MManagement of frailty as a new anagement of frailty as a ...
Dietary practices in patients with chronic kidney
disease not yet on maintenance dialysis:
What are the relevant components?
3rd International Conference of
European Renal Nutrition Working Group of ERA-EDTA
T. Alp Ikizler, MD
Vanderbilt University Medical Center
Considerations for Nutritional Requirements in Kidney Disease
Protein intake
CKD - Progression
ESRD - Protein wasting
CKD and ESRD
Na/K/PO4 (HTN; Hyperkalemia; Bone Mineral Disorders)
Metabolic Disorders (Inflammation; Oxidative Stress)
Calorie intake
CKD - Obesity; Insulin Resistance
ESRD - Wasting-Obesity Paradox

1. Sanches FM, et al. Am J Kidney Dis. 2008;52:66-73.
2. Campbell KL, et al. Clin Nutr. 2008;27:537-544.
PEW is present in 12-18% of stages 3 and 4 CKD patients
2 studies reported PEW prevalence up to 18% in patients with early-stage CKD (3 and 4)
• 18% prevalence in CKD stages 3 and 4 patients in Brazil using SGA (n=122, age 55 ±11)1
• 12% prevalence in CKD stage 4 patents in Australia, using SGA (n=56, age 70 ±14)2

Appetite decreases as CKD progresses
Carrero JJ. J Ren Nutr. 2009;19:10-15.
eGFR<90 mL/min
Retention of uremic toxins – suppress
appetite Increased dialysis dose improves feeding behavior
Dialysisbegins
Transplantation
Starts when eGFR<10-25% of normal
eGFR<60 mL/min
Ap
pet
ite
eGFR<30 mL/min
eGFR<15 mL/min
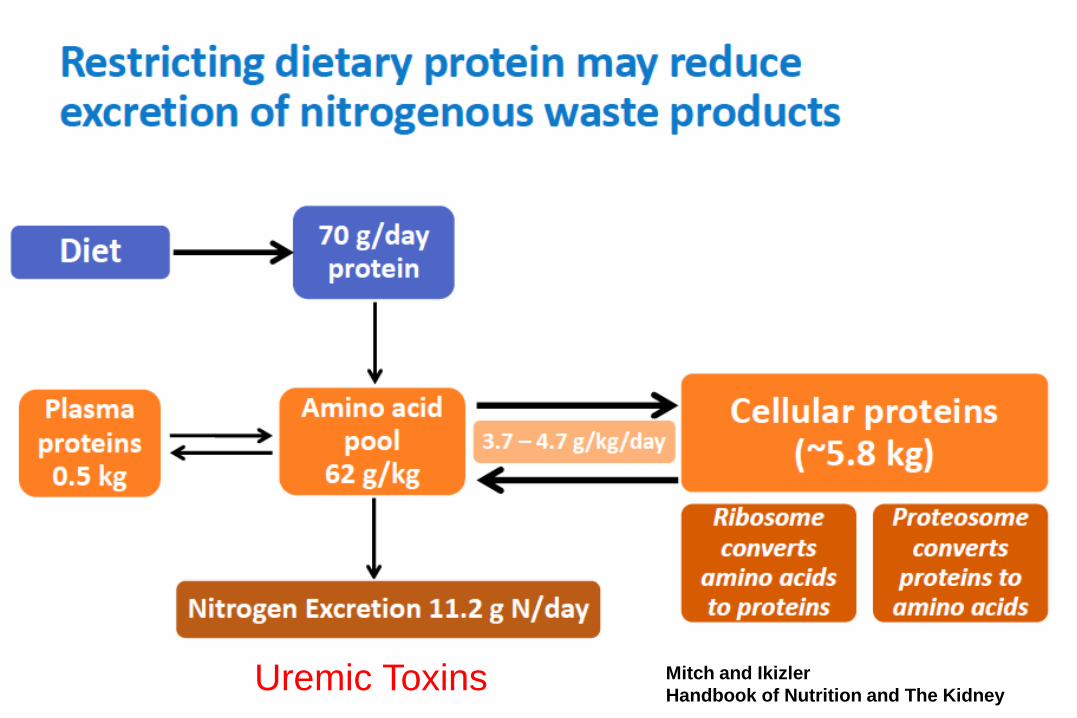
5Mitch and Ikizler
Handbook of Nutrition and The KidneyUremic Toxins

