Direct invasion of the transverse colon by a cecal tumor
3
Abdom Imaging 18:20-22 (1993) Abdominal Imaging Springer-Verlag NewYorkInc. 1993 Direct Invasion of the Transverse Colon by a Cecal Tumor Philip Goodman and Suppiah Balachandran Department of Radiology, University of Texas Medical Branch, Galveston, Texas, USA Abstract. Direct invasion of the transverse colon is known to result from noncontiguous primary tumors spreading along ligamentous attachments or from di- rect extension of metastatic disease involving the greater omentum. The resultant desmoplastic reac- tion produces characteristic findings on barium en- ema. However, to our knowledge, these findings have not been reported to result from extension of a cecal tumor to the transverse colon via the perico- lonic fat. We present such a case and discuss the radiographic findings. Key words: Colon, neoplasms- Barium enema- Computed tomography. Barium enema showed a large irregular annular lesion in the cecum and proximal ascending colon. A persistent focal area of nodularity and tethered folds was also seen along the inferior aspect of the redundant right transverse colon medial to the cecal mass (Fig. 1). Abdominal computed tomography (CT) demon- strated extension of the cecal mass to the right transverse colon via the pericolonic fat (Fig. 2). A subtotal colectomy and ileosigmoid anastomosis were then performed. Pathologic examination of the resected colon revealed matting together of the cecum and right transverse colon. A 9-cm fungating, partially necrotic cecal tumor infiltrated the adjacent pericolonic fat and extended into the wall and mucosa of the adherent transverse colon. Histologically, the mass represented a combined well-differentiated adenocarcinoma and carcinoid tu- mor, with the carcinoid component predominating. No interven- ing normal tissue was present within the mass to suggest a multi- focal origin. Of 20 pericolonic lymph nodes resected, none contained tumor. Barium enema is a useful method for detecting direct neoplastic invasion of the transverse colon. Charac- teristic findings of tethered or spiculated folds, nod- ularity, and luminal distortion may result from ex- tension of pancreatic or gastric carcinoma along tiga- mentous attachments or from direct extension of metastatic disease involving the greater omentum [1-3]. We present a patient in whom similar findings on barium enema resulted from direct invasion of the transverse colon by a large cecal tumor. Case Report A 51-year-old woman complained of right lower quadrant pain, shortness of breath, and an enlarging right lower quadrant mass. She had undergone a hysterectomy and appendectomy 16 years previously. Physical examination demonstrated a 7-cm right lower quadrant mass, and rectal examination revealed guaiac- negative stool. Hemoglobin was 3.6 g/dl and hematocrit was 12.6%. Address offprint requests to: Philip Goodman, M.D., Department of Radiology, University of Texas Medical Branch, Galveston, TX 77555-0709, USA Discussion Direct invasion of the transverse colon from non- contiguous primary tumors has been well described on barium enema examinations. Pancreatic carci- noma may spread directly along the transverse mesocolon to involve the inferior wall between the taenia mesocolica and the taenia libera. Similarly, gastric carcinoma may spread via the gastrocolic lig- ament to involve the superior wall between the taenia mesocolica and the taenia omentalis. Invasion of the transverse colon by pancreatic or gastric car- cinoma produces a desmoplastic reaction. This can cause various findings on barium enema study in- cluding tethered folds, nodularity, and luminal dis- tortion or fixation. Involvement is typically eccen- tric, but in advanced disease may appear circumferential [1-31. Similar findings have been reported in direct in- vasion of the transverse colon from tumors which have metastasized to the greater omentum. The greater omentum, whose superior portion forms the gastrocolic ligament, attaches to the transverse co-
-
Upload
philip-goodman -
Category
Documents
-
view
224 -
download
0
Transcript of Direct invasion of the transverse colon by a cecal tumor

Abdom Imaging 18:20-22 (1993)
Abdominal Imaging
�9 Springer-Verlag New York Inc. 1993
Direct Invasion of the Transverse Colon by a Cecal Tumor
Philip Goodman and Suppiah Balachandran Department of Radiology, University of Texas Medical Branch, Galveston, Texas, USA
Abstract. Direct invasion of the transverse colon is known to result from noncontiguous primary tumors spreading along ligamentous attachments or from di- rect extension of metastatic disease involving the greater omentum. The resultant desmoplastic reac- tion produces characteristic findings on barium en- ema. However, to our knowledge, these findings have not been reported to result from extension of a cecal tumor to the transverse colon via the perico- lonic fat. We present such a case and discuss the radiographic findings.
