Dislocation Lusi

of 46
-
Upload
samira-mira -
Category
Documents
-
view
248 -
download
0
Transcript of Dislocation Lusi
-
7/27/2019 Dislocation Lusi
1/46
DISLOCATION
Lecturer :
dr. Erwien Isparnadi, Sp.OT
Author :
Lusiana Ayu Lestari
201210401011027
27/07/2013 1
-
7/27/2019 Dislocation Lusi
2/46
Definition
JOINT
Is a relationship between two or more bones are
connected through the connective tissue wrapping onthe outside and on the inside there is a joint cavitywith the bone surface covered by cartilage.
Dislocation A condition in which the bones that form the joint is
no longer connected anatomically (off the bone ofjoints).
27/07/2013 2
-
7/27/2019 Dislocation Lusi
3/46
27/07/2013 3
-
7/27/2019 Dislocation Lusi
4/46
clasification
Congenital
Patoligik Traumatik
Paralitic
27/07/2013 4
-
7/27/2019 Dislocation Lusi
5/46
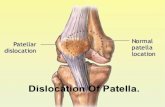
Clinical manifestasion
acute
chronic
recurent
27/07/2013 5
-
7/27/2019 Dislocation Lusi
6/46
Etiology
Falls
patologist
Trauma
notrelated to
sports
Sportinjury
27/07/2013 6
-
7/27/2019 Dislocation Lusi
7/46
ANATOMI
27/07/2013 7
-
7/27/2019 Dislocation Lusi
8/46
-
7/27/2019 Dislocation Lusi
9/46
Repositioning immediately
Dislocation reduction: restored to its originalplace, it is necessary to use anesthesia ifsevere dislocation.
Head of bone dislocation manipulated andreturned into the joint cavity
Imobillized casts, splints, traction Several days to weeks after the reduction
carried out mobilization smooth 3-4x a day.
Management
27/07/2013 9
-
7/27/2019 Dislocation Lusi
10/46
ANATOMI
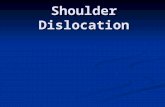
Shoulder dislocation
Sternoklavikularjoin
Akromioklavikularjoin
Humeroskalpulerjoin
27/07/2013 10
-
7/27/2019 Dislocation Lusi
11/46
Adult >>
Arms are usually forced to abduction,
external rotation, and extensionHumerus is
pushed forward, tearing the capsule or
causing avulsi the edge of the glenoid
Bankart lesion
Anterior shoulder dislocation
27/07/2013 11
-
7/27/2019 Dislocation Lusi
12/46
Arm injuries sustained by other hand
Deformity
Position tilted to the position of the sick
Painful
Palpable bumps on clavicle
Unable to move his arm
On palpation palpable under the acromion isempty
Clinical manifestasion
27/07/2013 12
-
7/27/2019 Dislocation Lusi
13/46
27/07/2013 13
-
7/27/2019 Dislocation Lusi
14/46
27/07/2013 14
-
7/27/2019 Dislocation Lusi
15/46
Overlap between the humeral head and
glenoid fossa, caput usually in below and
medial to the joint bowl
X- RAY
27/07/2013 15
-
7/27/2019 Dislocation Lusi
16/46
repositioning immediately
With the indication:
no fracture
absence of neurological deficits1. axilarry sensory nerves in m.deltoideus
2. n.radialis hand extension
3. a.brachialisradial pulse
Treatment
27/07/2013 16
-
7/27/2019 Dislocation Lusi
17/46
27/07/2013 17
-
7/27/2019 Dislocation Lusi
18/46
Close reduction
STIMPSON
This method is simple and
does not require
anesthesia.
Patients in prone position
and sleep on the table,hanging downward. Arm
were given a weight 5-7 kg.
At the time of the shoulder
muscles in a state ofrelaxation, is expected to
occur due to therepositioning of heavy arms
that hung beside the bed.
