Disease-Specific Patient-Reported Outcome Tool in Head and ...€¦ · Disease-Specific...
9
Disease-Specific Patient-Reported Outcome Tool in Head and Neck Cancer Patients Kathryn M. Campion, BSN, RN, CEN Bimbola F. Akintade, PhD, MBA, MHA, ACNP-BC, NEA-BC Background Purpose Methods Results Discussion Conclusions Acknowledgements • Head and neck cancers (HNC) have a five-year survival rate of 62% • Effects of chemotherapy, radiation, and the disease can be debilitating • Common side effects: dysphagia, dysgeusia, insomnia, nausea, vomiting, fatigue, and mucositis • Patient reported outcome tools (PROs) provide a quantitative measurement of symptoms • Can improve symptom management, communication, and patient satisfaction • The Functional Assessment of Cancer Therapy: Head and Neck Symptom Index (FACT: HNSI) is a validated and reliable HNC PRO The purpose of this quality improvement project (QI) is to implement the FACT: HNSI PRO tool among dual modality HNC (DMHNC) patients in outpatients at a large, academic, urban hospital by December 1, 2019 Short-term goals: • Interview the team to assess barriers to use of the PRO tool • >65% of DMHNC patients completing the PRO tool each week • >65% of the HNC team referring to the PRO in progress notes Desired long-term impact: decrease in DMHNC treatment deviations, unplanned admissions, ER visits, and oncology urgent care visits Inclusion criteria: • All new adult DMHNC patients with access to patient portal • In weeks one to three of treatment as of October 1, 2019 Exclusion criteria: • Decline to participate, non-DMHNC, no access to patient portal Implementation: October 1, 2019- December 1, 2019 Structure change: • Imbed FACT: HNSI into the patient portal • Interdepartmental approval, dedicated information technology specialist, funding for expedited build Process changes: • Patients completing PROs each week • Staff using dedicated smartphrase in weekly progress notes Procedures: • Staff and patient education (verbal and written) • Pre- and post- implementation surveys to evaluate perceived usefulness of the PRO tool and ease of use • Weekly audits to monitor staff/patient compliance • Chart audit on 20 encounters to evaluate staff’s consistency of capturing symptoms from the FACT:HNSI before implementation Eleven patients participated in the weekly PROs • Overall use of PRO by patients was 68.2% Six HNC treatment staff participated in utilization of the designated smartphrase • Overall use of smartphrase by staff was 78.8% 68% 32% Patient Compliance Compliant Non- compliant 79% 21% Staff Compliance Compliant Non- compliant Staff survey results revealed an overall view that PROs are beneficial, the FACT: HNSI was a useful tool, easy to use, and it did not extend the length of visits 0 1 2 3 4 5 PROs are beneficial. FACT:HNSI is useful in alerting of symptoms. PRO extends the length of patient visits/assessments. Perceived ease of use. Average Response (1=Strongly Disagree; 5= Strongly Agree) Survey Questions Pre- and Post- Staff Survey Comparison Pre- Implementation Average Post-Implementation Average In the retrospective chart audit: • 46% of the symptoms listed in the FACT-HNSI were routinely captured by the HNC treatment team in the six months before PRO implementation Staff feedback: • Instances of smartphrase omission were unintentional Patient feedback: • Helpful in communicating with team; discomfort with technology • Difficulty completing surveys with more severe side effects Limitations: • English as a second language, illiteracy, no home computer and smart devices limits widespread patient use • Small sample size and limited implementation time • Unverified PRO author may introduce bias Lessons Learned: • Training staff to manually enter results can help mitigate barriers • Champions useful to maintain patient and staff compliance • Survey in the electronic health record facilitated use by patients and staff References • This QI project achieved the short-term goals of >65% compliance for patient and staff participation during the nine-week implementation • The chart audit revealed 46% of the FACT: HNSI symptoms were identified by staff in the six months prior to implementation. During implementation 100% of the symptoms were captured each time a PRO was completed by a patient and reviewed with a staff member • Future QI projects: • Impact of the FACT: HSNI on unplanned admissions, emergency department visits, and oncology urgent care visits long-term • Facilities treating outpatient HNC patients should incorporate the FACT: HNSI to improve the detection of symptoms and patient and staff communication Niska, J. R., Halyard, M. Y., Tan, A. D., Atherton, P. J., Patel, S. H., & Sloan, J. A. (2017). Electronic patient-reported outcomes and toxicities during radiotherapy for head-and-neck cancer. Quality of Life Research, 26, 1721- 1731. doi: 10.1007/s11136-017-1528-2 Peng, L. C., Hui, X., Cheng, Z., Bowers, M. R., Moore, J., Cecil, E., … & Quon, H. (2018). Prospective evaluation of patient reported swallow function with the Functional Assessment of Cancer Therapy (FACT), MD Anderson Dysphagia Inventory (MDADI) and the Sydney Swallow Questionnaire (SSQ) in head and neck cancer patients. Oral Oncology, 84, 25-30. https://doi.org/10.1016/j.oraloncology. 2018.05.0 ◇ Dr. MiKaela Olsen ◇ Dr. Tanguy Lim-Seiwert ◇ Mr. Benjamin Smith ◇ Implementation team ◇ Skip Viragh staff 0 10 20 30 40 50 60 70 80 General pain Swallowing Trouble breathing Nausea Worry % of Time Symptoms Present on Chart Audit Symtoms from FACT:HNSI Retrospective Chart Audit *Question three is phrased in the negative*
Transcript of Disease-Specific Patient-Reported Outcome Tool in Head and ...€¦ · Disease-Specific...

