A brief history of hearing aids and tinnitus sound enrichment devices.

Christopher Spankovich, AuD, PhD, MPH
Associate Professor, Director of Clinical Research
Dietary Factors in Hearing and
Tinnitus
Department of Otolaryngology and
Communicative Sciences
Edward Evan Evans-Pritchard, 1926

Rosen et al., 1962

Wang et al. (2002)

Center for Evidence Based Medicine (CEBM)
Study Design

o Meta-analysis, randomized control trial, cohort
study, case-control study, case report
o Epidemiology: Studies patterns, causes, and
effects of health and disease conditions in
defined populations
Study Design

Host
Agent
Hearing Loss
Environment

o Study Design: Prospective vs. Cross-Sectional
oBeaver Dam and NHANES
o Definition of Hearing Loss
oPTA?
o How Measured
oBekesy, HW, Reported?
o Adjusted Variables
oAge, Sex, Race/Ethnicity, Education…….
o Population
Epidemiology: For your consideration


oGenetics
oRace/Ethnicity
oAge
oSex
oSES/PIR/Education
oHealth/Disease
oEnvironment
oLifestyle & Diet
Non-Modifiable Modifiable


oLifestyle oSmoking
o Mahboubi et al. 2013
o Agrawal et al. 2010
oSecond-hand smoke
o Fabry et al. 2011
Lifestyle

Spankovich et al., 2013, 2014
Lin et al., 2011

oLifestyle oAlcohol intake o Curhan et al. 2011
o No relationship
o Except increased risk with low B12
o Popelka et al. 2000
o Moderate good/high bad
o High >4 drinks/day
oAnalgesic Use & other Drugs oCurhan et al. 2010/2012
oDille et al. 2010
oBainbridge et al., 2008
Lifestyle


• Fitness and NIHL (Kolkhorst et al., 1998): Better markers of physical fitness reduced level of TTS to 108 dB SPL for 10 min.
• 2 month of aerobic training reduced TTS (Cristell et al., 1988)
• Sedentary behavior increases odds of hearing loss (Loprinzi et al., 2013).
• Association between odd of of hearing loss and lower physical activity (Gispen et al., 2014).
• Association with physical activity and hearing loss in persons with diabetes (Loprinzi et al., 2014)
Physical Activity

• Simultaneous noise and exercise increases level of TTS induced by noise (Lindgren & Axelsson, 1988; Vittitow et al., 1994)
• Simultaneous noise and exercise did not increase TTS (Alessio & Hutchinson, 1991)
Physical Activity



DM • Glucose is the primary energy source of the
cochlea via conversion to ATP
–Helps to maintain the endocochlear potential through
active transport of K+ and Na+
–Hypoglycemia will reduce this driving force and reduce
active mechanism
–Otoacoustic emissions: an objective measure of
reflections and distortions from the cochlea are
sensitive to changes in glucose
OAEs have been explored as an indirect measure of glucose
status (Jacobs et al. 2012)

DM • Glucose can also
affect peripheral nerve
conduction including
auditory evoked
potentials
–Hypoglycemia can cause
delay in latency of later
ABR waves (Kern et al.
1994)
–Effects can also be seen
on efferent pathway

DM • Microangiopathy
• Mitochondrial dysfunction
• Advanced glycation end products
• Inflammation
• Glutathione dysregulation
• Protein synthesis dysfunction
• Glutamate excitotoxicity

DM • Low Frequency
–Apical portion of cochlea Microangiopathy?
Fluid composition & dynamics?
• Mid Frequency –3000-6000 Hz
Resonance area for broadband sound
High susceptibility to Noise
• Higher Frequency –Basal portion of the cochlea
High metabolic requirement
Lower levels of glutathione
High susceptibility to noise and ototoxic drugs

