Dilator for high rectal strictures
1
Survival in malignant jaundice: P. Gillen and A. L. G. Peel Gudjonssen B, Livistone E, Spiro H. Cancer of the pancreas: diagnostic accuracy and survival statistics. Cancer 1978; 42 2494506. Peel ALG, Dillon E, Dellipiani AW. High bile duct cancer: incidence and pattern of investigation in the general hospital setting. Br J Surg 1981; 68: 459-62. Eyre-Brook IA, Ross B, Johnson AG. Should surgeons operate on the evidence of ultrasound alone in jaundiced patients? Br J Surg 12. 13. 14. 1983; 70 587-9. 8. Dixon JM, Armstrong CP, Duffy S, Davies GC. Statistical analysis of the factors affecting mortality and morbidity in biliary tract surgery. Gut 1983; 24: 845-52. Anderson JB, Cooper MJ, Williamson RCN. Adenocarcinoma of the extra-hepatic biliary tree. Ann R Coll Surg Engl 1985; 67: 13943. Blamey SL, Fearon KCH, Gilmour WH, Osborne DH, Carter DC. Prediction of risk in biliary surgery. Br J Surg 1983; 70 11. Feduska NJ, Dent T, Lindeneur SM. Results of palliative operations for carcinoma of the pancreas. Arch Surg 1971; 103: 330-4. 9. 10. 5 35--8. Surgical workshop Paper accepted 18 February 1986 Br. J. Surg. 1986, Vol. 73, August, 633 Dilator for high rectal strictures Kathryn Hood and A. Lewis The Royal Free Hosplal, London, UK Correspondence to: Mr A. Lewis, Royal Free Hospital, Pond Street, London NW32QG, UK Dilators, such as a straight Hegar’s instrument or a flexible bougie, have been employed successfully in the treatment of low rectal strictures for many years’.’. No satisfactory dilator is available to deal with strictures at the level of the sacral prominence, which are typically due to anastomotic dehiscence following anterior resection3. These strictures are difficult to dilate with a straight instrument, whether rigid or flexible, because the curvature of the sacrum causes the stricture to lie at an approximate right-angle to the line of the lower rectum (Figure I). For several years, a curved ended metal dilator modelled on the Lister urethral dilator has been used in the management of these high strictures. Six sizes have been made (5,9,13,16,18and 21 mm) the largest being of sufficient diameter to allow the subsequent passage of a small Lloyd-Davies sigmoidoscope (Figure 2). The patient is given a saline rectal washout before surgery, and prophylactic metronidazole and cefotaxime are administered peroperatively, and for 24 h postoperatively. Gram-negative septicaemia has occurred on two occasions when antibiotics were omitted. Under general anaesthesia, the patient is placed in the lithotomy position, and the lubricated dilators are passed through the stricture. If this is at a right angle to thc rectum, the tip of the dilator can be rotated accordingly, but this manoeuvre must be precisely reversed on withdrawal, as the curved tip will otherwise prevent removal of the instrument. Postoperatively, immediate relief of obstructive symptoms occurs. The procedure may need repeating at 2-3 monthly intervals for up to 1 year before an adequate lumen is maintained, but is much preferred to further abdominal surgery which, despite the use of stapling methods4 is usually difficult. The instrument is available from: ISB Surgical Limited, 140 Arkwrights, Harlow, Essex CM2 3L2, UK. References 1. 2. Miles RPM. Benign strictures of the rectum. Ann R Coll Surg Engl Hartmann H. An addresson inflammatorystrktures of the rectum. Lancet 1922; i: 307-10. 1972; 50 310-11. Figure 1 place Diagrammatic cross-section of the pelvis, showing dilator in Figure 2 The dilator, size range 5-21 mm 3. Cade D, Gallagher P, Schofield PF, Turner L. Complication of anterior resection of the rectum using the EEA staplingdevice. BrJ Surg 1981; 68 33940. 4. McLean Ross AH. Rectal stricture resection using EEA autostapler. Br J Surg 1980 67: 281-2. Paper accepted 15 January 1986 Br. J. Surg., Vol. 73, NO. 8. August 1986 633
-
Upload
kathryn-hood -
Category
Documents
-
view
213 -
download
1
Transcript of Dilator for high rectal strictures

Survival in malignant jaundice: P. Gillen and A. L. G. Peel
Gudjonssen B, Livistone E, Spiro H. Cancer of the pancreas: diagnostic accuracy and survival statistics. Cancer 1978; 42 2494506. Peel ALG, Dillon E, Dellipiani AW. High bile duct cancer: incidence and pattern of investigation in the general hospital setting. Br J Surg 1981; 68: 459-62. Eyre-Brook IA, Ross B, Johnson AG. Should surgeons operate on the evidence of ultrasound alone in jaundiced patients? Br J Surg
12.
