
Dietary Supplements To Prevent Recurrent UTI: The Evidence · UTI and to develop methods of...
35
Kris Cvach Fellow Female Pelvic Medicine and Reconstructive Surgery UBC 31st March 2010 Dietary supplements to prevent recurrent UTI: The evidence Outline • Epidemiology of UTI • Pathophysiology of UTI • Supplements - definition • Cranberry • Probiotics • Other supplements • Recommendations
Transcript of Dietary Supplements To Prevent Recurrent UTI: The Evidence · UTI and to develop methods of...

Kris CvachFellow
Female Pelvic Medicine and Reconstructive SurgeryUBC
31st March 2010
Dietary supplements to prevent recurrent UTI:
The evidence
Outline• Epidemiology of UTI
• Pathophysiology of UTI
• Supplements - definition
• Cranberry
• Probiotics
•Other supplements
• Recommendations
Burden of Disease
• Estimated annual cost of UTI in both men and women is $US 3.5 billion *
•♀:♂ 50:1
• Lifetime risk of a single UTI episode in women 50%
*Griebling, TL.J Urol 2005;174:1281-87 & 1288-94
Pathophysiology

•Colonisation of periurethral tissue with uropathogenic organisms
•Ascension of these organisms up urethra into bladder
•E. coli causes over 95% of UTIs*
Huertas AX, et al. Cochrane Database Syst Rev, 2009(2)
•Adhesion to uroepithelial cells
•Type I fimbriae bind to mannose-like receptors
•P-type fimbriae bind to oligosaccharide receptors
THE LANCET • Vol 353 • January 2, 1999 7
COMMENTARY
Prevention of recurrent urinary-tractinfections in womenAcute cystitis is the commonest form of urinary-tractinfection (UTI). Women are disproportionately affected,the annual incidence among young women in the USAbeing 0·5–0·7 episodes per person-year.1 Furthermore,about 25% of women who have had an episode of acutecystitis develop frequent recurrent infections.2 Sincerecurrent UTIs are a substantial burden to society in costof diagnosis and treatment, timelost from work, and morbidity,research efforts aim to elucidatefactors predisposing to recurrentUTI and to develop methods ofpreventing these infections. Theseefforts are especially important forwomen with recurrent UTI,because most of them have nodemonstrable underlying abnor-malities of the urinary tract.
At each step in the pathogenesisof UTI, key host or bacterialfactors influence susceptibility toUTI. A critical step is colonisationof the vaginal and periurethralmucosa with the infectinguropathogen, most commonlyEscherichia coli. At the cellular level,bacterial factors that influence
initial adherence between uropathogen and urogenitalmucosa include the expression of pili such as P fimbriae,which are over-represented among isolates from patientswith cystitis,3 and type I fimbriae, which are present in allE coli and probably have a role in promoting initialcolonisation.4 Little difference has been found invirulence characteristics between E coli infecting womenwith sporadic UTI and those infecting women withrecurrent infection.5 However, the receptor repertoire forthese organisms on host urogenital cells seems toinfluence susceptibility. Compared with women withoutrecurrent infection, those with such infections have longerdurations of vaginal colonisation with uropathogenic E coli and three-fold more E coli adhering to vaginal,buccal, and voided uroepithelial cells.6
In addition, women with recurrent UTI are three tofour times more likely to be non-secretors of ABH blood-group antigens than are women without recurrentinfections.7 The secretor gene encodes one of the manyglycosyltransferases that determine the carbohydratecomposition of cell-surface glycoproteins and glyco-sphingolipids, some of which also serve as binding sitesfor uropathogenic E coli.8 The vaginal epithelium of non-secretors, but not that of secretors, expresses twoextended-chain glycosphingolipids that bind uro-pathogenic E coli more avidly than do other glyco-sphingolipids.9,10 Thus, genetically determined differencesin urogenital cell-receptor availability and bindingcharacteristics may influence susceptibility to recurrentUTI.
Only certain features of the mucosal host response tobacterial attachment and infection have been investigated.Interleukins 6 and 8 are elaborated during UTI,presumably by the uroepithelium.11 In women with acutecystitis, systemic immune responses are very weak, andlocal antibody responses are short-lived. Much moredetailed knowledge of the role of the host immuneresponse in sporadic and recurrent UTI is needed for thedevelopment of vaccines against these infections.Urogenital tissues contain antimicrobial peptides,12 buttheir role in UTI is unknown.
The normal microbial ecology of the vagina may alsobe an important factor in the prevention of UTI. Severalfactors that disrupt the normal flora promote thedevelopment of a uropathogen-predominant vaginal floraas well as a propensity to recurrent UTI. Such factors
include the use of spermicidesforcontraception,13 the recent use of!-lactam antimicrobials,14 and the postmenopausal stateunsupplemented by exogenousoestrogen.15 Anatomical andbehavioural factors in the patientalso influence the likelihood ofrecurrent UTI, although some ofthese have been investigated onlywith respect to risk of sporadicUTI. Anomalies of urinary tractstructure, urinary stones, as wellas functional abnormalitiesassociated with ageing, such asreduced bladder tone, post-voidresidual urine, and bladder oruterine prolapse, may predisposeto infection. Among behaviouralrisks, sexual intercourse is a
suspect that the group of patients in whom the kidneybearing the primary tumour was not removed probablydid not fare very well, and that those who benefited mostwere those whose primary lesion had been removedsurgically and who had a very low metastatic tumourburden. Primary lesions rarely respond to biologicaltherapy.
