
Diktyoma*
7
NOTES, CASES, INSTRUMENTS DIKTYOMA* (EMBRYONAL MEDULLO-EPITHELIOMA) REVIEW OF THE LITERATURE AND REPORT OF A CASE SADÎ DE BUEN, M.D. AND AMADOR GONZÂLEZ-ANGULO, M.D. Mexico, D.F., Mexico The malignant tumors which originate in the ciliary portion of the retina (pars ciliaris retinae) are rare. There are two forms, the adult medullo-epithelioma which develops in adult people and the embryonal medullo- epithelioma, or diktyoma, which occurs in young individuals. In addition, benign growths have been described arising in the ciliary epithelium, such as the benign epithelioma of Fuchs, 11 which is an epithelial hyperplasia appearing in senile eyes affected with chronic inflam- mation, 36 and the adenoma of the ciliary body 20 · 35 , also quoted by Grinker. 13 Fuchs 11 and Nordmann 18 have extensively described these tumors. The former in 1908, described four cases of a tumor which he called "diktyoma" (from Greek, diktyos = net), due to the peculiar arrangement of cells forming netlike structures. Verhoeff 34 sug- gested, in 1904, the name of teratoneuroma because he found structures of nerve origin within the tumor. Medullo-epithelioma is the best name to express the origin 8 · 11 · 20 of this tumor. Few diktyoma cases have been published in the literature and according to Reese 20 there are less than 80. Some of the published cases are listed in Table 1. Andersen in a review of the literature * From the Service of Ophthalmology, General Hospital, Mexico City and the Pathology Unit of the University of Mexico in the General Hospital, Mexico City. found 22 cases, among which seven were considered to be doubtful. 1 In addition, we know of three more cases, reported to the Ophthalmic Pathology Club in Washington, D.C., by Wadsworth, Chris- tensen, and Rones, 22 in 1951, 1955, and 1956 respectively. To these may still be added an- other recent case studied by Christensen 5 in 1958. Diktyoma is a tumor which arises from the undifferentiated neuroectoderm of the primary optic vesicle. Because of its slow growing and slightly invasive power, the correct diagnosis is usually not established until after the eyeball is enucleated and the microscopic study of the specimen is per- formed. Usually, the clinical diagnosis is ret- inoblastoma or pseudoglioma of the retina. 34 The purpose of this paper it to report a case of diktyoma (embryonal medullo-epithe- lioma) which showed a great invasive power. REPORT OF CASE J. P. A., a 13-year-old boy, at two years of age had whitish spots in his left eye with impairment of vision. When he was 11 years of age, the eye suffered traumatic rupture and subsequently was enucleated. Since that time a tumorlike tissue was noticed growing within the orbit. The tumor mass enlarged to 10 by 6.0 cm. during two years, and by that time the patient was admitted to the Service of Ophthalmology of the General Hospital in Mexico City. The intraorbital tumor was firm, warm, and adherent to deeper tissue. Laboratory examinations and X-ray films of the thorax were negative. X-ray films of the skull showed persistence of the metopic suture with sepa- ration of the edges and deformity of the left orbit, all due to an oval tumorlike tissue, and invasion of the maxillary antrum and surrounding tissues. Ten days after admission, on September 26, 1957, a biopsy of the tumor was taken and the micro- scopic study revealed that the tumor cells were ar- ranged in several rows as is found in the embryonic retina when differentiation of nuclei in individual layers has not yet occurred. The cells borders were perceptible, the nuclei were elongated, rounded, and deeply basophilic. Tumor cells formed solid masses or were arranged in cords which surrounded a cen- tral blood vessel. The stroma was scanty (fig. Γ). Occasionally the cells formed cavities, which were concave on one side and convex on the other side. The concave side which invaginates toward the 606
Transcript of Diktyoma*
NOTES, CASES, INSTRUMENTS DIKTYOMA*
(EMBRYONAL MEDULLO-EPITHELIOMA)
REVIEW OF THE LITERATURE AND REPORT OF A CASE
SADÎ D E BUEN, M.D.
AND
AMADOR GONZÂLEZ-ANGULO, M.D. Mexico, D.F., Mexico
The malignant tumors which originate in the ciliary portion of the retina (pars ciliaris retinae) are rare. There are two forms, the adult medullo-epithelioma which develops in adult people and the embryonal medullo-epithelioma, or diktyoma, which occurs in young individuals.
