
Diffusion-Weighted Magnetic Resonance Imaging in the Prostate...
9
Diffusion-Weighted Magnetic Resonance Imaging in the Prostate Transition Zone Histopathological Validation Using Magnetic ResonanceYGuided Biopsy Specimens Caroline M. A. Hoeks, MD,* Eline K. Vos, MD,* Joyce G. R. Bomers, MSc,* Jelle O. Barentsz, MD, PhD,* Christina A. Hulsbergen-van de Kaa, MD, PhD,Þ and Tom W. Scheenen, PhD* Objectives: The objective of this study was to evaluate the apparent diffusion coefficient (ADC) of diffusion-weighted magnetic resonance (MR) imaging for the differentiation of transition zone cancer from non-cancerous transition zone with and without prostatitis and for the differentiation of transition zone cancer Gleason grade (GG) using MR-guided biopsy specimens as a reference standard. Materials and Methods: From consecutive MR-guided prostate biopsies (2008Y2012) in our referral center, we retrospectively included patients from whom diffusion-weighted MR imaging ADC values were acquired during MR-guided biopsy and whose biopsy cores had a (cancer) core length 10 mm or greater and originated from the transition zone. Two radiologists, whowere blinded to the ADC data, annotated regions of interest on biopsy sampling locations of MR-guided biopsy confirmation scans in consensus. Median ADC (mADC) of the regions of interest was related to histopathology out- come in MR-guided biopsy core specimens. Mixed model analysis was used to evaluate mADC differences between 7 histopathology categories predefined as MR-guided biopsy core specimens with primary and secondary GG 4Y5 (I), primary GG 4Y5 secondary GG 2Y3 (II), primary GG 2Y3 secondary GG 4Y5 (III) and primary and secondary GG 2Y3 cancer (IV), and noncancerous tissue without (V) or with degree 1 (VI) or degree 2 prostatitis (VII). Diagnostic accuracy was evaluated using areas under the receiver operating characteristic (AUC) curve. Results: Fifty-two patients with 87 cancer-containing biopsy cores and 53 patients with 101 non-cancerous biopsy cores were included. Significant mean mADC dif- ferences were present between cancers (mean mADC, 0.77Y0.86 Â 10 j3 mm 2 /s) and noncancerous transition zone without (1.12 Â 10 j3 mm 2 /s) and with degree 1 to 2 prostatitis (1.05Y1.12 Â 10 j3 mm 2 /s; P G 0.0001Y0.05). Exceptions were mixed primary and secondary GG cancers versus a degree 2 of prostatitis (P = 0.06Y0.09). No significant differences were found between subcategories of primary and sec- ondary GG cancers (P = 0.17Y0.91) and between a degree 1 and 2 prostatitis and non-cancerous transition zone without prostatitis (P = 0.48Y0.94). The mADC had an AUC of 0.84 to differentiate cancer versus non-cancerous transition zone. AUCs of 0.84 and 0.56 were found for mADC to differentiate prostatitis from cancer and from non-cancerous transition zone. The mADC had an AUC of 0.62 to differentiate a primary GG 4 versus GG 3 cancer. Conclusions: The mADC values can differentiate transition zone cancer from non-cancerous transition zone and from a degree 1, and from most cases of a degree 2 prostatitis. However, because of substantial overlap, mADC has a moderate accuracy to differentiate between different primary and secondary GG subcategories and cannot be used to differentiate non-cancerous transition zone from degrees 1 to 2 of prostatitis. Diffusion-weighted imaging ADC may therefore contribute in the detection of transition zone cancers; however, as a single functional MR imaging technique, diffusion-weighted imaging has a mod- erate diagnostic accuracy in separating higher from lower GG transition zone cancers and in differentiating prostatitis from non-cancerous transition zone. Key Words: apparent diffusion coefficient, Gleason grade, MR imaging, prostate cancer, transition zone (Invest Radiol 2013;48: 693Y701) P rostate cancer is the second most frequently diagnosed cancer in men worldwide. 1 Based on radical prostatectomy and saturation biopsy specimens, at least 30% to 45% of diagnosed cancers are situated in the prostate transition zone. 2,3 In patients with an elevated prostate-specific antigen (PSA) and cancer-negative transrectal ultrasound-guided biopsies, high proportions of transition zone can- cer (57%Y63%) are detected upon magnetic resonance (MR)Yguided biopsy. 4,5 The latter finding reflects that many transition zone cancers are missed by transrectal ultrasound-guided biopsy, probably because of undersampling of the ventral prostate transition zone. Performing MR imaging 6 and MR-guided biopsy in patients with an elevated PSA and negative transrectal ultrasound-guided biopsies may there- fore improve detection of transition zone prostate cancer. However, upon MR imaging of the prostate transition zone, differentiation of prostate cancer from healthy tissue is difficult because of the overlap of signal intensities and quantitative parameters between prostate cancer and stromal benign prostatic hyperplasia. 7,8 Prostate cancer should also be differentiated from prostatitis, which is often present also in the transition zone. 9 In prostatitis, in- flammatory infiltrates may increase cellular density and may therefore decrease T2-weighted MR imaging signal intensity and diffusion- weighted MR imaging apparent diffusion coefficient (ADC) values. For the peripheral zone, prostatitis can be differentiated from healthy tissue and from lowYGleason grade (GG) cancer; however, for the transition zone, differentiation of prostatitis from a high-GG cancer and from healthy tissue has not been described earlier. 10 Once a transition zone cancer is detected on MR imaging, accurate determination of its Gleason score is important because transition zone cancers are known to have lower Gleason scores and lower biochemical recurrence rates. 11 Lower diffusion-weighted im- aging ADC values have been related to higher prostate cancer Gleason scores, predominantly for peripheral zone cancers. 12,13 Most of these studies have been performed using radical prostatectomy specimens as a reference standard. However, exact alignment of MR imaging slices with prostatectomy specimen sections remains diffi- cult because of differences in angulations of imaging slicing and specimen sectioning and because of prostate shrinkage during his- topathology processing. Furthermore, observer bias is almost un- avoidable in attributing a certain region of interest (ROI) on MR imaging to a tumor, which is identified in a prostatectomy specimen ORIGINAL ARTICLE Investigative Radiology & Volume 48, Number 10, October 2013 www.investigativeradiology.com 693 Received for publication October 11, 2012; and accepted for publication, after revision, February 19, 2013. From the *Departments of Radiology, and †Pathology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands. Conflicts of interest and sources of funding: Supported by the ERC grant agreement no. 243115 from the European Research Council under the European Com- munity’s Seventh Framework Programme (FP7/2007Y2013) and by the program grant KUN 2007/3971 from the Dutch Cancer Society. The authors report no conflicts of interest. Reprints: Caroline M. A. Hoeks, MD, Department of Radiology, Radboud Uni- versity Nijmegen Medical Centre, Geert Grooteplein 10, Postbus 9101, 6500 HB Nijmegen, The Netherlands. E-mail: [email protected]. Copyright * 2013 by Lippincott Williams & Wilkins ISSN: 0020-9996/13/4810Y0693 Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Diffusion-Weighted Magnetic Resonance Imaging in the Prostate...