Although interferon alfa may be effective in a fewpatients with metastatic renal-cell carcinoma, andalthough when given as a single agent it has areproducible antitumour effect in renal-cell carcinoma,the effect is modest. Thus, the study of novel treatmentstrategies and identification of new agents with betterantitumour activity remain the highest priority for clinicaltrials in patients with metastatic renal-cell carcinoma.
Robert AmatoMD Anderson Cancer Center, Houston, TX 77030, USA
1 1998 Cancer Statistics. Atlanta, Georgia: American Cancer Society.
2 Nanus DM, Pfeffer LM, Bander NH, et al. Antiproliferative andantitumor effects of alpha-interferon in renal cell carcinomas:correlation with the expression of a kidney-associated differentiationglycoprotein. Cancer Res 1990; 50: 4190–94.
3 Wirth MP. Immunotherapy for metastatic renal cell carcinoma.Urol Clin North Am 1993; 20: 283–95.
4 Minasian LM, Motzer RJ, Gluck L, Mazumdar M,Vlamis V, KrownSE. Interferon-alpha 2a in advanced renal cell carcinoma: treatmentresults and survival in 159 patients with long-term follow-up. J ClinOncol 1993; 11: 1368–75.
5 Fossa SE, Martinelli G, Ott U, et al: Recombinant interferon alpha-a2with or without vinblastine in metastatic renal cell carcinoma: resultsof a European multi-center phase III study. Ann Oncol 1992; 3:301-05.
6 Neidhart JA, Anderson SA, Harris JE, et al.Vinblastine fails toimprove response of renal cancer to interferon-alpha-a1: how responserate with patients with pulmonary metastases. J Clin Oncol 1991; 9:832–36.
7 Krown SE. Interferon treatment of renal cell carcinoma: current statusand future prospects. Cancer 1987; 59: 647–51.
Piliated uropathogenic Escherichia coliTube-like structure is the flagellum, which seems to havebeen detached from the bacterium.Magnification x20 000, reduced by about 40%.
CFe
nnel
l, C
Wob
be, J
CLa
ra
Copyright © 1999. All rights reserved.
Stapleton S. Lancet 1999;353:7-8
Introduction
Urinary tract infections (UTIs) affect nearly 13 millionwomen annually in the United States alone and can result insignificant costs and morbidity [1–5]. Uropathogenic Escher-ichia coli (UPEC) is the predominant causative agent,responsible for up to 85% of community-acquired infections[6,7]. The majority of UTIs are thought to arise whenuropathogens present in the fecal flora colonize the vaginalintroitus, ascend into the bladder, and initiate a hostresponse manifested by secretion of cytokines, pyuria, andthe onset of symptoms [8].
Women have a 25% chance of experiencing a recurrentUTI within six months [9] of an index episode and a 44%chance of recurrence within one year [10] despite appro-priate therapy of the initial infection and negative follow-upurine cultures. Over one-half of all recurrent episodes ofacute uncomplicated cystitis are caused by the same bacterialstrain as the initial infection [11,12]. As with initial UTIs, it iswidely thought that recurrences occur through reascensionand reinoculation of the bladder lumen by a UPEC strain thathas persisted in the periurethral or fecal flora following theprevious UTI.
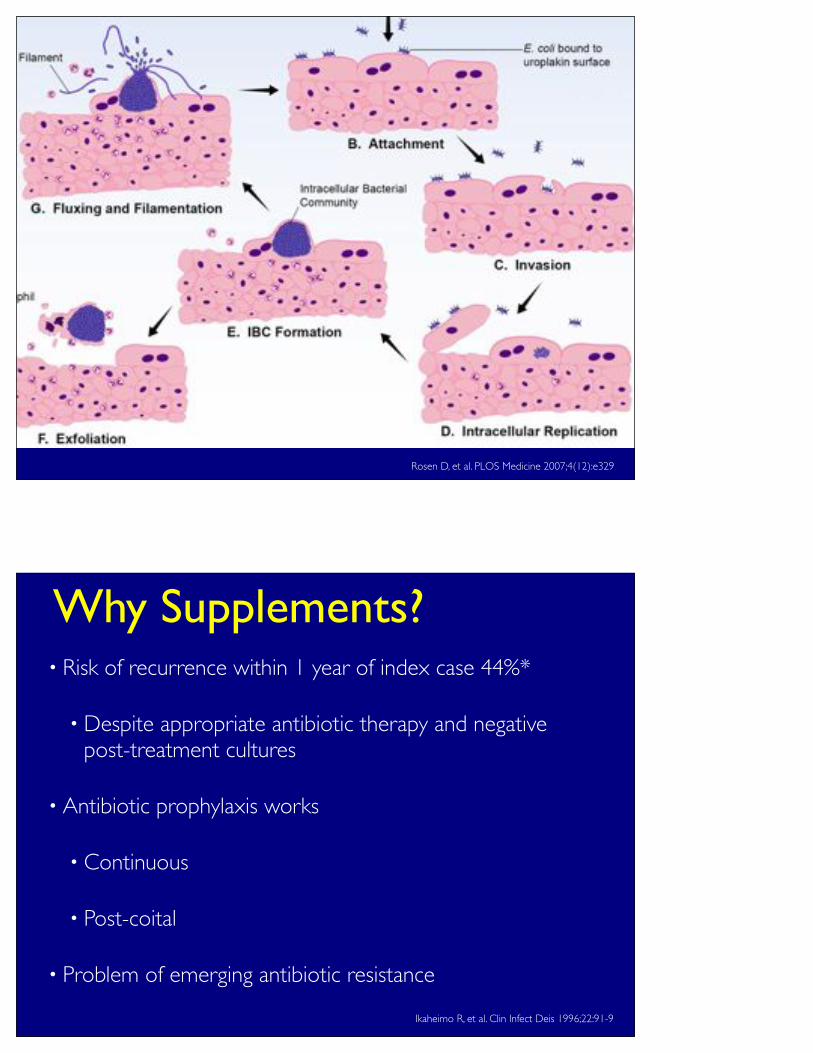
Recently, it was demonstrated in a murine model of cystitisthat UPEC utilize a multistep pathogenic cycle duringinfection in which they progress through an intracellularniche within the bladder (Figure 1) [13–15]. UPEC expressadhesive fibers known as type 1 pili that mediate binding toand invasion of luminal facet cells of the bladder [16–18]. Thisintracellular niche is conducive to UPEC replication andformation of intracellular bacterial communities (IBCs) withbiofilm-like properties [13]. IBCs exist only transiently beforethe bacteria dissociate and migrate out of the facet cell, manyadopting a filamentous morphology [14]. The filamentousUPEC avoid engulfment by neutrophils, thus allowing themto reinvade the urothelium [14]. Upon infection, the hostexfoliates and expels bladder epithelial cells into the urine.Ultimately, UPEC are able to form quiescent intracellularreservoirs composed of small rosettes of bacteria withinLamp-1–positive endocytic vesicles that can persist forseveral weeks protected from antibiotics and, presumably,undetected by the host immune system [15,19,20]. Epithelialturnover may cause the quiescent bacteria to revert to anactively replicative form, leading to recurrent bacteriuria[19].To date, an intracellular bacterial pathway has not been
Figure 1. UPEC IBC Pathogenic Pathway Observed in the Murine Cystitis Model
The bladder urothelium (A) is a pseudostratified transitional epithelium lined by large facet cells. These cells have an apical asymmetric unit membranecontaining uroplakins that help form the impermeable bladder barrier and also serve as receptors for UPEC. Bacteria introduced into the bladder adhereto the bladder surface via type 1 pili (B). Upon attachment, bacteria are able to invade (C) and replicate (D) within the facet cell cytoplasm. UPEC formlarge biofilm-like IBCs within these cells (E). Ultimately the bacteria flux out of their intracellular niche (G), some adopting a filamentous morphology;they then adhere to other host cells and re-enter the infectious cycle. During this process, infected urothelial cells are sloughed into the urine (F) andneutrophils are recruited to the site of infection.doi:10.1371/journal.pmed.0040329.g001
PLoS Medicine | www.plosmedicine.org December 2007 | Volume 4 | Issue 12 | e3291950
Intracellular Niche during UTI Pathogenesis
Rosen D, et al. PLOS Medicine 2007;4(12):e329
Why Supplements?• Risk of recurrence within 1 year of index case 44%*
•Despite appropriate antibiotic therapy and negative post-treatment cultures
• Antibiotic prophylaxis works
• Continuous
• Post-coital
• Problem of emerging antibiotic resistance
Ikaheimo R, et al. Clin Infect Deis 1996;22:91-9

