Diseases of the Cornea. Keratitis Infectious – Bacterial (Streptococcus pneumoniae) – Bacterial...
34
Diseases of the Cornea
-
Upload
christian-mcdonald -
Category
Documents
-
view
233 -
download
2
Transcript of Diseases of the Cornea. Keratitis Infectious – Bacterial (Streptococcus pneumoniae) – Bacterial...
Diseases of the Cornea
Keratitis
• Infectious– Bacterial (Streptococcus pneumoniae)– Bacterial (Pseudomonas aeruginosa)– Fungal– Herpes simplex
• Physical – Abrasion
Bacterial (Streptococcus pneumoniae)
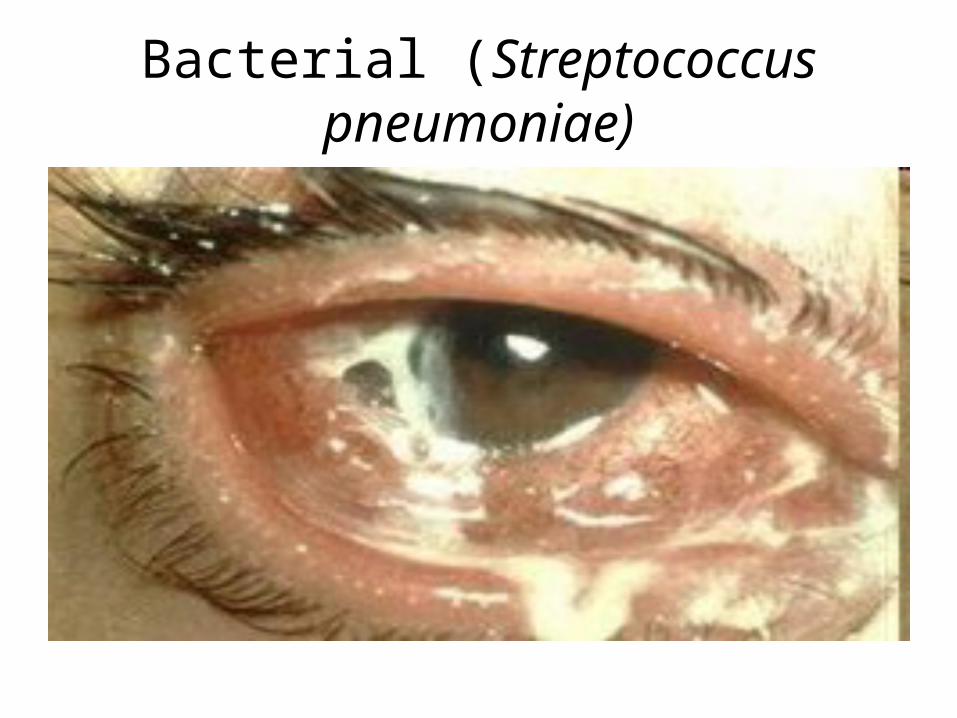
• Streptococcus pneumoniae: lancet-shaped, encapsulated, gram + diplococci
• Serpingous, gray-white stromal infiltrate and hypopyon (pus)
• Distinct borders with overhanging edges; usually with overhanging defect or ulcer
• Suppuration not usually extend over the entire corneal surface
• Sterile hypopyon is common
Bacterial (Streptococcus pneumoniae)
Bacterial (Streptococcus pneumoniae)
• History of the patient: trauma or URTI for 5-7 days• Pneumococcal ulcer manifests 24-48 hrs after
inoculation of the abraded cornea• Spread erratically from original site towards the
center • Advancing border shows active ulceration as the
trailing border begins to heal acute serpingous ulcer
• Superficial corneal layers involved first then the deep parenchyma
Bacterial (Streptococcus pneumoniae)
• Topical erythromycin• Chloramphenicol • 4th gen fluroquinolones (Moxifloxacin and
Gatifloxacin)• Oral cephalosporins and erythromycin• Concurrent dacrocystitis and nasolacrimal
duct obstruction should be treated

Bacterial (Pseudomonas aeruginosa)
• Gram (-) corneal ulcer • Rapid evolution; marked tendency to spread• Common among immunocompromised, soft
contact lens with faulty hygiene, contaminated fluorescein solution or eye drops

Bacterial (Pseudomonas aeruginosa)