Disease-Specific Patient-Reported Outcome Tool in Head and Neck Cancer Patients
Kathryn M. Campion, BSN, RN, CENBimbola F. Akintade, PhD, MBA, MHA, ACNP-BC, NEA-BC
Background
Purpose
Methods
Results Discussion
Conclusions
Acknowledgements
• Head and neck cancers (HNC) have a five-year survival rate of 62%• Effects of chemotherapy, radiation, and the disease can be
debilitating• Common side effects: dysphagia, dysgeusia, insomnia, nausea,
vomiting, fatigue, and mucositis• Patient reported outcome tools (PROs) provide a quantitative
measurement of symptoms• Can improve symptom management, communication, and
patient satisfaction• The Functional Assessment of Cancer Therapy: Head and Neck
Symptom Index (FACT: HNSI) is a validated and reliable HNC PRO
The purpose of this quality improvement project (QI) is to implement the FACT: HNSI PRO tool among dual modality HNC (DMHNC) patients in outpatients at a large, academic, urban hospital by December 1, 2019
Short-term goals:• Interview the team to assess barriers to use of the PRO tool• >65% of DMHNC patients completing the PRO tool each week• >65% of the HNC team referring to the PRO in progress notes
Desired long-term impact: decrease in DMHNC treatment deviations, unplanned admissions, ER visits, and oncology urgent care visits
Inclusion criteria:• All new adult DMHNC patients with access to patient portal• In weeks one to three of treatment as of October 1, 2019
Exclusion criteria:• Decline to participate, non-DMHNC, no access to patient portal
Implementation: October 1, 2019- December 1, 2019Structure change:
• Imbed FACT: HNSI into the patient portal• Interdepartmental approval, dedicated information technology
specialist, funding for expedited buildProcess changes:
• Patients completing PROs each week• Staff using dedicated smartphrase in weekly progress notes
Procedures:• Staff and patient education (verbal and written)• Pre- and post- implementation surveys to evaluate perceived
usefulness of the PRO tool and ease of use• Weekly audits to monitor staff/patient compliance• Chart audit on 20 encounters to evaluate staff’s consistency of
capturing symptoms from the FACT:HNSI before implementation
Eleven patients participated in the weekly PROs• Overall use of PRO by patients was 68.2%
Six HNC treatment staff participated in utilization of the designated smartphrase• Overall use of smartphrase by staff was 78.8%
68%
32%
Patient Compliance
Compliant
Non-compliant 79%
21%
Staff Compliance
Compliant
Non-compliant
Staff survey results revealed an overall view that PROs are beneficial, the FACT: HNSI was a useful tool, easy to use, and it did not extend the length of visits
012345
PROs arebeneficial.
FACT:HNSI isuseful in alerting of
symptoms.
PRO extends thelength of patient
visits/assessments.
Perceived ease ofuse.
Aver
age
Res
pons
e(1
=Stro
ngly
Dis
agre
e;
5= S
trong
ly A
gree
)
Survey Questions
Pre- and Post- Staff Survey Comparison
Pre- Implementation Average Post-Implementation Average
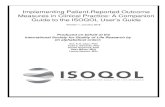
In the retrospective chart audit:• 46% of the symptoms listed in the FACT-HNSI were routinely captured by
the HNC treatment team in the six months before PRO implementation
Staff feedback: • Instances of smartphrase omission were unintentional
Patient feedback: • Helpful in communicating with team; discomfort with technology• Difficulty completing surveys with more severe side effects
Limitations:• English as a second language, illiteracy, no home computer and
smart devices limits widespread patient use• Small sample size and limited implementation time• Unverified PRO author may introduce bias
Lessons Learned:• Training staff to manually enter results can help mitigate barriers• Champions useful to maintain patient and staff compliance• Survey in the electronic health record facilitated use by patients
and staff
References
• This QI project achieved the short-term goals of >65% compliance for patient and staff participation during the nine-week implementation
• The chart audit revealed 46% of the FACT: HNSI symptoms were identified by staff in the six months prior to implementation. During implementation 100% of the symptoms were captured each time a PRO was completed by a patient and reviewed with a staff member
• Future QI projects: • Impact of the FACT: HSNI on unplanned admissions, emergency
department visits, and oncology urgent care visits long-term• Facilities treating outpatient HNC patients should incorporate the
FACT: HNSI to improve the detection of symptoms and patient and staff communication
Niska, J. R., Halyard, M. Y., Tan, A. D., Atherton, P. J., Patel, S. H., & Sloan, J. A. (2017). Electronic patient-reported outcomes and toxicities during radiotherapy for head-and-neck cancer. Quality of Life Research, 26, 1721- 1731. doi: 10.1007/s11136-017-1528-2
Peng, L. C., Hui, X., Cheng, Z., Bowers, M. R., Moore, J., Cecil, E., … & Quon, H. (2018). Prospective evaluation of patient reported swallow function with the Functional Assessment of Cancer Therapy (FACT), MD Anderson Dysphagia Inventory (MDADI) and the Sydney Swallow Questionnaire (SSQ) in head and neck cancer patients. Oral Oncology, 84, 25-30. https://doi.org/10.1016/j.oraloncology. 2018.05.0
◇ Dr. MiKaela Olsen ◇ Dr. Tanguy Lim-Seiwert◇ Mr. Benjamin Smith ◇ Implementation team◇ Skip Viragh staff
0 10 20 30 40 50 60 70 80
General pain
Swallowing
Trouble breathing
Nausea
Worry
% of Time Symptoms Present on Chart Audit
Sym
tom
s fro
m F
ACT:
HN
SI
Retrospective Chart Audit
*Question three is phrased in the negative*

Integration of TeamSTEPPS Framework and Escape Room to Improve Teamwork and Collaboration
Suzanna Fitzpatrick, MS, CRNP; Dr. Hazel Jones-Parker, DNP, CRNP, AACRN;& Dr. Andrea Smith, MBA, DNP, CRNP
University of Maryland School of Nursing
Difficulty with communication and teamwork in a large adult emergency department has been identified and senior nursing leadership wanted to enhance collaboration and communication in their workplace. This DNP project leveraged the integration of TeamSTEPPS training and tools in an escape room setting in order to optimize team performance of a group of senior nurse leaders. • Currently, standard leadership courses, conferences and other
didactic learning methods are utilized for teamwork improvement. • Poor communication and team work can threaten patient safety• Escape rooms, live action, team-based exercises (Adams & Crawford,
2018), supplemented with TeamSTEPPS tools can assist in optimizing team performance, while keeping the participant engaged in a new learning environment and has been shown to improve leadership skills.
Problem Statement
An evidence-based Quality Improvement project at a large inner city Adult Emergency Room with senior clinical nurses aimed to:
• Improve communication and teamwork skills• Utilize an escape room as a training tactic• Assess escape room concept as a training tool
Goals: • Short Term: 4-6 members of the quality improvement team will
have completed TeamSTEPPS training and familiarization with escape room and exercise so they may train others on TeamSTEPPS utilizing the escape room tactic and team dynamics and leadership improvement for project sustainability.
• Long Term: All SCN Emergency Department nurses will change their leadership skills and improve team cohesiveness by completing an escape room and TeamSTEPPS course
Purpose
ResultsThis group of ED nurses completed 2 escape rooms and a TeamSTEPPS training and all agreed that an escape room can be a fun way to motivate while providing an effective team building activity. • This group of nurse leaders validated the integration of
TeamSTEPPS tools and strategies in an escape room setting• All participants voiced the experience was enjoyable and an
engaging way to learn while providing an effective team building activity.
• This small cohort, in line with the literature, demonstrates that new methods of learning such as an escape room should be explored for engaging participants and improving communication and teamwork skills.
