Diseases of the Penis Congenital Anomalies EPISPADIAS: Dorsal surface opening HYPOSPADIAS: Ventral...
46
Diseases of the Penis Congenital Anomalies EPISPADIAS: Dorsal surface opening HYPOSPADIAS: Ventral surface opening MISCELLANEOUS PHIMOSIS: Small prepuce orifice secondary to repeated infections INFLAMMATIONS: Balanoposthitis, infection of glans and prepuce with smegma.
-
Upload
megan-alexander -
Category
Documents
-
view
217 -
download
2
Transcript of Diseases of the Penis Congenital Anomalies EPISPADIAS: Dorsal surface opening HYPOSPADIAS: Ventral...

Diseases of the Penis Congenital Anomalies
EPISPADIAS: Dorsal surface opening
HYPOSPADIAS: Ventral surface opening
MISCELLANEOUSPHIMOSIS: Small prepuce orifice secondary to repeated infections
INFLAMMATIONS: Balanoposthitis, infection of glans and prepuce with smegma.
Organisms: candida, anaerobes, pyogenic

Tumors of the Penis
BENIGN:1. CONDYLOMA ACCUMINATUM: Human papilloma virus (HPV)
Sexual transmission
HPV types 6 - 11 associated with carcinoma
CARCINOMA IN SITU: 3 types
A. BOWEN DISEASE: Limited by basement membrane; mainly in shaft
B. ERYTHROPLASIA OF QUEYRAT: Similar to Bowen’s but in glans-prepuce
C. BOWENOID PAPULOSIS: Sexually active; pigmented lesions

Tumors of the Penis Malignant
SQUAMOUS CELL CARCINOMAHPV INFECTION: type 16 most common, also 18
40 - 70 years of age
More common in uncircumcised populations
Glans - inner surfer of prepuce
Papillary or flat
VERRUCOUS CARCINOMA: Giant condyloma (BUSCHKE-LOWENSTEIN TUMOR)
Also HPV related types 6, 11
Invasive carcinoma metastasizes to inguinal-iliac LN
66% 5-year survival, if LN involved 27% 5-year survival

SQUAMOUS CELL CARCINOMA

Testis Epididymis Congenital anomalies
CRYPTORCHIDISM: Undescended testis
Descent in 2 phases: a. Transabdominal, to lower abdomen b. Inguino-scrotal, to scrotum (MOST COMMON DEFECT)
Asymptomatic - bilateral 25%
Testicular atrophy; prominent Leydigcells
Complications: Sterility - cancer

CRYPTORCHID

Diseases of Testis Inflammation
TB, GONORRHEA: Epididymis, spreads to testis
SYPHILIS: Testis involved first
CHLAMYDIA: Epididymitis in sexually active
E. COLI PSEUDOMONAS: Epididymitis in older than 35; may cause abscess, sterility
MUMPS: Orchitis
VASCULAR DISTURBANCES: Torsion due to trauma, incomplete descent, may cause hemorrhage-infarction

GONORRHEA

Testicular Tumors
A. GERM CELL TUMORS
B. NONGERMINAL CELL TUMORS (STROMA - SEX CORD)

Germ Cell Tumors
A. SEMINOMA: Typical, anaplastic, spermatocytic
B. EMBRYONAL CARCINOMA
C. YOLK SAC TUMOR
D. POLYEMBRYOMA
E. CHORIOCARCINOMA
F. TERATOMA: Mature, immature, malignant
G. MIXED: Teratocarcinoma (EMBRYONAL, CHORIOCARCINOMA)

Testicular Tumors
A. SEMINOMAS
Morphology1. TYPICAL: Grossly white-gray homogeneous. Microscopic: large, polyhedral cells with large central nucleus, nucleoli, by IP positive for Placenta like alkaline phosphatase (PLAP) ; lymphocytic reaction, granulomas
2. ANAPLASTIC: Large, irregular cells, frequent mitoses
3. SPERMATOCYTIC: Medium and large cells, giant cells

SEMINOMA

Testicular Tumors
B. EMBRYONAL CARCINOMA: Hemorrhage - necrosis. Cells are large, hyperchromatic nuclei, nucleoli, arranged in glandular, alveolar or tubular patterns, with papillary convolutions. 20 - 30 years
C. YOLK SAC TUMORS (INFANTILE EMBRYONAL OR
ENDODERMAL SINUS TUMOR): Children up to 3 years
Cuboidal or elongated cells, with papillary formation
Endodermal sinus (50%): resemble primitive glomeruli, mesodermal core, central capillary lined by visceral and parietal layers
Eosinophilic globules with alpha-fetoprotein