Rates of Death and CV Events in Patients
According to GFR

CVD
Frailty
InfectionCo-Morbid Conditions(Diabetes, CVD, Depression)
Dialysis-Associated Catabolism
Metabolic Derangements(Insulin Resistance, Metabolic Acidosis, IGF-1/GH Resistance)
Dietary Nutrient Intake
Loss of Kidney Function Uremic Toxin Retention
Protein-Energy WastingSarcopenia
Inflammation
Etiology and Consequences of Protein Energy Wasting in CKD
Carrero JJ et al on behalf of ISRNM; JREN 2013
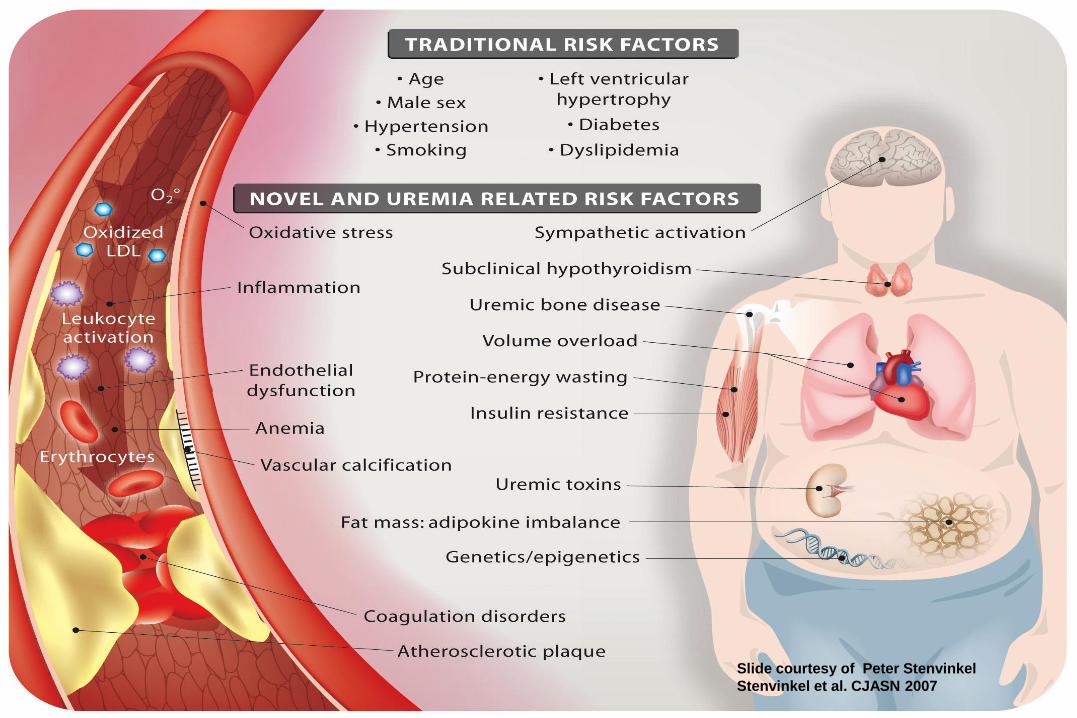
Slide courtesy of Peter Stenvinkel
Stenvinkel et al. CJASN 2007
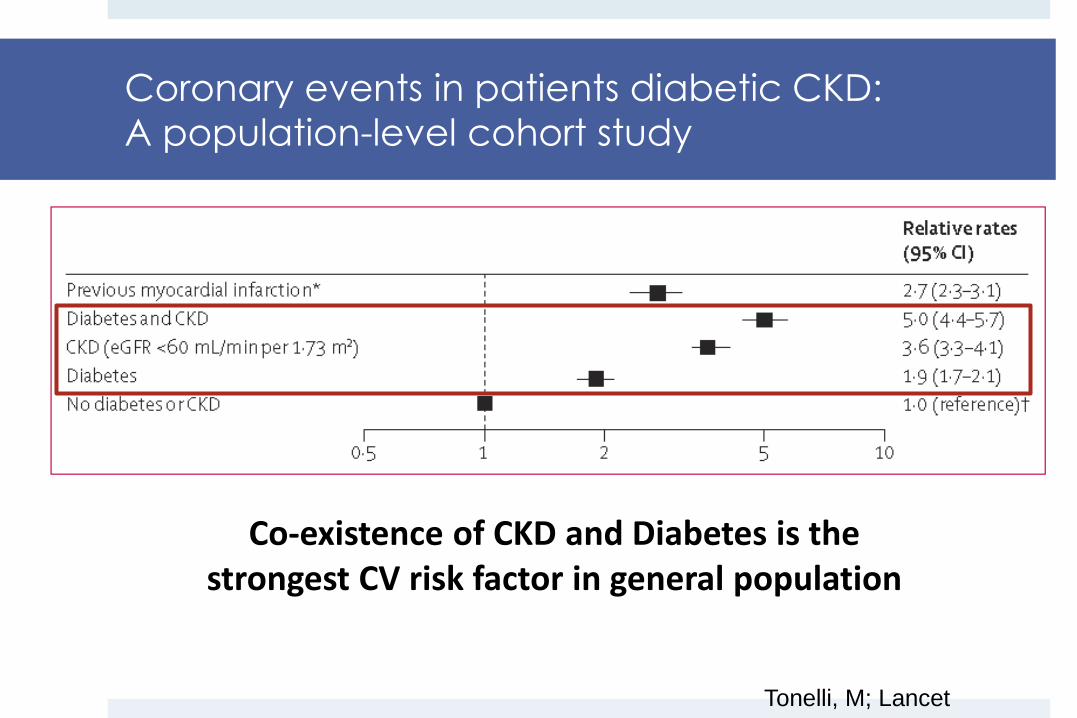
Coronary events in patients diabetic CKD:
A population-level cohort study
Tonelli, M; Lancet
Co-existence of CKD and Diabetes is the strongest CV risk factor in general population

Obesity is a global health issue that seems to worsen overtime
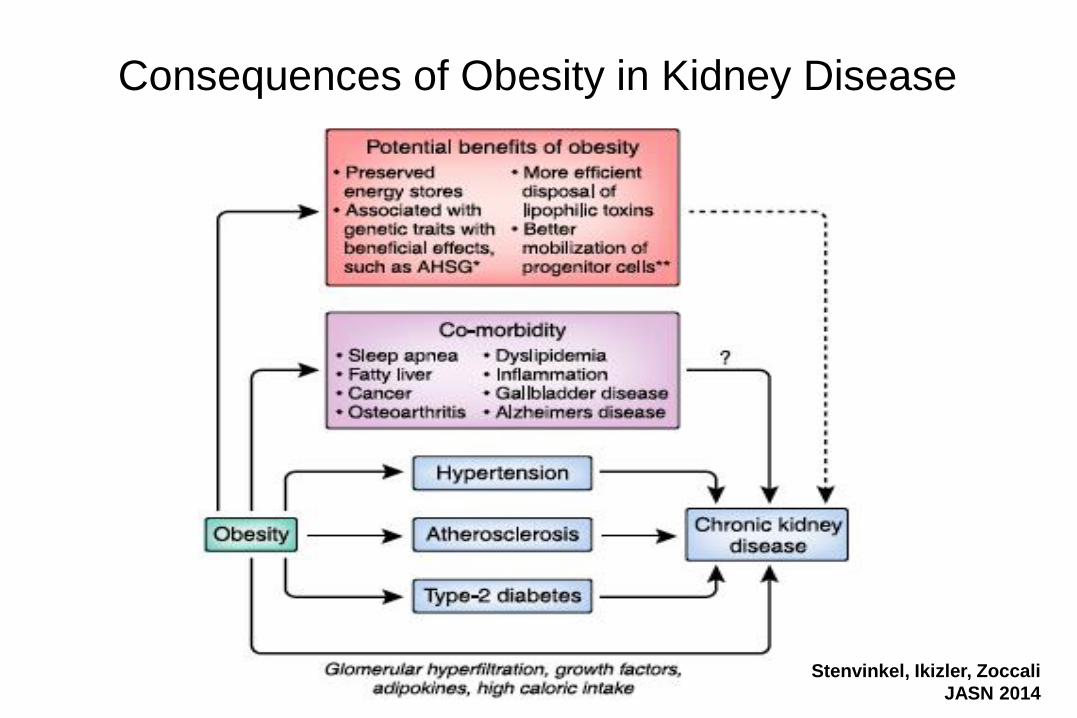
Consequences of Obesity in Kidney Disease
Stenvinkel, Ikizler, Zoccali
JASN 2014

