Differential Diagnosis in Psychosis and...
23
www.mghcme.org Differential Diagnosis in Psychosis and Autism Abigail Donovan, MD Director, First Episode and Early Psychosis Program Associate Director, Acute Psychiatry Service Massachusetts General Hospital Assistant Professor of Psychiatry Harvard Medical School
Transcript of Differential Diagnosis in Psychosis and...

www.mghcme.org
Differential Diagnosis in Psychosis and Autism
Abigail Donovan, MD Director, First Episode and Early Psychosis Program
Associate Director, Acute Psychiatry Service Massachusetts General Hospital Assistant Professor of Psychiatry
Harvard Medical School

www.mghcme.org
Disclosures
Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest
to disclose.
www.mghcme.org
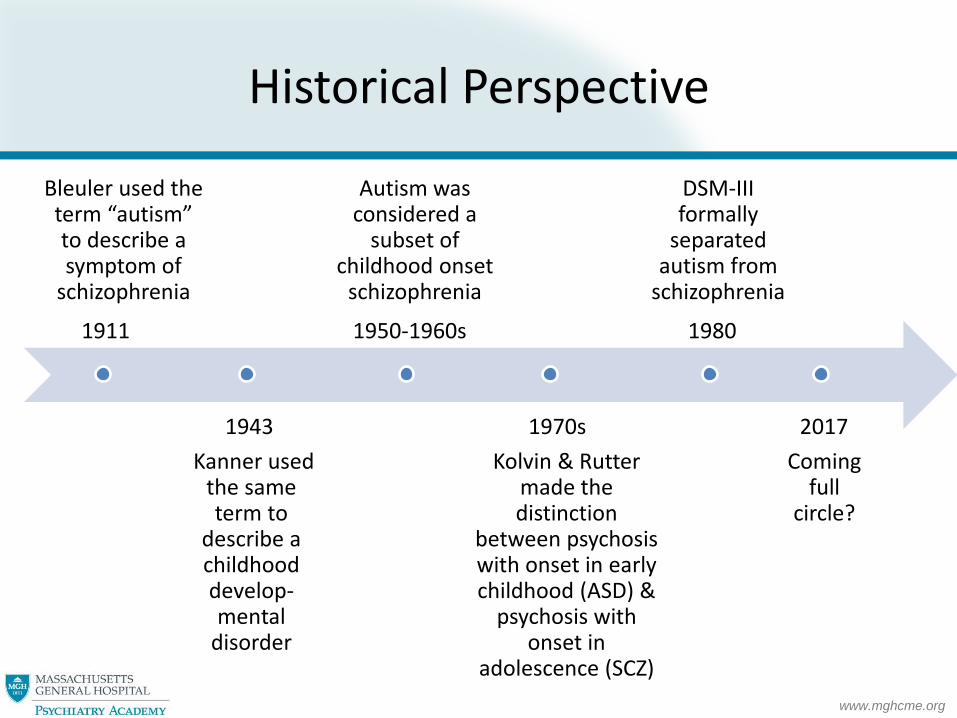
Historical Perspective
Bleuler used the term “autism” to describe a symptom of
schizophrenia
Kanner used the same term to
describe a childhood develop-mental
disorder
Autism was considered a
subset of childhood onset
schizophrenia
Kolvin & Rutter made the distinction
between psychosis with onset in early childhood (ASD) &
psychosis with onset in
adolescence (SCZ)
DSM-III formally
separated autism from
schizophrenia
Coming full
circle?
1911
1943
1950-1960s
1970s
1980
2017
www.mghcme.org
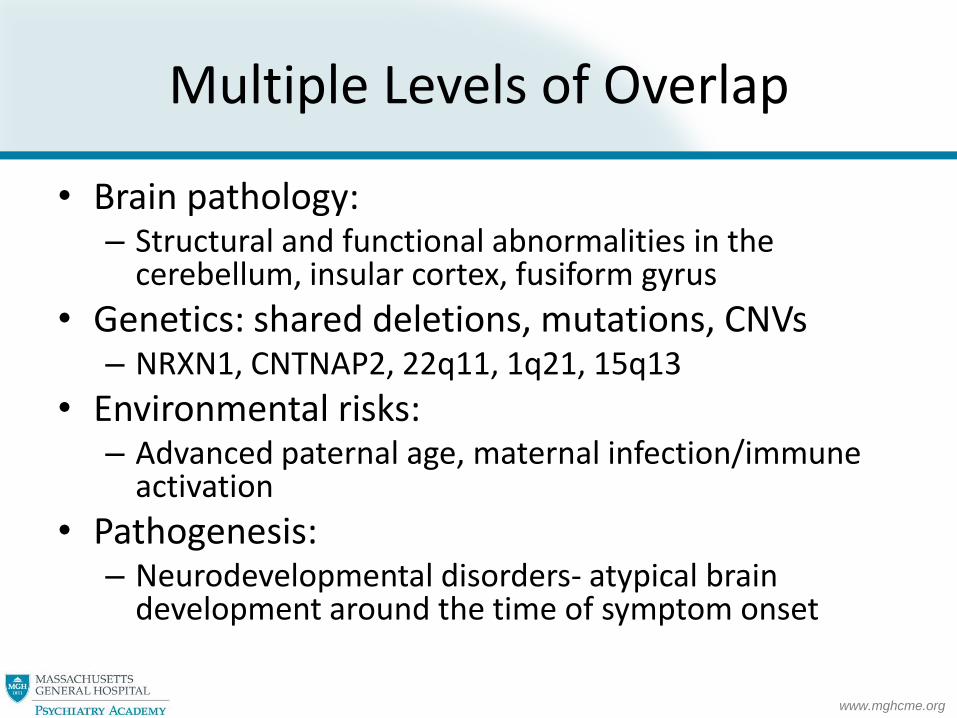
Multiple Levels of Overlap
• Brain pathology: – Structural and functional abnormalities in the
cerebellum, insular cortex, fusiform gyrus
• Genetics: shared deletions, mutations, CNVs – NRXN1, CNTNAP2, 22q11, 1q21, 15q13
• Environmental risks: – Advanced paternal age, maternal infection/immune
activation
• Pathogenesis: – Neurodevelopmental disorders- atypical brain
development around the time of symptom onset