Bacterial (Pseudomonas aeruginosa)
• Begins as a gray or yellow mucopurulent discharge adherent to ulcer surface bluish green
• Ulcer is diffused with uniform penetration severe pain
• More discharge• Opacification and edema around the ulcer • Rapid stromal necrosis due to proteolytic enzymes • Corneal perforation and severe intraocular
infection
Bacterial (Pseudomonas aeruginosa)
• Moxifloxacin, Gatifloxacin, Ciprofloxacin, Tobramycin, Gentamycin
• Other fluoroquinolones, polymyxin B or carbenicillin
Fungal Keratitis
• Indolent or slow-type (usually months)• Filamentous– Gray white– Feathery border – Satellite infiltrates– Deep: endothelial plaque
• Yeast – Focal– Dense suppuration similar to Pneumococcus
Fungal Keratitis
• Intense suppuration, progressive hypopyon• Anterior chamber membranes• Gray infiltrate with irregular edges• Marked inflammation of the globe with
superficial ulceration • Endothelial plaque with corneal abscess

Fungal Keratitis
Fungal Keratitis
• Candida, Fusarium, Aspergillus, Penicillium, Cephalosporium
• Except Candida: Hyphal elements• Candida: pseudohyphae or budding

Fungal Keratitis
• No effective topical agent • Combination of anti-fungal tablets (Amikacin,
Cefaxolin, Gentamicin, Neomycin, etc)• Oral tablets (Amphotericin B with saline)
dropped every 5 mins• Debridement to remove dead tissue and to
increase drug absoprtion • Candida: Natamycin, Ketoconazole,
Voriconazole, Amphotericin B

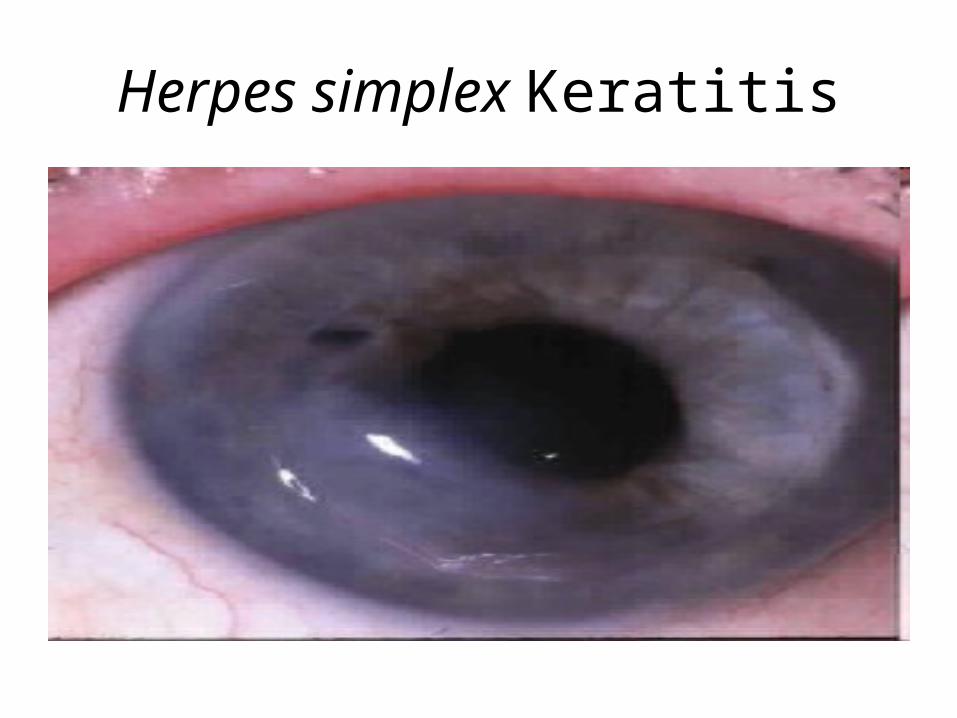
Herpes simplex Keratitis
• Discrete punctate epithelial keratitis coalesce into branching or dendritic lesion (swollen, opaque epithelial cells)
• Terminal bulbs• Ulcer in the center of dendrite due to lysis and
desanquamation of infected cells• Centrifugal spread (center to peripheral)
geographic ulcer
Herpes simplex Keratitis
Herpes simplex Keratitis
• Usually among young children • Mild stromal edema and subepitelial infiltrates• Irritation, photophobia, tearing • If central cornea affected reduction in vision • Can have fever, blisters
Herpes simplex Keratitis
• Debridement • Idoxuridine, Trifluridine, Vidarabine, Acyclovir• Penetrating keratoplasty: only for inactive
infections • Control reactivation of HSV infection – Aspirin for fever – Avoid exposure to ultraviolet light – Prophylactic antivirals

