Diseases of excretory system
52
DR.A.S.SHIVA SARAVANAN,B.H.M.S.,M.D(HOM) ASSISTANT PROFESSOR DEPARTMENT OF SURGERY VMHMC SALEM DISEASES OF EXCRETOY SYSTEM
-
Upload
shiva-saravanan -
Category
Healthcare
-
view
19 -
download
0
Transcript of Diseases of excretory system

DR.A.S.SHIVA SARAVANAN,B.H.M.S.,M.D(HOM)ASSISTANT PROFESSOR
DEPARTMENT OF SURGERYVMHMCSALEM
DISEASES OF EXCRETOY SYSTEM

HAEMATURIA
Types Gross (visible to unaided eye). Microscopic (>5 RBC’s / HPF).
Early (initial) haematuria: Urethral origin, distal to external sphincter.
Terminal haematuria: Bladder neck or prostrate orgin.
Diffuse (total) haematuria: Source is in the bladder or upper urinary tract.
False haematuria: Discolouration of urine from pigments such as food colouring
and myoglobin.Silent haematuria is due to tumors of kidney or
bladder unless proved otherwise.2/10/2017
2

CAUSES
Renal injury Urinary stones Wilm’s tumorTuberculosis Renal cell carcinomaCysititis Bladder tumourUrinary bilharziasisBPH, carcinoma prostateRenal infarctGlomerulonephritisBlood dyscrasias
2/10/2017
3

INVESTIGATION
Urine culture and sensitivity (urine test for haematuria – Benzidine test).
Ultrasound to look for the stone, tumor in the urinary tract.
Cystourethroscopy to look for bladder or urethral pathology.
IVU look for function of the kidneys.Urinary cytology for diagnosing urothelial
malignancy.Bleeding time; clotting time; prothrombin time;
platelet count.CT abdomen.Renal function tests – blood urea, serum creatinine.
2/10/2017
4

MANAGEMENTCauses should be identified and treated.Blood transfusion.Antibiotics.Nephro – ureterectomy for RBC; removal of stone
from kidney, ureter, urinary bladder.Treatment of bladder tumour by cystoscopic
resection; intravesical chemotheraphy using BCG; radiotheraphy; systemic chemotherapy.
Treatment of medical causes like glomerulonephritis.
Correction of BPH.Correction of bleeding diathesis.
2/10/2017
5

HORSESHOE KIDNEY
2/10/2017
6

It is a developmental anomaly where there is failure of complete ascent of kidneys with the fusion of lower or upper poles.
It is due to fusion of subdivisions of mesonephric duct, when the embryo is as early as 30-40 days old.
This condition is common in males.Fusion of lower pole is common (rarely upper
poles). Commonest site is in front of the 4th lumbar
vertebrae. The part in front of the vertebrae is called as isthumus.
It has blood supply which freely communicates one kidney to other.
Isthumus usually lies in front of aorta.2/10/2017
7

CLINICAL FEATURES
Presents as a fixed, nonmobile, firm mass in the midline at the level of 4th lumbar vertebra which is resonant on percussion.
It is more prone for infection, stone formation, hydronephrosis, tuberculosis.
2/10/2017
8

DiagnosisIUV – medialisation of lower calyces and curving
of ureter like a ’flower vase’.
U/S abdomen.
Urine analysis, blood urea and serum creatinine are supportive investigations.
CT abdomen.
TreatmentWhatever the complications occurs in horseshoe
kidney, it is treated accordingly.2/10/2017
9

CYSTIC DISEASES OF THE KIDNEY
2/10/2017
10

Kidney cyst Types
Genetic:Adult polycystic kidney disease (Autosomal
dominant)
Infantile polycystic kidney disease (Autosomal recessive)
Nongenetic – Simple cyst, multicystic kidney, medullary sponge kidney.
Acquired renal cystic kidney may develop in patient on long term dialysis. 2/10/2017
11

POLYCYSTIC KIDNEY DISEASE (PCKD)
2/10/2017
12

Adult PCKD is inherited as autosomal dominant disease. It is common in females.
It is bilateral and presents in third decade. One side presents little earlier than other side.
AassociationsPolycystic disease of liver (18%), pancreas and lung.Berry aneurysm in the circle of willis.Cyst formation occurs at the junction of the distal
tubule and the collecting duct.Grossly it contains multiple cysts with a clear or
brownish fluid (due to haemorrhage).2/10/2017
13