What is a supplement?
• “a plant or a plant material, an alga, a bacterium, a fungus or a non-human animal material, vitamins, an amino acid, an essential fatty acid, a mineral or a probiotic” and “that supplements the diet.”
•Definition varies by country
Natural Health Products Directorate 2003. www.hc-sc.gc.ca/hpfb-dgpsa/nhpd-dpsn/index_e.html
According to Health Canada:
FDA Dietary Supplement Health and Education act (DHSEA) 1994
• “manufacturer is responsible for ensuring that its dietary supplement products are safe before they are marketed”
• Unlike drug products that must be proven safe and effective for their intended use before marketing, there are no provisions in the law for FDA to "approve" dietary supplements for safety or effectiveness before they reach the consumer”

•Other than the manufacturer's responsibility to ensure safety, there are no rules that limit a serving size or the amount of a nutrient in any form of dietary supplements. This decision is made by the manufacturer and does not require FDA review or approval.
FDA 2010
•Dietary supplements must comply with “good manufacturing practices”, and be produced under "controls that result in a consistent product free of contamination, with accurate labeling"
•Report to the FDA "all serious dietary supplement related adverse events"
Supplements

•Cranberry
•Probiotics
•Other - Uva ursi, Forskolin, Juniper, Golden Rod, D-Mannose
Cranberry
•Vaccinium macrocarpon
•Historically used for disorders of stomach, blood, liver ; fever, scurvy
•1800’s treatment for bladder disorders
•Ocean Spray earnings 2008 US$1.9 Billion
•90% of world’s annual production from MA, NJ, WI (USA); 8% from Quebec and BC
•95% of berries are used for juice
•5% left whole