Diffusion-Weighted Magnetic Resonance Imagingin the Prostate Transition Zone
Histopathological Validation Using Magnetic ResonanceYGuided Biopsy Specimens
Caroline M. A. Hoeks, MD,* Eline K. Vos, MD,* Joyce G. R. Bomers, MSc,* Jelle O. Barentsz, MD, PhD,*Christina A. Hulsbergen-van de Kaa, MD, PhD,Þ and Tom W. Scheenen, PhD*
Objectives: The objective of this study was to evaluate the apparent diffusioncoefficient (ADC) of diffusion-weighted magnetic resonance (MR) imagingfor the differentiation of transition zone cancer from non-cancerous transitionzone with and without prostatitis and for the differentiation of transition zonecancer Gleason grade (GG) using MR-guided biopsy specimens as a referencestandard.Materials and Methods: From consecutive MR-guided prostate biopsies(2008Y2012) in our referral center, we retrospectively included patients fromwhom diffusion-weighted MR imaging ADC values were acquired duringMR-guided biopsy and whose biopsy cores had a (cancer) core length 10 mmor greater and originated from the transition zone. Two radiologists, who wereblinded to the ADC data, annotated regions of interest on biopsy samplinglocations of MR-guided biopsy confirmation scans in consensus. MedianADC (mADC) of the regions of interest was related to histopathology out-come in MR-guided biopsy core specimens. Mixed model analysis was usedto evaluate mADC differences between 7 histopathology categories predefinedas MR-guided biopsy core specimens with primary and secondary GG 4Y5 (I),primary GG 4Y5 secondary GG 2Y3 (II), primary GG 2Y3 secondary GG 4Y5(III) and primary and secondary GG 2Y3 cancer (IV), and noncancerous tissuewithout (V) or with degree 1 (VI) or degree 2 prostatitis (VII). Diagnosticaccuracy was evaluated using areas under the receiver operating characteristic(AUC) curve.Results: Fifty-two patients with 87 cancer-containing biopsy cores and 53 patientswith 101 non-cancerous biopsy cores were included. Significant mean mADC dif-ferences were present between cancers (mean mADC, 0.77Y0.86 � 10j3 mm2/s)and noncancerous transition zonewithout (1.12� 10j3 mm2/s) and with degree 1 to2 prostatitis (1.05Y1.12 � 10j3 mm2/s; P G 0.0001Y0.05). Exceptions were mixedprimary and secondary GG cancers versus a degree 2 of prostatitis (P = 0.06Y0.09).No significant differences were found between subcategories of primary and sec-ondary GG cancers (P = 0.17Y0.91) and between a degree 1 and 2 prostatitis andnon-cancerous transition zone without prostatitis (P = 0.48Y0.94).
The mADC had an AUC of 0.84 to differentiate cancer versus non-canceroustransition zone. AUCs of 0.84 and 0.56 were found for mADC to differentiateprostatitis from cancer and from non-cancerous transition zone. The mADC hadan AUC of 0.62 to differentiate a primary GG 4 versus GG 3 cancer.Conclusions: The mADC values can differentiate transition zone cancer fromnon-cancerous transition zone and from a degree 1, and from most cases of adegree 2 prostatitis. However, because of substantial overlap, mADC has amoderate accuracy to differentiate between different primary and secondary
GG subcategories and cannot be used to differentiate non-cancerous transitionzone from degrees 1 to 2 of prostatitis. Diffusion-weighted imaging ADC maytherefore contribute in the detection of transition zone cancers; however, as asingle functional MR imaging technique, diffusion-weighted imaging has a mod-erate diagnostic accuracy in separating higher from lower GG transition zonecancers and in differentiating prostatitis from non-cancerous transition zone.
Key Words: apparent diffusion coefficient, Gleason grade, MR imaging,prostate cancer, transition zone
(Invest Radiol 2013;48: 693Y701)
P rostate cancer is the second most frequently diagnosed cancer inmen worldwide.1 Based on radical prostatectomy and saturation
biopsy specimens, at least 30% to 45% of diagnosed cancers aresituated in the prostate transition zone.2,3 In patients with an elevatedprostate-specific antigen (PSA) and cancer-negative transrectalultrasound-guided biopsies, high proportions of transition zone can-cer (57%Y63%) are detected upon magnetic resonance (MR)Yguidedbiopsy.4,5
The latter finding reflects that many transition zone cancersare missed by transrectal ultrasound-guided biopsy, probably becauseof undersampling of the ventral prostate transition zone. PerformingMR imaging6 and MR-guided biopsy in patients with an elevatedPSA and negative transrectal ultrasound-guided biopsies may there-fore improve detection of transition zone prostate cancer. However,upon MR imaging of the prostate transition zone, differentiation ofprostate cancer from healthy tissue is difficult because of the overlapof signal intensities and quantitative parameters between prostatecancer and stromal benign prostatic hyperplasia.7,8
Prostate cancer should also be differentiated from prostatitis,which is often present also in the transition zone.9 In prostatitis, in-flammatory infiltrates may increase cellular density and may thereforedecrease T2-weighted MR imaging signal intensity and diffusion-weighted MR imaging apparent diffusion coefficient (ADC) values.For the peripheral zone, prostatitis can be differentiated from healthytissue and from lowYGleason grade (GG) cancer; however, for thetransition zone, differentiation of prostatitis from a high-GG cancerand from healthy tissue has not been described earlier.10
Once a transition zone cancer is detected on MR imaging,accurate determination of its Gleason score is important becausetransition zone cancers are known to have lower Gleason scores andlower biochemical recurrence rates.11 Lower diffusion-weighted im-aging ADC values have been related to higher prostate cancerGleason scores, predominantly for peripheral zone cancers.12,13 Mostof these studies have been performed using radical prostatectomyspecimens as a reference standard. However, exact alignment of MRimaging slices with prostatectomy specimen sections remains diffi-cult because of differences in angulations of imaging slicing andspecimen sectioning and because of prostate shrinkage during his-topathology processing. Furthermore, observer bias is almost un-avoidable in attributing a certain region of interest (ROI) on MRimaging to a tumor, which is identified in a prostatectomy specimen
ORIGINAL ARTICLE
Investigative Radiology & Volume 48, Number 10, October 2013 www.investigativeradiology.com 693
Received for publication October 11, 2012; and accepted for publication, afterrevision, February 19, 2013.
From the *Departments of Radiology, and †Pathology, Radboud University NijmegenMedical Centre, Nijmegen, The Netherlands.
Conflicts of interest and sources of funding: Supported by the ERC grant agreementno. 243115 from the European Research Council under the European Com-munity’s Seventh Framework Programme (FP7/2007Y2013) and by the programgrant KUN 2007/3971 from the Dutch Cancer Society.
The authors report no conflicts of interest.Reprints: Caroline M. A. Hoeks, MD, Department of Radiology, Radboud Uni-
versity Nijmegen Medical Centre, Geert Grooteplein 10, Postbus 9101, 6500HB Nijmegen, The Netherlands. E-mail: [email protected].