CLINICAL FEATURES
Bilateral palpable renal massLoin painHaematuria InfectionHypertension, uraemia.
2/10/2017
14

Differential DiagnosisRenal cell carcinomaHydronephrosisSolitary renal cystInvestigationsU/S confirms the presence of cysts.IUV – Spider leg pattern with an elongated compressed
renal pelvis, narrowed and stretched calyces.Blood urea and serum creatinine to rule out renal
failure.Urine shows low specific gravity.
2/10/2017
15

TREATMENTWait and watch policy.If one of the cysts overdistends causing pain,
haemorrhage, infection, then surgical intervention is required.
Rovsing operation – The kidney is exposed. The cyst is opened. The fluid is evacuated. The cut edge is marsupialised.
Presently U/S guided aspiration is done as a simpler approach.
Laproscopic / retro peritoneoscopic aspiration / deroofing of the renal cyst.
Once renal failure sets in, in then initial haemodialysis followed by bilateral nephrectomy, is done and later renal transplantation should be planned for. 2/10/2017
16

SOLITARY RENAL CYST
Solitary renal cyst is never congenital.It is due to an earlier trauma or infection
resulting in blockage of tubule, leading to cyst formation.
It is usually unilateral, presents as a renal mass which is smooth, often if infected or haemorrhagic.
InvestigationU/S and IVU confirms the diagnosis.CT scan positive.
2/10/2017
17

TREATMENT
Kidney is exposed. The cyst is aspirated and a portion of the cyst wall is removed
( Kirwin’s operation) and cavity is filled with perinephric fat.
Occasionally if the cyst is in one of the pole, partial nephrectomy is done.
Laparoscopic approach.
2/10/2017
18

RETROCAVAL URETER
2/10/2017
19

RETROCAVAL URETER
It is due to developmental defect of IVC, as a result of which right ureter passes behind the IVC, causing right sided hydronephrosis with upper third hydroureter.
IVU shows hydronephrosis with ‘reverse J sing’.
Treatment: Anderson Hynes’ operation
2/10/2017
20

URETEROCELE
2/10/2017
21

URETEROCELE
It is a cystic enlargement of the intramural portion of ureter due to congenital atresia of the ureteric orifice. Its wall contains mucous membrane only.
It is common in females, often bilateral (10%).
Complication Stone formationRecurrent infectionHydronephrosis
2/10/2017
22

INVESTIGATION
IVU-Shows Adder-head appearance or cobra head appearance.
Cystoscopy-Shows translucent cyst which is thin walled surrounding the ureteric orifice.
TreatmentCystoscopic ureteric meatotomy with the
removal of cyst wall.In addition to that co-existing complications
should be treated.Often ureteric re-implantation is needed.
2/10/2017
23

INJURIES TO KIDNEY
Commonly it is due to a blunt injury.Often it is associated with other abdominal
injuries of liver, spleen, bowel, mensentery, etc.Per se renal injury is extraperitoneal.TYPE OF RENAL INJURYSmall subcapsularLarge subcapsularCortical lacerationLaceration with perinephric haematoma.
2/10/2017
24

Medullary laceration with bleeding into the renal.
Corticomedullary complete rupture.Hilar injury (most dangerous).Grading Of Renal InjurySubcapsular non-expanding haematoma
without parenchymal lancerationCortical laceration < 1 cm of parenchymal
depth, no extravasation; perirenal haematomaCortical lacertion > 1 cm depth; no urine
extravasationParenchymal laceration extending through
cortex and medulla with collecting system; with extravasation of urine
Renal pedicle avulsion; shattered kidney2/10/2017
25

CLINICAL FEATURES
Features of shock.Haematuria-may be mild to profuse
depending on the type of injury.Clot colic.Bruising, swelling and tenderness in the loin.Paralytic ileus with abdominal distension
occurs due to retroperitoneal haematoma implicating splanchnic nerves.
2/10/2017
26

COMPLICATIONS
Clot retention in the bladder and may go for renal failure
Pararenal pseudo hydronephrosisInfectionPerinephric abscessAneurysm of the renal arteryRenal failureHypertension occurs 3 months later
2/10/2017
27