• Initial studies focused on the potential role of hippuric acid
•Quinic acid in cranberry is a precursor of hippuric acid, a known potent bacteriostatic agent
• requires ingestion of 240ml of cranberry juice at 80% concentration*
• Subsequent studies did not reproduce these results
Kinney AB, et al. Nurs Res 1979;28:287-90
Mechanism of Action
Introduction
Urinary tract infections (UTIs) affect nearly 13 millionwomen annually in the United States alone and can result insignificant costs and morbidity [1–5]. Uropathogenic Escher-ichia coli (UPEC) is the predominant causative agent,responsible for up to 85% of community-acquired infections[6,7]. The majority of UTIs are thought to arise whenuropathogens present in the fecal flora colonize the vaginalintroitus, ascend into the bladder, and initiate a hostresponse manifested by secretion of cytokines, pyuria, andthe onset of symptoms [8].
Women have a 25% chance of experiencing a recurrentUTI within six months [9] of an index episode and a 44%chance of recurrence within one year [10] despite appro-priate therapy of the initial infection and negative follow-upurine cultures. Over one-half of all recurrent episodes ofacute uncomplicated cystitis are caused by the same bacterialstrain as the initial infection [11,12]. As with initial UTIs, it iswidely thought that recurrences occur through reascensionand reinoculation of the bladder lumen by a UPEC strain thathas persisted in the periurethral or fecal flora following theprevious UTI.
Recently, it was demonstrated in a murine model of cystitisthat UPEC utilize a multistep pathogenic cycle duringinfection in which they progress through an intracellularniche within the bladder (Figure 1) [13–15]. UPEC expressadhesive fibers known as type 1 pili that mediate binding toand invasion of luminal facet cells of the bladder [16–18]. Thisintracellular niche is conducive to UPEC replication andformation of intracellular bacterial communities (IBCs) withbiofilm-like properties [13]. IBCs exist only transiently beforethe bacteria dissociate and migrate out of the facet cell, manyadopting a filamentous morphology [14]. The filamentousUPEC avoid engulfment by neutrophils, thus allowing themto reinvade the urothelium [14]. Upon infection, the hostexfoliates and expels bladder epithelial cells into the urine.Ultimately, UPEC are able to form quiescent intracellularreservoirs composed of small rosettes of bacteria withinLamp-1–positive endocytic vesicles that can persist forseveral weeks protected from antibiotics and, presumably,undetected by the host immune system [15,19,20]. Epithelialturnover may cause the quiescent bacteria to revert to anactively replicative form, leading to recurrent bacteriuria[19].To date, an intracellular bacterial pathway has not been
Figure 1. UPEC IBC Pathogenic Pathway Observed in the Murine Cystitis Model
The bladder urothelium (A) is a pseudostratified transitional epithelium lined by large facet cells. These cells have an apical asymmetric unit membranecontaining uroplakins that help form the impermeable bladder barrier and also serve as receptors for UPEC. Bacteria introduced into the bladder adhereto the bladder surface via type 1 pili (B). Upon attachment, bacteria are able to invade (C) and replicate (D) within the facet cell cytoplasm. UPEC formlarge biofilm-like IBCs within these cells (E). Ultimately the bacteria flux out of their intracellular niche (G), some adopting a filamentous morphology;they then adhere to other host cells and re-enter the infectious cycle. During this process, infected urothelial cells are sloughed into the urine (F) andneutrophils are recruited to the site of infection.doi:10.1371/journal.pmed.0040329.g001
PLoS Medicine | www.plosmedicine.org December 2007 | Volume 4 | Issue 12 | e3291950
Intracellular Niche during UTI Pathogenesis
CRANBERRYX
•Anti-adherance properties - human studies showed 68% adherence inhibition after ingestion of cranberry juice cocktail*
*Sobota AE. J Urol 1984;131:1013-16

•Fructose - inhibits Type 1 (mannose-specific) fimbriated E. coli in vitro*, but no in vivo studies to support this
*Foo LY, et al. Phytochemistry 2000;54:173-81
•Proanthocyanidins (PACs)
• Flavonoid compounds in tannin-rich foods
•Conjugated dimers and trimers of anthocyanidins
•PACs derived from cranberry exhibit A-type linkages
• superior anti-adhesion properties compared to B-type linkages found in PACs from apples, grapes, green tea*
*Howell AB, et al. Phytochemistry 2005;66:2281-91
• Inhibit adhesion of P fimbriated E. coli (as well as Proteus, Klebsiella, Enterbacter, Pseudomonas)
•Competetively binding to fimbriae or reduce adhesion capabilities by altering P-fimbriae
•Cranberry PAC levels related to:
•pH
•Temperature
•Light
•Not well studied in humans
•Peak urinary PAC concentrations seen 3-6 hours after intake; completed by 12 hours
•Approximately 5% of oral dose excreted in urine
•Colonic excretion - potential role for selection of non-pathogenic E coli in gut
Pharmacokinetics of PACs
Formulations
•Pure juice - pH <2.5
•Cranberry juice cocktail - most common 25-27%, sweetened
•Tablets, capsules