DM • Testing low frequencies
–Low frequency hearing loss associated with Diabetes and risk for cardio-metabolic risk (Friedland et a. 2009)
• Testing mid frequencies –3000-6000 Hz region particularly susceptible to effects of
noise
–Diabetes can increase risk for noise pathology (Wu et al. 2009; Win et al. 2015, Ishii et al. 1992)
• Testing higher frequencies –Testing > 8000 Hz may be a useful marker for early effects
of DM (Austin et al. 2009)
–High metabolic demand and sensitive to both noise and ototoxic drugs


Diet and Health • Nutrition is a meaningful determinant of all major
chronic health conditions
• 2nd half of 20th century saw move from largely plant based diet to higher fat, energy-dense diets with substantial content from animals
• Challenges can be unique to region
• Even in developed countries like the US, poverty and access to nutritional foods can be an issues
• The other issue is health and nutritional literacy to increase healthy behaviors


Kopke, 2002

Diet & Hearing o Fat, Fatty acids, Cholesterol
o Protein
o Carbohydrates oGlycemic index
o Vitamin A oRetinoic Acid
oBeta-Carotene
o Lycopene
o B-vitamins (Folate, B-12, and etc.)
o Vitamin C
o Vitamin D
o Vitamin E
o Magnesium
o Calcium
o Zinc
o Sodium
o Potassium
o Selenium
o Phenolics & Flavanoids oResveratrol
o Caloric intake
o Other trace chemicals oNAC
oMET (D-MET)

Animals, Diet and Hearing • Caloric Restriction (Seidman 2000; Someya et al., 2007 )
• Protein deficiency (Lautermann et al., 1995; Ohinata et al., 2000).
• Vitamin A deficiency (Biesalski et al., 1990)
• Vitamin A as retinoic acid (Ahn et al., 2005; Shim et al., 2009)
• Vitamin B12 (Zhu et al., 2006)
• Vitamin C (McFadden et al., 2005; Henrich et al., 2008)
• Vitamin D deficiency (Zou et al., 2008)
• Vitamin E (Scholik et al., 2004)
• Hyperlipidemia via High Cholesterol/Fat Diet (Sikora et al., 1986; Pillsbury, 1986)
• Magnesium (Joachims et al., 1983; Haupt et al., 2002)
• Combination of A, C, E, Mg (Le Prell et al., 2007)
• Vitamin P (term used in 1950s) Phenolic compounds – Resveratrol (Seidman et al., 2003)
• Other diet derived chemicals (usually in trace to lower amounts, amino acids, enzymes, and etc.) – D-methionine, Coenzyme Q10, ebselen, N-acetyl cysteine, and etc.



Direct Effect Indirect Effect





Humans, Diet, and Hearing • Ototoxic Drug
• Sudden Hearing Loss
• Age
• Noise

Humans, Diet, and Hearing : Drug • Cisplatin (Weijl et al., 2004)
Sayin et al. (2014) found that mice with lung
tumors supplemented with antioxidants had
accelerated growth in tumor size and
increased mortality.

Humans, Diet, and Hearing : ISSHL • Fresh Vegetables (Nakashima et al., 1997)
–More fresh veggies reduce odds of SSHL
• Western diet (Nakamura et al., 2001)
–Western diet increased risk of SSHL
• Vitamin C and E (Hatano et al., 2008)
–All patients treated with steroids, experimental group
also received vitamin E (600 mg/day) and C (1200
mg/day)
–Recovery was on average 30 dB in experimental group
compared to 18 dB in control
Humans, Diet, and Hearing : Age
• Vitamins –Vitamin A (Peneau et al., 2013; Gopinath et al., 2011a;
Spankovich et al., 2011)
–Vitamin B9 (Durga et al., 2007, Lasisi et al., 2010)
–Vitamin B12 (Peneau et al., 2013)
–Vitamin C (Takumid & Anniko 2009; Lonergan et al., 1975)
–Vitamin E (Spankovich et al., 2011; Gopinath et al., 2011a)
• Magnesium (Spankovich et al., 2011)
• Carotenoid: Lycopene (Spankovich et al., 2011)
• Shargorodsky et al., 2010 (No Benefit, B9 may reduce risk in older men)
• Antioxidant vitamins (A,C, E, carotenoids, iron, zinc) not associated with 5 year incidence of hearing loss (Gopinath et al. 2011)