Applied 15 to 20 minutes
27/07/2013 18
-
7/27/2019 Dislocation Lusi
19/46
When Stimson failed
patient supine
grasps the affected side at thehand and forearm and abduksi
foot pressed into axiila(tilting the humeral head to
the lateral and posterior)
Shoulder position maintainedendorotasi by a buffer chest
min 3 weeks
HIPPOCRATES
27/07/2013 19
-
7/27/2019 Dislocation Lusi
20/46
-
7/27/2019 Dislocation Lusi
21/46
27/07/2013 21
-
7/27/2019 Dislocation Lusi
22/46
After reposition shoulder joints were fixed with chest, with verband and
forearm suspended by slings. 3-6 weeks of immobilization enough.27/07/2013 22
-
7/27/2019 Dislocation Lusi
23/46
-
7/27/2019 Dislocation Lusi
24/46
operation
bristow-helfet
Brankartprosedur
putti-plat
27/07/2013 24
-
7/27/2019 Dislocation Lusi
25/46
-
7/27/2019 Dislocation Lusi
26/46
Rarely Indirect force that causes internal rotation and
strong adduction.
Clinical features The arm was swollen and deformity locked in
position adduction and internal rotation,
protrusion of the posterior humeral head, the
blank subakromion Limited adduction can not be rotated to
external
Posterior shoulder dislocation
27/07/2013 26
-
7/27/2019 Dislocation Lusi
27/46
27/07/2013 27
-
7/27/2019 Dislocation Lusi
28/46
caput humeris looks abnormal (such as light
bulbs), away from the glenoid fossa (glenoid
sign blank)
Radiological examination
27/07/2013 28
-
7/27/2019 Dislocation Lusi
29/46
-
7/27/2019 Dislocation Lusi
30/46
The humeral head trapped under the cavities
glenoidale locked in position abduction.
Treatmen like anterior dislocation
Inferior shoulder dislocation
27/07/2013 30
-
7/27/2019 Dislocation Lusi
31/46
Adult >>
Common in traumatic35 years
Congenital dislocation of about 2-4 casesper 1000 live births, 80-85% in women
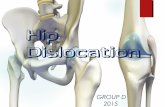
HIP DISLOCATION
DefinitionA situation where the femur head out
of the acetabulum
27/07/2013 31
-
7/27/2019 Dislocation Lusi
32/46
Posterior hip dislocation
27/07/2013 32
-
7/27/2019 Dislocation Lusi
33/46
27/07/2013 33
-
7/27/2019 Dislocation Lusi
34/46
-
7/27/2019 Dislocation Lusi
35/46
supine
Assistant pressing the crista
iliaca to the table
Operators do traction of the
femur one way direction of
the axis
endorotasi
eksorotasi
Ekstensi hip join
treatment
THE BIGELOW MANEUVER
27/07/2013 35
-
7/27/2019 Dislocation Lusi
36/46
supine
Fixation crista iliaca to the
operating table
Traction direction axis of the
femur + endorotasi femur
Immobilized with skin
traction with minimal
flexion of the hip joint
Endorotasi for 2-3 weeks
Non-weight bearing
mobilization2-3 weeks
METODE ALLIS
27/07/2013 36
-
7/27/2019 Dislocation Lusi
37/46
-
7/27/2019 Dislocation Lusi
38/46
-
7/27/2019 Dislocation Lusi
39/46
Early lesions n. Ischiadicus
Lately nekrosis avaskuler
artrosis degeneratif
COMPLICATION
27/07/2013 39
-
7/27/2019 Dislocation Lusi
40/46
fell from a high place and rub the head femur in front of the
acetabulum
Anterior HIP DISLOCATION
27/07/2013 40
-
7/27/2019 Dislocation Lusi
41/46
Leg is be laid Eksorotasi, in a abductionposition
patient can not move Flexion actively when
in a state of dislocation. Kaput femur in
front of the femoral triangle.
sinar x
clinical manifestation
27/07/2013 41
-
7/27/2019 Dislocation Lusi
42/46
Pattien supine
Fixation crista iliaca to
the operating table
Traction in the direction
of the axis of the femur
Endorotasi and adduksi
femur
management
REVERSE BIGELOW
27/07/2013 42
-
7/27/2019 Dislocation Lusi
43/46
27/07/2013 43
-
7/27/2019 Dislocation Lusi
44/46
excessive abduction of the pelvis trochanter
major moves agains pelvis to tilting kaput
femur out of the acetabulum.
clinical symptoms and examination
abduction and can not in normal position
trochanter and pelvic region pain
Can do a limp movements
Central hip dislocation
27/07/2013 44
-
7/27/2019 Dislocation Lusi
45/46
Treatment
Changing thesedislocations into
anterior / posteriorhip dislocation
reduced with true
appropriate
27/07/2013 45
-
7/27/2019 Dislocation Lusi
46/46