•Cochrane review 2008*
•10 RCTs - 5 cross-over, 5 parallel group
•7 juice vs placebo or water
•2 tablets vs placebo
•1 juice vs tablets vs placebo
*Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database of Systematic Reviews 2008(1)
The Evidence
•Cochrane review 2008
•4 studies included in meta-analysis
•UTI incidence at 12 months RR 0.66 (0.47-0.92)
•Women with recurrent UTI had 39% risk reduction
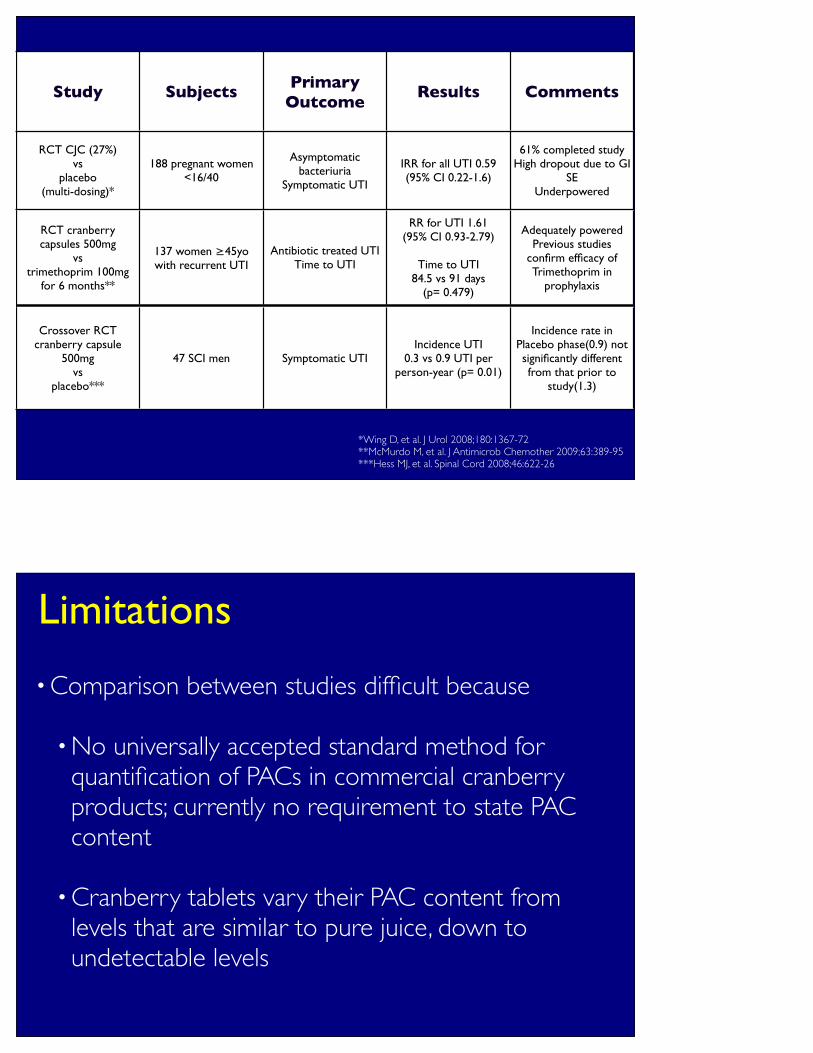
Study Subjects Primary Outcome
Results Comments
RCT CJC (27%) vs
placebo(multi-dosing)*
188 pregnant women <16/40
Asymptomatic bacteriuria
Symptomatic UTI
IRR for all UTI 0.59 (95% CI 0.22-1.6)
61% completed studyHigh dropout due to GI
SEUnderpowered
RCT cranberry capsules 500mg
vs trimethoprim 100mg
for 6 months**
137 women ≥45yo with recurrent UTI
Antibiotic treated UTITime to UTI
RR for UTI 1.61 (95% CI 0.93-2.79)
Time to UTI 84.5 vs 91 days
(p= 0.479)
Adequately poweredPrevious studies
confirm efficacy of Trimethoprim in
prophylaxis
Crossover RCT cranberry capsule
500mg vs
placebo***
47 SCI men Symptomatic UTIIncidence UTI
0.3 vs 0.9 UTI per person-year (p= 0.01)
Incidence rate in Placebo phase(0.9) not significantly different from that prior to
study(1.3)
*Wing D, et al. J Urol 2008;180:1367-72**McMurdo M, et al. J Antimicrob Chemother 2009;63:389-95***Hess MJ, et al. Spinal Cord 2008;46:622-26
•Comparison between studies difficult because
•No universally accepted standard method for quantification of PACs in commercial cranberry products; currently no requirement to state PAC content
•Cranberry tablets vary their PAC content from levels that are similar to pure juice, down to undetectable levels
Limitations
•No objective measure of adherence to treatment protocol (measurement of urinary output of PACs)
•No systematic evaluation of the frequency of dose-administration or dose-response relationship
•Different definitions of UTI - asymptomatic bacteriuria, symptomatic UTI, colony count
•Varying study duration
•High withdrawal rates - up to 47% (GI symptoms)
Adverse Events
•Allergic reaction
•GI upset 10-40%

Adverse Events• Interaction with warfarin
•May inhibit activity of CYP2C9
•Case reports detailing increased INR in patients taking cranberry products concurrently
•2 RCTs do not support this
•Current recommendation
•Close monitoring of INR in patients taking warfarin and cranberry
•Nephrolithiasis
•Cranberry contains high levels of oxalate
•Conflicting results in literature
• Increased urinary excretion of oxalate, but also of magnesium, potassium*
•Decreased excretion of oxalate and phosphate, increased citrate excretion**
*Terris MK, et al. Urology 2001;57:26-9**McHarg TA, et al. BJU Int 2003;92:765-68