13.
14.
1983; 7 0 587-9.
8. Dixon JM, Armstrong CP, Duffy S, Davies GC. Statistical analysis of the factors affecting mortality and morbidity in biliary tract surgery. Gut 1983; 24: 845-52. Anderson JB, Cooper MJ, Williamson RCN. Adenocarcinoma of the extra-hepatic biliary tree. Ann R Coll Surg Engl 1985; 67: 13943. Blamey SL, Fearon KCH, Gilmour WH, Osborne DH, Carter DC. Prediction of risk in biliary surgery. Br J Surg 1983; 7 0
11. Feduska NJ, Dent T, Lindeneur SM. Results of palliative operations for carcinoma of the pancreas. Arch Surg 1971; 103: 330-4.
9.
10.
5 3 5--8.
Surgical workshop
Paper accepted 18 February 1986
Br. J. Surg. 1986, Vol. 73, August, 633
Dilator for high rectal strictures
Kathryn Hood and A. Lewis
The Royal Free Hosplal, London, UK Correspondence to: Mr A. Lewis, Royal Free Hospital, Pond Street, London NW32QG, UK
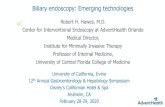
Dilators, such as a straight Hegar’s instrument or a flexible bougie, have been employed successfully in the treatment of low rectal strictures for many years’.’. No satisfactory dilator is available to deal with strictures at the level of the sacral prominence, which are typically due to anastomotic dehiscence following anterior resection3. These strictures are difficult to dilate with a straight instrument, whether rigid or flexible, because the curvature of the sacrum causes the stricture to lie at an approximate right-angle to the line of the lower rectum (Figure I ) .
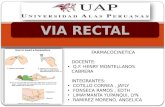
For several years, a curved ended metal dilator modelled on the Lister urethral dilator has been used in the management of these high strictures. Six sizes have been made (5,9,13,16,18 and 21 mm) the largest being of sufficient diameter to allow the subsequent passage of a small Lloyd-Davies sigmoidoscope (Figure 2).
The patient is given a saline rectal washout before surgery, and prophylactic metronidazole and cefotaxime are administered peroperatively, and for 24 h postoperatively. Gram-negative septicaemia has occurred on two occasions when antibiotics were omitted. Under general anaesthesia, the patient is placed in the lithotomy position, and the lubricated dilators are passed through the stricture. If this is at a right angle to thc rectum, the tip of the dilator can be rotated accordingly, but this manoeuvre must be precisely reversed on withdrawal, as the curved tip will otherwise prevent removal of the instrument.
Postoperatively, immediate relief of obstructive symptoms occurs. The procedure may need repeating at 2-3 monthly intervals for up to 1 year before an adequate lumen is maintained, but is much preferred to further abdominal surgery which, despite the use of stapling methods4 is usually difficult.
The instrument is available from: ISB Surgical Limited, 140 Arkwrights, Harlow, Essex CM2 3L2, UK.
References 1.
2.
Miles RPM. Benign strictures of the rectum. Ann R Coll Surg Engl
Hartmann H. An addresson inflammatorystrktures of the rectum. Lancet 1922; i: 307-10.
1972; 5 0 310-11.
Figure 1 place
Diagrammatic cross-section of the pelvis, showing dilator in
Figure 2 The dilator, size range 5-21 mm
3. Cade D, Gallagher P, Schofield PF, Turner L. Complication of anterior resection of the rectum using the EEA staplingdevice. BrJ Surg 1981; 6 8 33940.
4. McLean Ross AH. Rectal stricture resection using EEA autostapler. Br J Surg 1980 67: 281-2.
Paper accepted 15 January 1986
Br. J. Surg., Vol. 73, NO. 8. August 1986 633