In addition, benign growths have been described arising in the ciliary epithelium, such as the benign epithelioma of Fuchs,11
which is an epithelial hyperplasia appearing in senile eyes affected with chronic inflammation,36 and the adenoma of the ciliary body20·35, also quoted by Grinker.13
Fuchs11 and Nordmann18 have extensively described these tumors. The former in 1908, described four cases of a tumor which he called "diktyoma" (from Greek, diktyos = net), due to the peculiar arrangement of cells forming netlike structures. Verhoeff34 suggested, in 1904, the name of teratoneuroma because he found structures of nerve origin within the tumor.
Medullo-epithelioma is the best name to express the origin8·11·20 of this tumor. Few diktyoma cases have been published in the literature and according to Reese20 there are less than 80. Some of the published cases are listed in Table 1.
Andersen in a review of the literature
* From the Service of Ophthalmology, General Hospital, Mexico City and the Pathology Unit of the University of Mexico in the General Hospital, Mexico City.
found 22 cases, among which seven were considered to be doubtful.1
In addition, we know of three more cases, reported to the Ophthalmic Pathology Club in Washington, D.C., by Wadsworth, Chris-tensen, and Rones,22 in 1951, 1955, and 1956 respectively. To these may still be added another recent case studied by Christensen5 in 1958.
Diktyoma is a tumor which arises from the undifferentiated neuroectoderm of the primary optic vesicle. Because of its slow growing and slightly invasive power, the correct diagnosis is usually not established until after the eyeball is enucleated and the microscopic study of the specimen is performed. Usually, the clinical diagnosis is ret-inoblastoma or pseudoglioma of the retina.34
The purpose of this paper it to report a case of diktyoma (embryonal medullo-epithelioma) which showed a great invasive power.
REPORT OF CASE
J. P. A., a 13-year-old boy, at two years of age had whitish spots in his left eye with impairment of vision. When he was 11 years of age, the eye suffered traumatic rupture and subsequently was enucleated. Since that time a tumorlike tissue was noticed growing within the orbit. The tumor mass enlarged to 10 by 6.0 cm. during two years, and by that time the patient was admitted to the Service of Ophthalmology of the General Hospital in Mexico City. The intraorbital tumor was firm, warm, and adherent to deeper tissue.