Probiotics
What are they?
• “live microorganisms which when administered in adequate amounts confer a health benefit to the host” (FAO/WHO criteria for probiotic)
• bacteria, yeasts
• dairy products, probiotic fortified foods
• freeze-dried form - tablets, capsules, powders
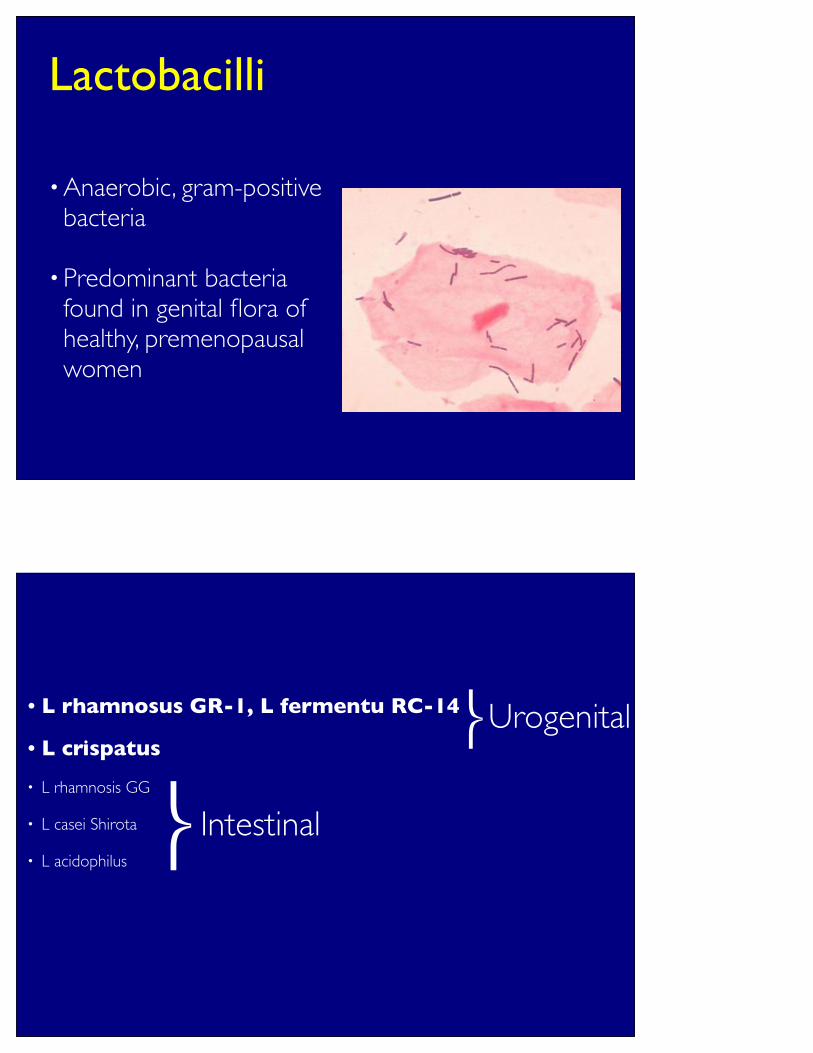
•Anaerobic, gram-positive bacteria
•Predominant bacteria found in genital flora of healthy, premenopausal women
Lactobacilli
• L rhamnosus GR-1, L fermentu RC-14
• L crispatus
• L rhamnosis GG
• L casei Shirota
• L acidophilus!
!
Intestinal
Urogenital
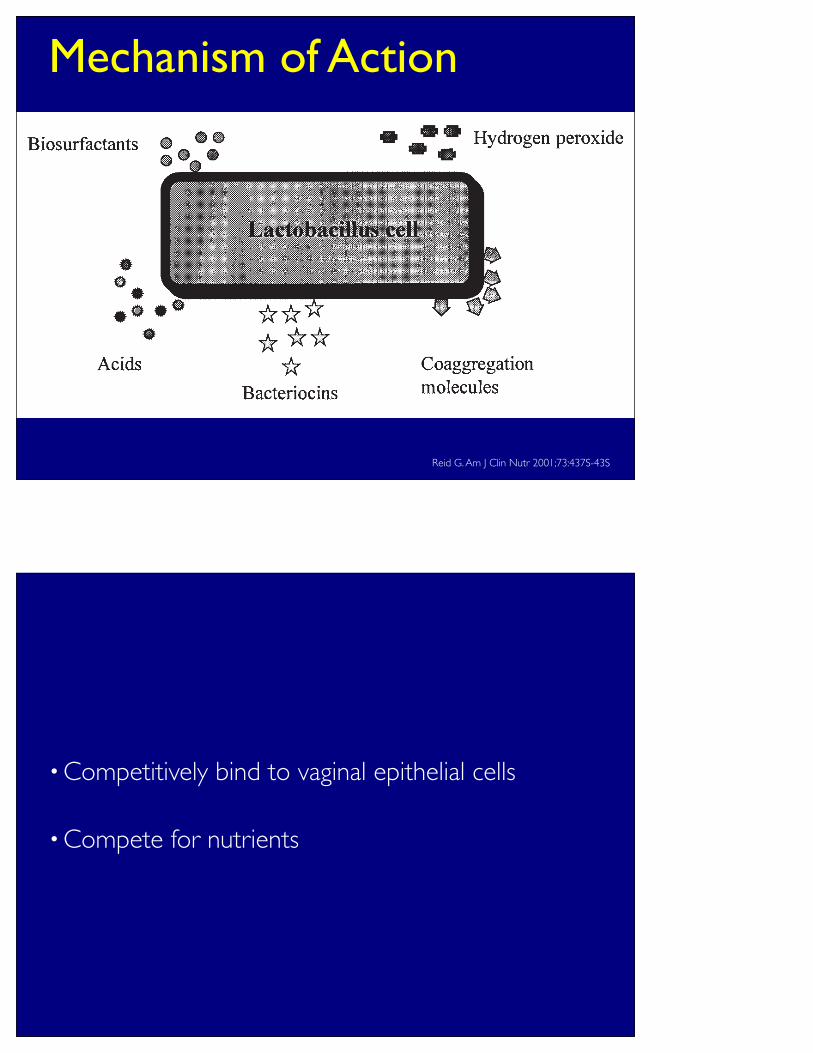
Mechanism of Action
growth requirement. They prefer an acidic environment and helpcreate one by producing lactic and other acids. In general, lacto-bacilli have not been associated with disease and for > 100 yhave been regarded as nonpathogenic members of the intestinaland urogenital floras (65).
Lactobacilli have long been of interest to the dairy andagriculture industries (66, 67), although over the past century,studies in relation to human health were sporadic and ofteninconclusive. Some examples can be found in which lactic acidbacteria have been used to treat or prevent infections of theintestinal and genital tracts with different degrees of success(68–71). However, there has been failure in identifying the prop-erties of lactobacilli required to prevent and treat disease; indetermining the optimal dosage, duration, and mode of lacto-bacilli delivery; and including a placebo in the study. Studieshave failed to recover and document lactobacilli properly andshow their mechanisms of action.
A further problem with probiotic therapeutics is their reliabil-ity. In one study, this was highlighted by the fact that thecontents of some health food products were inconsistent and dif-ferent from those stated on the labels (72). More recently, wediscovered that some health food products in Canada appear tocontain ! 1 common Lactobacillus strain, apparently identical toATCC strain 21052, and that US and Canadian products containLactobacillus plantarum, although its presence is not stated onthe food label (73).
In more recent years, the use of probiotics per se and lacto-bacilli specifically has received greater attention as an alterna-tive, inexpensive, and natural remedy to restore and maintainhealth (74–79). Two strains, Lactobacillus GG (ATCC 53103)and Lactobacillus rhamnosus GR-1 appear to be effective at col-onizing and protecting the intestine (80–86) and urogenital tract(87–91), respectively, against microbial infection.
There is one obvious question: what properties do thesestrains possess that make them effective probiotic agents? Theanswer is not fully known, but some common denominatorsappear to exist, namely the ability to adhere to and colonize tis-sues and the capacity to inhibit the pathogenesis of disease-causing organisms (Figure 2). Another question can be raised: dowe expect an exogenous probiotic strain to colonize the gastro-intestinal and urogenital tracts of a given person for a long timeand even become part of the normal flora, replacing or coexist-ing with the endogenous lactobacilli organisms? Or is the aim to
substitute the endogenous bacteria only while the normal flora isrepressed (eg, as a result of antibiotic therapy) (92)? Again, noclear answers are available.
To more fully ascertain which properties are required by lac-tobacilli to protect the host, we recommend a series of extensivemicrobiological, physico-chemical, and molecular biology method-ologies (89, 93–97). It appears that a given strain of Lactobacil-lus can express several, but not necessarily all, of the known keyfactors and be able to compete in the urogenital microenviron-ment. For example, lactobacilli can use many mechanisms toadhere to surfaces, such as electrostatic, hydrophobic, hydrophilic,capsular, and fimbrial mechanisms (95, 98–102): in the urogeni-tal tract, hydrophilic L. rhamnosus GR-1 and hydrophobic Lac-tobacillus fermentum B-54 both colonize (91). Some strains canbind better to intestinal cells and inhibit pathogen adhesion (103,104), but they may not be able to effectively inhibit growth ofuropathogens (94).
Before commencing more human studies, L. rhamnosus GR-1was found to be the best of a group of 34 Lactobacillus strains iso-lated from dairy, poultry, health food, and human sources, withrespect to adhesion to squamous and transitional uroepithelialcells, competitive exclusion of pathogens, and production ofinhibitors of uropathogen growth (94). In 1995 another character-istic of lactobacilli was discovered that appeared to be importantin conferring probiotic action against uropathogens. Fifteenstrains were found to produce biosurfactant (105). The substanceor substances adsorbed to surfaces and inhibited the initial adhe-sion of E. faecalis by 70%. The crude substance was analyzed andwas found to contain proteins and carbohydrates. Amino acidanalysis of hydrolyzed material from strain Lactobacillus aci-dophilus RC-14 showed a high alanine content compared with lessactive strains. The activity is not due to lipoteichoic acid or glyco-syldiglycerides or to factors such as acid or bacteriocins, whichinhibit bacterial growth. Sodium dodecyl sulphate-polyacrylamidegel electrophoresis showed a variety of proteins with molecularmasses of from 14.4 to 140 kDa (106, 107). The biosurfactantactivity is resistant to trypsin and pepsin, and sensitive to !-amylaseand lysozyme, and resistant to 75 oC degree heating. The antiad-hesive molecules produced by certain lactobacilli hold promise forapplication to many human sites where pathogens attach, colonize,and confer disease. More recently, the activity was shown to affecta broad range of pathogens (Table 1) (108) and an active compo-nent was found to be a collagen binding protein (109). The
UROGENITAL TRACT PROTECTION BY PROBIOTICS 439S
FIGURE 2. Byproducts of lactobacillus metabolism that have an antagonistic effect against urinary and vaginal pathogens. The biosurfactantsinhibit adhesion; the acids, bacteriocins, and hydrogen peroxide inhibit growth; and the coaggregation molecules block the spread of the pathogens.
by o
n M
arc
h 3
0, 2
01
0
ww
w.a
jcn
.org
Do
wn
loa
de
d fro
m
Reid G. Am J Clin Nutr 2001;73:437S-43S
•Competitively bind to vaginal epithelial cells
•Compete for nutrients