Copyright * 2013 by Lippincott Williams & WilkinsISSN: 0020-9996/13/4810Y0693
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
section.14 Recently, size and positioning of an ROI were shown toinfluence tumor ADC measurements and interobserver variability inrectal cancer.15
Magnetic resonanceYguided biopsy specimens may be areference-standard alternative for radical prostatectomy specimensbecause the highest GG of an MR-guided biopsy specimen has ahigh concordance (88%) with the highest GG of the radical prosta-tectomy specimen.16 This high concordance rate is caused by theability of multiparametric MR imaging and especially of diffusion-weighted MR imaging to predict and localize the cancer areas withthe highest GG.17 When using MR-guided biopsy as a referencestandard, T2*-weighted gradient echo images, which confirm needlepositioning, are available.5 Locations where prostate cancer biopsyspecimens were sampled can be determined from signal voids of thebiopsy needle on these MR-guided biopsy confirmation scans. Be-cause annotation of biopsy sampling areas on confirmation scans isunrelated to the ADC map, it may reduce observer bias in relatingADC values to MR-guided biopsy histopathology.
Therefore, our purpose was to evaluate the ADC of diffusion-weighted MR imaging for the differentiation of the transition zonecancer from the non-cancerous transition zone with and withoutprostatitis and for the differentiation of transition zone cancer GGsusing MR-guided biopsy specimens as a reference standard.
MATERIALS AND METHODSPatients
The need for informed consent for this retrospective studywas waived by the institutional review board. From all consecu-tively performed MR-guided biopsies between March 2008 andFebruary 2012 in our referral center, we included patients using thefollowing inclusion criteria:
- Performed diffusion-weighted imaging and ADC maps as part of theMR-guided biopsy procedure.
- Magnetic resonanceYguided biopsy cores with prostate cancer in acancer core length of 10 mm or greater and a transition zone locationon MR-guided biopsy confirmation scans. A cancer core length of10 mm or greater is 60% of a standard needle notch length of 17 mmand was chosen to limit variation because of mADC measurementsin noncancerous tissue. By choosing this limit, at least 60% of theannotated ROI was related to prostate cancer.
- Magnetic resonanceYguided biopsy cores without prostate cancer witha core length of 10 mm or greater and a transition zone location of theneedle sample on MR-guided biopsy confirmation scans.
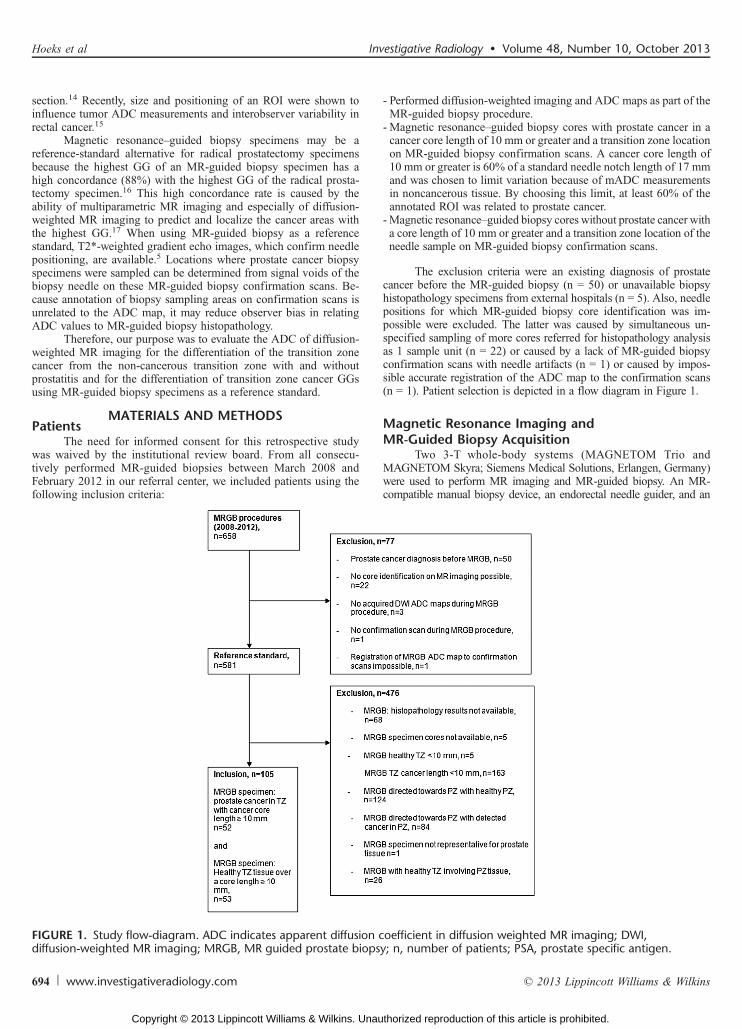
The exclusion criteria were an existing diagnosis of prostatecancer before the MR-guided biopsy (n = 50) or unavailable biopsyhistopathology specimens from external hospitals (n = 5). Also, needlepositions for which MR-guided biopsy core identification was im-possible were excluded. The latter was caused by simultaneous un-specified sampling of more cores referred for histopathology analysisas 1 sample unit (n = 22) or caused by a lack of MR-guided biopsyconfirmation scans with needle artifacts (n = 1) or caused by impos-sible accurate registration of the ADC map to the confirmation scans(n = 1). Patient selection is depicted in a flow diagram in Figure 1.
Magnetic Resonance Imaging andMR-Guided Biopsy Acquisition
Two 3-T whole-body systems (MAGNETOM Trio andMAGNETOM Skyra; Siemens Medical Solutions, Erlangen, Germany)were used to perform MR imaging and MR-guided biopsy. An MR-compatible manual biopsy device, an endorectal needle guider, and an
FIGURE 1. Study flow-diagram. ADC indicates apparent diffusion coefficient in diffusion weighted MR imaging; DWI,diffusion-weighted MR imaging; MRGB, MR guided prostate biopsy; n, number of patients; PSA, prostate specific antigen.
Hoeks et al Investigative Radiology & Volume 48, Number 10, October 2013
694 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE
1.Mag
netic
Resona
nceIm
agingan
dMR-Guide
dBiop
syPa
rameters
Protocol
Sequence
TA
(min:s)
TR
(ms)
TE(m
s)Flip
Angle(degrees)
Slice
Thickness(m
m)
Field
ofView
(mm�
mm)
MatrixSize
Voxel
Size
(mm�
mm�
mm)
b-Values
(s/m
m2)
Tem
poral
Resolution
(s)
Multip
aram
etricMRim
aging(SiemensTrioTim
)usingthe32
-chann
elspinal
andpelvic
phased
arraycoils
T2W
MRim
aging
TSEsagittal
3:33
4950
110
120
3.0
180�
180
320�
320
0.6�
0.6�
3.0
n.a.
n.a.
Axial
3:22
4480
103
120
3.0
180�
180
320�
320
0.6�
0.6�
3.0
n.a.
n.a.
Coron
al1:55
4250
110
120
3.0
180�
180
320�
320
0.6�
0.6�
3.0
n.a.
n.a.
DWI
EPI
3:08
2500
64n.a.