Limitations: • Small sample size• Time constraints• Varying escape room exercises• Lack of demographics• Not all survey questions were answered by all participants
Further recommendations:• Larger sample size • Dedicated time for TeamSTEPPS training and strategies
Discussion
Escape rooms can be a dynamic and interactive way to promote team training and education. Integration of TeamSTEPPS tools and strategies within the escape room framework provides for an engaging learning environment where participants can deepen their understanding of concepts through active learning. While this was just a small sample in one intercity hospital, new methods for learning should be reviewed for successful teamwork
Conclusions
Study Design• 14-week Quality Improvement Project
Guided by MAP-IT Framework Includes Observation at staff meetings Weekly check-ins with manager and assistant manager Escape room exercise with TeamSTEPPS training completion of
perceptions tools Weekly education on teamwork via email following escape room
• Completion of pre/ post-escape room toolsSample• 12 senior clinical nurse (n=12)
1- less than 1 year SCN experience 5 – 1-4 years SCN experience 6- greater than 4 years SCN experience
• Including 1 nurse manager• Including 1 assistant nurse manager
11 female: 1 male
Methods
• Adams, V., Burger, S., Crawford, K., & Setter, R. (2018). Can you escape? Creating an Escape Room to facilitate active learning. Journal for Nurses in Professional Development 34 (2). E1-E5. doi:10.1097/NND.0000000000000433.
• Sheppard, F., Williams, M., & Klein, V. (2013) TeamSTEPPS and patient safety in healthcare. Risk Management. 32(3); 5-10. doi: 10.1002/jmrm.21099.
• Yi, Y. (2015). Effects of team-building on communication and teamwork among nursing students. International council of nurses. 63 (1) 33-40. doi: 10.111/inr.12224.
References
Figure 1: Feedback Results
Figure 2: Perceptions Tool Results
2
5
0
7
1 1
4
2
1
2
0
2
1
0 0 0 0
2
0 0
2
3
0 0
3 3
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10 11 12 13
Num
ber o
f Fee
dbac
ks
Interval In Weeks
Total Feedback During Project
Negative Written Feedback Positive Documented Feedback
Perceptions Category Before Intervention After Intervention Score Change
Team Structure 3.39 3.76 0.37
Leadership 3.86 4.22 0.36
Situational Monitoring 3.27 3.72 0.45
Mutual Support 3.75 3.73 -0.02
Communication 3.5 3.82 0.32
Standard Deviation 0.163535929
p= 0.0111
Figure 3 : Observation Tool Results
Observational Category Before Intervention After Intervention Score Change
Team Structure 11 12.5 1.5
Communication 9.5 15.5 6
Leadership 15.5 24 8.5
Situational Monitoring 14.5 19 17.5
Mutual Support 9.5 15.5 6
Standard Deviation 6.73764301
p=0.004933

1. Ajzen I. (1985) From Intentions to Actions: A Theory of Planned Behavior. In: Kuhl J., Beckmann J. (eds) Action Control. SSSP Springer Series in Social Psychology. Springer, Berlin, Heidelberg
2. American Academy of Pediatrics. (2014). Addressing adverse childhood experiences and other types of trauma in the primary care setting. American Academy of Pediatrics.
3. Purewal, S. K., Bucci, M., Wang, L. G., Koita, K., Marques, S. S., Oh, D., & Harris, N. B. (2016). Screening for adverse childhood experiences in an integrated pediatric care model. Zero to Three, 36(3), 10-17.
• Training was effective in increasing stakeholder knowledge, ability, and value towards screening for ACEs
• Results support that an ACEs screening program using the CYW ACE-Q screening tools is an effective strategy for pediatric primary care providers to identify and refer children at high risk for mental and physical illnesses to MHS
• Underscreening attributed to patient/caregiver factors or workflow constraints
• Under-referral attributed to provider oversight or unfamiliarity with procedure
• Failure to make referral appointment suggests gap in obtaining mental health care after referral
• Low overall need for referral reflects high sociodemographic of practice site, supports tool reliability and the current literature
• Barriers and Limitations: • Limited generalizability of findings• Sensitive nature of screening subject• Non-electronic format• Completed screens not being seen by the provider
Adverse Childhood Experiences (ACEs) are stressful or traumatic events experienced before age 18 years old that correlate with increased risk for poor physical, mental, and behavioral health outcomes• 50-60% of children have >1 ACE and over 25% have >3
ACEs• ACEs cross all demographics and socioeconomic strata• There is a graded relationship between number of ACEs
and risk for physical and mental illness• Screening for ACEs allows for early identification and
referral to mental health services (MHS) to reduce risk for poor physical and mental health outcomes
Background
To evaluate implementation of an ACEs Screening Program in a pediatric primary care practice to identify and refer children at high risk for mental illnessShort-term Goals• Increase staff and health care provider’s knowledge,
ability, and value for ACEs screening• Screen >25% of eligible patients at the project site during
the first month of implementationLong-term Goal• Screen >80% of eligible patients at the project site by
project end• Refer 100% of positive-screening patients to MHS by
project end
Purpose Statement and Goals Results
Discussion
Conclusions
• Ajzen’s Theory of Planned Behavior guided the Quality Improvement project in a privately-owned pediatric primary care practice in N.W. Washington, D.C.