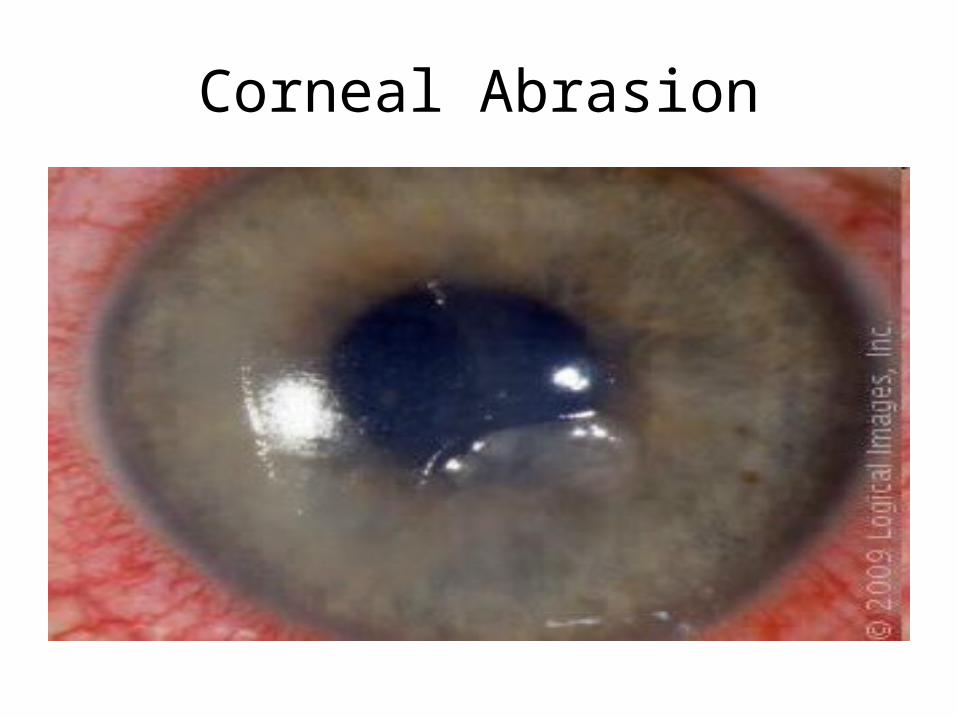
Corneal Abrasion
• Scraping of the superficial part that may heal in a matter of hours
• Acute pain after trauma• Photophobia, tearing, blepharospasm (eyelid
spasm), foreign body sensation, blurred vision• Adjacent cells expand and fill the defect basal
epithelial cells undergoes mitosis • Patching/bandage, topical antibiotics,
cycloplegic
Corneal Abrasion
Glaucoma
Glaucoma (Acute angle closure)
• True emergency!!• Route of aqueous humor: cilliary body drains
anteriorly from iris pupil canal of Schlemm• Occlusion at the anterior chamber angle by
the peripheral iris increase IOP• Pupillary block: from posterior to anterior
chamber peripheral iris balloon forward• Plateau iris: peripheral iris lax contact with
the angle
Glaucoma (Acute angle closure)
• Ocular pain, headache• Unilateral blurring of vision • Iridescent vision (halos)• Nausea and vomiting• Redness
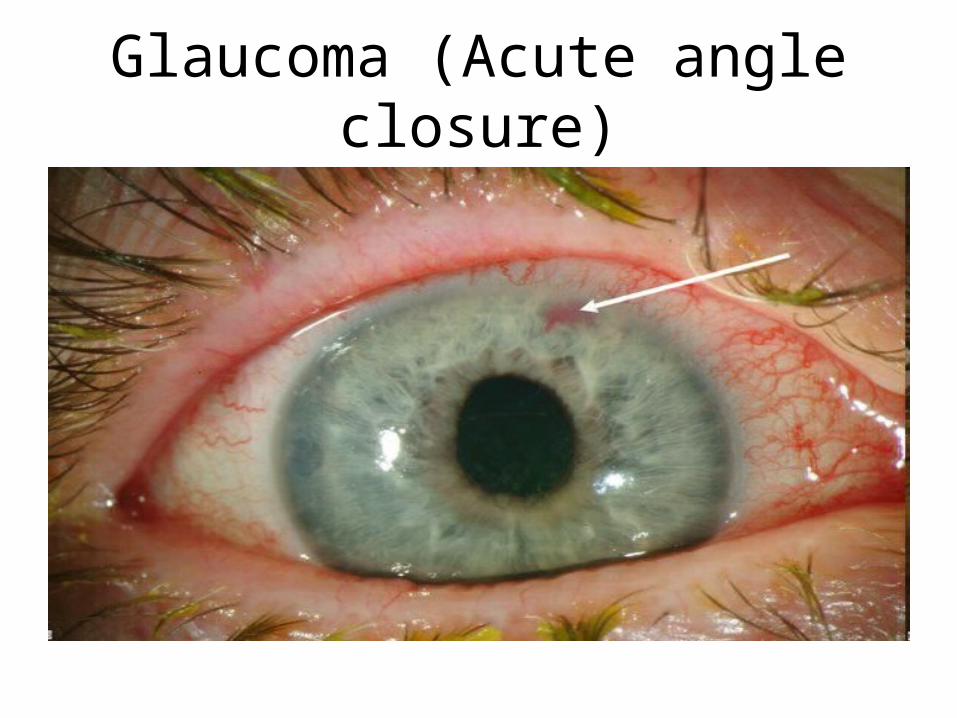
Glaucoma (Acute angle closure)
• Elevated IOP (60-80 mmHg) on tonometry “rock hard”
• Deep circumlimbal conjunctiva and episcleral injection ciliary flush
• Fixed, mid-dilated pupil• Edematous or steamy cornea• Shallow anterior chamber • Thinning out or excavation of optic disc
“glaucomatous cupping” chronic cases
Glaucoma (Acute angle closure)
Glaucoma (Acute angle closure)
• Increased IOP acute ischemic changes in iris corneal edema optic nerve damage