4.0
256�
256
128�
128
2.0�
2.0�
4.0
50/500
/800
n.a.
DCE-M
RI
3DUltrafast
2:43
32*
1.47
104.0
230�
230
128�
128
1.8�
1.8�
4.0
n.a.
4.7
GE
Axial
Multip
aram
etricMRim
aging(SiemensMAGNETOM
Skyra)
T2W
MRim
aging
TSEsagittal
2:53
5590
101
160
3.0
180�
180
320�
320
0.6�
0.6�
3.0
n.a.
n.a.
Axial
4:15
5660
104
160
3.0
192�
192
384�
384
0.5�
0.5�
3.0
n.a.
n.a.
Coron
al1:57
4320
101
160
3.0
192�
192
320�
320
0.6�
0.6�
3.0
n.a.
n.a.
DWI
EPI
3:29
2700
63n.a.
3.0
256�
256
128�
128
2.0�
2.0�
3.0
50/500
/800
n.a.
Axial
DCE-M
RI
3DUltrafast
2:34
36*
1.41
143.0
192�
192
128�
128
1.5�
1.5�
3.0
n.a.
3.5
GE
Axial
MRGB(SiemensTrioTim
)
T2w
MRim
aging
TSE
3:35
4570
101
120
3.0
256�
256
320�
224
1.1�
0.8�
3.0
n.a.
n.a.
Axial
DWI
EPI
3:08
2500
64n.a.
4.0
256�
256
128�
128
2.0�
2.0�
4.0
50/500
/800
n.a.
Axial
2DBalancedSSFP
GE
0:09
4.48
2.24
703.0
280�
280
256�
256
1.1�
1.1�
3.0
n.a.
n.a.
Axial
0:08
Sagittal
MRGB(SiemensMAGNETOM
Skyra)
T2w
MRim
aging
TSE
3:32
4510
101
120
3.0
256�
256
320�
320
0.8�
0.8�
3.0
n.a.
n.a.
Axial
DWI
EPI
3:29
2700
63n.a.
3.0
256�
256
128�
128
2.0�
2.0�
3.0
50/500
/800
n.a.
Axial
2Dbalanced
SSFP
GE
0:09
4.56
2.28
703.0
280�
280
256�
256
1.1�
1.1�
3.0
n.a.
n.a.
Axial
andsagittal
0:08
*Allpartition
s.
2Dindicates2-dimension
al;3
D,3
-dim
ension
al;D
WI,diffusion-weigh
tedmagnetic
resonanceim
aging;
DCE-M
RI,dy
namiccontrast-enh
ancedmagnetic
resonanceim
aging;
EPI,echo
-planarim
aging;
GE,gradientecho;MR,m
agnetic
resonance;SSEPI,steady-stateecho
planarim
aging;SSFP,steady
statefree
procession;T
2wMRim
aging,T2-weightedmagnetic
resonanceim
aging;TA
,acquisitio
ntim
e;TE,echotim
e;TR,repetition
time;
TSE,turbospin
echo.
Investigative Radiology & Volume 48, Number 10, October 2013 Validation of ADC in the Prostate Transition Zone
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 695
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

18-gauge biopsy gun (all from Invivo, Gainesville, FL) were used toperform the MR-guided biopsy. To detect prostate cancer, MR-guidedbiopsies were performed on the basis of the results of a previouslyperformed multiparametric MR imaging examination, consisting ofT2-weighted, diffusion-weighted, and dynamic contrast-enhanced MRimaging.5 The multiparametric MR imaging and MR-guided biopsysequence parameters are depicted in Table 1. Two radiologists with 10and 19 years of experience in prostate MR imaging (J.J.F. and J.O.B.)evaluated the initial MR images on a clinical software workstationwhile having access to patient data.18 Cancer suspicious regions weredefined as described earlier.19
The patients received antibiotic prophylaxis of 2 daily dosesof 500-mg ciprofloxacin orally for 3 days and the biopsy wasperformed on the second day. Biopsies were performed by 1 radiolo-gist with 3 years (C.M.A.H.), 1 radiologist with 2 years (J.G.R.B.),and 1 radiologist (E.K.V.) with 1 year of experience in MR-guidedbiopsy.19 Initially, T2-weighted MR imaging and diffusion-weightedimaging were performed for the re-identification of previously de-fined cancer suspicious regions. Consequently, sagittal and axial bal-anced gradient echo sequences were acquired during the repositioningof an endorectally inserted needle guide towards a cancer-suspiciousregion. When the needle guide was accurately targeted at a cancer-suspicious region, biopsies were taken by insertion of the 18-gaugeneedle biopsy gun (In vivo, Schwerin, Germany) through the needleguide. Directly after the MR-guided biopsy with the needle situated inthe prostate, gradient echo sequences were repeated to confirm theposition of the (sampling part of the) needle in a cancer-suspicious re-gion. Acquisition times for the transverse and sagittal confirmationscans for MAGNETOM Trio and Skyra were 8.9 and 9.0 secondsfor the axial scans and 7.5 and 7.6 seconds for the sagittal scans,respectively.
HistopathologyBiopsy core specimens were directly fixated in formalin. The
cores were fixated and analyzed separately. All cores were histopa-thologically re-evaluated by 1 experienced urogenital pathologist with20 years of experience (C.A.H.), who was blinded to the MR imagingresults. Gleason grade was evaluated using the 2005 International So-ciety of Urological Pathology-modified Gleason grading criteria.20
Prostatitis was defined as the presence of inflammatory infiltrates in theprostate.21 A degree 1 (mild), 2 (moderate), and 3 (severe) prostatitiswere respectively defined as follows: an MR-guided prostate biopsyspecimen core tissue area involvement of 1 lower than 10% by inflam-matory cell infiltrates consisting of individual cells, separated by dis-tinct intervening spaces (G100 cells/mm2), 2 10% to 50% consisting ofconfluent sheets of inflammatory cells with no tissue destruction orlymphoid nodule or follicle formation (100Y500 cells/mm2), 3 greaterthan 50% consisting of confluent sheets of inflammatory cells withtissue destruction or nodule/follicle formation (9500 cells/mm2).21
Differentiation was made between chronic, chronic active, and granu-lomatous prostatitis.21
Annotation of MR-Guided BiopsyConfirmation Scans
Magnetic resonance-guided biopsy confirmation scans wereanalyzed with an in-houseYdeveloped software.18 Two radiologists(one with 3 years [C.M.A.H.] and one with 1 year [E.K.V.] of expe-rience in prostate MR imaging) annotated ROIs in consensus whilethey were blinded for histopathology results. In case of prostate dis-placement during the MR-guided biopsy procedure, the ADC mapswere manually registered with the post-biopsy confirmation scans tocorrect for this displacement. Slices that most optimally represented
the middle of the needle artifact were identified on both the sagittaland the transversal post-biopsy T2-weighted balanced gradient echoimages. Subsequently, the presumed in vivo needle track of 22 mmwas measured from the visible needle tip inside the signal void,taking into account a signal void of the needle artifact (2Y3 mm) infront of the needle trajectory. The last 17 mm of this 22 mm repre-sented the needle notch, where the tissue core was obtained. This last17 mm area was annotated on the transverse T2-weighted balancedgradient echo image. The notch length of 17 mm was annotated withoverlapping ROIs (4.0 � 4.0 � 4.0 mm) matching the visible needlewithin the artifact signal void. An example of our annotation methodis depicted in Figure 2. The radiologists annotated all cores over theentire core length (17 mm) in all patients. In patients in whom thecore sample involved extraprostatic tissue, only the core parts situ-ated in the prostate were annotated. All ROIs of 1 notch length rep-resented 1 core and were analyzed as a unit. For every annotatedcore, the mean, the SD, and the median ADC (mADC) were calcu-lated by the software using the ADC values from all annotated ROIsin the core.