Spankovich et al., 2011

Humans, Diet, and Hearing : Age
• Lipids (Simpson et al., 2012; Jones & Davis,
1999; Spankovich et al., 2011; Dullemeijer et al.,
2010; Gopinath et al., 2010; Gopinath et al.,
2011b, Rosen et al., 1965, 1970)
–Serum vs. Diet
• Carbohydrates: Glycemic Index bad, fiber good
(Gopinath et al., 2010)
• Protein (Spankovich et al., 2011)
• Eat more meat and fish (Peneau et al., 2013)
• Cardiovascular disease (Gates et al., 1993) and
Diabetes (Bainbridge et al., 2008)

Humans, Diet, Hearing : Noise
• Antioxidants –Rabinowitz et al., 2002 found factory workers with higher levels of
plasma vitamin E had better high frequency thresholds
–Shemesh et al., 1993 found persons with NIHL and tinnitus more likely had B12 serum deficiency
–Gok et al., 2004 found B12 and B9 serum levels reduced in persons with NIHL and higher levels of homocysteine
–Quaranta et al., 2004 found high levels of B12 reduced risk of TTS, subjects were given B12 shots and exposed to 10 min of 112 dB.
–Le Prell et al., 2011 found no effects of ACEMg in Swedish military as no subjects had reliable shift in hearing
–Kapoor et al., 2011 showed Vitamin E supplementation reduced markers of oxidative stress in noise exposed workers

Humans, Diet, Hearing : Noise
• Lipids
–Sutbas et al., 2007 found that persons with noise
exposure and hyperlipidemia placed on low cholesterol
diet and therapy had reduced effects on hearing after 2
years
–Chang et al., 2007 found that persons with elevated
serum triglycerides not cholesterol were at increased
risk of NIHL
–Toppila et al. 2000 found that in workers with noise
exposure, elevated serum cholesterol, analgesics, and
smoking was related to poorer hearing

Dietary Intake
o Single nutrient analysis
Limitations
oEffect size
oInteractions (biochemically &
statistically)
oError (chance findings)
oWe don’t eat in single nutrients

NHANES o Started in early 1960’s
o Survey that combines interviews and physical
examinations
o Examines a nationally representative sample of
~5,000 persons each year
o Weightings are applied to generalize to US
population
o Limitation: cross-sectional
o Hearing has been included as a measure since
the first Survey NHES 1 (1959-1962)

Health Eating Index


Spankovich & Le Prell (2013)

Spankovich & Le Prell
(2013)