www.mghcme.org
Symptom Overlap
• Social deficits – Both disorders have impaired social cognition,
including Theory of Mind1
• Cognitive deficits – Abstract reasoning, working memory, processing
speed, executive function2
• Language deficits – Decreased verbal communication/output3,
pragmatic language deficits
1. Lugnegard et al. Schiz Res 2013; 277-284. 2. Goldstein et al. Arch Clin Neuropsychology 2002; 461-475. 3. Fitzgerald Clinical Neuropsychiatry 2012; 171-176.

www.mghcme.org
Comorbidity
• Reports on prevalence are variable
• Patients with ASD:
– with psychosis: 3-16%1-4
– with schizophrenia: 0.6-3.4%5,6
• Patients with schizophrenia:
– with PDD NOS: 20-50%7-9
– with ASD: 0-11%7-9
1. Larsen Eur Child Adolesc Psychiatry 1997;181-90. 2. Wing Psychol Med 1981;115-29. 3. Wolff Psychol Med 1980;85-100. 4. Tsakanikos J Autism Dev Disord 2006;1123-9. 5. Volkmar Am J Psychiatry 1991;1705-7. 6. Mouridsen J Psychiatr Pract 2008;5-12. 7. Solomn Schizophrenia Research 2011;146-51. 8. Waris Eur Child Adolesc Psychiatry 2013;217-223. 9. Rapoport J Am Acad Child Adolesc Psychiatry 2009; 10-18.