Decreased clearance
Adipokine
imbalance
Increased fat mass
Adipose tissueAdiponectin
Muscle tissue
• Insulin resistance
• Lipid accumulation
• Muscle breakdown
Vasculature
• Endothelial activation
• Inflammation
• Oxidative stress
• Vascular calcification
Leptin
Resistin
TNF-a
IL-6
• Anorexia
• Depression
• Increased REE
• Sympathetic overactivity
Brain
BBB
Slide courtesy of Dr. Peter Stenvinkel
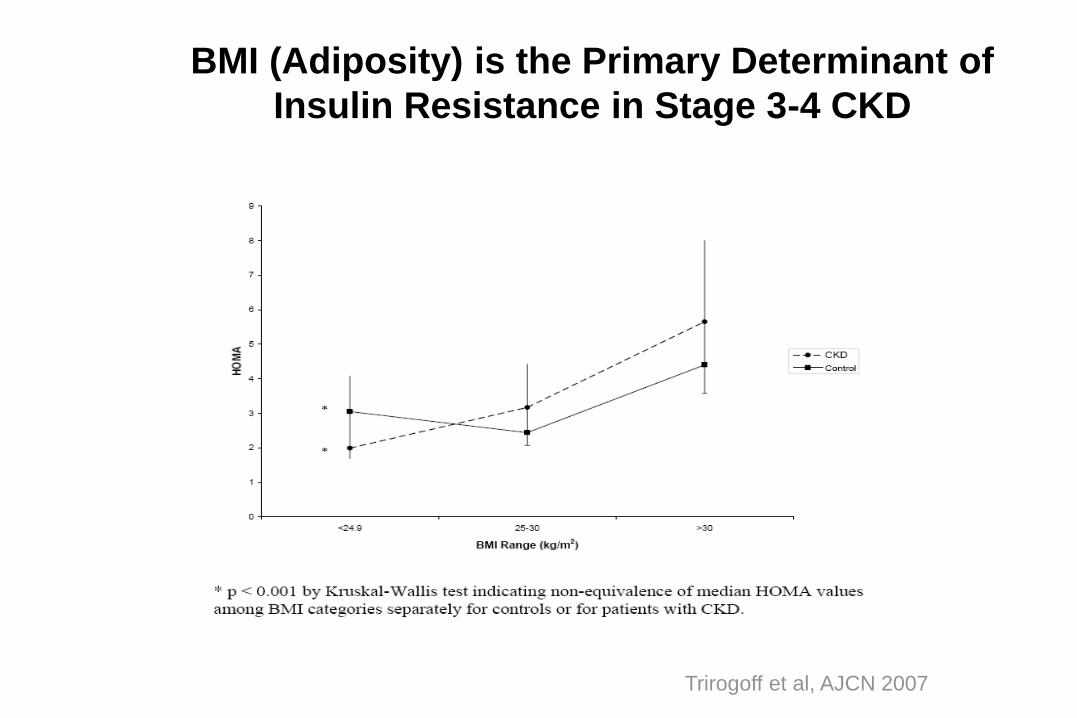
BMI (Adiposity) is the Primary Determinant of
Insulin Resistance in Stage 3-4 CKD
Trirogoff et al, AJCN 2007

BMI (Adiposity) is an Independent Determinant of Oxidative
Stress in Stage 3-4 CKD
Ramos et al, JASN 2008

A Proposed Mechanism for Uremia-Induced CVD Risk

Interventions Targeted at Non-Traditional CV Risk
Factors in Uremia – Lifestyle Interventions
Uremia Oxidative stress
Inflammation
Endothelial Dysfunction
Insulin resistance
CV
Risk
Diet

17
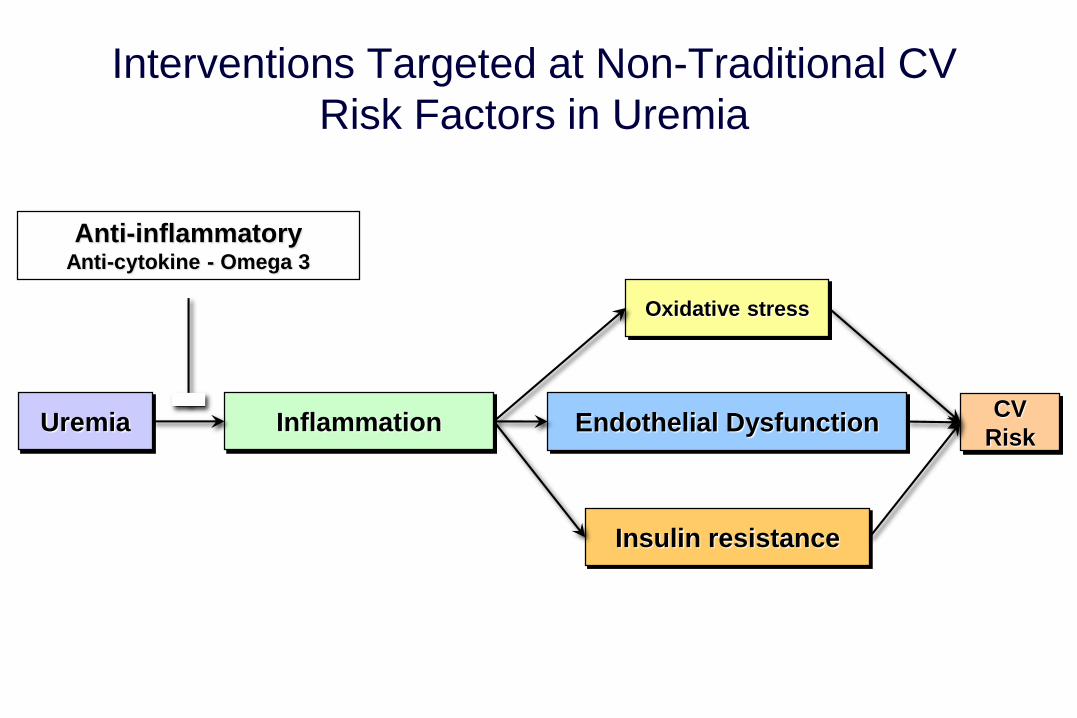
Interventions Targeted at Non-Traditional CV
Risk Factors in Uremia
Uremia Inflammation
Oxidative stress
Endothelial Dysfunction
Insulin resistance
CV
Risk
Anti-inflammatoryAnti-cytokine - Omega 3
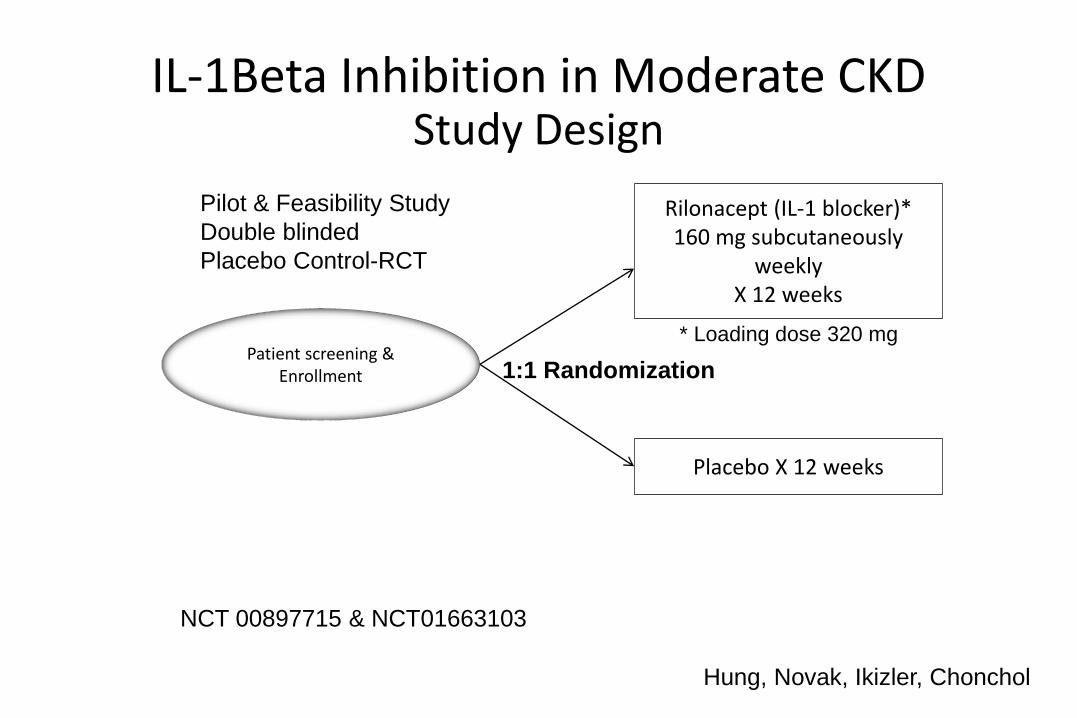
Study Design
Patient screening &Enrollment
Rilonacept (IL-1 blocker)*160 mg subcutaneously
weekly X 12 weeks
Placebo X 12 weeks
1:1 Randomization
Pilot & Feasibility Study
Double blinded
Placebo Control-RCT
* Loading dose 320 mg
NCT 00897715 & NCT01663103
IL-1Beta Inhibition in Moderate CKD
Hung, Novak, Ikizler, Chonchol