Spankovich & Le Prell (2013)
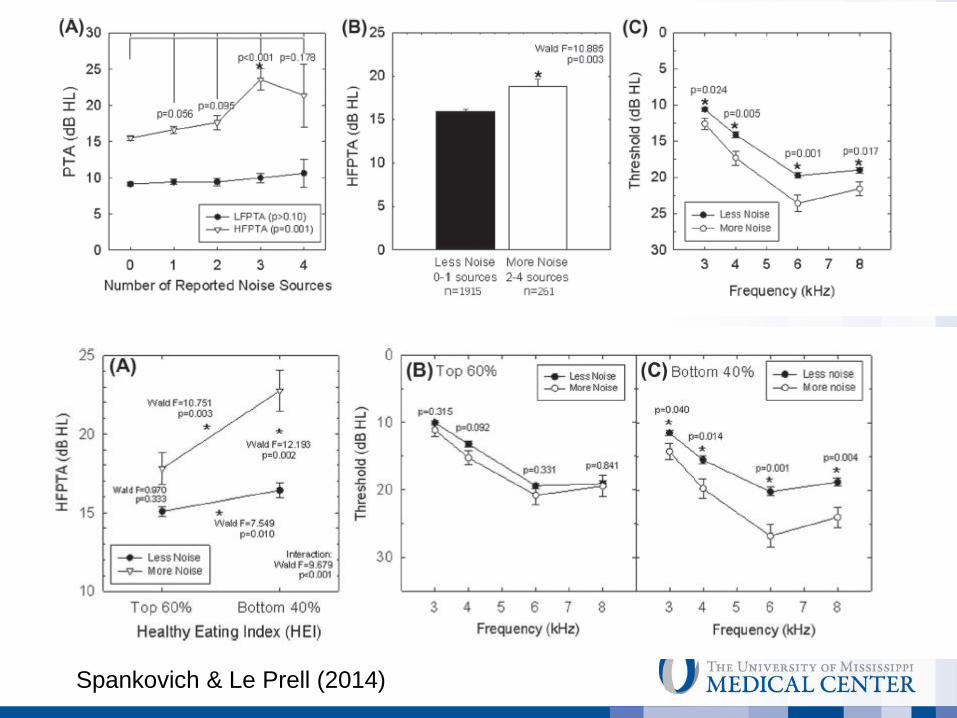
Spankovich & Le Prell (2014)

Spankovich & Le Prell (2014)

Spankovich & Le Prell (2014)

Kelly, Jolley, Spankovich
(2016 AAA)

• Lutz et al. (2013)
–Characterized HEI of soldiers during BCT
–NO relation to age, sex, race, or physical activity
–Smokers 4.5 times likely to be in low HEI category
–Dining provided during BCT increased HEI scores by up to 46% for
those in the low initial category and 22% in those in the medium
HEI
• Purvis et al. (2013)
–Associations between Healthy Eating Score (5) and passage of the
Army Physical Fitness Test (APFT) and emotional, social, family,
social fitness.
• Smith et al. (2013)
–DOD survey found only 3% of >15,000 participants reported eating
fruit, vegetables, and whole grains to minimal Healthy People 2010
guidelines
HEI & Military


o Case-Control and Intervention Studies o Decreased progression of hearing loss with folic acid
supplementation (Durga et al., 2007)
oB12 supplementation had no effect in ameliorating hearing loss of tinnitus (Berkiten et al., 2013)
oB12 supplementation was shown to protect against TTS
oMagnesium was show to reduce TTS and PTS (Joachims et al., 1993; Attias et al., 1994, 2004)
oPlasma Mg was not associated with NIHL in US Army (Walden et al., 2000)
oAlso previously mentioned cisplatin (Weijl et al., 2004) and sudden hearing loss studies (Joachims et al., 2013; Hatano et al., 2008)
Supplemented Diets

• D-Methionine, N-Acetyl Cysteine (NAC),
Acetylcarnitine (ALCAR), Ebselen, nicotinamide
ribosidem,Vitamins A, C, E, Mg, sodium
thiosulfate, vinceriquinone, etc.
Pill or Food?

oClinical Trials
oTemporary Threshold Shift
oMusic player (4 hrs) @ 100 dBA
oPre and post testing
oFDA thru IND monitored by DSMB
Pill or Food?

93 dB: N=10 subjects. 98 dB: N=11 subjects. 100 dB: N=12 subjects.
Le Prell, C.G., Dell, S., Hensley, B.N., Hall, J.W.I., Campbell, K.C.M., Antonelli, P.A., Green,
G.E., Miller, J.M., Guire, K. 2012. Digital music exposure reliably induces temporary threshold
shift (TTS) in normal hearing human subjects. Ear Hear. 33, e44-58.