StatisticsThe analyses were performed using Predictive Analytics
SoftWare (PASW) Statistics version 18 (SPSS, Inc, Quarry Bay,Hong Kong). The threshold for significance was defined as P G 0.05.Differences in patient characteristics were evaluated using independentt tests for parametric continuous variables and the Mann-Whitneytest for non-parametric continuous variables.
The ROI ADC was related to the histopathology outcome inMR-guided biopsy specimens, which served as a reference standard.Linear multilevel mixed model analysis was used to evaluate mADCdifferences for 7 histopathology categories, defined as MR-guidedbiopsy core specimens with a primary and secondary GG 4Y5 (I), pri-mary GG 4Y5 secondary GG 2Y3 (II), a primary GG 2Y3 secondaryGG 4Y5 (III) and primary and secondary GG 2Y3 cancer (IV) cancer,and noncancerous transition zone tissue without (V) or with degree 1prostatitis (VI) or degree 2 prostatitis (VII). To correct for possible cor-relations between different cores coming from 1 patient, patients wereused as a random factor in this model. Because non-cancerous parts incancer-containing cores may have caused mADC variation, we com-pared mADC for cancer core lengths of respectively 10 to 12, 13 to 15,and greater than 15 mm.
Receiver operating characteristic (ROC) analyses were per-formed to evaluate diagnostic accuracy for mADC to differentiatebetween predefined histopathological categories.
RESULTSWe included 87 MR-guided biopsy cores containing transi-
tion zone cancer in 52 patients and 101 non-cancerous transitionzone cores in another 53 patients. Patient characteristics are de-picted in Table 2. For every patient, MR-guided biopsy cores weretaken from 1 cancer-suspicious region. A patient example is de-picted in Figure 3.
Of the 87 cancer-containing cores, 27 cores had a primary andsecondary GG 4Y5, 12 cores had a primary GG 4Y5 and a secondaryGG 2Y3, 24 cores had a primary GG 2Y3 and a secondary GG 4Y5, andanother 24 cores had both primary and secondary GG 2Y3. Of the 101non-cancerous transition zone cores, 46 cores existed out of healthytransition zone tissue without prostatitis, 50 cores contained a degree 1prostatitis (of which 88% [44/50] were of a chronic type and 12% [6/50]were of a chronic active type), and 5 cores involved prostatitis up to adegree of 2 (2 of the chronic and 3 of the chronic active type). Becausethe subtotals of cores with a chronic (active) type of prostatitis were verysmall, no further analyses were performed to differentiate between thechronic and chronic active types of prostatitis.J.J.F., one of the radiologists in this study, is not an author of this article.
Hoeks et al Investigative Radiology & Volume 48, Number 10, October 2013
696 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

For patients with transition zone cancer, MR-guided biopsy corelengths ranged from 12.0 to 16.0 mm (interquartile range) and wereinvaded by cancer (cancer core length) in a length of (interquartile range)11.0 to 14.0 mm. Core length of the non-cancerous MR-guided biopsyspecimens ranged from 10.3 to 15.0 mm.
Upon linear mixed model analysis, significant mADC differ-ences were present between transition zone cancers (mean mADC,0.77Y0.86� 10j3 mm2/s) and non-cancerous transition zone without(1.12� 10j3 mm2/s) and with degrees 1 to 2 prostatitis (1.05Y1.12�10j3 mm2/s; P G 0.0001Y0.05). The exceptions were transition zonecancers with a primary GG 4Y5 and a secondary GG 2Y3 or a pri-mary GG 2Y3 and a secondary GG 4Y5 versus a degree 2 of pros-tatitis (P = 0.06Y0.09). No significant differences were found
between subcategories of transition zone cancer primary and sec-ondary GG (P = 0.17Y0.91) and between healthy transition zone with-out prostatitis versus both degree 1 and 2 prostatitis (P = 0.48Y0.94). InFigure 4, boxplots of mADC values for MR guided biopsy specimenhistopathological categories are presented. Comparing the cores with aGleason score 3+3 (n = 14) versus a Gleason score 4+4 (n = 6) only,the mean ADC values were 0.85 � 10j3mm2/s (95% confidenceinterval [CI], 0.70Y0.99 � 10j3mm2/s) and 0.79 � 10j3mm2/s (CI,0.57Y1.01� 10j3mm2/s), respectively (P = 0.66). Because only 1 corehad a single GG 5 pattern, this core was left out of the analysis. Forcancer-containing cores, a scatterplot depicting mADC values fordifferent Gleason scores is shown in Figure 5. Taking into accountthe MR-guided biopsy cancer core length, no significant mADC
FIGURE 2. A to C, Illustration of the annotation of an MR-guided biopsy core on a T2-weighted balanced gradient echoconfirmation scan. Note the appearance of the inserted needle with a signal void around it, exaggerating the true size of the needle(diameter, 1.27 mm). The needle is visible within this signal void. A, Measurement of the needle pathway of 22 mm in the needleartifact on a transversal T2-weighted balanced gradient echo confirmation scan (repetition time [TR], 4.48 milliseconds; echo time[TE], 2.24 milliseconds). B, Annotation of the core length (the last 17 mm of the 22 mm as depicted in A with ROIs on a transversalT2-weighted balanced gradient echo confirmation scan (TR, 4.48 milliseconds; TE, 2.24 milliseconds). This anatomical scan wasused to reconfirm correct positioning of the whole needle sampling part within the prostate transition zone. C, Completedannotation of an MR-guided biopsy core. Regions of interest are appended in 1 unit for analysis. The location of the annotated core(IV) can be seen in the baseline diffusion-weighted image (TR, 3300 milliseconds; TE, 60 milliseconds) (I), baseline T2-weightedimage (TR, 3620 milliseconds; TE, 103 milliseconds) (II), and the corresponding sagittal T2-weighted balanced gradient echoconfirmation scan (TR, 4.48 milliseconds; TE, 2.24 milliseconds) (III).
Investigative Radiology & Volume 48, Number 10, October 2013 Validation of ADC in the Prostate Transition Zone
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 697
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

differences were present for cancer core lengths of, respectively, 10 Y e12, 9 12 Y e 15 and greater than 15 mm for patients with primaryGG 3 (P = 0.22Y0.87), 4 (P = 0.05Y0.84), and 5 cancers (P = 0.70Y0.91).