Outcomes • Primary outcomes:
Measurements of vascular health: endothelial
function ( brachial FMD%) and arterial stiffness (aPWV)
• Secondary outcomes:
Biomarkers of inflammation
Adiponectin and other markers of insulin resistance
FGF23 and other markers of MBD
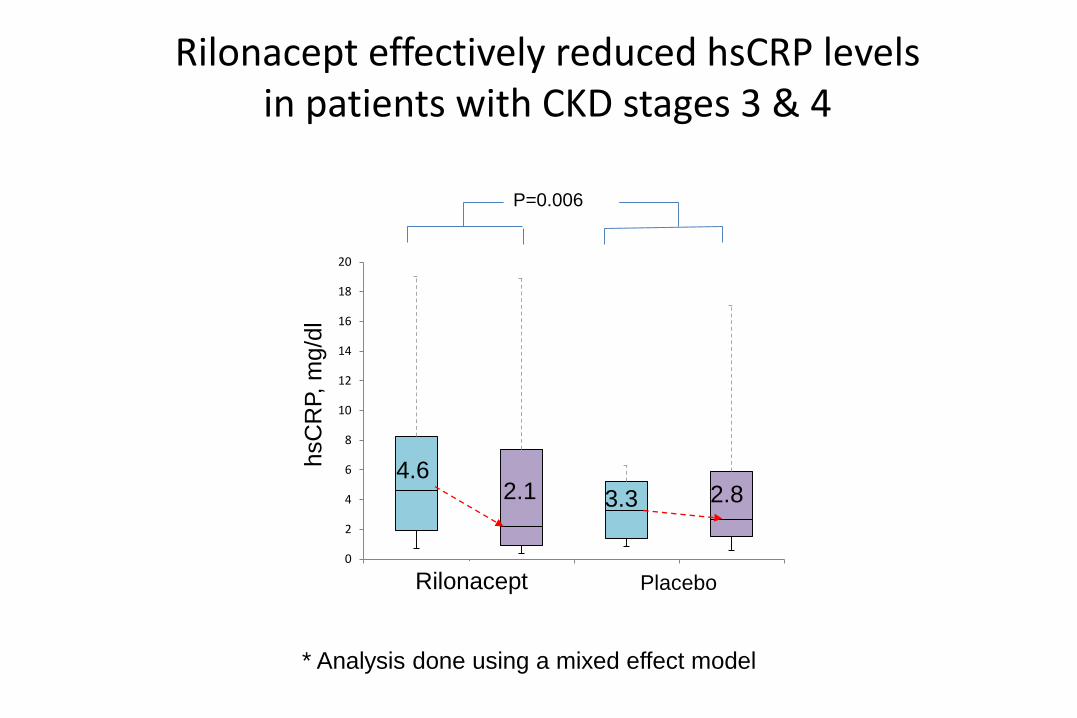
Rilonacept effectively reduced hsCRP levels in patients with CKD stages 3 & 4
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4
P=0.006
hsC
RP,
mg/d
l
Rilonacept Placebo
4.62.1 3.3 2.8
* Analysis done using a mixed effect model
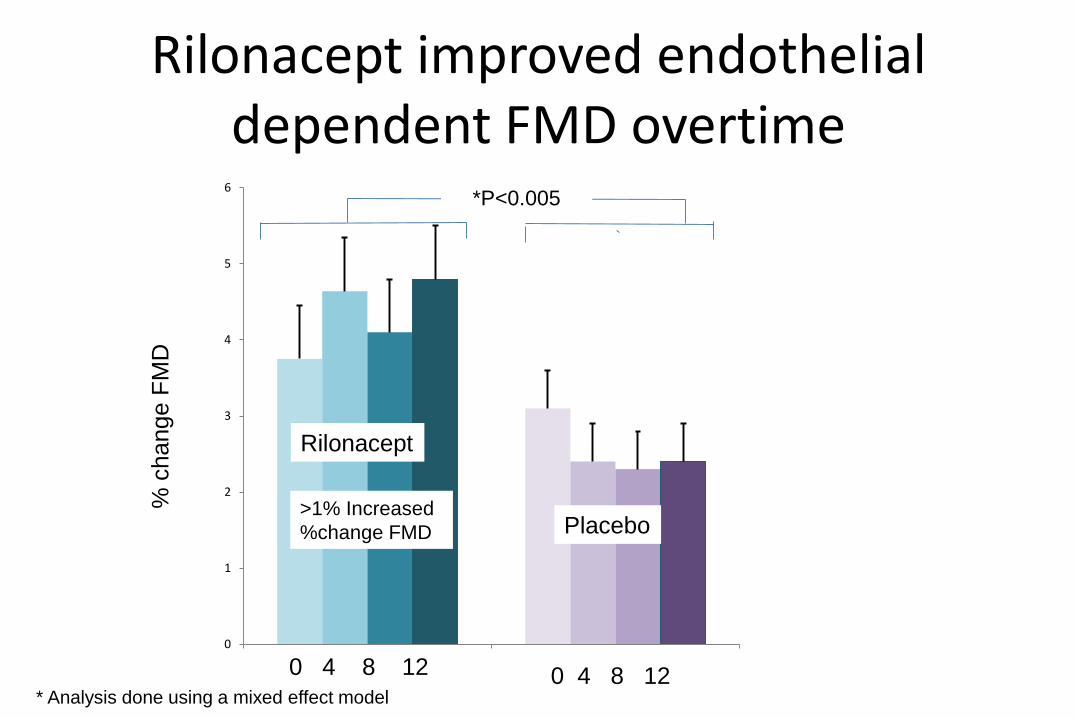
Rilonacept improved endothelial dependent FMD overtime
