Disease Burden and Intensity of Antidiabetic Drug Use by Medicare Beneficiaries with Diabetes: Will...
25
Disease Burden and Intensity of Antidiabetic Drug Use by Medicare Beneficiaries with Diabetes: Will Part D Make a Difference? AcademyHealth June 25, 2006 Bruce Stuart, Thomas Shaffer, Linda Simoni-Wastila, Ilene Zuckerman The Peter Lamy Center on Drug Therapy and Aging University of Maryland Baltimore
-
Upload
matthew-roberts -
Category
Documents
-
view
213 -
download
0
Transcript of Disease Burden and Intensity of Antidiabetic Drug Use by Medicare Beneficiaries with Diabetes: Will...

Disease Burden and Intensity of Antidiabetic Drug Use by Medicare Beneficiaries with Diabetes: Will Part D Make a Difference?
AcademyHealth June 25, 2006
Bruce Stuart, Thomas Shaffer, Linda Simoni-Wastila, Ilene Zuckerman
The Peter Lamy Center on Drug Therapy and Aging University of Maryland Baltimore

Page 2The Peter Lamy Center on Drug Therapy and Aging
Outline
• Sponsor acknowledgment: funding provided by The Commonwealth Fund under grant Benchmarking the Quality of Medication Use by Medicare Beneficiaries
• Background: the growing controversy over the importance of glycemic control for frail diabetics
• Study objectives and hypotheses
• Data and study sample
• Measures
• Statistical strategy
• Results
• Discussion and study implications for policy

Page 3The Peter Lamy Center on Drug Therapy and Aging
The Importance of Glycemic Control among Frail Older Persons
Traditional diabetes guidelines
• Glycemic control is the mainstay of traditional guidelines for treatment of diabetes promulgated by the ADA, AHRQ, NCQA, AMDA, and other organizations.
• Most guidelines recognize the importance of comorbidity and frailty in making clinical treatment decisions, but offer no quantitative guidance
New thinking
• Current approaches to assessing quality of diabetes treatment do not account for heterogeneity among older patients
• Less intense targets for glycemic control are warranted for older diabetics in poor health and low life expectancy

Page 4The Peter Lamy Center on Drug Therapy and Aging
Study Objectives and Hypotheses
Objectives
• Benchmark prevalence and level of use of antidiabetic agents (oral hypoglycemic agents and insulins) among community-dwelling Medicare beneficiaries with diabetes stratified by burden of illness
• Identify factors associated with differences in antidiabetic use by burden of illness
Hypotheses
• Factors hypothesized to be associated with higher antidiabetic drug use
- Income, prescription drug coverage, severity of diabetes, obesity, health system contacts (surveillance hypothesis)
• Factors hypothesized to be associated with lower antidiabetic drug use
- Increasing disease burden, kidney disease, hospitalization, health system contacts (competing demands hypothesis)

Page 5The Peter Lamy Center on Drug Therapy and Aging
Data and Study Sample
Data
• 2002 MCBS Cost and Use files (N=12,697)
Study Sample
• Inclusion criteria:
- Self report of diabetes and/or ICD-9 diagnosis codes: 250.xx, 357.2, 362.01, 362.02, 366.41. Two or more Dx of diabetes on outpatient and carrier claims or one diagnosis on an impatient claim
• Exclusion criteria
- In MCBS facility sample all or part year, Part A and/or B part year, any Medicare HMO enrollment, incomplete surveys
• Final study sample: N=1,956

Page 6The Peter Lamy Center on Drug Therapy and Aging
Measures
Overall Burden of Illness
• Stratify study sample into 10 equal sized groups (deciles) by cumulative spending for all medical services including drugs
Dependent Variables
• Any antidiabetic drug use in 2002 by type (orals, insulin), number of prescription fills per year, total pill count for oral hypoglycemics
Explanatory Variables
• 6 domains: (1) decile assignment, (2) demographics (age, sex, race, census region), (3) economic variables (income, prescription coverage), (4) health (self-reported, ADLs, BMI, self-reported DM/no claims, diabetes complication, chronic kidney disease) (5) contacts with health system (inpatient hospital, SNF, HHA, hospice, count of physician E&M visits, count of different physicians seen in office visits), (6) denominator days

Page 7The Peter Lamy Center on Drug Therapy and Aging
Statistical Strategy
Descriptive Charts
• Prevalence rates for common comorbidities by decile of medical spending
• Prevalence and level of antidiabetic drug use by decile of medical spending
Regression Analysis
• Stepwise logistic and OLS regressions with explanatory variables entered in blocks representing the 6 domains of explanatory variables. Objective is to determine whether differences in drug use observed in the unadjusted stratification by decile lose significance with additional covariates, and if so which are responsible
Digging Deeper
• Within-decile regression analysis

