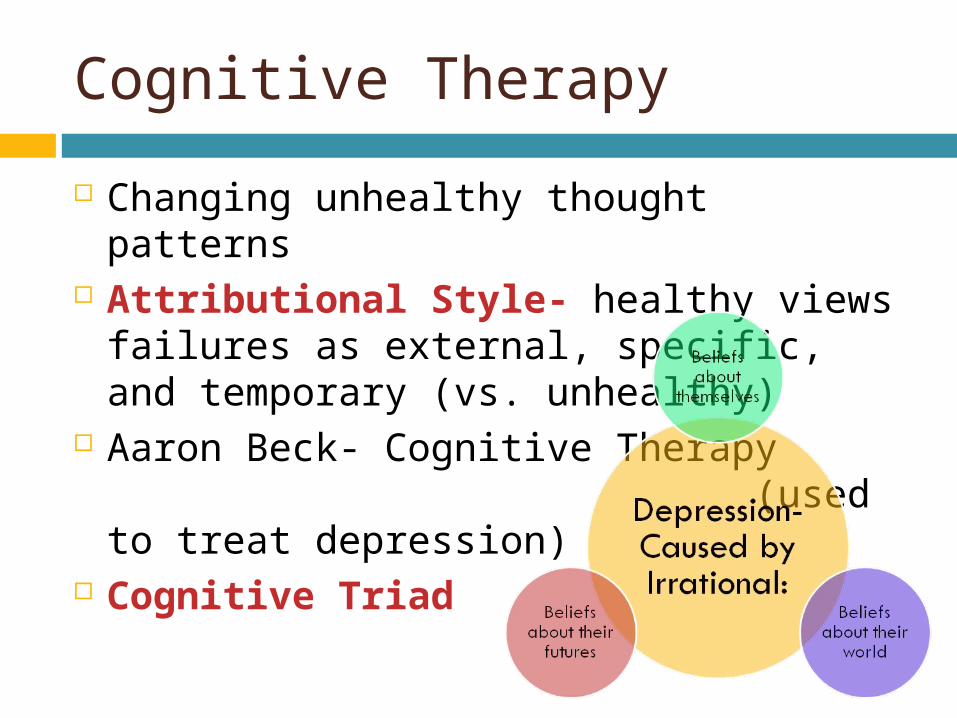
Cognitive Therapy
Changing unhealthy thought patterns Attributional Style- healthy views
failures as external, specific, and temporary (vs. unhealthy)
Aaron Beck- Cognitive Therapy (used to treat depression)
Cognitive Triad

Cognitive Behavioral Therapies (CBT) Rational Emotive (REBT)- Albert Ellis
Expose and confront the dysfunctional thoughts of their clients
Question the likelihood of an event occurring and the impact that would result
Goal is to show the client that failure is an unlikely occurrence but that even if it did occur, its not that big of a deal

Somatic Therapy
Pharmacology/Chemotherapy- Drug Treatment
Type of Disorder
Treatment Type of Drug Drug Names
Anxiety Disorders
Depress CNS activity
Barbiturates, Benzodiazepines
Miltown, Zanax, Valium
Unipolar Depression
Increase Serotonin
MAOIs, Tricyclic Antidepressants, serotonin-reuptake inhibitors
Zoloft, Prozac
Bipolar Depression
Lower manic phase
Lithium
Schizophrenia Block dopamine receptor sites
Antipsychotics, Neuroleptics
Haldol

Somatic Therapy
Electroconvulsive Therapy (ECT) Passing electric current through the brain,
causing a brief seizure Can result in memory loss Used as a last resort for severe depression Not completely understood
Psychosurgery Prefrontal lobotomies- calmed patients to a
vegetative state

Practice Questions
1) All schizophrenics suffer from Depression Multiple personalities Flat affect Distorted thinking Delusions of persecution

2) Juan hears voices that tell him to kill people. Juan is experiencing Delusions Obsessions Anxiety Hallucinations Compulsions

3) Depression is associated with low levels of Acetylcholine Epinephrine Serotonin Dopamine GABA

4) What kind of psychologist would be most likely to describe depression as the result of an unconscious process in which anger is turned inward? Biomedical Psychoanalytic Cognitive Behavioral Sociocultural
5) Coretta’s therapist says little during their sessions and never makes any recommendations about what Coretta ought to do. What kind of therapy does Coretta’s therapist most likely practice? Psychdynamic Behavioral Cognitive Biomedical Humanistic

6) Maria has been in analysis for over a year. Recently, she has begun to suspect that she has fallen in love with Dr. Chin, her analyst. When she confesses her feelings, Dr. Chin is likely to tell Maria that she is experiencing Resistance Transference A breakthrough Irrational expectations Unconditional positive regard


