Laboratory examinations and X-ray films of the thorax were negative. X-ray films of the skull showed persistence of the metopic suture with separation of the edges and deformity of the left orbit, all due to an oval tumorlike tissue, and invasion of the maxillary antrum and surrounding tissues.
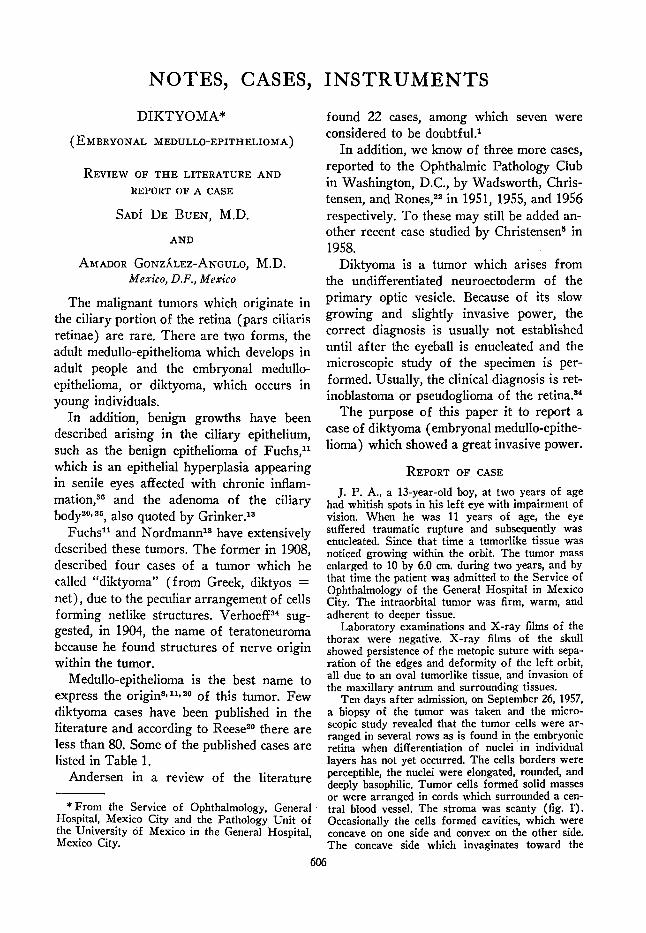
Ten days after admission, on September 26, 1957, a biopsy of the tumor was taken and the microscopic study revealed that the tumor cells were arranged in several rows as is found in the embryonic retina when differentiation of nuclei in individual layers has not yet occurred. The cells borders were perceptible, the nuclei were elongated, rounded, and deeply basophilic. Tumor cells formed solid masses or were arranged in cords which surrounded a central blood vessel. The stroma was scanty (fig. Γ). Occasionally the cells formed cavities, which were concave on one side and convex on the other side. The concave side which invaginates toward the
606
NOTES, CASES, INSTRUMENTS 607
TABLE 1 SOME OF THE PUBLISHED CASES OF DIKTYOMA
Author
Badal and Lagrange3
Emanuel9
Verhoeff34
Kuthe and Ginsberg17
Greeves12
Spicer and Greeves30
Velhagen, et al.32
Hine14
Redslob19
Year
1892 1900 1904 1905 1911 1914 1917 1920 1923
Author
Cucchia6
Satanowsky25
Bock4
Van der Hoeve31
Soudakoff29
Shepkalova27
Satanowsky, et al. Klien«
Year
1928 1928 1929 1930 1936 1938 1939 1939
Author
Czukrâsz7
Imre16
Shepkalova28
Rubino23
Rubino24
Asbury and Vail2
Andersen1
Fralick and Wilder10
Reese21
Year
1941 1941 1941 1941 1942 1944 1948 1949 1957*
* This tumor did not originate in the ciliary portion of the retina but in the optic papilla.
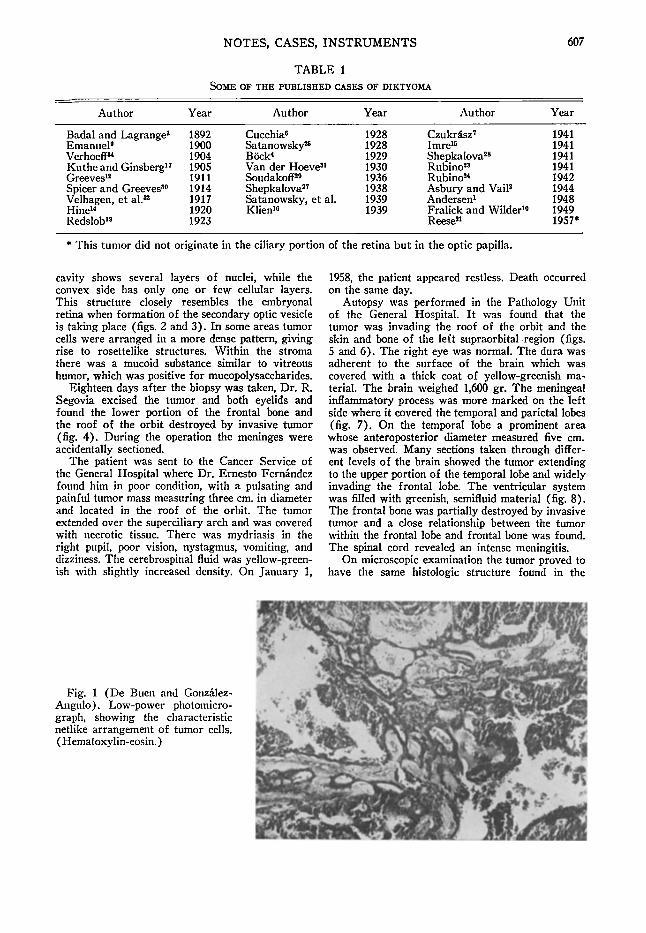
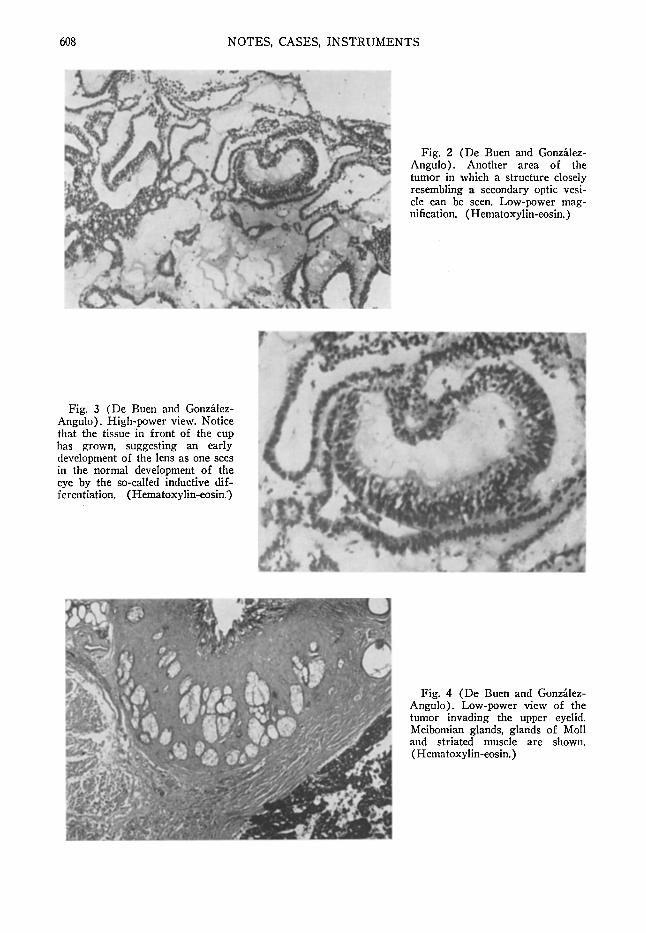
cavity shows several layers of nuclei, while the convex side has only one or few cellular layers. This structure closely resembles the embryonal retina when formation of the secondary optic vesicle is taking place (figs. 2 and 3). In some areas tumor cells were arranged in a more dense pattern, giving rise to rosettelike structures. Within the stroma there was a mucoid substance similar to vitreous humor, which was positive for mucopolysaccharides.
Eighteen days after the biopsy was taken, Dr. R. Segovia excised the tumor and both eyelids and found the lower portion of the frontal bone and the roof of the orbit destroyed by invasive tumor (fig. 4). During the operation the méninges were accidentally sectioned.