• Primary open-angle glaucoma– IOP doesn’t increase >30 mmHg– Retinal damage develops over a period of time
• Normal-tension glaucoma– Retinal ganglion cells susceptible to changes in IOP– Optic nerve ischemia
Glaucoma (Acute angle closure)
• Carbonic anhydrase inhibitors• Hyperosmotic agents – Oral glycerin – IV mannitol
• Pilocarpine• Supportive: corticostroids, analgesics
Uveitis
Uveitis (Iridocyclitis)
• Anterior chamber • Inflammation of the iris, ciliary body, choroid• Deep, dull pain• Photophobia may be severe– Ciliary body controls the opening and closing of
the iris muscles • Tearing
Uveitis (Iridocyclitis)
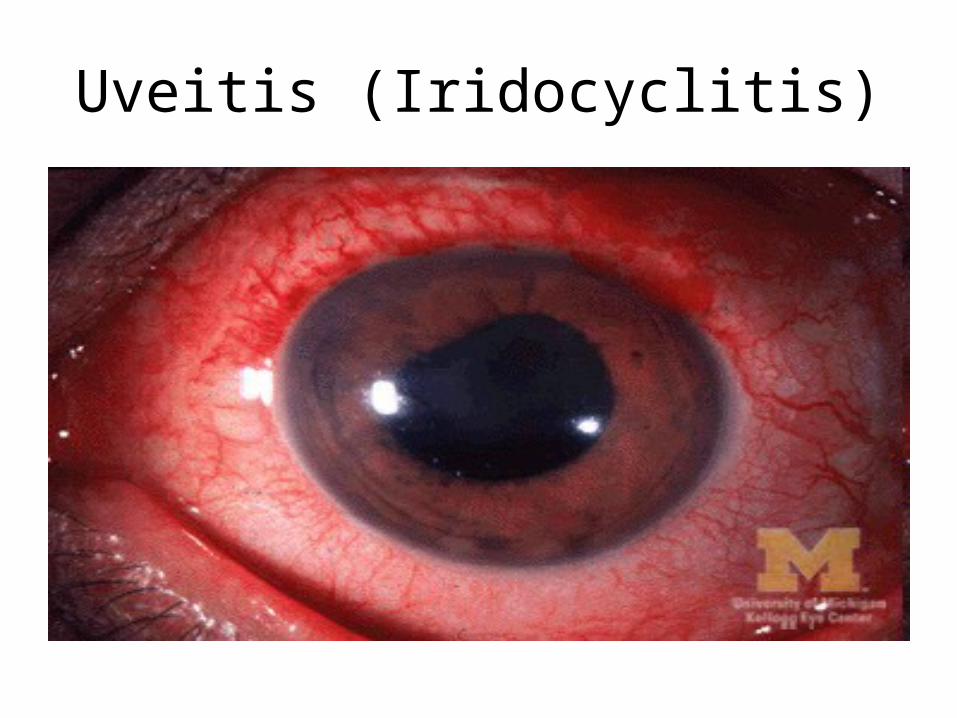
• Visual acuity not significantly impaired• Reading difficulty• Ciliary flush • Mildly edematous cornea• Sterile hypopyon if severe
Uveitis (Iridocyclitis)
• Hallmark: cells and flare• Cells– Leukocytes floating in aqueous
• Flare – Protein from inflamed iris or ciliary body
• Keratic precipitates (clumps of white cells and inflamatory debris) in active inflammation
• Koeppe nodules (granulomatous nodules in iris)• Busacca nodules (within iris stroma)• Berlin’s nodules (anterior chamber angle)
Uveitis (Iridocyclitis)

Uveitis (Iridocyclitis)
• Underlying systemic disease– TB, Ankylosing spondylitis, Behcet’s syndrome,
JRA, syphilis• Treatment – Immobilize iris and ciliary body to decrease pain – Cycloplegia (atropine, cyclopentolate)– Topical steroids – Treat underlying systemic disease