• Target Sample: Caregivers of patients ages 8-18 years old and patients ages 13-18 years old presenting for well visits or consults
Pre-Intervention• Pre-Implementation chart audits to collect baseline data
on documented ACEs and referrals to mental health care• Training session to educate all staff and health care
providers on ACEs and the upcoming Screening ProgramIntervention• ACEs Screening Tool completed by guardian or patient at
time of check-in for scheduled primary care appointment• ACEs Screening results reviewed with health care
provider during visit• Patients with a positive screen referred by health care
provider to MHS• Follow up phone calls by nurses to all referred patients 60
days after referral to see if MHS appointment obtained
Methods
References
Screening for Adverse Childhood Experiences in Pediatric Primary Care
Sarah M. Gross, BSN, RN & Renee Franquiz, DNP, RN, CNE University of Maryland School of Nursing
• This project demonstrated that successful implementation of an ACEs screening program in the pediatric primary care setting is feasible and valued by health care providers
• Data supports the CYW ACE-Q screening tools as accurate and reliable for detecting ACEs as the first step in the mental health care continuum
• Gaps exist in continuity of care as evidenced by limited patient follow-up with mental health services after referral
• Future initiatives recommended to improve use of tool’s symptom criteria, referrals, and referred patient follow-up with MHS. Ideas for strengthening include using an electronic tool, robust tracking after referral, and expanding the population demographic
Median
Goal
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
Week 7
Week 8
Week 9
Week 10
Week 11
Week 12
Week 13
Percentage of Eligible Patients Screened for ACEsPercentage of Completed ACEs Screens
25%
50%
80%
71%
MeasuresStakeholder Knowledge-Skill-Attitude Survey of ACEs Screening:• 8 item Likert, student developed, anonymous survey, administered electronically
pre, mid, and post-implementationACEs Screening Tool- Center for Youth Wellness Adverse Childhood Experiences Questionnaires (CYW ACE-Q):• Age-dependent, 17-19 item, yes/no, aggregate-level validated screening tool• Higher score equates with higher risk of health and social problems• Three Versions: Child or Teen Caregiver Report and Teen Self-Report Project Tracking/Audit Tool• ACEs Screening Audit Tool and Referral Follow-Up Tracking Tool• Weekly tracking of progress to goals
ACEs Screening Program Outcomes
Post-Implementation Stakeholder Survey n %“Agree” or ”Strongly Agree” Responses: Screening Program is Feasible 8* 88%Desire to Continue ACEs Screening Program 8* 100%
Screening ResultsScreens Distributed to Eligible Patients 245/325 75%Screens Completed 232/325 71%Positive Screens• Currently under MHS• Referred for MHS
32/23226/32 4/6
14%81%66%
Referral Follow-Up with MHS 1/4 25%Note. *= 8 stakeholders completed surveys out of 12 total stakeholders; MHS= Mental Health Services
Special thanks to Jessica Long, M.D. (Clinical Site Representative) and Angel Jackson (Project Champion) for their continued support and guidance through this project

• Primary care practice in rural Maryland county reported high rates of alcohol or drug use disorders
• County drug related overdoses: 2016=412; 2017=510• Practice lacked screening tools and referral resources• SBIRT is a comprehensive early intervention approach that
includes universal substance screening and appropriate interventions to help patients reduce substance-related risks
Background Results
• Monitor missed screening opportunities • Acknowledge staffing issues and time constraints • Use validated screening tools • Facilitate team approach • Foster organizational leadership and physician involvement• Increase knowledge of alcohol and drug use• Reduce stigma of addiction
Practice Recommendations
Short Term Goals:• Universal screening of at least 80% of eligible patients; • 100% of all individuals with a positive screen will receive
either a Brief Intervention or a Referral to TreatmentLong Term Goals:• Improved rates of treatment referrals• Improved rates of treatment completion • Reduction of substance-related risks
Objectives
Evidence Table/Selected Results
Aldridge, A., Linford, R., & Bray, J. (2015). Substance use outcomes of patients served by a large US implementation of screening, brief intervention, and referral to treatment (SBIRT). Addiction. 112(2), 43-53. doi:10.1111/ass.13651
Gryczynski, J., Mitchell, G.S., Peterson, T.R., Gonzales, A., Moseley, A., & Schwartz, R.P. (2011). The relationship between services delivered and substance use outcomes in New Mexico’s screening, brief intervention, referral and treatment (SBIRT) initiative. Drug and Alcohol Dependence. 118,152-157. doi:10.1016/j.drugalcdep.2011.03.012
Moyer, V.A. & U.S. Preventive Services Task Force (2013). Screening and behavioral counseling interventions in primary care to reduce alcohol misuse: U.S. Preventive Services Task Force recommendation. Annals of Internal Medicine.159, 210-218.
References
• Practice Question: • Can SBIRT be implemented feasibly and effectively within
a small, rural Maryland primary care practice?• Population: Adults 18 years old and older• Search Platform: PubMed and the Cumulative Index of
Nursing and Allied Health Literature • Keywords searched: “substance use screening”; “SBIRT in
primary care”; “screening brief intervention and referral to treatment in primary care”
• Appraisal of level & quality of evidence: Johns Hopkins Nursing Evidence-based Practice Rating Scale (Newhouse, et al., 2006)
• Project Development: Seven Steps of Evidence-based Practice Model (Melnyk & Fineout-Overholt, 2011)
• Project Implementation: Mobilize, Assess, Plan, Implement and Track (MAP-IT) Framework
• SBIRT Instruments:• Alcohol Pre-Screen: 3-item Alcohol Use Disorders
Identification Test (AUDIT-C)• Alcohol Full Screen: 10-item full AUDIT• Drug Screen: Single Drug Question• Readiness to Change: Readiness Ruler
EBP Model & Appraisal Methods
Substance Screening, Brief Intervention, and Referral to Treatment in Rural Primary Care
Kabrina Johnson, MS, AGNP-CKatherine Fornili, DNP, MPH, RN, CARN, FIAAN
82.3%
14.7%0.0% 2.9%
0%10%20%30%40%50%60%70%80%90%
Level I (Low risk orabstainers; AUDIT
score= 0-7)
Level II (Moderate Risk;AUDIT score=8-15)
Level III (High Risk;AUDIT score 16-20)
Level IV (Very High Risk;AUDIT score= >20)
Perc
enta
ge o
f Pat
ient
s
Level of Alcoholism Risk
Full Alcohol Use Disorders Identification Test (AUDIT) Scores
Table 1. Statistical Analysis: Relationship between Gender and Screening ResultsNote: *= Fisher’s Exact test; **= Chi Square Test; p<0.05= significant
• 290 eligible patients seen over 10 weeks• Received Pre-Screen: n=199 (68.6%) • Of all screened, most were low risk or abstainers: n=28 (82.3%)• Positive Pre-Screen: n=38 patients (19.1%)
• Brief Intervention for alcohol misuse (n=6, 15.7%) • Referral to Treatment for probable alcohol dependence (n=1, 2.6%).
• Significant gender differences among those with positive screens (Table 1)• All with a positive drug screen (n=4, 2.0 %) received a Brief Intervention• Low rates of screening may be due to short duration of implementation,
low patient census, busy clinic days, and staffing issues
Authors Study Objective Design Sample (N) Outcomes studied Results *Level and
Quality Rating
Aldridge, Linford, & Bray, 2017
To assess substance use behaviors of patient who received SBIRT services.
Pre-post comparison of outcomes within individual patients screened and recommend-ed to one of the screen-positive categories. (intention-to-treat)
Sample consisted of 17,575 randomly selected adult patients
Substance misuse data, pre- and post-SBIRT services
Statistically significant decreases for most substance use measures (p=<0.01). Patients who consumed alcohol, drank 1.8 fewer days at follow-up. Greater intervention intensity was associated with larger decreases in substance use. Brief intervention patients decreased days of drinking by 1.0, compared to 2.2 for brief therapy patients, and 4.7 for referral to treatment patients. Number of days of consuming alcohol and illicit drugs increased slightly in the brief intervention group and decreased 0.6 days in the brief therapy group (p<0.1).
II, B
Gryczynski, Mitchell, Peterson, Gonzales, Moseley, & Schwartz 2011
To assess the relationship between unhealthy substance use outcomes and service variables within SBIRT implementation.