Page 8The Peter Lamy Center on Drug Therapy and Aging
Descriptive Results

Page 9The Peter Lamy Center on Drug Therapy and Aging
Characteristics of the Study Population (N=1,956)
Characteristic Frequency or count (SE)
Demographics
Age (%) Under 65 65 – 69 70 – 74 75 – 79 80+
14.817.124.720.822.6
Female sex (%) 54.8
Nonwhite (%) 20.7
Geographic residence (%) East Midwest South West
18.525.643.312.6

Page 10The Peter Lamy Center on Drug Therapy and Aging
Characteristics of the Study Population (N=1,956)
Economic variables
Annual income (%) < $10,000 $10,000 – 20,000 $20,001 – 30,000 >$30,000
25.131.421.522.0
Supplementary medical insurance No coverage (%) Full year (%) Part year (%) Covered months (count)
8.588.03.5
6.4 (0.5)
Prescription drug coverage No coverage (%) Full year (%) Part year (%) Covered months (count)
25.065.19.9
6.0 (0.2)

Page 11The Peter Lamy Center on Drug Therapy and Aging
Characteristics of the Study Population (N=1,956)
Health status and disease severity factors
Self-reported health (%) Poor Fair Good to excellent
13.028.757.6
3 or more activity limitations (ADLs) (%) 5.5
BMI >= 30 (%) 39.1
Self reported diabetes/no claim diagnosis (%) 10.5
Diabetes complication (ICD-9 250.1 – 250.9) (%)
52.5
Chronic kidney disease (ICD-9 ) (%) 7.1
Died (%) 4.6
Denominator days* (count) 353.3

Page 12The Peter Lamy Center on Drug Therapy and Aging
Characteristics of the Study Population (N=1,956)
Health system contact variables
Any hospital admission (%) 27.8
Any SNF stay (%) 4.3
Any home health visit (%) 11.4
Any hospice stay (%) 1.2
Number of office visits for evaluation and management
(E&M) (count)
9.1
Number of different physicians seen for E&M visits (count)
4.8

Page 13The Peter Lamy Center on Drug Therapy and Aging
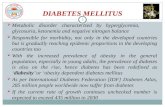
Figure 1. Prevalence of Selected Diseases among Medicare Beneficiaries with Diabetes Stratified by Decile of Annual Medical Spending, 2002
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
1 2 3 4 5 6 7 8 9 10
Spending Decile
Prev
alen
ce (%
)
Ischemic Heart Disease Cancer COPD/Asthma
Stroke Arthritis/non-traumatic joint disorders Dementia incl Alzheimer's
Pneumonia Peptic ulcer/dyspepsia Depression/other mood disorders

Page 14The Peter Lamy Center on Drug Therapy and Aging
Disease Burden and Medication Use: the Inverted “U”

Page 15The Peter Lamy Center on Drug Therapy and Aging
Figure 2. Unadjusted Annual Prevalence of Antidiabetic Medication Use by Decile of Annual Medical Spending
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
1 2 3 4 5 6 7 8 9 10Decile
Per
cen
tag
e o
f D
iab
etic
s
% using any antidiabetic medication % using oral antidibetic medications % using insulin

Page 16The Peter Lamy Center on Drug Therapy and Aging
Figure 3. Unadjusted Mean Annual Prescription Fills for Oral Antidiabetic Medications by Users of These Drugs
0.0
2.0
4.0
6.0
8.0
10.0
12.0
1 2 3 4 5 6 7 8 9 10
Spending Decile
Mea
n #
of F
ills

Page 17The Peter Lamy Center on Drug Therapy and Aging
Figure 4. Unadjusted Mean Annual Pill Counts for Oral Antidiabetic Medications Stratified by Users of These Drugs
0.0
100.0
200.0
300.0
400.0
500.0
600.0
700.0
800.0
1 2 3 4 5 6 7 8 9 10
Spending Decile
Mea
n N
um
ber
of
Pill
s

Page 18The Peter Lamy Center on Drug Therapy and Aging
Multivariate Results

Page 19The Peter Lamy Center on Drug Therapy and Aging
Adjusted Odds Ratios for Any Use of Antidiabetic Medications by Study Subjects
Decile Decile Only RegressionUnadj. Odds (95% CI)
Full ModelAdj. Odds (95% CI)
1 2 3 4 5 6 7 (reference) 8 9 10
0.40 (0.26-0.60)**0.61 (0.40-0.91)*0.79 (0.52-1.20)0.82 (0.54-1.24)
0.64 (0.42-0.97)*0.87 (0.57-1.33)
1.000.81 (0.53-1.23)0.83 (0.55-1.27)
0.53 (0.36-0.81)**
0.56 (0.34-0.91)*0.71 (0.45-1.13)0.81 (0.51-1.28)0.87 (0.56-1.37)0.66 (0.42-1.03)0.80 (0.51-1.24)
1.000.79 (0.50-1.25)0.83 (0.52-1.35)0.69 (0.41-1.16)
*p <.05
**p <.01