0
1
2
3
4
5
6
IL-1 Trap Placebo
*P<0.005
% c
hange F
MD
>1% Increased
%change FMD
Placebo0 4 8 12 0 4 8 12
Rilonacept
Placebo
* Analysis done using a mixed effect model
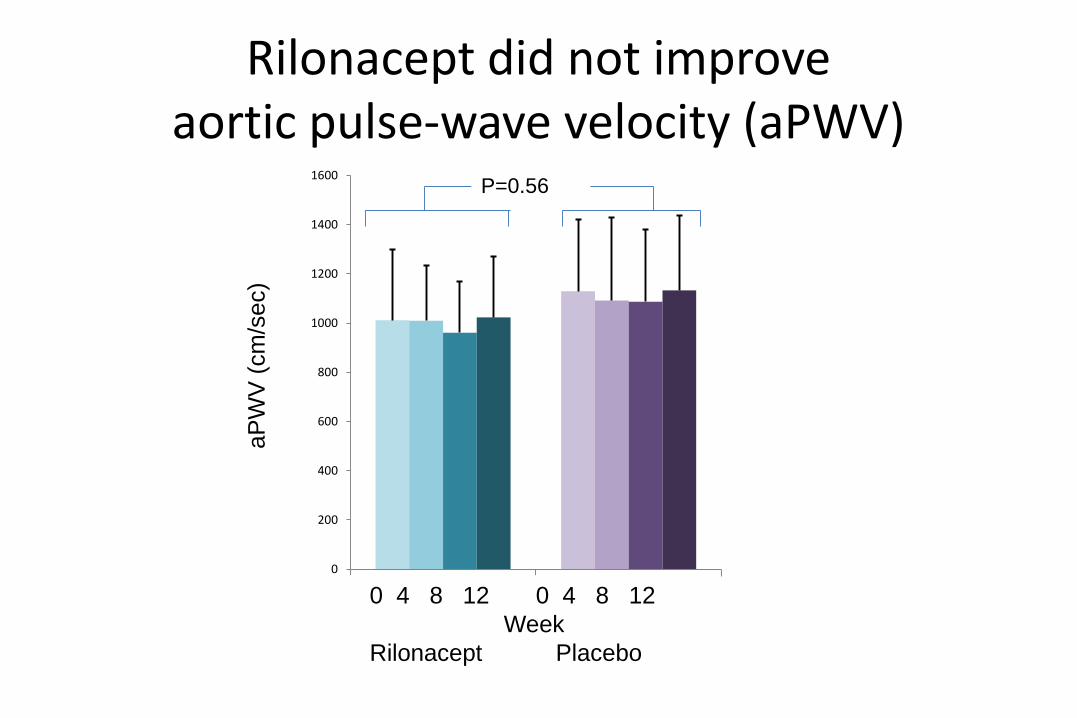
Rilonacept did not improveaortic pulse-wave velocity (aPWV)
0
200
400
600
800
1000
1200
1400
1600
Rilonacept Placebo
aP
WV
(cm
/sec)
0 4 8 12 0 4 8 12
Week
Rilonacept Placebo
P=0.56
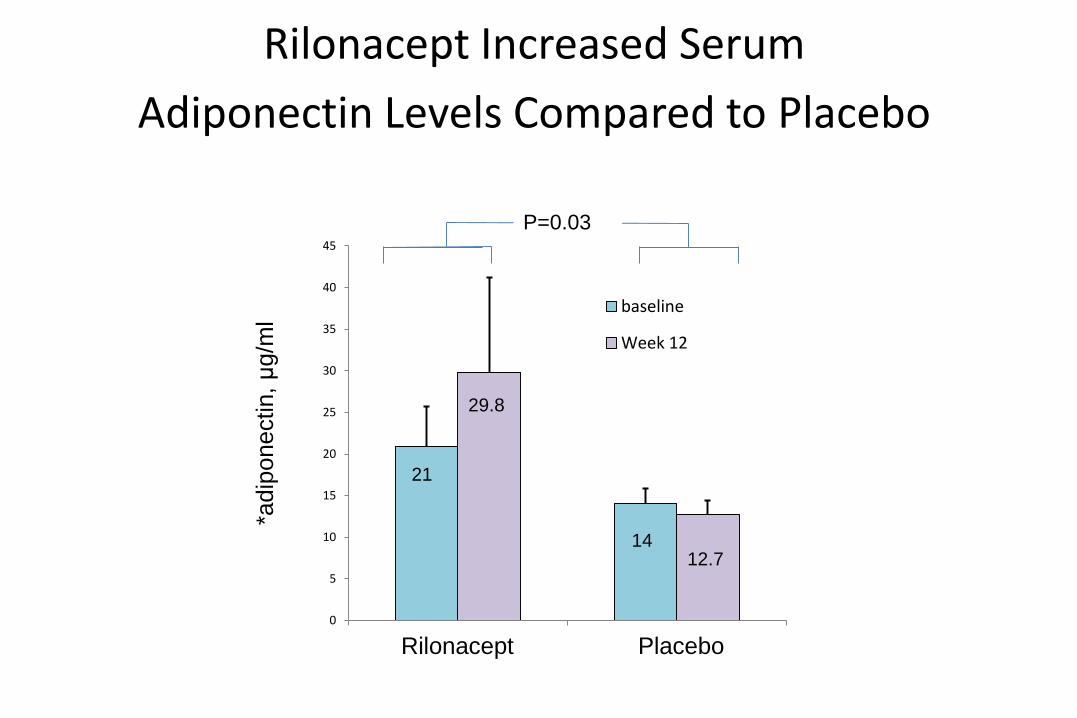
Rilonacept Increased Serum
Adiponectin Levels Compared to Placebo
0
5
10
15
20
25
30
35
40
45
IL-1 Trap Placebo
baseline
Week 12
P=0.03
1412.7
29.8
21
*adip
onectin, μ
g/m
l
Rilonacept Placebo