Receiver operating characteristic analysis for mADC to dif-ferentiate transition zone cancer cores (n = 87) from non-canceroustransition zone cores (n = 46) resulted in an AUC of 0.84 (95% CI,0.77Y0.91). For the differentiation between the cancerous (n = 87)and non-cancerous cores with prostatitis (n = 55), the AUC alsowas 0.84 (0.77Y0.90). The AUC for differentiating the non-cancerouscores with any degree of prostatitis (n = 55) versus the non-cancerouscores without (n = 46) prostatitis was 0.56 (0.44Y0.67). The mADChad an AUC of 0.62 (0.49Y0.74) for the differentiation of primaryGG 4Y5 (n = 39) from GG 2Y3 (n = 48) cancers.
DISCUSSIONOur results show that mADC values can differentiate the transi-
tion zone cancer from the non-cancerous transition zone (AUC 0.84) andfrom any degree of prostatitis (AUC 0.84). However, because of sub-stantial overlap, mADC has a poor accuracy to distinguish primaryGG 4Y5 from GG 2Y3 transition zone cancers (AUC 0.62) and cannot beused to differentiate between noncancerous transition zone with andwithout prostatitis (AUC 0.56).
Our significant mADC differences for transition zone cancerversus non-cancerous transition zone confirm findings in other stud-ies.8,13,22,23 The ADC for transition zone cancer in these studies variedbetween 0.61Y1.13�10j3mm2/s versus the ADC values for non-cancerous transition zone of 1.08Y1.73�10j3mm2/s. In so far as the
ADC values can be compared for diffusion-weighted MR imagingsequences with different b-values, our mean mADC values for bothcancer (0.77Y0.86 �10j3mm2/s) and for non-cancerous transitionzone tissue (1.12�10j3mm2/s) were in the lower range of thesereported values. As we targeted cancer-suspicious regions using MR-guided biopsy specimens as a reference standard, our ADC valuesmay have been in the lower ranges of the former radical prostatectomy-referenced studies.
To our knowledge, one other study also used MR-guided bi-opsy specimens as a reference standard for diffusion-weighted im-aging ADC.10 Our significant mADC differences between degreesand 1 and 2 of prostatitis and most transition zone cancers confirmedthe results of the latter study, in which a significant ADC differencebetween prostatitis and low-GG transition zone cancer was found(P G 0.001).10
Inflammatory infiltrates in prostatitis lead to an increased cel-lular density and may therefore decrease ADC.21 In a healthy transitionzone, a large ADC variation may be present because of higher vari-ability of the different tissue components with different cellular den-sities. Stromal benign prostatic hyperplasia has a more compact andmore homogeneous cell density and is known to have lower ADCvalues (1.27� 10j3 mm2/s) compared with glandular benign prostatichyperplasia (1.73 � 10j3 mm2/s).8 Therefore, a relative local ADCdecrease due to focal chronic prostatitis may not be discerned in thetransition zone. The higher the degree of the prostatitis is, the lower themADC is, as is depicted in Figure 4. Despite only including 5 coreswith a degree 2 of prostatitis, we showed that, because of a lower ADC
TABLE 2. Patient Characteristics
Characteristic Median (IQR)Patients With Cores Containing
TZ Cancer (n = 52)Patients With Cores ContainingNon-cancerous TZ (n = 53) P†
Age (yr) 67 (63Y71) 66 (61Y68) n.a.
PSA (ng/mL) 19.6 (11.4Y26.6) 14.0 (9.5Y20.6) 0.02*
Prostate volume (mL) 43.0 (35.0Y62.0) 57.3 (55.1Y107.6) G0.001
PSA density (ng/mL/mL) 0.42 (0.28Y0.70) 0.19 (0.09Y0.32) G0.001*
Previous TRUS biopsy sessions 3 (2Y4) 2 (1Y3) n.a.
Included MRGB cores per patient 2 (1Y2) 2 (2Y3) n.a.
MRGB cancer core length (mm) 12.0 (11.0Y14.0) n.a. n.a.
MRGB total core length (mm) 15.0 (12.0Y16.0) 13.0 (10.3Y15.0) 0.008
Gleason score‡
2+4 1 n.a. n.a.
3+2 10 n.a. n.a.
3+3 14 n.a. n.a.
3+4 18 n.a. n.a.
3+5 5 n.a. n.a.
4+3 9 n.a. n.a.
4+4 6 n.a. n.a.
4+5 13 n.a. n.a.
5+3 3 n.a. n.a.
5+4 7 n.a. n.a.
5+5 1 n.a. n.a.
Gleason score is given on a core basis because some patients had different Gleason scores in different magnetic resonanceYguided prostate biopsy cores.
Continuous parametric variables were compared with independent t tests.
A significance level of P G 0.05 was used.
*The Mann-Whitney test was used to evaluate the differences between continuous non-parametric variables.
†P values between the patients with magnetic resonanceYguided prostate biopsy specimens containing transition zone cancer versus the patients with magneticresonanceYguided prostate biopsy specimens containing non-cancerous transition zone.
‡Numbers of MR guided biopsy core specimens.
IQR indicates interquartile range; MRGB, magnetic resonanceYguided prostate biopsy; n.a., not applicable; PSA, prostate-specific antigen; TRUS, transrectalultrasound.
Hoeks et al Investigative Radiology & Volume 48, Number 10, October 2013
698 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

in a higher degree of prostatitis, a significant mADC difference be-tween the magnetic resonanceYguided prostate biopsy (MRGB) spec-imen cores with degree 2 prostatitis (mADC, 1.12 � 10j3 mm2/s)versus the primary GG 4Y5 and secondary GG 2Y3 transition zonecancers and vice versa (histopathological categories II and III) did notexist (P = 0.06Y0.09). This significant mADC difference did exist forcores with a degree 1 prostatitis (mADC, 1.05� 10j3 mm2/s), which hada higher ADC compared with any transition zone cancer (P G 0.0001).