Role in Genitourinary health•Women with history of recurrent UTI have altered vaginal flora
• reduced Lactobacillus species
•prolonged vaginal colonization with uropathogens, predominantly E coli*
•So, theoretically use of probiotics restores normal vaginal flora, inhibits overgrowth of uropathogens and prevents recurrent UTIs
*Gupta K, et al. J Infect Dis 1998;178:446-50
The Evidence!
•L. rhamnosus GR-1/L fermentum RC-14
•L crispatus
L rhamnosus GR-1/L fermentum RC-14
•L rhamnosus GR-1
• adheres to vaginal epithelial cells
•bacteriostatic properties
•L fermentum RC-14
•produces surface-active proteins, preventing adhesion of uropathogens to vaginal epithelial cells
Reid G, et al. J Urol 1987;138:330-35McGroarty JA, et al. Can J Microbiol 1988;34:974-98
Heinemann C, et al. FEMS Microbiol Lett 2000;190:177-80
• For probiotics to be clinically effective vaginal colonization has to occur irrespective of route of administration
•Both oral and vaginal administration has been shown to result in conversion of abnormal to normal vaginal flora
•This change is shown to persist following cessation of probiotic administration
Cadieux P, et al. JAMA 2002;287:1940-41Reid G, et al. FEMS Immunol Med Microbiol 2001;32:37-41Reid G, et al. FEMS Immunol Med Microbiol 2003;35:131-34