www.mghcme.org
Psychosis
SCZ
ASD

www.mghcme.org
Is it really psychosis?
• Patients with ASD may report symptoms that sound psychotic, but really aren’t
– Auditory hallucinations
– Paranoia
www.mghcme.org
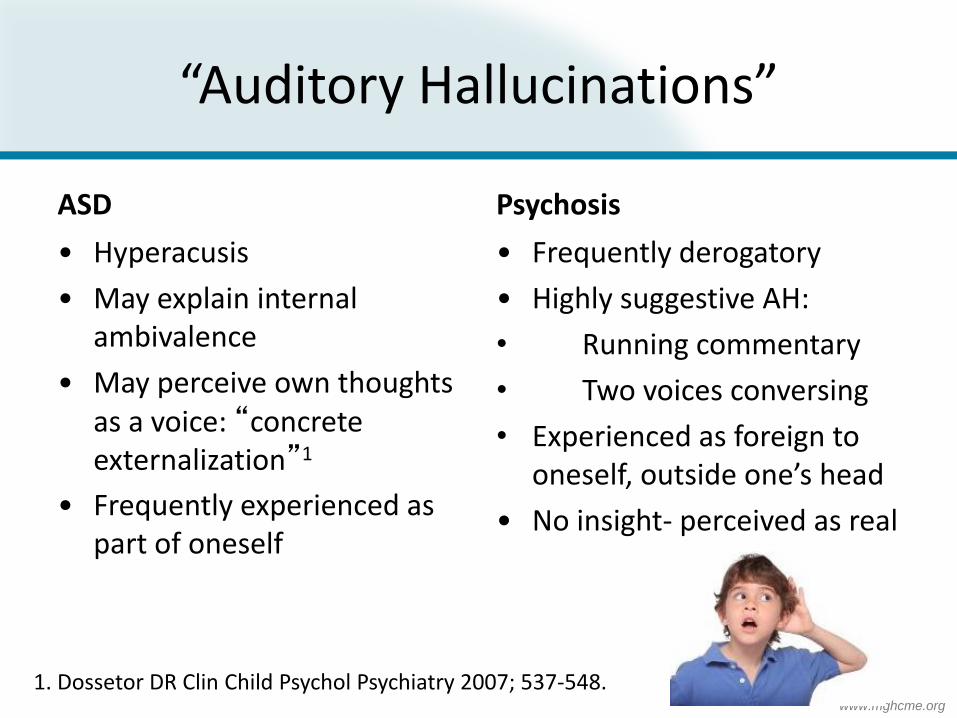
“Auditory Hallucinations”
ASD
• Hyperacusis
• May explain internal ambivalence
• May perceive own thoughts as a voice: “concrete externalization”1
• Frequently experienced as part of oneself
Psychosis
• Frequently derogatory
• Highly suggestive AH:
• Running commentary
• Two voices conversing
• Experienced as foreign to oneself, outside one’s head
• No insight- perceived as real
1. Dossetor DR Clin Child Psychol Psychiatry 2007; 537-548.
www.mghcme.org
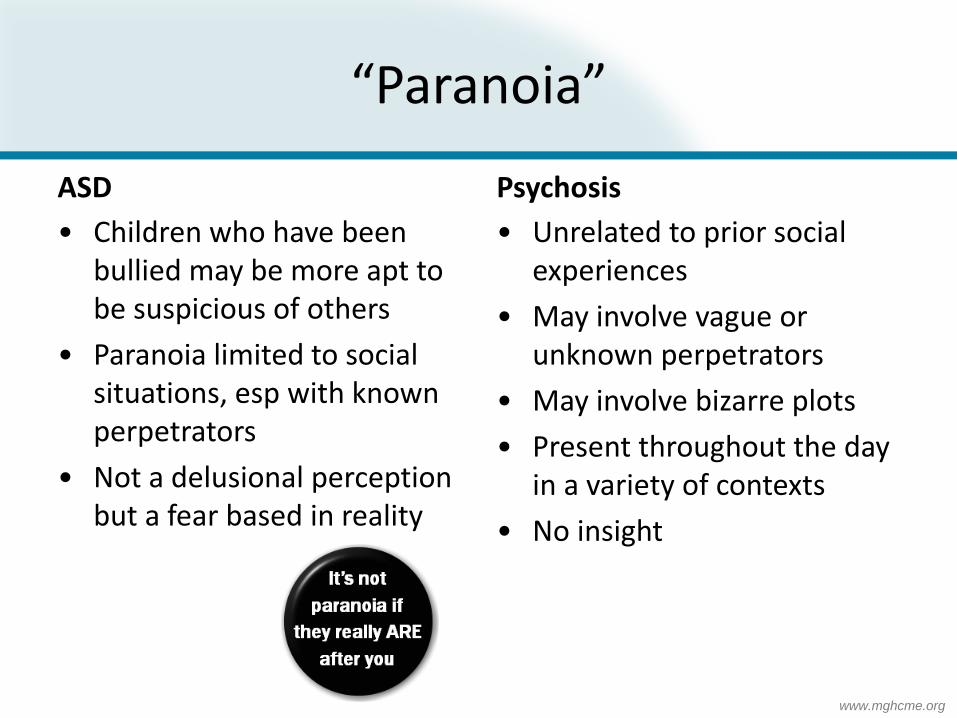
“Paranoia”
ASD
• Children who have been bullied may be more apt to be suspicious of others
• Paranoia limited to social situations, esp with known perpetrators
• Not a delusional perception but a fear based in reality
Psychosis
• Unrelated to prior social experiences
• May involve vague or unknown perpetrators
• May involve bizarre plots
• Present throughout the day in a variety of contexts
• No insight