The patient was sent to the Cancer Service of the General Hospital where Dr. Ernesto Fernandez found him in poor condition, with a pulsating and painful tumor mass measuring three cm. in diameter and located in the roof of the orbit. The tumor extended over the superciliary arch and was covered with necrotic tissue. There was mydriasis in the right pupil, poor vision, nystagmus, vomiting, and dizziness. The cerebrospinal fluid was yellow-greenish with slightly increased density. On January 1,
1958, the patient appeared restless. Death occurred on the same day.
Autopsy was performed in the Pathology Unit of the General Hospital. It was found that the tumor was invading the roof of the orbit and the skin and bone of the left supraorbital region (figs. 5 and 6). The right eye was normal. The dura was adherent to the surface of the brain which was covered with a thick coat of yellow-greenish material. The brain weighed 1,600 gr. The meningeal inflammatory process was more marked on the left side where it covered the temporal and parietal lobes (fig. 7). On the temporal lobe a prominent area whose anteroposterior diameter measured five cm. was observed. Many sections taken through different levels of the brain showed the tumor extending to the upper portion of the temporal lobe and widely invading the frontal lobe. The ventricular system was filled with greenish, semifluid material (fig. 8). The frontal bone was partially destroyed by invasive tumor and a close relationship between the tumor within the frontal lobe and frontal bone was found. The spinal cord revealed an intense meningitis.
On microscopic examination the tumor proved to have the same histologie structure found in the
Fig. 1 (De Buen and Gonzâlez-Angulo). Low-power photomicrograph, showing the characteristic netlike arrangement of tumor cells. ( Hematoxylin-eosin. )
608 NOTES, CASES, INSTRUMENTS
Fig. 2 (De Buen and Gonzalez -Angulo). Another area of the tumor in which a structure closely resembling a secondary optic vesicle can be seen. Low-power magnification. (Hematoxylin-eosin.)
Fig. 3 (De Buen and Gonzâlez-Angulo). High-power view. Notice that the tissue in front of the cup has grown, suggesting an early development of the lens as one sees in the normal development of the eye by the so-called inductive differentiation. ( Hematoxylin-eosin.')