• Randomized placebo-controlled, double-blind, between-subjects design
Placebo x 4d
Screening
Nutrients x 4d
Baseline 2,
exposure,
post tests
Baseline 1 1 week
post tests 1 day post
tests

oACEMg o4 days of dosing total
oB-carotene (18 mg), vitamin C (as a ascorbic acid 500
mg), Vitamin E (as α tocopherol 305 mg), and
Magnesium (287.26 citrate and 6.5 stearate)
oNo significant decrease in TTS
Le Prell, C.G., Fulbright, A., Spankovich, C., Griffiths, S., Antonelli, P.A., Campbell, K.C.M.,
Green, G.E., Miller, J.M., Guire, K. In preparation. Use of a dietary supplement did not
prevent temporary threshold shift (TTS) after digital music exposure (submitted to Audiology
and Neurotology)
Pill or Food?

oEbselen (Sound Pharmaceuticals)
oGlutathione peroxidase mimic
o4 days of total dosing (200 to 600 mg)
oMedical exam, blood work, chest x-ray
oSignificant decrease in TTS
Kil J, Lynch ED, Griffiths SK, Lobarinas E, Spankovich C, Antonelli PJ, Le Prell CG. Efficacy of SPI-1005 for Prevention of Noise Induced Hearing Loss: Phase 2 Clinical Trial Results. Presented at AAOHNS on 9/21/14.
Pill or Food?

• Iowa Women’s Health Study
(2011)
• Men’s SELECT Study (2011)
• Chronic vs. Acute Prevention
• http://www.nytimes.com/2013/06/
09/opinion/sunday/dont-take-
your-
vitamins.html?pagewanted=all&_
r=0
Pill or Food?

GNC, Target, Walmart, Walgreens selling
bogus herbal supplements, NY charges
DNA tests found only 21% of tested
supplements contained what the labels
promised (Washington Post, 2/3/15)
From Target, Up & Up brand
Gingko Biloba
No gingko biloba found
Found garlic, rice and mung/French bean
St. John’s Wort
No St. John’s Wort found
Found garlic, rice and dracaena (houseplant)
So what was in the bottle:
Garlic, rice, dracaena, pine, grass,
primrose, mung
What was not in the bottles:
No traceable levels of Gingko biloba,
No St. John’s Wort, No Ginseng, No
Echinacea,

• What can you advise your patients?
–Currently no drug or dietary treatment is approved
by the FDA for hearing loss prevention
–But, eating a healthy diet and exercise as approved
by their primary care physician is not going to hurt!
Application
• What I tell my patients?
–Eat healthy and exercise, discuss any change in diet
and exercise with your physicians and seek further
information from a nutrition expert.
–Simple changes you can start with are to reduce white
foods replace with brown, reduce processed foods,
increase veggies (particularly green leafy veggies) and
fruit, nuts, and seeds. These changes are dependent
on other health factors.
–Supplements will not replace the benefit of a healthy
diet.
Application





Tinnitus o Increased hazard of developing tinnitus over 10 year
period oHistory of arthritis
oHistory of head injury
oHistory of hearing loss (among women)
oHistory of smoking
o Decreased hazard of developing tinnitus over 10 year period oAge (among women): under-report?
oModerate alcohol consumption
oObesity (among men)
Nondahl et al., 2010
Tinnitus o Physical activity associated with lower levels of
tinnitus severity (Carpenter-Thompson et al.
2015)
o Adolescents and adults with higher physical
activity were less likely to report tinnitus (Loprinzi
et al. 2013)

Tinnitus o Zinc (DeBartolo et al. 1989)
oReduced tinnitus in people with zinc deficiency
o Low cholesterol diet and antilipid therapy (Sutbas et al. 2007) oReduced tinnitus severity with diet
and therapy
o Taurine (Brozoski et al. 2010, rats) oReduce tinnitus in rats (glycine
agonist)
o Caffeine abstinence (Claire et al. 2010) oNo effect on reducing tinnitus

Tinnitus o Increased with fruit/vegetable intake, bread, dairy
avoidance
o Reduced with fish consumption, egg avoidance,
consumption of caffeinated coffee
oMcCormack et al., 2014