www.mghcme.org
Psychosis
SCZ
ASD
www.mghcme.org
Case
• 11 yo f diagnosed with ASD at age 6
• Started 5th grade at her public school with an IEP
• Experiencing profound academic stress
• Parents going through contentious divorce
• She developed AH of several voices mocking her, experienced as real, present 24/7
• Symptoms resolved with intensive treatment, risperidone and modified IEP, and she was able to return to school at prior level of functioning

www.mghcme.org
ASD with Psychosis
• Premorbid ASD - chronic social, cognitive and behavioral deficits
• Followed by later emergence of new psychotic symptoms – Brief reactive psychosis- stress induced psychosis
– Mood disorder with psychotic features
• Accompanied by functional impairment – Typically mild to moderate
– Always time limited

www.mghcme.org
ASD with Psychosis
• Stress-induced psychosis in ASD1
– “Micro-episodes” of psychosis: brief and transient
– Triggered by stress, resolve when stress is absent
• ASD patients are at 3x greater risk for having isolated psychotic symptoms2
• ASD patients display psychotic symptoms with stress or anxiety3
1. Tantam D et al. Br Med Bull 2009; 41-62. 2. Sullivan et al. J Amer Acad Child Adolesc Psychiatry 2013; 806-814. 3. Solomon et al. J Autism Dev Disord 2008; 1474-1484.
www.mghcme.org
Psychosis
SCZ
ASD

www.mghcme.org
Is it ASD or Schizophrenia?
Features of ASD
Impairment in non-verbal
communication
Lack emotional reciprocity
Stereotyped language
Features of Schizophrenia
Flat affect
Social withdrawal
Alogia
Cochran DM et al. Child Adolesc Psychiatric Clin N Am; 2013:609-627.
www.mghcme.org
How do you distinguish?
• Developmental history is critical
• ASD symptoms are present from an early age
– May become more prominent over time
• SCZ symptoms emerge after grossly normal development
– Followed by gradual, persistent functional decline
– Then emergence of positive symptoms

www.mghcme.org
Social Deficits
ASD
• Present from early childhood
• May be socially motivated, but clumsy
• May be verbal but inappropriate
Schizophrenia
• Develop after a period of normal functioning
• Lack of social motivation
• Withdrawal from friends and family
• Paucity of speech/content
www.mghcme.org
Case
• 24 yo male with ASD, limited social function, good academic function
• Just started first year of business school- developed difficulty with concentration and memory
• Withdrew from family and few friends • Developed PI (being followed by CIA) and AH • Calling police several times a day, eventually
hospitalized • Stabilized on olanzapine but continued to have
functional impairment and unable to return to school

www.mghcme.org
ASD with Schizophrenia
• Rare but real
• Premorbid ASD - chronic social, cognitive and behavioral deficits
• Followed later in development by further functional decline (social and cognitive)
• Then, emergence of new psychosis – True AH, paranoia, delusions, disorganization
– DSM 5: “prominent delusions or hallucinations must be present for one month”

www.mghcme.org
ASD with Schizophrenia
Key aspects of differential (with brief reactive psychosis):
• Onset may be influenced by stress, but symptoms are not solely stress dependent
• Functional impairment
– Additional impairment from baseline- typically severe
– Chronic- patients do not return to baseline

www.mghcme.org
Conclusion
• Substantial symptom overlap and true comorbidity between ASD, psychosis and schizophrenia
• Accurate diagnosis can be made by:
– Careful, detailed symptom history
– Developmental history- timing of onset of symptoms
– Functional assessment over time

www.mghcme.org
Thank you!