Fig. 4 (De Buen and Gonzâlez-Angulo). Low-power view of the tumor invading the upper eyelid. Meibomian glands, glands of Moll and striated muscle are shown. ( Hematoxylin-eosin. )

NOTES, CASES,
Fig. S (De Buen and Gonzâlez-Angulo). Photograph of the external surface of frontal and parietal bones showing the tumor mass (arrow) protruding through the orbit. A portion of the surrounding skin can still be seen.
Fig. 6 (De Buen and Gonzâlez-Angulo). Internal view of the same portion of the skull showing the tumor on the roof of the orbit and extending outward (arrow).
previous biopsy and surgical specimen. The tumor was demonstrated microscopically in the same places where it was grossly found (figs. 9, 10 and 11).
There were no other demonstrable abnormalities in the body with the exception of an ascaris lum-bricoides which was found in the terminal ileum.
DISCUSSION
During its development, the diktyoma reproduces the structure of embryonal retina. The epithelial cells which form the non-pigmented epithelial layer of ciliary body are derived from the retinal germinative ceils. These did not differenciate into true retina but retained their epithelial properties.
Fig. 9 (De Buen and Gonzâlez-Angulo). Low-power view of tumor cells invading the brain. ( Hematoxylin-eosin. )
INSTRUMENTS 609
Fig. 7 (De Buen and Gonzâlez-Angulo). Photograph showing the basal meningitis and tumor in the left frontal lobe.
Fig. 8 (De Buen and Gonzâlez-Angulo). Photograph showing purulent material within the ventricular system.

610 NOTES, CASES, INSTRUMENTS
Fig. 10. (De Buen and Gonzalez-Angulo). High-power view of tumor cells. (Hematoxylin-eosin.)
Diktyoma occurs in young people, the average age being five years,20 although Bock4 reported a case of a 16-year-old girl ; Soudakoff29 published a case of a 28-year-old man, Rubino23 another, in a 19-year-old man, and Hine14 a case of a 28-year-old man.
Diktyoma originates in the pars ciliaris retinae although theoretically the iris could also be the primary site.20 Recently Reese21
reported a diktyoma arising in the optic papilla. Wolter38 and Reese stated that diktyoma may arise in any portion of the retina.
The case herein reported, which has been mentioned by Lorenz E. Zimmerman in Lauren V. Ackerman's Surgical Pathology (St. Louis, Mosby, 1959, p. 1073) showed a great invasive power, with destruction of the frontal bone and invasion of the brain. There was extension by continuity from the orbital location into the brain, as has been found by other authors.20·36 The tumor formed pseudorosettes in some areas, similar to those seen in retinoblastoma. In other places, the cells were arranged in one or several layers as in embryonal retinas. In none of the sections was it possible to identify cartilage as Böck,4,Shepkalova,27,2S Klien,16 Fralick and Wilder10 were able to demonstrate. There were no cones and rods as has been reported,20 or glial tissue as Verhoeff,34 Bock4
and Velhagen have found. Fralick and Wilder designated "glioneuromatous diktyo-mas"18 those diktyomas with glial tissue.
The demonstration of primary optic vesicles in adult medullo-epithelioma has lead Wolter36 to the conclusion that there is a possible relationship between this tumor and diktyoma as has been pointed out by Fuchs11
and Andersen.1
In the present case the exact site of origin of the tumor is unknown, although probably it was in the pars ciliaris retinae, taking into consideration the very high predominance of this site over the others.
This case is of great value because of the postmortem studies which revealed a lack of métastases, since the extension to the brain was exclusively due to direct continuity. This finding confirms what is generally accepted. Also the patient did not improve under X-ray therapy which is the same as reported previously by other authors.
The histologie morphology of the diktyoma is so typical that the diagnosis could be established even without having to study the primary tumor within the eye.
The exact diagnosis of diktyoma is strictly microscopic. However, it should be considered in the differential diagnosis of intraocular tumors, especially in youthful patients.
Another interesting fact is that it was possible to study the. natural history of the tumor for a much longer period of time than usual. In general, the eye containing the diktyoma is enucleated, and when the microscopical diagnosis of diktyoma is established the tumor has already been totally excised.
Fig. 11 (De Buen and Gonzalez-Angulo). High-power magnification of another area of the tumor. ( Hematoxylin-eosin. )
REFERENCES
1. Andersen, S. R.: Medullo-epitheliomas, dictyoma and malignant-epithelioma of the ciliary body: General Review and a new case of dictyoma. Acta Ophth., 26:313-330, 1948.