Quasi-Experimentalnaturalistic pre–post services study
55,000 adult patients systemically screened for substance misuse, (n=1208) received SBIRT services
Administrative services record and the Government Performance and Results Act (GPRA) Questionnaire at Baseline and 6 months post intervention
Significant decrease in the participant’s frequency of illicit drug and alcohol use six months after receiving SBIRT services (p<.001 for each). Participants who received brief therapy and referral to treatment has higher reductions in alcohol use and intoxication (p<.05 for each). The number of brief intervention sessions were linked to decrease frequency of alcohol use (p<.01) and alcohol intoxication (p< .05)
IV, B
Moyer & U.S. Preventive Services Task Force, 2013
To provide recommendations on screening and behavioral interventions in primary care for alcohol misuse
Clinical Practice Guideline
RCT Trials, meta-analysis, systematic reviews
23 RCTs-Compared effects of behavioral counseling interventions with usual care.Meta-analysis and systematic reviews measures adults screening detected alcohol misuse drinking habits
Brief counseling interventions in adults with screening-detected alcohol misuse positively affect several unhealthy drinking behaviors in the primary care setting (P = 0.04)Unhealthy, risky alcohol misuse includes consuming more than 4 drinks/day or 14 drinks weekly for men and 3 drinks/day or 7 drinks weekly for women and a pattern of drinking that leads to damage to physical to mental healthProject TrEAT (N=774). Reported a statistically significant difference in hospital days in the last 6 months for the intervention group compared with the control group at 6, 12, and 48 months (35 vs. 180, 91 vs. 146, and 420 vs. 664, p<0.001, p<0.001, and p<0.05)
I,A
*Not all studies included in Evidence Table
Relationship Male Female p valueGender and Positive Drug Prescreen Results
Drug Screen PositiveDrug Screen Negative
459
0136 p=0.0094*
Gender and Alcohol Prescreen Results (AUDIT-C)Alcohol Prescreen PositiveAlcohol Prescreen Negative
2241
12124 p<0.001**
Gender and Full AUDIT Results Level I (0-7)Level II-1V (8- >20)
594
1342 p=0.061205*
Contact Information: Kabrina Johnson- [email protected] Fornili- [email protected]

Following ZapVAP implementation:• Staff met/exceeded 80% adherence 11 weeks in a row, after Week 4.• VAP rate decreased from 6:1000 VD to 0:1000 VD. • Total number of sputum cultures decreased 16%.• Positive sputum cultures decreased 30%, with a 58% decrease in the
sputum rate.• An appreciable change in sputum organism noted:
• 2018: S. aureus, K. pneumoniae, E. coli• 2019: M. catarrhalis, H. influenzae, S. aureus
An interdisciplinary, evidence-based, VAP bundle can improve care and is effective in reducing VAP rates.
• A ZERO VAP rate is attainable and best achieved by bedside interventions that prevent infection, most importantly effective oral care and standardized equipment rotation.
• Outcome findings are consistent with prior evidence that support ZapVAP as a means to improve care and patient outcomes.
• Limitations include inability to control for alternative explanations or outcomes.
• Given the low patient risk and cost/benefit analysis, ZapVAP is recommended as a feasible, high-value practice change.
This Nursing and Respiratory Therapy (RT) quality improvement project, implements ZapVAP in a 19-bed Pediatric Intensive Care Unit (PICU) in an urban, academic medical center.
• Introduction: Team Mobilization • Registered Nurses (RN), RTs, nurse assistants (NA), medicine,
pharmacy, infectious disease receive presentation of ZapVAP• Preparation: Education and Resource Mobilization
• Education competency• Post-test validation for RNs, RTs, & NAs
• 100% of bundle supplies obtained• Pre-Implementation: roll-out of one bundle component/week
• Bedside audits introduced by RN/RT champions• Ineffective oral care – algorithm developed to improve
effectiveness of oral care with tooth brushing• Full Implementation: all bundle components implemented
• Bedside, observational audits of bundle adherence tracked daily by RN/RT champions
• Real-time feedback given at bedside• RN/RT monthly lottery with prizes for ZapVAP adherence
• Bi-weekly stakeholder communication of outcomes
Lauren Manrai, BSN, RN, CCRN & Renee Franquiz, DNP, RN, CNE
Ventilator-Associated Pneumonia (VAP) is the development of pneumonia 48 hours after endotracheal intubation.
• VAP increases morbidity and mortality due to prolonged ventilator dependence that increases length of stay.
Evidence supports bundles as a means to reduce VAP • Oral care, suctioning techniques, equipment management,
positioning with head of bed elevation, and hand hygieneNational VAP benchmark is 1.8 per 1000 ventilator days (National Health and Safety Network).• Project site VAP rate in 2018, was 6 per 1000 ventilator days (VD).
BACKGROUND
RESULTS
DISCUSSION AND CONCLUSIONS
.
To develop, implement, and evaluate a VAP bundle, called ZapVAP, that improves bedside care and decreases the VAP rate.Short term goal:
• Exceed 80% adherence with ZapVAP.• Reduce the sputum rate by 50% after ZapVAP implementation.
Long term goal: • Reduce VAP rate below the National benchmark of 1.8 per 1000 VD.
PURPOSE
MEASURES
REFERENCESMETHODS
ACKNOWLEDGEMENTS
American Associated for Respiratory Care [AARC]. (2010). Endotracheal suctioning of mechanically ventilated patients with artificial airways. Respiratory Care, 55(6), 758-764. Klompas, M., Branson, R., Eichenwald, E., Greene, L., Howell, M., Lee, G., … Berenholtz, S. (2014). Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infection Control and Hospital Epidemiology, 35(8). doi:10.1086/677144McBeth, C., Montes, R., Powne, A., North, S., Natale, J. (2018). Interprofessional approach to the sustained reduction in ventilator-associated pneumonia in a pediatric intensive care unit. Critical Care Nurse, 38(6), 36-45.