Uremia Oxidative Stress
Inflammation
Endothelial Dysfunction
Insulin Resistance
CV
Risk
Antioxidants
Interventions Targeted at Non-Traditional CV
Risk Factors in Uremia

Tocopherols and Alpha Lipoic Acid Therapy
(TALAT) in CKD Trial
Randomized, double-blind, placebo-controlled trial
N = 80 Stage 3-4 CKD patients
Tocopherols + a-lipoic acid vs. placebo x 8 weeks
Primary endpoint, change in F2-isoprostanes
Secondary endpoints
Inflammatory biomarkers
Insulin resistance
Endothelial dysfunction
CH3CHCH33
H3CHH33CC
HOHOHO
OOO
CH3CHCH33
H3CHH33CC
HOHOHO
OOO
OH
O
S S

TALAT in CKD TrialF2-isoprostane
F2-Iso
0
0.02
0.04
0.06
0.08
0.1
0.12
Placebo VitE/ALA
F2
-Is
op
ros
tan
es
Baseline
Month2

Diet and Exercise Intervention to Improve CV Risk Factors in
Stage 3-4 CKD Patients
Uremia Oxidative stress
Inflammation
Endothelial Dysfunction
Insulin resistance
CV
Risk
Diet & Exercise
Ikizler, Himmelfarb et al, JASN 2017
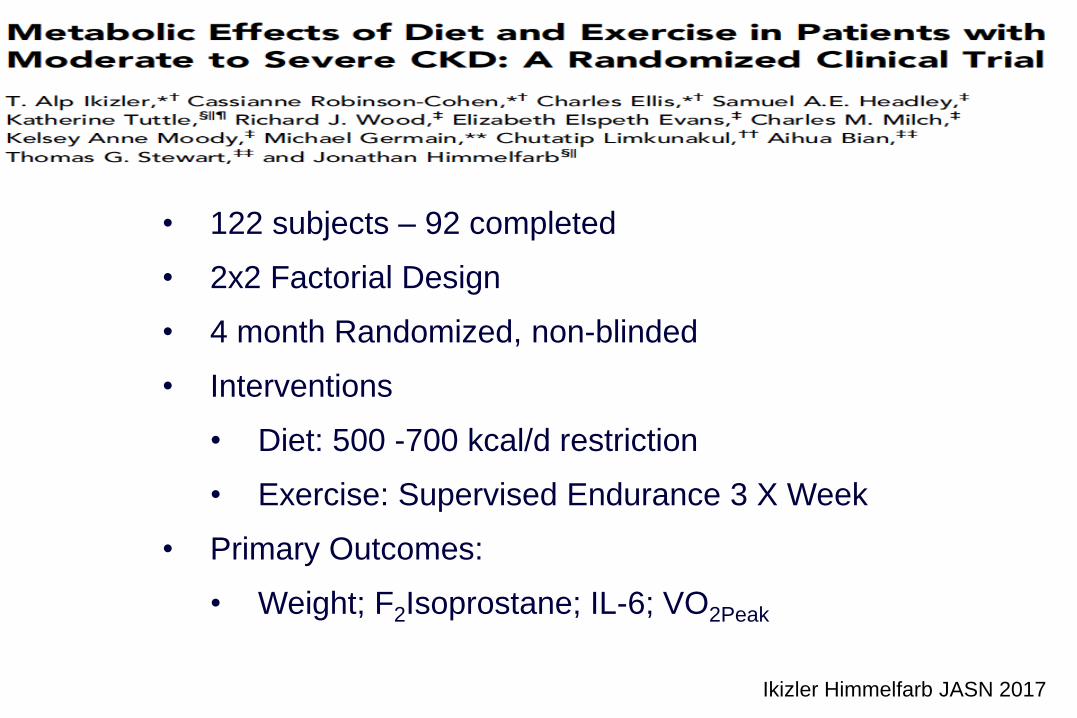
• 122 subjects – 92 completed
• 2x2 Factorial Design
• 4 month Randomized, non-blinded
• Interventions
• Diet: 500 -700 kcal/d restriction
• Exercise: Supervised Endurance 3 X Week
• Primary Outcomes:
• Weight; F2Isoprostane; IL-6; VO2Peak
Ikizler Himmelfarb JASN 2017

Diet and Exercise Intervention to Improve CV
Risk Factors in Stage 3-4 CKD Patients
Primary Outcomes:
F2-isoprostane; Weight; VO2peak
Secondary Outcomes:
Interleukin-6; Adipocytokines; Physical Activity

Changes in VO2 peak in Response to Diet and Exercise Interventions Compared to Changes in Control Group
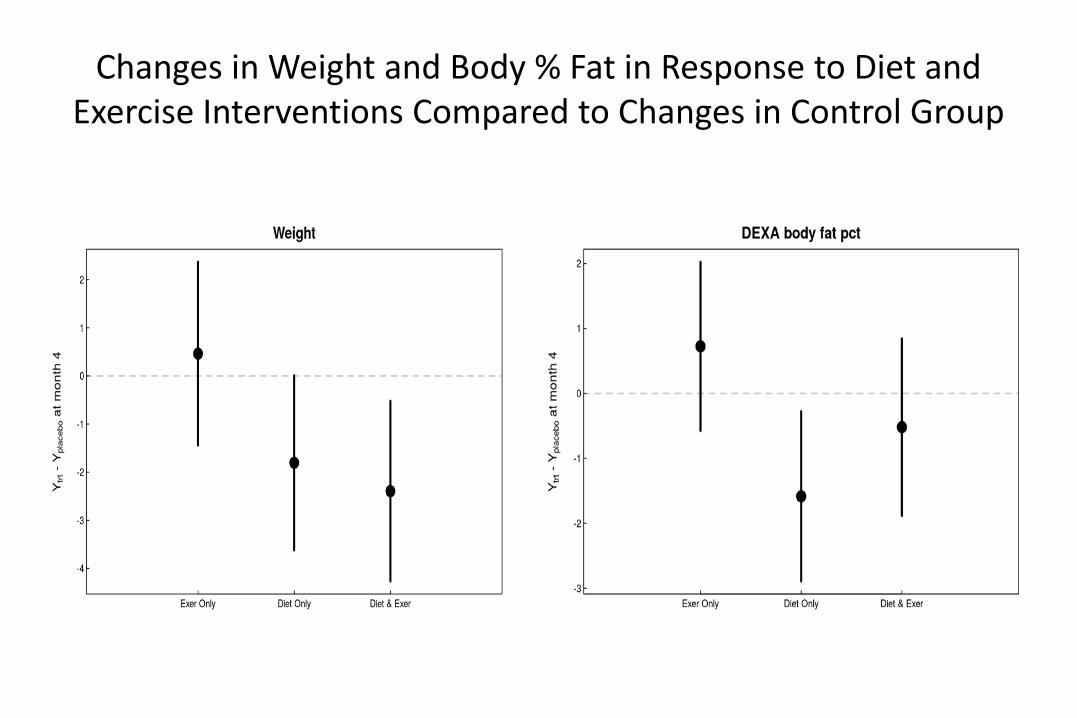
Changes in Weight and Body % Fat in Response to Diet and Exercise Interventions Compared to Changes in Control Group

Changes in F2-isoprostane and Interleukin-6 in Response to Diet and Exercise Interventions Compared to Changes in Control Group

Changes in Adipocytokine levels in Response to Diet and Exercise Interventions Compared to Changes in Control Group
Alsouqi, Ikizler, Himmelfarb Submitted
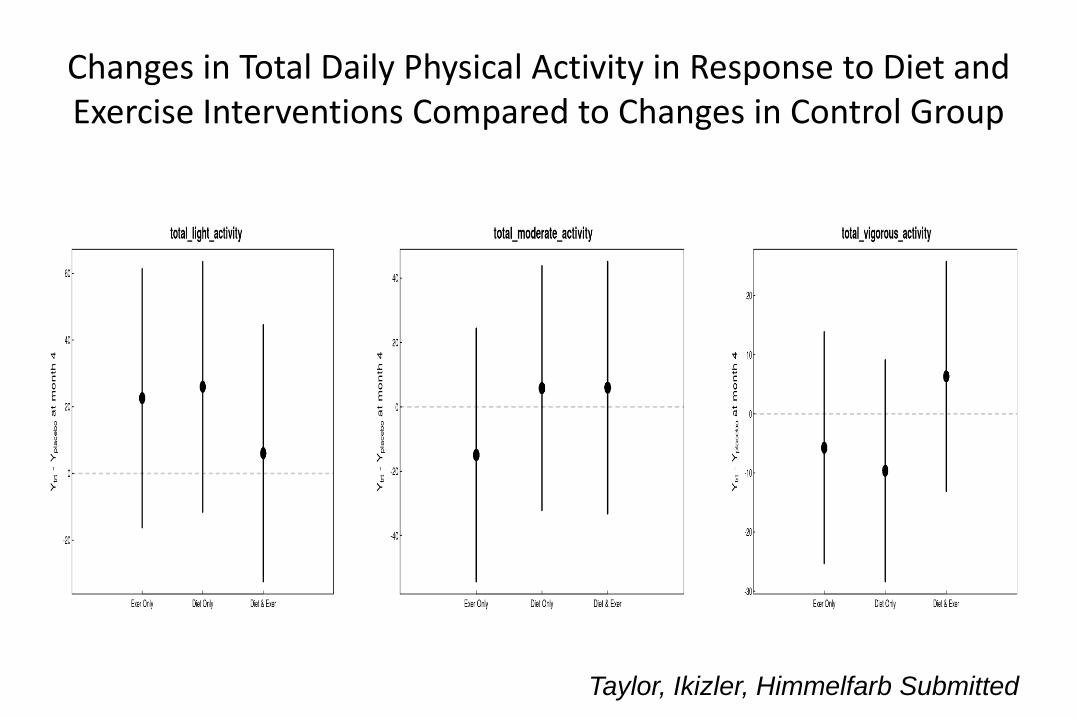
Changes in Total Daily Physical Activity in Response to Diet and Exercise Interventions Compared to Changes in Control Group
Taylor, Ikizler, Himmelfarb Submitted