INVESTIGATIONS
IVU(high dose)-It is the investigation of choice. Here function of not only the injured kidney but also of the contralateral kidney can be soon. It is observed that often opposite renal artery undergoes a reflex spasm, temporarily ceasing the function of the contralateral kidney.
U/S abdomen-Done to see the type of injury, amount of haematoma and other associated at regular intervals to see the progress (at 12-24 hourly).
Blood urea and serum creatinine should be repeated at regular intervals.
Blood grouping and cross-matching for blood transfusion.
Emergency CT scan is very useful.
2/10/2017
28

TREATMENTInitially always conservation:Catheterise and watch the urine colour and output.Blood transfusion.Sedation observation with regular monitoring of
the pulse, BP, temperature, U/S follow-up daily.75% of patients respond to conservative mana-
gement.While treating conservatively, regular monitoring
of blood urea and serum creatinine is a must.If the patient goes in for 6-8 weeks. Meanwhile,
other kidney starts functioning again and patient recovers without any further problem.
2/10/2017
29

Indications for surgical intervention: When there are signs of progressive blood loss
with the condition of the patient deteriorating. Formation of progressive perinephric
haematoma. When there are associated other injuries. Hilar injury.
Surgery Options:Gentle suturing of the laceration. Often
kidney is friable, this is not possible.Then nephrostomy is in the poles partial
nephrectomy is done.In hilar injury and severe laceration,
nephrectomy is the only choice.2/10/2017
30

RENAL CALCULI
2/10/2017
31

RENAL CALCULI
It is more common in males;
90% are radiopaque (gallstones are more common in females; 90% are radioluscent).
AETIOLOGYDiet: Vitamin A
deficiency – it causes desquamation of epithelium which acts as a nidus for stone formation.
2/10/2017
32

Climate: In hot climate urinary solutes will increase with decrease in colloids, which leads to chelation of solute with calcium forming a nidus for stone.
Citrate level in urine (300-900 mg/ 24 hours) maintains the calcium phosphate and carbonate in soluble state and any decrease in citrate level in urine causes stone formation.
Infection in kidney: Urea splitting organisms commonly cause stone formation.
Prolonged immobilization causes decalcification of bones and so hypercalciuria leading to stone formation.
2/10/2017
33

Hyperparathyroidism causes hypercalciuria causing multiple bilateral stones or often bilateral nephrocalcinosis.
Hyperoxaluria, as a result of altered glycine metabolism.
Cystiniuria.
Stasis due to obstruction to urine flow.
Medullary sponge kidney.
Randall’s plaque theory is erosion and deposition of urinary salts as Randall’s plaque at the apex of renal papillae. 2/10/2017
34

Carr’s postulates states that minute concentrations called as microliths normally develop in the subendothelial part of the tubule which will be carried away as particles by renal lymphatic network vessels. If these lymphatics are blocked, microliths enlarge and acts as nidus for stone formation.
Others: sarcoidosis, myelomatosis, gout, idiopathic hypercalciuria, hypervitaminosis D, neoplasms on treatment, hypomagnesuria.
Renal tubular acidosis: Commonly causes calcium phosphate stone (10%). 2/10/2017
35

Stages of stone formation Supersaturation Nucleus formation Crystillisation Aggregation Matrix formation Stone
Epitaxy:
Growth of one type of stone on another type.
2/10/2017
36

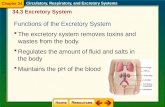
RENAL CALCULI-TYPES
Oxalate stones (75%) also called as mulberry stone as it is brown in colour, with sharp projections.
It is invariably calcium oxalate stone, shows envelope crystals in urine.
Phosphates stones (10-15%): it is either calcium phosphate or calcium, magnesium, ammonium phosphate stone usually occurring in an infected urine.
It is smooth and white occurring in an infected urine. It is smooth and white in colour.
In an alkaline urine it enlarges rapidly, filling renal calyces taking their shape called as staghorn calculus. It is radiopaque and attains a large size.
2/10/2017
37