Our mean mADCs for primary GG 2Y3 and 4Y5 cancer-containing cores (mean [SD], 0.84Y0.85 � 10j3mm2/s and 0.77Y0.86 �10j3mm2/s, respectively) differ from the ADC values reported forprimary GG 2Y3 versus 4Y5 cancers upon radical prostatectomy by
Kobus et al13 (respectively, minimum 25th percentiles of 0.51Y0.95 �10j3mm2/s and 0.61� 10j3mm2/s) and by Kitajima et al22 (respectively,mean ADC of 1.12Y1.21 � 10j3mm2/s and 0.64Y1.01 � 10j3mm2/s).Kobus et al13 reported minimum 25th percentiles, which are lowercompared with our mean 50th percentiles, whereas Kitajima et al22
reported mean ADC values, which may be higher compared with ourmedian values. Next to differences in image to histopathology corre-lation between studies, these ADC differences may have been causedby the application of b-values of 0 and 1000 s/mm2 by Kitajima et al22
versus the applied b-values of 50, 500, and 800 s/mm2 in our study.22
Our AUC value of 0.84 for discriminating transition zonecancer from non-cancerous transition zone tissue agrees with the
FIGURE 3. Projection of annotated cores on the MR-guided biopsy ADC maps. A 63-year-old man with a PSA of 20 ng/mLand 1 previous negative transrectal ultrasound biopsy session. During the MR-guided biopsy, a GG 3+5 prostate cancer wasdetected in 100 volume percent of the depicted core. A, The annotated MR-guided biopsy core on a transversal T2-weightedbalanced gradient echo confirmation scan (TR, 4.48milliseconds; TE, 2.24milliseconds). B, Gradient echo image (A) fused withthe diffusion-weighted imaging ADC map in color. The diffusion-weighted imaging ADC values within the annotatedMR-guided biopsy core (black demarcations) are visible. In the middle of the core, the ADC was 0.4 � 103 mm2/s, whereas, atboth core ends, the ADC was 0.7Y0.9 � 10j3 mm2/s. The color scale of the ADC map on image B and C was as follows:red-pink, 0.135 � 10j3 mm2/s or less; dark blue, 0.852 � 10j3 mm2/s or less; light blue, 1.330 � 10j3 mm2/s or less; andgreen-yellow 1.750 � 10j3 mm2/s or less. C, The same annotated MR-guided biopsy core (black demarcations) over a sagittalprojection of the diffusion-weighted imaging ADC map. D, Hematoxylin and eosinYstained tissue section of the prostatebiopsy core with indications of GG at scanning magnification of �10. This core is corresponding to the core in A to C. I to III,Higher magnifications of the different areas indicated by the boxes (�20). The lower ADC value in the middle of the coreagrees with a primary GG 5 situated in between lower GGs.
Investigative Radiology & Volume 48, Number 10, October 2013 Validation of ADC in the Prostate Transition Zone
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 699
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

results reported by Kitajima et al22 (0.87Y0.89) and by Oto et al8
(0.78Y0.99). To our knowledge, our study is the first to report AUCvalues for mADC differentiation of prostatitis from the transitionzone cancer (0.84) and from the noncancerous transition zone (0.56).
Our moderate AUC value for differentiation of a primary GG4Y5 versus a GG 2Y3 in MR-guided biopsy cores acquired in thetransition zone (0.62) is comparable with AUC values of 0.61 to0.62 found by Verma et al12 for differentiation of a radical prosta-tectomy specimen Gleason score higher than 6 versus 6 or lower inthe transition zone using both mean ADC and tumor volume. Ourmoderate accuracy in differentiating primary GG 4 from GG 3cancer cores was caused by mADC overlap between the GGs,which, itself, may have been the result of mADC variations. mADCvariations may have been caused by the inclusion of a secondaryGG core tissue and by inter-patient and intra-patient mADC varia-tions.24 Variation of the amount of noncancerous tissue in thecancer-containing cores did not cause significant mADC differ-ences when we analyzed mADC for the primary GG 3 and 4 tran-sition zone cancer cores with a cancer core length of 10Ye12, 912Ye 15,and 915 mm (P = 0.22Y0.87).
This study has limitations. First, our results are subject to se-lection bias. Because we used a cancer core length of 10 mm andgreater, we excluded smaller cancers from our retrospective analysis.However, because MR-guided biopsy is performed in a larger patientgroup compared with patients undergoing surgery, still, less patientselection bias is present compared with radical prostatectomy speci-mens. Second, as mentioned, including secondary GG tissue thatwas different from the primary GG may have reduced accuracy of ourdifferentiation of primary GG 4 from primary GG 3 cancers. Al-though present in a smaller volume compared with the primary GG,the presence of adifferent secondary GG causes variation and overlapin ADCs for primary GG. As mentioned earlier, our results clearlyshowed a larger ADC difference and less overlap for a secondary GG,which was identical to the primary GG compared with a secondaryGG, which was different from the primary GG. Furthermore, inac-curacies in our measurements may have been caused by possibleneedle, prostate, or patient movement in the short time gap betweenthe actual biopsy and the acquisition of confirmation scans.25 Despiteour manual registration of confirmation scans to the diffusion-weighted imaging ADC maps, some variation in measurements dueto patient movement throughout the whole MR-guided biopsy pro-cedure may still have occurred. Third, we took into account a larger
apparent size of the needle tip artifact on the MR images comparedwith the actual needle size. However, we did not adjust this measurefor the angle of needle insertion with the static field (B0) of the MRscanner, which may influence the apparent needle size.26 Fourth,because our reference standard MR-guided biopsy was based ontargeting MR imaging cancer-suspicious regions, selection bias mayhave occurred. Cancer-suspicious regions may have a relativelyhigher cell density, resulting in lower ADC values compared with thewhole transition zone.
To clinically apply our detected mADC differences for dif-ferent histopathology entities in the transition zone, variation of ADCvalues should be reduced. In a recent study, correction for interpatientvariation of healthy peripheral zone ADC significantly improved(P = 0.04; AUC, 0.91Y0.96) differentiation of GG 4 and/or 5 versusGG 2 and/or 3 cancers.27 This principle may also be applied forcancers located in the transition zone.
In conclusion, mADC values can differentiate the transitionzone cancer from the non-cancerous transition zone and from degree1 and, sometimes, from degree 2 prostatitis. However, because ofmADC overlap between the histopathology categories, mADC hada poor accuracy to distinguish between different subcategories oftransition zone cancer primary and secondary GG and cannot be used
FIGURE 5. Scatterplot of median ADC values in annotatedROIs on MRGB needle artifacts versus MRGB core specimenGleason scores. ADC indicates apparent diffusion coefficent;MRGB, MR guided biopsy; ROI, region of interest.
FIGURE 4. Box plot of median ADC values in annotated ROIs onMRGB needle artifacts versus MRGB core specimen histopathologycategories. Values in between 1.5 to 3 box lengths above the upper box margin are presented as outliers with a circle. GG indicatesGleason grade; mADC, median apparent diffusion coefficient values; MRGB, MR guided biopsy; TZ, prostate transition zone.
Hoeks et al Investigative Radiology & Volume 48, Number 10, October 2013
700 www.investigativeradiology.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

for differentiation between non-cancerous transition zone with andwithout prostatitis. Diffusion-weighted MR imaging ADC maytherefore contribute in the detection of transition zone cancers, butas a single functional MR imaging technique, diffusion-weighted MRimaging has a moderate diagnostic accuracy in separating higherversus lower GG components in transition zone cancers and in dif-ferentiating prostatitis from non-cancerous transition zone.
REFERENCES1. Ferlay J. Estimates of worldwide burden of cancer in 2008: GLOBOCAN
2008. Int J Cancer. 2010;127:2893Y2917.2. McNeal JE, Redwine EA, Freiha FS, et al. Zonal distribution of prostatic ad-
enocarcinoma. Correlation with histologic pattern and direction of spread. AmJ Surg Pathol. 1988;12:897Y906.
3. Patel V, Merrick GS, Allen ZA, et al. The incidence of transition zone prostatecancer diagnosed by transperineal template-guided mapping biopsy: implica-tions for treatment planning. Urology. 2011;77:1148Y1152.