Prevalence and severity of kidney disease in patients admitted with Acute Decompensated Heart Failure
118,465 Patients Hospitalized with ADHF (ADHERE Database)

CKD, Heart Failure & Nutrition
• Similar etiological factors
– Na, Obesity, Inflammation, Altered Metabolism
• Epidemiology of Chronic disease (? paradox)
• Difficulty in nutritional assessment
– Na intake; Dietary patterns; Body Composition
• Lack of evidence based guidelines
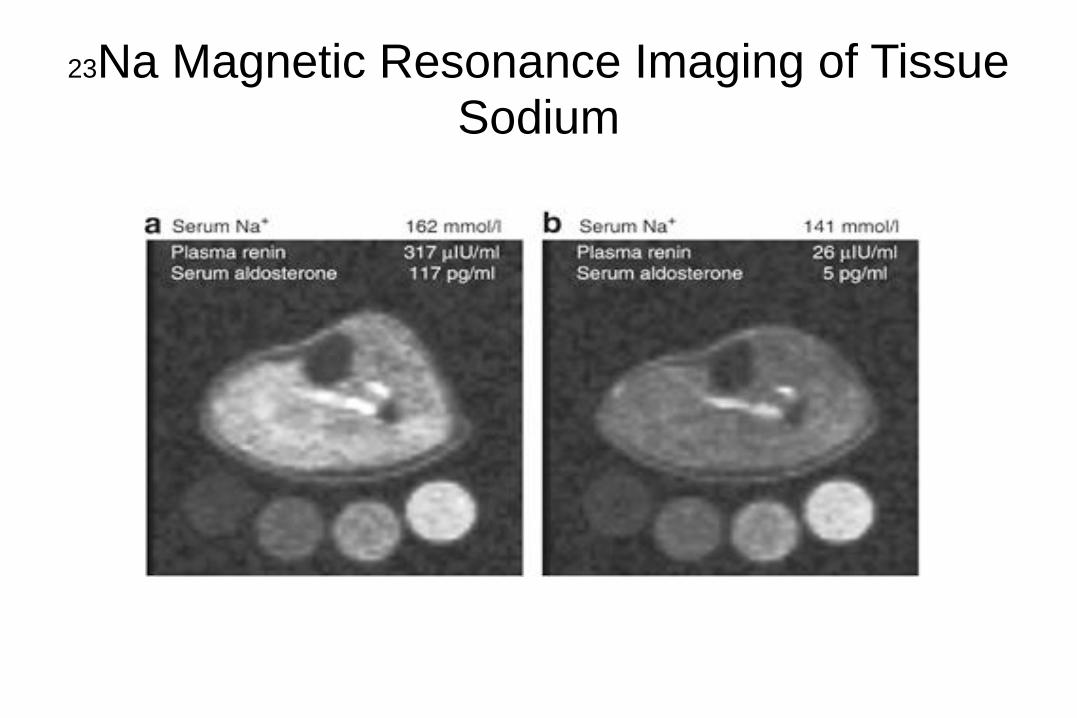
23Na Magnetic Resonance Imaging of Tissue Sodium
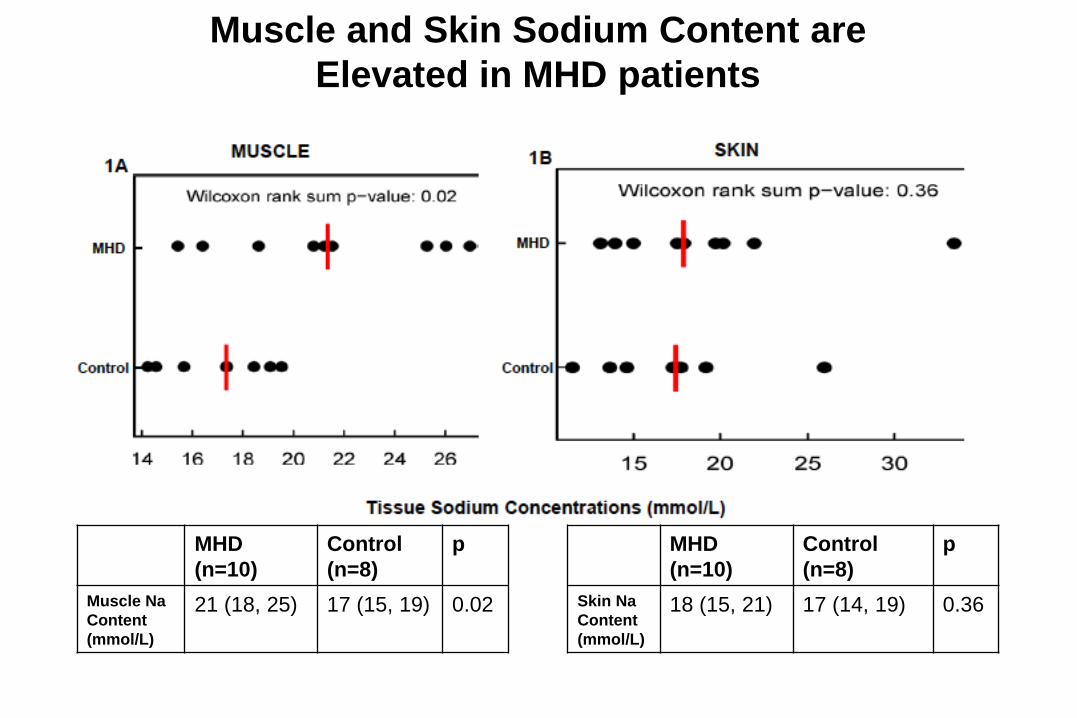
Muscle and Skin Sodium Content are
Elevated in MHD patients
MHD
(n=10)
Control
(n=8)
p
Muscle Na
Content
(mmol/L)
21 (18, 25) 17 (15, 19) 0.02
MHD
(n=10)
Control
(n=8)
p
Skin Na
Content
(mmol/L)
18 (15, 21) 17 (14, 19) 0.36
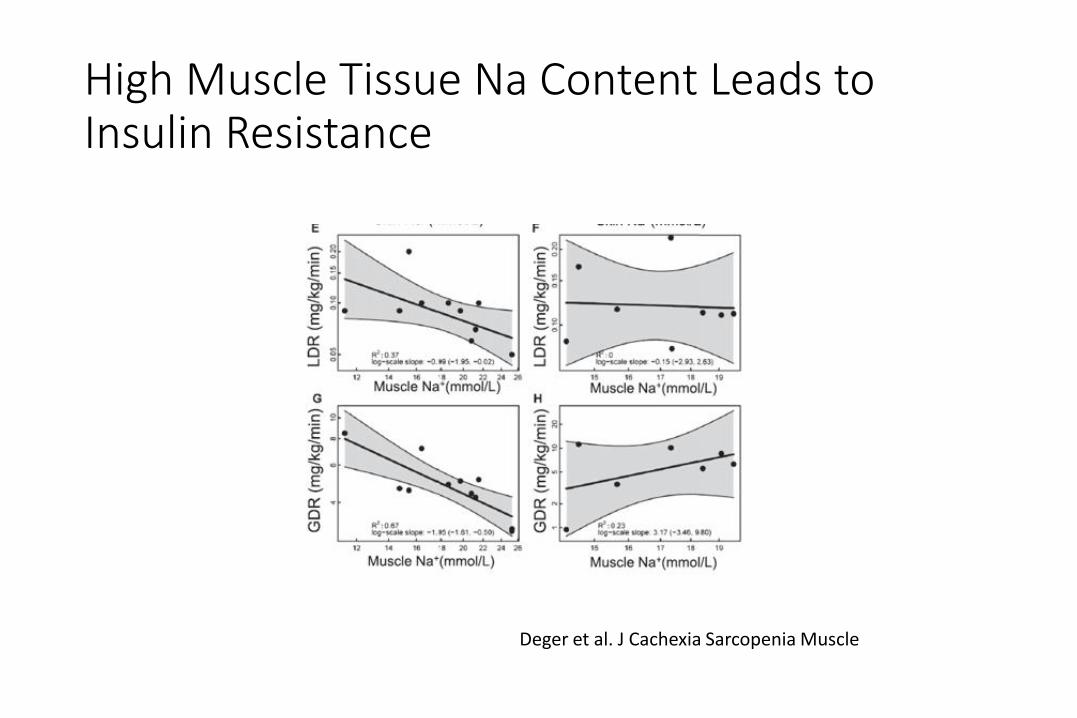
Deger et al. J Cachexia Sarcopenia Muscle
High Muscle Tissue Na Content Leads to Insulin Resistance