2. Asbury, M. K.: Epithelial tumors of the iris. Am. J. Ophth., 27:1094-1106, 1944. 3. Badal, J., and Lagrange, F.: Arch, d'ophtal., 12:143, 1892. (Quoted by Andersen'.) 4. Bock, J.: Zur Kenntnis des Diktyoma retinae. Ztschr. f. Augenh., 69:17-30, 1929. 5. Christensen, L., Personal communication. 6. Cucchia, Α.: Contributo alia Conoscenza dei tumori della pars ciliaris retinae. Ann. di Ottalm. &
Clin. Ocul., 56:577,1928. 7. Czukrasz, I.: Arch. f. Ophth., 142:619, 1941. (Quoted by Andersen'.) 8. Elwyn, H.: Diseases of the Retina. Toronto and Philadelphia, Blakiston, 1948, p. 448. 9. Emanuel, C : Virchows Arch. f. Path. Anat., 161:338, 1900. (Quoted by Andersen'.) 10. Fralick, F. B., and Wilder, H. C ; Intraocular dictyoma and glioneuroma. Tr. Am. Ophth. Soc,
47:317-324, 1949. 11. Fuchs, Ε.: Wucherunger und Gschwulste des Ciliare Epithels. Arch. f. Ophth., 68:435, 1908. 12. Greeves, R.: Tr. Ophth. Soc U. Kingdom, 31:261, 1911. (Quoted by Imre".) 13. Grinker, R. R.: Gliomas of the retina. Arch. Ophth., 5:920, 1931. 14 Hine, M.: Tr. Ophth. Soc. U. Kingdom, 40:146, 1920. 15. Imre, H.: Dictyoma in an early stage. Arch. Ophth., 25:629, 1941. 16. Klien, B. Α.: Dictyoma retinae. Arch. Ophth., 22:432-438, 1939. 17. Küthe, R., and Ginsberg, S.: Malignes Epithelioma des Ciliarkorpers, Festschrift Julius. Hirsch
berg, in: Beit. Augenh. Veit U. Co., 1905, p. 127. 18. Nordmann, J.: Les timieurs de la retine ciliare. Ophthalmologica, 102:257-274, 1941. 19. Redslob, Ε.: Neuroepitheliome gliomateux de la retine. Contribution a I'etude des tumeurs re-
tiniennes. Bull. A. Frang. Cancer, 12:573-584, 1923. 20. Reese, A. B.: Tumors of the eye and adnexa. Section X, fascicle 38. Washington, D C , 1956. 21. : Medullo-epithelioma (diktyoma) of the optic nerve. Am. J. Ophth., 4 4 : 1 , 1957. 22. Rones, B.: Personal communication. 23. Rubino, Α.: Annali Ott., 69:385, 1941. (Quoted by Andersen'.) 24 : Arch. Ottal, 49:219, 1942. (Quoted by Andersen'.) 25. Satanowsky, P.: Semana Med., 2:1017-1028, 1928. (Quoted by Imre".) 26. Satanowsky, P., Bernasconi, L. E., and Cramer, E.: Arch. Oftal. (Buenos Aires), 13:523, 1939.
(Quoted by Imre".) 27. Shepkalova, V. M.: Ueber Diktyoma der Netzhaut. Vestnik Oftal., 13:95-99, 1938. 28. Shepkalova, V. M.: Dictyoma of retina. Vestnick Oftal., 18:323, 1941. 29. Soudakoff, P. S.: An advanced stage of dictyoma. Arch. Ophth., 65:680-685, 1936. 30. Spicer, W., and Greeves, R.: Proc Royal Soc Med., 8 - 9 : (Ophth.) 1914-1915. (Quoted by Ander
sen'.) 31. Van der Hoeve: Nederl. Tijdschr. Geneesk., 74:11 , 4731, 1930. 32. Velhagen, et al.: Klin. Monatsbl. f. Augenh., 58:239, 1917. 33. Velhagen, C : Eine Cliomännliche Geschwlst (neuroepithelioma Glioma tosum syringomyeloides
des Corpus Ciliaris. Klin. Monatsbl. f. Augenh., 62:571, 82, 1919. 34. Verhoeff, F. H.: A rare tumor arising from the pars ciliaris retinae (teratoneuroma) of a nature
SUMMARY
A case of diktyoma (embryonal medullo-epithelioma) in a 13-year-old boy is reported. The tumor had probably grown since the patient was two years of age. The tumor invaded the left frontal bone and brain, and the patient died with a generalized cerebrospinal meningitis.