2/10/2017
38

2/10/2017
39

Uric acid stones are smooth, hard, yellowish, multiple and radioluscent. They are seen in gout, hyperuricosuria, altered purine metabolism.
Urate stones.
Cystine stones occur in cystinuria where there is defective absorbtion of cystine from the renal tubules. It is seen in young girls, occurs only in acidic urine.
It is multiple, soft, yellow in colour changes to greenish hue on exposure. It attains large size.
It is radiopaque because it contains sulphur.2/10/2017
40

Xanthine stones are very rare, smooth, brick red in colour, due to altered xanthine metabolism. Here there is deficiency in xanthine oxidase enzyme.
Indigo stones: very rare. Blue in colour.
Struvite stone: it is compound of magnesium, ammonium phosphate mixed with carbonate. It occurs in presence of ammonia and urea splitting organisms in urine, eg. Proteus; Klebsiella.
2/10/2017
41

CLINICAL FEATURESPain – renal pain is located over renal angle,
hypochondrium and lumbar region.
Often severe radiating to groin and testis in males, with vomiting due to pylorospasm. Pain worsens on movements.
Haematuria is common, Pyuria, Fever.
Tenderness in renal angle, with often a mass in the loin due to hydronephrosis which moves with respiration and is bimanually palpable, ballotable, smooth, soft. 2/10/2017
42

As urinary tract infection.Incidental finding.Often hypertension
2/10/2017
43

INVESTIGATIONS
2/10/2017
44

Blood: ESR, serum calcium, phosphate, creatinine, blood urea, uric acid, PTH level.
Urine: Calcium, urate, cystine if suspected only pH, specific gravity.
Plain X-ray, KUB: to see kidney shadow, stones (90% - radiopaque).
IVU to see renal functions and HN.RGP if required.U/S abdomen – can detect even radioluscent
stones and gives information about the changes in renal parenchyma.
Urine analysis and C/S to identify bacteria.
2/10/2017
45

SURGICAL TREATMENT
PCNL (Percutaneous Nephrolithotomy)
Indications:
Stones more than 2.5cm in size.
Multiple stones
Stones not responding for ESWL
2/10/2017
46

Procedure: Under the guidance of C-Arm or U/S, needle puncture is
made in the loin percutaneously. Through kidney, calyx and pelvis are approached. Guidewire is passed. Graduated dilators are passed and so track is widened. Then through that, a nephroscope is passed. After fragmentation, stone is removed using different methods.
COMPLICATIONS OF PCNLHaemorrhage
Perforation of collecting duct
Injury of collecting duct2/10/2017
47

ESWL (Extracorporeal Shock Wave Lithotripsy)
Piezo-Ceramic or Electromagnetic shock waves are passed to the stone through water bath or water n which acts as a media. Shock are produced at 2/sec, 1000-4000 shocks are required for each stone.
Dornier Lithotripter is used for fragmenting stones.
Stone is located and observed through fluoroscope (C-ARM) or ultrasound. Shock waves are triggered to create compressive waves over the stone, to fragment it. These fragments are flushed out later.
2/10/2017
48

SURGERIES
Pyelolithotomy.Suitable for stones in extra renal pelvis.By loin incision, kidney is approached.Renal pelvis is opened, the stone is removed
and pelvis is closed. A drain is placed and wound is closed
2/10/2017
49

Extended pyelolithotomy: In case of intrarenal pelvis, incision is done on the hilum
between the pelvis and kidney over the renal sinus, dissection is carried out so as to remove the stones from pelvis as well as calyces.
Nephrolithotomy: By placing incision just behind the most convex surface,
stone is removed.
Nephropyelolithoyomy: by making incisions both over the kidney and pelvis, stones /
stones are removed. It is often done in staghorn calculus.
2/10/2017
50

Partial nephrectomy: done when there are multiple stones occupying a pole, usually lower pole of the kidney or when there is damage to the calyx, if not removed may encourage further stone formation.
Bench surgery: kidney is removed out temporarily, cooled by ice packs or inosine or liquid nitrogen. Stones are searched and removed completely. Later kidney is replaced in right iliac fossa. 2/10/2017
51

Anatrophic pyelolithotomy: after exposing the kidney, it is cooled with ice packs for 20 minutes and posterior branch of the renal artery is clamped temporarily using bull-dog clamp.
The most avasular plane behind the Brodel’s line is thus visualized properly. Kidney is opened trough this line and stone/stones are removed
2/10/2017
52