4. Hambrock T, Somford DM, Hoeks C, et al. Magnetic resonance imagingguided prostate biopsy in men with repeat negative biopsies and increasedprostate specific antigen. J Urol. 2010;183:520Y527.
5. Hoeks CM, Schouten MG, Bomers JG, et al. Three-tesla magnetic resonance-guided prostate biopsy in men with increased prostate-specific antigen andrepeated, negative, random, systematic, transrectal ultrasound biopsies: detec-tion of clinically significant prostate cancers. Eur Urol. 2012;62:902Y909.
6. Scheenen TW, Futterer J, Weiland E, et al. Discriminating cancer fromnoncancer tissue in the prostate by 3-dimensional proton magnetic resonancespectroscopic imaging: a prospective multicenter validation study. InvestRadiol. 2010;45:121Y125.
7. Akin O, Sala E, Moskowitz CS, et al. Transition zone prostate cancers: features,detection, localization, and staging at endorectal MR imaging. Radiology.2006;239:784Y792.
8. Oto A, Kayhan A, Jiang Y, et al. Prostate cancer: differentiation of central glandcancer from benign prostatic hyperplasia by using diffusion-weighted anddynamic contrast-enhanced MR imaging. Radiology. 2010;257:715Y723.
9. Delongchamps NB, de la Roza H, Chanan V, et al. Evaluation of prostatitis inautopsied prostatesVis chronic inflammation more associated with benignprostatic hyperplasia or cancer? J Urol. 2008;179:1736Y1740.
10. Nagel K, Schouten MG, Hambrock T, et al. Differentiation of prostatitis andprostate cancer using diffusion weighted imaging and MR guided biopsy at 3T.Radiology. 2013 [Epub ahead of print].
11. Augustin H, Erbersdobler A, Hammerer PG, et al. Prostate cancers in thetransition zone: part 2; clinical aspects. BJU Int. 2004;94:1226Y1229.
12. Verma S, Rajesh A, Morales H, et al. Assessment of aggressiveness of prostatecancer: correlation of apparent diffusion coefficient with histologic grade afterradical prostatectomy. AJR Am J Roentgenol. 2011;196:374Y381.
13. Kobus T, Vos PC, Hambrock T, et al. Prostate cancer aggressiveness: in vivoassessment of MR spectroscopy and diffusion-weighted imaging at 3 T. Ra-diology. 2012;265:457Y467.
14. Selnaes KM, Heerschap A, Jensen LR, et al. Peripheral zone prostate cancerlocalization by multiparametric magnetic resonance at 3T: unbiased canceridentification by matching to histopathology. Invest Radiol. 2012;47:624Y633.
15. Lambregts DM, Beets GL, Maas M, et al. Tumour ADC measurements in rectalcancer: effect of ROI methods on ADC values and interobserver variability.Eur Radiol. 2011;21:2567Y2574.
16. Hambrock T, Hoeks C, Hulsbergen-van de KC, et al. Prospective assessment ofprostate cancer aggressiveness using 3-T diffusion-weighted magnetic reso-nance imaging-guided biopsies versus a systematic 10-core transrectal ultra-sound prostate biopsy cohort. Eur Urol. 2012;61:177Y184.
17. Somford DM, Hambrock T, Hulsbergen van de Kaa CA, et al. Initial experiencewith identifying high-grade prostate cancer using diffusion-weighted MR im-aging (DWI) in patients with a Gleason score e3+3=6 upon schematic TRUS-guided biopsy: a radical prostatectomy correlated series. Invest Radiol. 2012;47:153Y158.
18. Vos PC, Hambrock T, Hulsbergen-van de Kaa CA, et al. Computerized analysisof prostate lesions in the peripheral zone using dynamic contrast enhancedMRI. Med Phys. 2008;35:888Y899.
19. Hambrock T, Futterer JJ, Huisman HJ, et al. Thirty-two-channel coil 3T mag-netic resonance-guided biopsies of prostate tumor suspicious regions identifiedon multimodality 3T magnetic resonance imaging: technique and feasibility.Invest Radiol. 2008;43:686Y694.
20. Epstein JI, Allsbrook WC Jr, Amin MB, et al. The 2005 International Society ofUrological Pathology (ISUP) Consensus Conference on Gleason Grading ofProstatic Carcinoma. Am J Surg Pathol. 2005;29:1228Y1242.
21. Nickel JC, True LD, Krieger JN, et al. Consensus development of a histo-pathological classification system for chronic prostatic inflammation. BJU Int.2001;87:797Y805.
22. Kitajima K, Takahashi S, Ueno Y, et al. Clinical utility of apparent diffusioncoefficient values obtained using high b-value when diagnosing prostate cancerusing 3 tesla MRI: comparison between ultra-high b-value (2000 s/mm2) andstandard high b-value (1000 s/mm2). J Magn Reson Imaging. 2012;36:198Y205.
23. Yoshizako T, Wada A, Hayashi T, et al. Usefulness of diffusion-weighted im-aging and dynamic contrast-enhanced magnetic resonance imaging in the di-agnosis of prostate transition-zone cancer. Acta Radiol. 2008;49:1207Y1213.
24. Hosseinzadeh K, Schwarz SD. Endorectal diffusion-weighted imaging inprostate cancer to differentiate malignant and benign peripheral zone tissue. JMagn Reson Imaging. 2004;20:654Y661.
25. Pondman KM, Futterer JJ, ten HB, et al. MR-guided biopsy of the prostate: anoverview of techniques and a systematic review. Eur Urol. 2008;54:517Y527.
26. Schouten MG, Ansems J, Renema WK, et al. The accuracy and safety aspectsof a novel robotic needle guide manipulator to perform transrectal prostatebiopsies. Med Phys. 2010;37:4744Y4750.
27. Litjens G, Hambrock T, Hulsbergen-van de Kaa CA, et al. The effect of inter-patient normal peripheral zone apparent diffusion coefficient variation on theprediction of prostate cancer aggressiveness. Radiology. 2012;265:260Y266.
Investigative Radiology & Volume 48, Number 10, October 2013 Validation of ADC in the Prostate Transition Zone
* 2013 Lippincott Williams & Wilkins www.investigativeradiology.com 701
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

![KAA 507 – Surface and Thermal Analysis [Analisis Permukaan ...web.usm.my/chem/pastyear/files/KAA507_Sem1_2008_2009.pdf · [KAA 507] UNIVERSITI SAINS MALAYSIA First Semester Examination](https://static.fdocuments.us/doc/165x107/5acea13c7f8b9a1d328c08d3/kaa-507-surface-and-thermal-analysis-analisis-permukaan-webusmmychempastyearfileskaa507sem120082009pdfkaa.jpg)


![KAA 503 – Molecular Spectroscopy [Spektroskopi Molekul]web.usm.my/chem/pastyear/files/KAA503_Sem1_2010_2011.pdf · KAA 503 – Molecular Spectroscopy [Spektroskopi Molekul] Duration](https://static.fdocuments.us/doc/165x107/5a73714a7f8b9a98538e90f3/kaa-503-molecular-spectroscopy-spektroskopi-molekulwebusmmychempastyearfileskaa503sem120102011pdf.jpg)