Study Subjects Primary Outcome
Results Comments
RCT L rham PV weekly
vs LGF for 12 months*
55 premenopausal women UTI incidence
No intergroup difference in UTI
incidenceUTI I 6.0 per patient-
year pre-study to 1.6/1.3 with treament
(p=0.001)
RCT norfloxacin or TMP/SMX for 3 days
then L rham PV twice
weekly x 4 doses then 1 PV at 2 months
vs placebo**
41 premenopausal women with culture-
confirmed UTI
Bacterial eradication UTI recurrence
No difference between antibiotic groups
No significant difference in rec UTI
between L rham (21%) and placebo
(47%)
Study underpowered
RCT L rham# PV twice weekly
vs placebo for 26
weeks***
47 premenopausal women UTI incidence
IRR 1.41 (95%CI 0.88-1.98)
Strain not demonstrated to
inhibit E coli in vitro
*Reid G, et al. Microecol Ther 1995;23:32-45**Reid G, et al. Clin Ther 1992;14:11-16
***Baerheim A, et al. Scand J Prim Health Care 1994;12:239-43
L crispatus
•Adheres strongly to vaginal epithelial cells
•Lowers pH of vaginal environment
•Before and after study of 9 women with history of recurrent UTI*
•L crispatus PV 2 nightly for 1 year
• Incidence of UTI pre vs during treatment 5.0 per patient year to 1.3 per patient year (p<0.01)
*Uehara S, et al. Int J Antimicrob Agents 2006;28:s30-4
•Systemic infection
•Lactobacillus infection is rare
•When it occurs usually in patients with underlying chronic disease or immunocompromise
Adverse Events
Boyle RJ, et al. Am J Clin Nutr 2006;83:1256-64
Other Supplements
Uva Ursi (Bearberry)

•Species of Arctostaphylos
•Woody shrub high altitudes circumpolar
•Leaves are proposed therapeutic portion based on arbutoside content
Uva Ursi (Bearberry)
Hydroquinone (glucuronidated)
Hydroquinone glucuronide
Hydroquinone glucuronide in ph>7
Hydroquinone (proposed antimicrobial agent)
Arbutoside
Glusose + aglycone hydroquinone
Yarnell E. World J Urol 2002;20:285-93

• In Vitro studies
• Increases hydrophobicity of E coli, decreases ability of bacteria to adhere to urothelial cells*
•Antimicrobial activity against S aureus, S typhi, C albicans**
*Turi M, et al. APMIS 1997;105;956-62**Jahodar L, et al. Ceska Slov Farm 1985;34:174-78
• In Vivo study
•RCT 57 women with recurrent UTI*
•Uva-E (Arbutin & Dandelion) 3 tabs tid vs placebo for 1 month
• F/u 12 months
•UTI 0% vs 23% (p<0.05)
•No reported side effects
*Larsson B, et al. Curr Ther Res 1993;53:441-43
•Concerns regarding long term use of Uva Ursi relate to hydroquinone
•Excessive doses: GI upset, tinnitus, liver dysfunction
•Mutagenic/carcinogenic effects
• Interaction with CYP450 isoenzymes
•Bull’s eye maculopathy
•Avoid in pregnancy, lactation, children < 12yo
Forskolin
•Extract from Colues forskohlii
•Basic science studies
•Elevator of Cyclic AMP
•May have a role in decreasing IBCs
•No human RCT to support use

Juniper Berries
•Conifers
•Over 60 species In Northern hemisphere
•Leaves contain antimicrobial and diuretic properties of terpenoids (animal studies)
•Human clinical trials not reported on efficacy or safety in UTI
Yarnell E World J Urol 2002;20:285-93
Golden Rod
Flowering perennial (Solidago spp)North American Native

•1 Double blind RCT
• Increase urine flow
•No single active ingredient isolated, mechanisms still undetermined
•Side effects: allergic reaction, renal failure
Bone K Br. J Phytoth. 1994
•Natural sugar
•Competitively blocks adhesion of E Coli
•Large literature in vivo and animal models
•Lacking human RCT
D Mannose

Current Trials
Cranberry
•Current NIH/NCCAM* funded studies addressing limitations of published studies
Quality control of the productDose responseDocumentation of complianceUrine quantification of PACsTracking of symptomatic UTI’sBacterial analysis (virulence)
*National Centre for Complementary and Alternative Medicine
Cranberry
www.clinicaltrials.gov Accessed March 12, 2010
• Effects of Cranberry-Containing Products in Women with Recurrent Urinary Tract Infection
• Cranberry for Prevention of Urinary Tract Infections in MS Patients
• Effect of Cranberry Capsules on Urinary Infection Rates in Spinal Cord Injured Patients During Post Acute Rehabilitation
• Cranberry Juice for the Prevention of Recurrent Urinary Tract Infections
• Dosing Study of Cranberry Capsules for the Prevention of Bacteriuria in Nursing Home Residents
• Cranberry Juice for Treatment of Urinary Tract Infections
Probiotics• Probiotics as a Prophylactic Aid in Women with Recurrent Urinary Tract
Infections
• Bacteriuria Eradication through Probiotics
• Intravaginal LACTIN-V for Prevention of Recurrent Urinary Tract Infection
• Probiotics for Girls with Recurring Urinary Tract Infections
• Probiotics in Girls With Spina Bifida
• Low Dose Estriol with Lactobacilli Treatment for Preventing Recurrent Urinary Tract Infection in Postmenopausal Women
www.clinicaltrials.gov Accessed March 12, 2010
Conclusions
•Cranberry
•Few high quality studies
•Conflicting results regarding efficacy of cranberry products in UTI prevention - No standard method for quantification of PACs in commercial products

•No consensus as to juice vs capsules, dose or dosing schedule
•Use diluted pure cranberry juice (1:4) 60ml bid
•Probiotics
•Specific for genitourinary tract (L Rhamnosus/L fermentum)

•National Centre for Complementary and Alternative Medicine (NCCAM) nccam.nih.gov
•The Office of Dietary Supplements ods.od.nih.gov
•Health Canada Natural health productswww.hc-sc.gc.ca/dhp-mps/prodnatur/index-eng.php
Useful Resources
Questions


