EMBRYONAL CARCINOMA
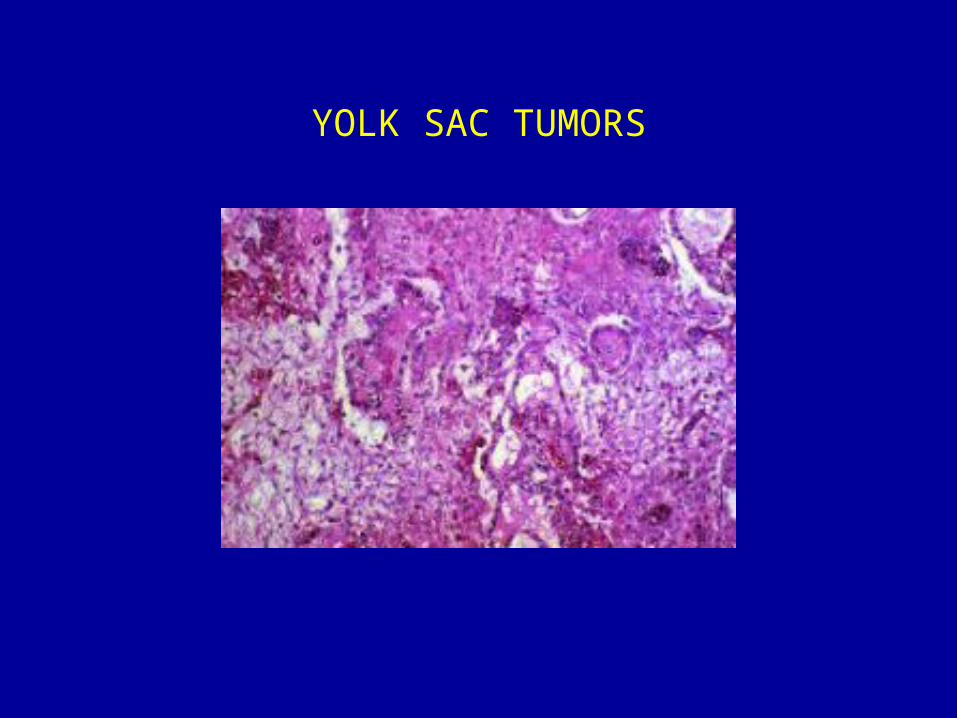
YOLK SAC TUMORS

Testicular Tumors
D. CHORIOCARCINOMA Aggressive, small tumors, metastasize widely
Hemorrhage - necrosis common
Syncytiotrophoblastic - Cytotrophoblastic components; positive for HCG

CHORIOCARCINOMA

Testicular TumorsE. TERATOMAS Common in child, rare in adults Gross: large (SOLID, CARTILAGINOUS, CYSTIC)
Three histologic variants
1. MATURE: nerve, muscle, cartilage, thyroid, bronchial, intestinal, brain in myxoid or fibrous stroma.
All well differentiated.
2. IMMATURE: poorly differentiated tissues, but identifiable.
Glands, neuroblasts, cartilage
3. MALIGNANT TRANSFORMATION: squamous or adenocarcinoma, sarcoma

Testicular Tumors
Mixed
60% e.g. teratomas - embryonal
teratoma - yolk sac
seminoma - embryonal or teratoma

TeratocarcinomaMixed: Embryonal and Choriocarcinoma
HCG

Testicular Tumors Clinical Features
CLINICALLY: Classified as seminomatous or nonseminomatous
Painless masses
LYMPHATIC SPREAD TO LYMPH NODES: Retroperitoneal, paraaortic, mediastinal, supraclavicular
HEMATOGENOUS SPREAD: Lung, liver, bones, brain
Testicular Tumors Staging
STAGE 1: Confined to testis, epididymis, spermatic cord
STAGE II:Retroperitoneal lymph nodes, below the diaphragm
STAGE III: Metastases into lymph nodes above thediaphragm
STAGE IV: Metastases into other organs: or lung, liver, brain, bones

Testicular Tumors Biologic Markers
1. HUMAN CHORIONIC GONADOTROPHINS (HCG) choriocarcinomas
2. ALPHAFETOPROTEIN (AFP) yolk sac tumors
3. PLACENTA-LIKE ALKALINE PHOSPHATASE (PLAP) seminomas
Others include placental lactogen, LDH
Helpful in diagnosis, staging, monitoringtesticular tumors
Testicular Tumors Sex Cord – Gonadal Stromal Tumors
SEX CORD (SERTOLI)
Estrogen or androgen producers
Gynecomastia, precocious masculinization
MORPHOLOGY: gray, white or yellow nodules
Entirely Sertoli type or partly granulosa cells
Cordlike structures, resembling seminiferoustubules
Benign tumors; 10% malignant