Key words: Colon, neop lasms- Barium e n e m a - Computed tomography.
Barium enema showed a large irregular annular lesion in the cecum and proximal ascending colon. A persistent focal area of nodularity and tethered folds was also seen along the inferior aspect of the redundant right transverse colon medial to the cecal mass (Fig. 1). Abdominal computed tomography (CT) demon- strated extension of the cecal mass to the right transverse colon via the pericolonic fat (Fig. 2).
A subtotal colectomy and ileosigmoid anastomosis were then performed. Pathologic examination of the resected colon revealed matting together of the cecum and right transverse colon. A 9-cm fungating, partially necrotic cecal tumor infiltrated the adjacent pericolonic fat and extended into the wall and mucosa of the adherent transverse colon. Histologically, the mass represented a combined well-differentiated adenocarcinoma and carcinoid tu- mor, with the carcinoid component predominating. No interven- ing normal tissue was present within the mass to suggest a multi- focal origin. Of 20 pericolonic lymph nodes resected, none contained tumor.
Barium enema is a useful method for detecting direct neoplastic invasion of the transverse colon. Charac- teristic findings of tethered or spiculated folds, nod- ularity, and luminal distortion may result from ex- tension of pancreatic or gastric carcinoma along tiga- mentous attachments or from direct extension of metastatic disease involving the greater omentum [1-3]. We present a patient in whom similar findings on barium enema resulted from direct invasion of the transverse colon by a large cecal tumor.
Case Report
A 51-year-old woman complained of right lower quadrant pain, shortness of breath, and an enlarging right lower quadrant mass. She had undergone a hysterectomy and appendectomy 16 years previously. Physical examination demonstrated a 7-cm right lower quadrant mass, and rectal examination revealed guaiac- negative stool. Hemoglobin was 3.6 g/dl and hematocrit was 12.6%.
Address offprint requests to: Philip Goodman, M.D., Department of Radiology, University of Texas Medical Branch, Galveston, TX 77555-0709, USA
Discussion
Direct invasion of the transverse colon from non- contiguous primary tumors has been well described on barium enema examinations. Pancreatic carci- noma may spread directly along the transverse mesocolon to involve the inferior wall between the taenia mesocolica and the taenia libera. Similarly, gastric carcinoma may spread via the gastrocolic lig- ament to involve the superior wall between the taenia mesocolica and the taenia omentalis. Invasion of the transverse colon by pancreatic or gastric car- cinoma produces a desmoplastic reaction. This can cause various findings on barium enema study in- cluding tethered folds, nodularity, and luminal dis- tortion or fixation. Involvement is typically eccen- tric, but in advanced disease may appear circumferential [1-31.
Similar findings have been reported in direct in- vasion of the transverse colon from tumors which have metastasized to the greater omentum. The greater omentum, whose superior portion forms the gastrocolic ligament, attaches to the transverse co-

P, Goodman and S. Balachandran: Tumor Invasion of the Transverse Colon 21
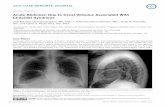
Fig. 1. A Barium enema shows a large annular cecal mass (curved arrow). Tethered folds and spiculation are seen along the inferior wall of the right trans- verse colon (open arrows). B An oblique film demonstrates nodu- larity along the inferior wall of the transverse colon (open ar- lOWS).