Page 20The Peter Lamy Center on Drug Therapy and Aging
Factors Affecting Treatment Odds (or not)
• None of the demographic or economic factors was a consistent predictor of likelihood of using antidiabetic medicine. Prescription coverage plays no significant role.
• Significant (p <.01) health and diabetes severity indicators (range of odds ratios in models 5 and 6): BMI >=30 (1.51 to 1.53), self reported diabetes/no claim (0.20), diabetes complications (1.75 to 1.80), chronic kidney disease (0.55)
• Only one significant (p <.05) health system contact variables (odds ratios in model 6): number of different physician seen in office visits (0.95)
• The adjusted treatment odds in the full model are 16 points higher in each tail of the distribution, but the inverted “U” pattern remains
•

Page 21The Peter Lamy Center on Drug Therapy and Aging
Adjusted Coefficients for Annual Prescription Fills for Study Subjects
Using Oral Antidiabetic Medications
Decile Decile Only RegressionUnadj. Coef. (95% CI)
Full ModelAdj. Coef. (95% CI)
1 2 3 4 5 6 7 (reference) 8 9 10
-3.79 (-5.30; -2.28)**-2.30 (-3.74; -0.86)**
-0.60 (-2.20; 1.00)-0.78 (-2.37; 0.80)-0.99 (-2.66; 0.69)-0.32 (-1.98; 1.33)
0.00-1.30 (-2.95; 0.35)-1.11 (-2.81; 0.59)
-2.77 (-4.36; -1.19)**
-4.37 (-6.07; -2.67)**-3.05 (-4.67; -1.43)**
-1.32 (-3.01; 0.38)-1.58 (-3.27; 0.12)-1.60 (-3.32; 0.13)-0.94 (-2.59; 0.72)
0.00-0.71 (-2.39; 0.98)0.43 (-1.43; 2.30)-0.38 (-2.26; 1.50)
*p <.05
**p <.01

Page 22The Peter Lamy Center on Drug Therapy and Aging
Factors Affecting Oral Hypoglycemic Treatment Levels (or not)
• Full year prescription coverage has a small effect in increasing antidiabetic drug use in models 4 and 5, but loses significance in the full model 6. Lower incomes are associated with higher drug use but the effect is small and not consistently significant
• Significant (p <.05) health and diabetes severity indicators (range of coefficients in models 5 and 6): BMI >=30 (0.90 to 0.93), self reported diabetes/no claim (-1.49 to -1.80), hospitalization (-2.37)
• Only two significant health system contact variables in model 6: any hospitalization (-2.37; p<.01), and number of different physicians seen in office visits (0.02; p <.05)
• Covariate control essentially eliminates the upper tail in the inverted “U” for level of antidiabetic drug use, but unexplained variance in the lower tail increases significantly

Page 23The Peter Lamy Center on Drug Therapy and Aging
Discussion: Main Points
High level of heterogeneity in antidiabetic drug use • Almost 1 in 4 Medicare beneficiaries with diabetes took no antidiabetic drugs
in 2002• All 6 variable domains combined could explain only a small fraction of the
likelihood and level of antidiabetic use among beneficiaries
The inverted “U” pattern in medication intensity by disease burden• Increasing disease burden is associated with a sharp rise in antidiabetic
medication intensity among the least sick, plateaus, and then falls sharply among those with the greatest disease burden
• Study limitations• No measure of blood glucose levels• Cross-sectional design precludes causal inferences

Page 24The Peter Lamy Center on Drug Therapy and Aging
Conclusions: Implications for Part D
Drug coverage makes no significant difference in antidiabetic drug use
Quality of care and the medication intensity curve• All three zones in the inverted “U” have potential clinical significance but
require additional study- Does the low level of antidiabetic use among diabetics with the least disease
burden reflect lack of need or underuse?
- Does the plateau in prevalence and level of antidiabetic use among those in the middle of the range of disease burden represent a meaningful target for improving the quality of diabetic treatment in the Medicare program?
- Is the sharp drop in medication use in the upper tail of the distribution of disease burden justified by new thinking about the need for glycemic control among frail older people or does it represent underuse?

Thank You!