SERTOLI TUMOR

Gonadal Stromal Tumors Leydig Cell Tumors
May produce androgens, estrogens, corticosteroids
Gynecomastia – sexual precocity in children
Golden brown, homogeneous nodules
Cells are large, round or polygonal
Eosinophilic cytoplasm, central, round nucleus
Reinke crystalloids in 25% of tumors
Benign; 10% invasive

Leydig Cell Tumor
Tunica Vaginalis
Hydrocele (FLUID ACCUMULATION)
Hematocele (TRAUMA)
Chylocele (ELEPHANTIASIS)
Spermatocele
Varicocele

Prostate
EMBRYO: 5 lobes Posterior, middle, anterior, 2 laterals
ADULT: 4 lobes
Peripheral, central, transitional, periurethral
GLANDS: 2 cell layers: basal, columnar

ProstateInflammation
ACUTE BACTERIAL: Gram negative rods, staphylococci
CHRONIC BACTERIAL: Same organisms
CHRONIC ABACTERIAL: Most common type
Sexual activity (CHLAMYDIA, MYCOPLASMA)
MORPHOLOGY: Necrosis, later fibrosis, chronic with lymphocytes, neutrophils,lymphs, macrophages

Prostate
InflammationACUTE

ProstateHYPERPLASIA:Glandular - stromal
INCIDENCE:20% over age 40, 70% by age 60, 90% by age 70
ENLARGEMENT:Androgens stimulate growth (DHT)
DHT synthesized in prostatic stromal cells
DHT inhibitors cause decrease in volume
MORPHOLOGY:Cellular nodules in transitional zone; later stromal periurethral nodules; compress urethra and prostate, creating cleavage (NOT CAPSULE). Nodules with squamous metaplasia or infarction.

HYPERPLASIA:
Glandular - stromal

Carcinoma of Prostate
Most common tumor in males
300,000 new cases / year – 69/100,000
20% 50 – 60 years
70% 70 – 80 years
Highest rates in blacks

Carcinoma of Prostate

Carcinoma of Prostate
ETIOLOGY: Unknown
RISK FACTORS: Age – environmental
Role of androgens
Genetics
Molecular
Carcinoma of Prostate
70% arise in peripheral zone, posterior aspect
Detectable by rectal examination
May invade seminal vesicles, base of bladder
HEMATOGENOUS METASTASES TO BONES:Lumbar spine, femur, pelvis, ribs (OSTEOBLASTIC)
LYMPHATIC SPREAD TO LYMPH NODES:Obturator, perivesical, hypogastric, iliac, paraaortic

Carcinoma of Prostate Morphology
MICROSCOPIC: Well-defined small glands
Uniform layer cuboidal or low columnar cells
Occasionally larger with papillary or cribriform pattern
Nuclei large, vacuolated, 1 – 2 nucleoli
Mitoses uncommon
GROWTH PATTERN: Rounded masses, back to back pattern
UNDIFFERENTIATED: Cords, nests, sheets
Tendency to invade capsule, lymphatic – vascular channel and nerves
PREMALIGNANT LESION: PIN (PROSTATIC INTRAEPITHELIAL NEOPLASIA)
DIFFERENCE: Presence of basal layer

Carcinoma of ProstateClinical Features
70% incidence in men over 80 years, Stage A
VISUAL COURSE:Non-progressive
Stage A2 progresses (30 – 50%)
Over 60% present with local disease
Urinary symptoms are late
DIAGNOSTIC APPROACH:Rectal exam, serum PSA, biopsy
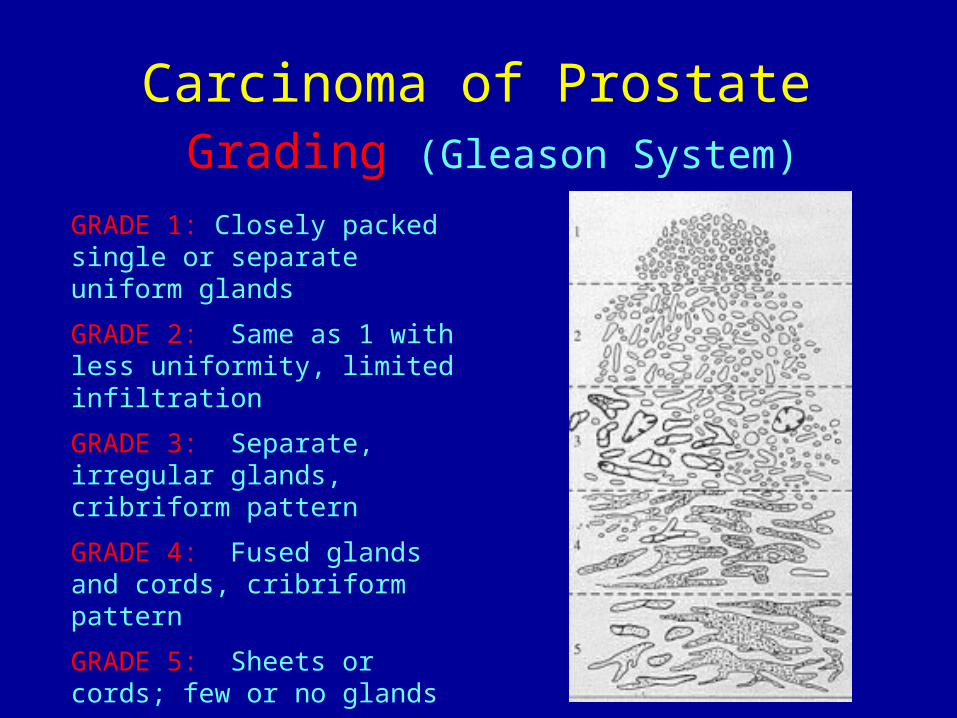
Carcinoma of Prostate Grading (Gleason System)
GRADE 1: Closely packed single or separate uniform glands
GRADE 2: Same as 1 with less uniformity, limited infiltration
GRADE 3: Separate, irregular glands, cribriform pattern
GRADE 4: Fused glands and cords, cribriform pattern
GRADE 5: Sheets or cords; few or no glands