ZapVAP Adherence:• Audit Tool measured adherence (one tool per bed; scored yes/no)• Adherence achieved when all ZapVAP components were met
VAP Rate:• VAP = ICD-10 VAP diagnosis tracked in 2018/2019 and used to
calculate a VAP rate. VAP Rate per 1000 VD = (VAP/VD) x 1000
Sputum Rate:• Sputum cultures (SC) tracked during pre/post intervention period
and scored positive/negative• Sputum Rate per 1000 VD = [(Positive sputum cultures that
occurred >48 hours after intubation)/VD] x 1000
Thank you: Adrian Holloway, MD, Mary Jo Simke, MS, BSN, RN, Greg Ludvik MS, RRT-NPS, Helen Felps, MSN, RN, Jennifer Arrington, MS, RN, CPN, CNL, Mary Ellen Connolly, DNP, CRNPChampions: Sarah Branigan, MSN, RN, Robby Guanzon, RRT, Sara Hartropp, BSN, RN, Melanie Hershberger BSN, RN, CCRN, Kelly Ho, BSN, RN, Kristin Lewis, BSN, RN, CCRN,Katie Martin BS, RRT-NPS, Brittany O’Branski, BS, RRT-NPS, Megan Tuma BSN, RN, Carl Wikerson, AS, CRT, & Karen Wockenfuss, RRT-ACCS
Equipment Maintenance:98.7%
FINAL ZapVAP ADHERENCE
PreZapVAP
(Sept-Dec) 2018
PostZapVAP
(Sept-Dec) 2019
Result
VentilatedPatients (N) 66 90 +36%
Total SC (N) 69 58 -16%Positive SC (N) 27 19 -30%
Positive SC>48 hours (N) 14 3 -79%
VD (N) 681 345 -50%
Sputum Rate 20.6 8.7 -58%
2018 2019VAP ICD-10 (N) 11 0
VD (N) 1830 1496VAP Rate 6 0
HOB & Positioning:98.6%
Oral Care: 95%
Hand Hygiene: 100%
Suctioning Techniques:95%
30%
48%
77%72%
83% 83%
93%
86%
79%
90%93% 94%
83%
97%
83%
0%
20%
40%
60%
80%
100%
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8 Week 9 Week 10 Week 11 Week 12 Week 13 Week 14 Week 15
PER
CEN
TAG
E
IMPLEMENTATION OVER 15 WEEKS
ZapVAP PERFORMANCE
Goal >80%
Circled items checked with daily audit

• In the United States:o Pacemakers: ~ 3 million patients o Implantable Cardioverter Defibrillators (ICD): ~300,000 patientso New CIED implantation: ~ 1 million patients yearlyo 2% of patients with CIEDs eventually undergo subsequent
surgical procedures.• Intraoperative significance to anesthesia:
• Electromagnetic interference (EMI): o Pacemaker = inhibition of pacing.o ICD = untimely delivery of anti-tachycardia therapy.
• This facility lacks a:• Clinical Practice Guideline (CPG) for anesthesia care.• Cardiology-led CIED team to interrogate the CIED and estimate
the battery life. The recommended interrogation schedule:o Pacemaker: ~ 1 year prior to surgeryo ICD: ~ 6 months prior to surgeryo Battery Life of < 3months = risk of CIED pulse generator
damage from EMI.
Problem Statement
• The purpose of this quality improvement (QI) project is to develop an evidence-based CPG for intraoperative anesthesia care of surgical patients with CIEDs.
• Short-term goal:o By October 31, 2019 all the anesthesia providers would be
educated on the approved CPG. • Long-term goal:
o By March 31, 2020, 90% of surgical patients with an implantable device will have a completed intraoperative documentation showing utilization of the approved CPG.
Purpose and Goals
Methods
Results
• PFQ: ~80% (30 out of 37) were collected post CPG presentation. Demographic data indicated: 47% CRNAs, 27% Anesthesiologist, 26% SRNAs.
• Evidence Limitations: Due to the limited amount of level 1 studies available, four Professional Societies including The American Society for Anesthesiologists, The Heart Rhythm Society, the Canadian Anesthesiologists’ Society and the Canadian Cardiovascular Society have developed the Perioperative advisories for this patient population.
• Strength: CPG was approved as policy by the chief anesthesiologist. Documentation section for CIED care already present on pre-existing electronic health record.
• Practice Implications: o This facility still lacks a Cardiology-led CIED Team
readily available for CIED interrogation for both routine and emergency surgeries.
Discussion
• The CPG created was successfully adopted by the anesthesia department as a standard of practice on January 28, 2020.
• Implementation of the approved CPG by anesthesia providers during intraoperative care will be paramount to patient safety.
• Sustainability:o A Unit Champion is essential to complete
quarterly chart audits, regular anesthesia staff interviews, track patient outcomes.
o Future QI projects should investigate the feasibility of a Cardiology-led CIED Team.
Conclusions
CPG Recommendations
• Setting: A Level II Trauma Hospital in Baltimore, Maryland. • Sample (N=37): Anesthesiologists, CRNAs, SRNAs.• CPG Development:
o Phase I: IRB Approval and Expert Panel: 2 CRNAs, 1 Anesthesiologist, and 1 Cardiac Electrophysiologist.
o Phase II: AGREE II Tool – completed by the expert panelo assess for reliability and quality of CPG.
o Phase III: Practitioner Feedback Questionnaire (PFQ)o assess for applicability of the CPG,o completed by the Anesthesia Providers during ground rounds on October 31,
2019.
Intraoperative Anesthesia Care of Patients with Cardiovascular Implantable Electronic Devices
Chioma Nwankwo, BSN, RN Faculty Advisor: Veronica Gutchell, DNP, RN, CNS, CRNP
References• Crossley, G.H., Poole, J.E., Rozner, M.A., Asirvatham, S, J., Cheng, A.,
Chung, M.K…Thompson, A. (2011). The Heart Rhythm Society (HRS)/American Society of Anesthesiologists (ASA) Expert consensus statement on the perioperative management of patients with implantable defibrillators, pacemakers and arrhythmia monitors: facilities and patient management. Heart Rhythm Society, 8(7), 1114-1154. Doi: 10.1016/j.hrthm.2010.12.023
• Gifford, J., Larimer, K., Thomas, C., & May, P. (2017). ICD-ON Registry for Perioperative Management of CIEDs: Most Require No Change. Pacing and Clinical Electrophysiology: PACE, 40(2), 128–134.https://doi.org/10.1111/pace.12990
• Intraoperative Recommendations:o Magnet available to switch CIED to asynchronous mode.o Bipolar electrocautery preferred for surgeries.o Positioning should allow for optimized surgical exposure and
CIED management.o High risk patients (surgery location within 6 inches of device):
o external pacer,o defibrillation pads attached, o arterial pressure monitoring.
CPG Recommendations
50.00%
23.30%
6.70%0%
6.70%
13.30%
0-5 years 5-10 years 10-15 years 15-20 years 20-25 years >25years
Anesthesia Staff Years of Experience
Gifford et al., 2017

Implementation of Cognitive Stimulation Therapy in Long Term Care Claire Regan, BSN, RN
Karen Yarbrough, DNP, ACNP-BC, CRNPGloria Lay, MSN, BSN, RN
University of Maryland School of Nursing
• Psychotropic medications are frequently prescribed to older adults with dementia to manage behaviors despite harmful side effects
• 40% of residents at selected facility prescribed at least one psychotropic
• Cognitive Stimulation Therapy (CST) is a non-pharmacological intervention for individuals with dementia that may improve quality of life, cognition, and reduce behaviors
Problem Statement
• Implement a CST program to:• Improve quality of life and cognition• Reduce behaviors and psychotropic drug use
• Short term goals:• 100% attendance and participation from all
enrolled residents• Barriers to attendance and participation identified
• Long-term goals:• Modest increase of 15% or maintenance of quality
of life and cognitive functioning scores• Decrease of 50% in frequency of behaviors and
psychotropic use• Achieve sustainability for program
Methods
Results
• One resident excluded due to death• Variance in attendance of sessions• Time constraints resulted in inability to incorporate
exercises during sessions• Challenges with differing auditory and cognitive ability• Evidence to show decreases in rates of depression• Most significant effects on promotion of language
function and orientation in the literature• Executive function plus extrapolation most affected in
this project• Observation of increased sustained socialization of
residents when not participating in CST
Discussion
• CST improves cognitive functioning• CST may be correlated with improving quality of life for
some residents• Additional research is needed to further investigate the
effect CST has on socialization of residents
Conclusions
Berg-Weger, M. & Stewart, D. (2017). Non-pharmacologic interventions for persons with dementia. Missouri Medicine, 114(2), 116-119.Folkerts, A., Roheger, M., Franklin, J., Middelstadt, J. & Kalbe, E. (2017). Cognitive interventions in patients with dementia living in long-term care facilities: systematic review and meta-analysis. Archives of Gerontology and Geriatrics, 73, 204-221.Spector, A., Orrell, M & Woods, B. (2010). Cognitive stimulation therapy: effects on different areas of cognitive function for people with dementia. Geriatric Psychiatry, 25, 1253-1258. Stewart, D., Berg-Weger, M., Tebb, S., Sakamoto, M., Roselle, K…& Hayden, D. (2017). Making a difference: a study of cognitive stimulation therapy for persons with dementia. Journal of Gerontological Social Work, 60(4), 300-312.