A review of the literature with a more detailed study of some of the more interesting reported cases is presented. Some authors stated that the total number of published cases is less than 80. The average age of the patients is five years, although there
are cases reported in an older age group. Diktyoma arises in the undifferentiated
neuro-ectoderm of the primary optic vesicle. It grows slowly and usually shows a slight invasive power, growing within the eye first and extending into the orbit later. It does not metastasize. X-ray therapy does not seem to modify this tumor.
The microscopic picture of diktyoma is described and its relation with adult medullo-epithelioma is mentioned.
The diagnosis of diktyoma can only be made by microscopic study.
Adolf ο Prieto 709-10 (12).
NOTES, CASES, I N S T R U M E N T S 611
612 NOTES. CASES, INSTRUMENTS
hitherto unrecognized and its relation to the so-called glioma retinae. Tr. Am. Ophth. Soc, 10:351-77, 1904.
35. Wadsworth, J. A.: Epithelial tumors of the ciliary body. Am. J. Ophth., 32:1487-501, 1949. 36. Wolter, J. R., and James, B. R.: Adult type of medullo-Epithelioma of the ciliary body. Am. J.
Ophth., 46:19-26,1958. .
UVEAL MALIGNANT MELANOMAS*
ARVID G. HOLM, M.D. AND
WERNER C. KAUFMANN, M.D. Milwaukee, Wisconsin
During the last five years 14 eyes with malignant melanoma of the ciliary body and choroid have been diagnosed at the Marquette University Department of Ophthalmic Pathology. This represents about 10 percent of the eyes studied.
Malignant melanoma is the most common malignant intraocular tumor. It is almost always unilateral and the most usual site is the posterior choroid. Malignant melanomas of the choroid and ciliary body usually manifest themselves in adult life and are extremely rare in children. In the extensive statistical studies that have been conducted on the material in the Registry of Ophthalmic Pathology, the highest frequencies for this tumor are found in the fifth and sixth decades. The average age of patients with a malignant melanoma of the iris is from one to two decades younger than that of patients with a malignant melanoma elsewhere in the uvea. The racial incidence is striking, the tumor being extremely rare in Negroes. It occurs with equal frequency in males and females.
ETIOLOGY
There is some controversy as to the etiology of malignant melanoma but evidence suggests that the neoplasm originates either from the Schwann sheath of the ciliary nerves or the stromal melanoblasts of the
* From the Department of Ophthalmology, Marquette University Medical School and-the Veterans Administration Hospital, Wood, Wisconsin.
uvea. Normally the Schwann cell does not produce pigment but in pathologic states it becomes very versatile and may produce melanin. A tumor arising from this cell or the stromal melanoblast may be benign or malignant. A benign melanoma may be activated into a malignant growth by irritation from inflammation or perhaps trauma.
DIAGNOSIS
Ophthalmoscopy reveals a brownish to slate-gray colored lesion. Except when there is a retinal detachment, the tumor usually gives a solid globular appearance (fig. 1). There is a relative or absolute scotoma if the lesion is near the macular region. If the neoplasm is located away from the macula it does not manifest itself until an appreciable defect occurs in the visual field. Secondary glaucoma or an iridocyclitis frequently cause the presenting symptoms. A hemorrhage in the vitreous or anterior chamber with or without glaucoma may be the first manifestations. Tumor necrosis seems to be the most common cause of hemorrhage and inflammation. Under all conditions which interfere with direct observation of the lesion it is usually necessary in making the diagnosis to rely on history, transillumination and other aids, such as uptake of radioactive phosphorus. It is interesting to note that about 10 percent of eyes with malignant melanoma have opaque media. Biopsy for diagnosis of melanoma of the uveal tract has very few indications because of unreliability and possibility of disseminating the tumor.
Perimetry is very helpful in differentiating between a benign and malignant melanoma of the choroid. A change in the visual field is sufficient evidence to diagnose the lesion as malignant. A field defect from a malignant melanoma is larger than would be


