GRADE 1: Closely packed single or separate uniform glands

GRADE 3: Separate, irregular glands, cribriform pattern
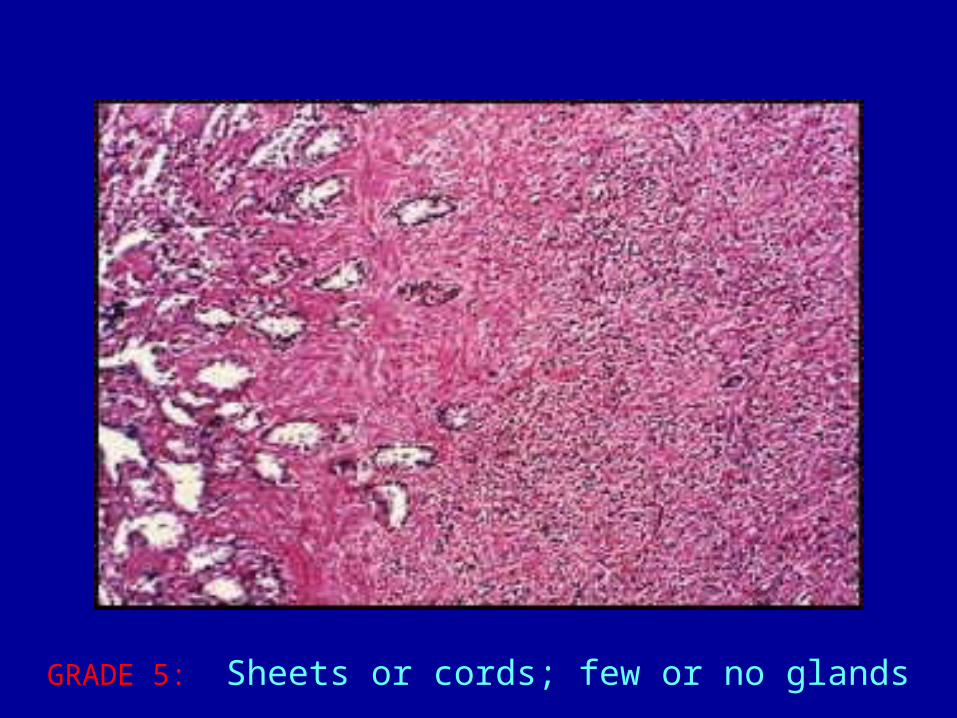
GRADE 5: Sheets or cords; few or no glands
Carcinoma of ProstateProstate Specific Antigen (PSA)
Serine protease produced by prostatic epithelium
SERUM LEVEL: 4 ng/ml upper limit
“Organ specific”, not “cancer specific”
Elevated in BPH, prostatitis cancer
BPH: 30% have elevated PSA
CARCINOMA: 80% have elevated PSA, 20 – 40% have less than 4 ng/ml

Prostatic Specific Antigen (PSA)
TWO FORMS:a) Free
b) Bound to alpha 1 antichymotrypsin
Free PSA is lower in cancer than in BPH
Specially important in values 4 – 10 ng/ml

Carcinoma of ProstateTreatment
SURGERY:Localized disease (Stages A – B)
RADIATION:Localized disease (Stages A – B)
HORMONAL TREATMENT:Metastatic disease (Stages C – D)(ESTROGEN THERAPY – ORCHIECTOMY)