References
• 200 bed long term care facility in Baltimore City• Nine residents selected
• Mild to moderate dementia• Can participate in meaningful conversation• Prescribed a psychotropic medication
• CST sessions: twice a week , 45 minutes, 7 weeks• cognitive stimulation, reality orientation, reminiscence therapy, and
validation therapy• Weekly staff education about behavioral charting• Pre and Post Testing
• St. Louis University Mental Status Exam • Quality of Life in Alzheimer’s Disease Scale• Medication administration record audit • Behavioral chart audit
Purpose and Goals
Psychotropic Use in Selected Facility Pre Implementation Antidepressants
Antipsychotics
Anxiolytics
Sedative/Hypnotic
0
5
10
15
20
25
3026
1716
18
13
18
14
12
28
22
19
21
18
20
18
14
SLUMS Scores Pre and Post Implementation
05
101520253035404550
26
3537
20
32 31
39
46
24
35
41
26
36 36
28
46QOL Scores Pre and Post
Implementation
• Average increase in SLUMS scores of 19%• Average increase in quality of life scores of 12% for six participants and
decrease of 20% for two participants• Psychotropic medication use remained 100%
Clock Drawing Pre and Post CST Program Participation

Background
Setting & Population: CPG to be utilized by anesthesia providers when guiding perioperative anesthetic decisions. Subjects include high-risk surgical patients (identified through preoperative screening or patients with baseline cognitive dysfunction) at a hospital in Baltimore, MD specializing in orthopedic surgery. CPG Development:
• CPG recommendations synthesized from recent literature published within ten years including: meta-analysis, systemic reviews, randomized controlled trials (RCTs), and current perioperative recommendations published by the American College of Surgeons & American Geriatric Society
• CPG draft revisions based on AGREE II Tool feedback by key stakeholders• AGREE II Tool critiques the CPG for methodology of development based on
6 Domains (Figure 1)CPG Presentation & Evaluation:
• Presentation to Anesthesia Department with solicitation of Practitioner Feedback Questionnaires (PFQ)
• PFQs assess CPG for quality, acceptability, applicability, and comparative improvement to current practice (Figure 2)
Results
Anesthetic Prevention Interventions for Postoperative Cognitive Impairment
Natalie Leikus Taylor, BSN, RNUnder the Supervision of Joseph Pellegrini, PhD, CRNA, FAAN & Natasha Hopkins, DNP, CRNA
Doctor of Nursing Practice Project University of Maryland School of Nursing
Postoperative Cognitive Impairment (PCI) includes:• Postoperative Delirium (POD): An acute and fluctuating change affecting a
patients cognition and ability to concentrate. • Incidence: 50% of elderly patients after orthopedic and emergency
surgeries• Postoperative Cognitive Dysfunction (POCD): A delayed onset resulting in
changes to memory and information processing. • Incidence: 40% of elderly patients after general anesthesia
Short-term goals: Development of a Clinical Practice Guideline outlining anesthetic prevention interventions for PCI & CPG presentation to anesthesia hospital staffLong-term goal: Perioperative CPG institutional acceptance & decreased incidence of PCI at a mid-sized community hospital in Baltimore, Maryland
Intraoperative• Bispectral Index (BIS) monitoring to minimize anesthesia depth• Dexmedetomidine administration• Minimize Volatile Agents- TIVA/Regional • Avoid/Minimize Benzodiazepines• Adequate Pain Control
Postoperative• Cognitive Reorientation- presence of family members • Early return of visual and hearing aids • Maintain oxygenation and pain control • Early mobility and physical rehabilitation • Nutrition and fluid repletion
AGREE II Tool (Figure 1)• Over 88% positive feedback within 5 responses by key stakeholders across
all 6 domains demonstrates CPG quality regarding scope, content, and development
Practitioner Feedback Questionnaire (Figure 2)• 37% (n=13) of hospital anesthesia staff polled (CRNAs & Anesthesiologists)• Overall positive feedback and agreement of 70% (SD=19.1)• Strong CPG Quality (88% positive) and CPG Acceptance (73% Positive) • Mixed opinions regarding CPG Applicability: Positive Response (35%) and
Neutral Response (38%) and Negative Response (27%)
• Key stakeholders regard CPG recommendations as clinically relevant for management of HIGH-RISK patients in minimizing postoperative cognitive impairment.
• Anesthesia providers (n=13) at this Baltimore hospital demonstrate reluctance in applicability of CPG content.
• Further education may enhance anesthesia staff buy-in prior to future CPG implementation.
• Limitations:• Small sample size (n=13) provided data for PFQ analysis• Available Evidence: Limited number of RCTs have been conducted in the
operating room setting concerning benzodiazepine and narcotic usage in the elderly.
• Outcomes: Based upon quality and applicability of CPG and not quantitative clinical outcomes regarding incidence of postoperative cognitive impairment.
Problem & Purpose
Methods
CPG Recommendations
Conclusion & Limitations
ReferencesDiscussion
• American College of Surgeons & American Geriatrics Society. (2016). Optimal perioperative management of the geriatric patient: Best practices guideline from ACS NSQIP/American geriatrics society.
• American Geriatrics Society Abstracted clinical practice guideline for postoperative delirium in older adults. (2015). Journal of the American Geriatrics Society, 63(1), 142–150.
• Punjasawadwong, Y. (2018). Processed electroencephalogram and evoked potential techniques for amelioration of postoperative delirium and cognitive dysfunction following non-cardiac and non-neurosurgical procedures in adults. Cochrane Database of Systematic Reviews, (10).