Special Considerations for Fat Intake in CKD
CKD patients are recommended to follow general advice for hearth health, including:
– Saturated fat <7% of total calories;
– Unsaturated fat to substitute saturated fat
Omega 3 fatty acids demonstrate promising benefits:
– triglyceride levels, dialysis access patency, and cardiovascular risk factors
Kris-Etherton et al Circulation (2002) 106: p2747-57;
Allomon & Moe CJASN (2006) 2: p182-192
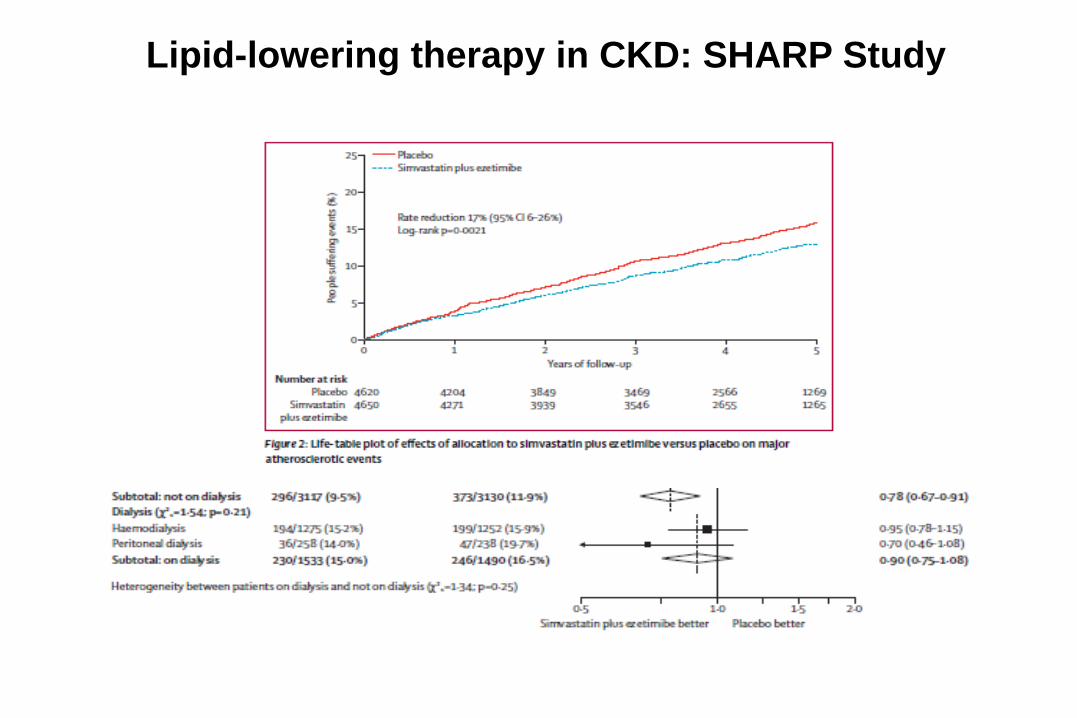
Lipid-lowering therapy in CKD: SHARP Study
Vitamins and Trace Elements
• Water-soluble vitamins (esp B6, C and folate)
– Losses: Dialysis removal > normal urinary losses
• Fat-soluble vitamins
– Usually only Vit D supplemented
– Vit A & E (risk of toxicity), intake should meet RDI
• Trace elements
– Zinc, selenium, copper, aluminium & magnesium
– Iron (oral supplements not recommended)
Nutritional Considerations in CKD
Loss of kidney function leads to number of metabolic
derangements
A multitude of dietary and other nutritional strategies can
be applied in the setting of moderate to advanced CKD
Healthy lifestyle interventions
Anti-inflammatory; Anti-oxidant; Insulin Sensitizing
Novel targets
Interventions personalized to individual patients are more
likely to succeed in CKD.

Funding/Other Support
NIH/NIDDK/NHLBI/NIEHS
RCG/FMC/Abbott/Baxter
NKF/AKF/ASN/ISRNM
SatelliteHealth grant program
Vanderbilt Clinical and Translational Research Award
Vanderbilt Center for Kidney Disease - Clinical
Research Group
Kidney Research Institute – UW; J. Himmelfarb





![[Beyond] morbid (aesthetic) symptoms](https://static.fdocuments.us/doc/165x107/62a9fb4db1576f77d233fc5d/beyond-morbid-aesthetic-symptoms.jpg)