Fig. 2. A Pelvic CT scan shows a large soft tissue density mass (M) extending from the cecum (C) to the right transverse colon (T). B Inferiorly, the cecal mass (M) is separated from the nor- mal mid-transverse colon (T) by pericolonic fat (curved arrow).
lon anteriorly. Peritoneal spread of tumor commonly involves the gastrocolic ligament, as well as the more inferior portion of the greater omentum. Direct extension of tumor from the greater omentum to the transverse colon produces a desmoplastic reaction which in one published series involved primarily the superior wall and in another series primarily the in- ferior wall [2, 3]. The findings on barium enema are similar to those seen in invasive pancreatic or gastric carcinoma, and likewise usually appear eccentric,
although concentric lesions may be noted in ad- vanced cases [2, 3].
To our knowledge, direct invasion of the trans- verse colon by an adjacent cecal tumor has not been reported, despite the frequency of pericolonie spread of cecal carcinoma seen on CT [4-7]. In our patient, barium enema showed a desmoplastic reac- tion involving the inferior wall of the transverse co- lon adjacent to a large annular cecal mass. The ap- pearance of the transverse colon lesion is indistinguishable from that caused by direct exten- sion of either pancreatic carcinoma or some cases of omental metastases.
The direct neoplastic invasion of the transverse colon seen in our patient is easily differentiated from a synchronous primary carcinoma arising in the transverse colon. Since desmoplastic reaction results from infiltration of the serosal layer of the bowel wall, findings on barium enema reflect mainly serosal involvement. In contrast, synchronous le- sions, which occur in approximately 3.5-5.5% of cases of colonic carcinoma [8-101, demonstrate mu- cosal abnormalities, such as ulceration, polypoid mass, or annular narrowing. The relationship of the transverse colon lesion to the cecal mass in our pa- tient is further supported by CT which demonstrated direct extension of tumor across the pericolonic fat and by histological examination which revealed no intervening normal tissue between the areas of co- lonic involvement [10].
The large size of the cecal mass and its proximity to the redundant transverse colon presumably al- lowed the tumor to extend through the pericolonic fat to reach the transverse colon. This unusual route of spread should be considered in the differential diagnosis of direct neoplastic invasion of the trans- verse colon.

22 P. Goodman and S. Balachandran: Tumor Invasion of the Transverse Colon
References 1. Meyers M. Intraperitoneal spread of malignancies and its ef-
fect on the bowel. Clin Radiol 1981;32:129-146 2. Rubesin SE, Levine MS. Omental cakes: colonic involvement
by omental metastases. Radiology 1985;154:593-596 3. Krestin GP, Beyer D, Lorenz R. Secondary involvement of
the transverse colon by tumors of the pelvis: spread of malig- nancies along the greater omentum. Gastrointest Radiol 1985;10:283-288
4. Solomon A, Bar-Ziv J, Stern D. Staging cecal and ascending colon carcinoma with computed tomography. Gastrointest Radiol 1988; 13:152-154
5. Keeney G, Jafri ZH, Mezwa DG. Computed tomographic evaluation and staging of cecal carcinoma. Gastrointest Ra- diol 1989;14:65-69
6. Balthazar E J, Megibow AJ, Hulnick D, Naidich DP. Carci- noma of the colon: detection and preoperative staging by CT. A JR 1988;150:301-306
7. Thoeni RF. CT evaluation of carcinomas of the colon and rectum. Radiol Clin North Am 1989;27:731-741
8. Abrams JS, Reines HD. Increasing incidence of right-sided lesions in colorectal cancer. Am J Surg 1979;137:522-526
9. Heald RJ, Bussey HJR. Clinical experiences at St. Mark's Hospital with multiple synchronous cancers of the colon and rectum. Dis Colon Rectum 1975;18:6-10
10. Fischel RE, Dermer R. Multifocal carcinoma of the large in- testine. Clin Radiol 1975;26:495-498
Received: April 6, 1992; accepted: May 13, 1992