• Zhou, C., Zhu, Y., Liu, Z., & Ruan, L. (2016). Effect of dexmedetomidine on postoperative cognitive dysfunction in elderly patients after general anaesthesia: A meta-analysis. The Journal Of International Medical Research, 44(6), 1182–1190.
Figure 1
Figure 2
DNP Project Goals
Consequences of Postoperative Cognitive Impairment:• Loss of independence• Increased mortality rates • Increased costs for both patients and providers
Purpose: The purpose of this DNP project was to identify evidence-based anesthetic interventions to be included in a clinical practice guideline (CPG) that outlines preoperative screening and perioperative anesthetic management of patients >65 in order to decrease the incidence of postoperative cognitive impairment.

➢ Allergen immunotherapy: (AIT, “allergy shots”)
▪ Sub-q injections in treatment (Tx) of allergies/allergic asthma▪ Tx goal: de-sensitize patient (Pt) to allergens & reduce symptoms
➢ AIT guidelines recommend:
▪ Monitoring Pt symptoms, Tx tolerance & efficacy:▪ Monthly Pt questionnaires▪ Allergist follow-up every 6 — 12 months
➢ Problem: Poor Pt follow-up during AIT → unknown Tx outcomes & potential sub-optimal care
▪ Baseline Pt data: 42.4% (n=32) overdue for follow-up (F/U)▪ Days since F/U: mean: 581, median: 261, range: 5 — 4165
Background & Problem
➢ Purpose & Long-term Goal: Improve AIT Tx safety and efficacy by
improving routine assessment and F/U utilizing a screening tool
➢ Process Measures & Short-term Goals:
1. Screening completion▪ Goal: 100% screening every 4 — 6 weeks
2. Positive screenings (indicating a need for F/U)3. Follow-up appointments scheduled (for positive screenings)
▪ Goal: 100% follow-up
Results
▪ Cox, L., Nelson, H., Lockey, R., Calabria, C., Chacko, T., Finegold, I., . . . Blessing-Moore, J. (2011). Allergen immunotherapy: A practice parameter third update. Journal of Allergy and Clinical Immunology,127(1).
▪ Cox, L., Esch, R. E., Corbett, M., Hankin, C., Nelson, M., & Plunkett, G. (2011). Allergen immunotherapy practice in the United States: Guidelines, measures, and outcomes. Annals of Allergy, Asthma & Immunology,107(4), 289-299.
▪ Lee, S., Stachler, R. J., & Ferguson, B. J. (2014). Defining quality metrics and improving safety and outcome in allergy care. International Forum of Allergy& Rhinology, 4(4), 284-291.
Improving Allergen Immunotherapy Assessmentand Follow-up Utilizing a Screening Tool
Ashley Witt, BSN, RN; Karen Scheu, DNP, FNP-BC; Elaine Y. Bundy, DNP, FNP-C
➢ Over 14 weeks:
▪ 85 Pt’s completed 204 screenings▪ Mean screenings/Pt: 2.4 ▪ Weekly screening: 0% → 86.1%
➢ Improved assessment:▪ 41.2% + screenings, identified:
▪ 35 concerns / symptoms▪ 50 overdue visits
➢ Improved follow-up:
▪ Weekly/screening F/U: 66.7%▪ Pt F/U guideline compliance:▪ 62.4% (n=53) → 98.8% (n=84)
▪ p>0.001
➢ Limitations:▪ Design:
▪ Small sample, adults only, short duration▪ Clinic documentation: electronic and paper charting
▪ Challenge for providers to review screenings▪ Improved with F/U chart review
▪ Knowledge deficits & compliance challenges ▪ Improved with education
▪ …
➢ Setting: Suburban MD asthma & allergy clinic
➢ Sample: Adult AIT patients (N=85)
➢ Interventions:
1. Monthly pre-AIT screening tool:a) Health questions:
▪ AIT concerns, side effects, reactions?▪ New medications or health changes/concerns?
b) Symptom severity questionnaires:▪ RCAT: Rhinitis Control Assessment Test▪ ACT: Asthma Control Test
c) Date of last visit:▪ Verified by clinic staff
2. Follow-up scheduling guide for staffa) Timeframe based on screening results
3. Pt & staff education4. AIT administration record revision, results trend
68%
50%40%
50%
100%
57%
100%
0%
86%100%
33% 33%
100%
80%
0%
20%
40%
60%
80%
100%
120%
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 10 11 12 13 14
% O
F SC
HEDU
LED
FOLL
OW
-UP
# O
F PA
TIEN
TS S
CHED
ULE
D
WEEK NUMBER
Process Measure 3: Follow-up Scheduled
Follow-up Scheduled Percentage of Scheduled Follow-up Median (80%) Trend Line
9.4%
58.8%
8.2%
23.5%
Process Measure 2: Positive Screenings
Multiple Factors (n = 8)
Overdue Visit (>12months) (n=50)
Health Screening Concern (n=7)
Uncontrolled Symptoms (RCAT/ACTSignificant) (n=20)
Figure 1: Process Measure 1: Rates of weekly screening completion = screenings completed (204)/patients eligible for screening (237): 86.1% screening completion, median: 100%.
Figure 3: Process Measure 3: Follow-up appointment scheduled (56)/number of positive screenings (84): 66.7% overall follow-up for each positive screening, median of 80%.
62.4%
98.8%
42.4%
1.2%
0
10
20
30
40
50
60
70
80
90
PRE POST
AIT
PATI
ENTS
F/U COMPLIANCE PRE VS. POST INTERVENTION
AIT Follow-up: Guideline Compliance
> 12 months (non-compliant)< 12 months (compliant)
Figure 4. AIT Follow-up Compliance
Pre vs. Post Intervention
0%
96%80%85%
100%
80%71%
50%36%
84%100%
82%
100% 100%
0%
20%
40%
60%
80%
100%
120%
0
10
20
30
40
50
60
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
% O
F SC
REEN
INGS
CO
MPL
ETED
# O
F SC
REEN
INGS
CO
MPL
ETED
BY
ELI
GIBL
E PT
’S
WEEK NUMBER
Process Measure 1: Screening Completion
Number of Screenings Completed Percentage of Sceening Completion Median (100%)
Project Purpose & Goals
Methods
Discussion
➢ Implications for practice:
▪ Improved AIT assessment and F/U▪ Increased guidelines knowledge & compliance▪ Ability to trend Pt screening data over Tx
➢ Future improvements:
▪ Inclusion of pediatric Pt’s ▪ Use of technology to improve screening and FU scheduling/reminders▪ Administer ACT prior to each asthma Pt injection▪ Improved safety, decreased reactions
➢ Additional clinic education, AIT quality improvement:▪ Guideline recommended: peak flow prior to AIT for asthma
Conclusion
References
Figure 2: Process Measure 2: Positive Screenings, N= 84, mean: 41.2%, median: 50%.