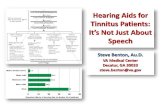
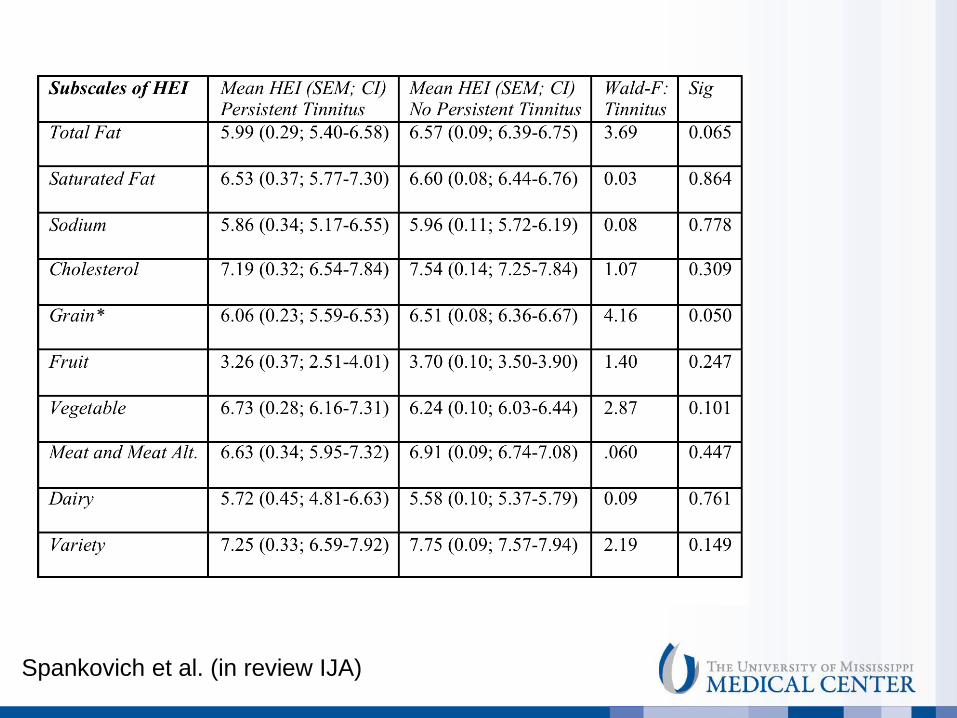
Spankovich et al. (in review IJA)

Spankovich et al. (in review IJA)
Spankovich et al. (in review IJA)

Wald F = 4.610 p = 0.032
Pe
rcen
tag
e (
%)
HEI Quintile (5 = Best)
Figure 1. Percentage of individuals with
(black bars) and without persistent
tinnitus (white bars) across HEI
quintiles; sampling weights applied.
Overall there was a significant
relationship between report of
persistent tinnitus and HEI quintile.
There was a significant increase in
odds of reporting persistent tinnitus
with decrease in HEI score.
Spankovich et al. (in review IJA)
o Supplements, essential oils, acupressure/acupuncture, etc. oNo evidence to support effectiveness
to treat tinnitus, not a cure for tinnitus
oEducate patient on lack of scientific support, role of placebo effect and let them make their own educated decision
oReductions in stress and anxiety can help with tinnitus
oGinkgo biloba-bioactive flavonoid with vasoactive and antioxidant properties, some studies have suggested benefit in form of EGb-761 o Evidence inconclusive
o Can interact with antiplatelet agents
SUPPLEMENTS and TINNITUS

SUPPLEMENTS and TINNITUS
o Over the Counter oNo evidence any work greater than a placebo
effect
oRobert DiSogra, AuD has some good reviews an textbook available through Oak Tree Products
ohttp://www.audiologyfreehold.com/ingredients-in-otc-tinnitus-relief-products


Diet: Pre-natal, Peri-natal, childhood o Challenges to nutrition also extend to prenatal
and childhood
o Iodine deficiency is the greatest single
preventable cause of brain damage
o Vitamin A deficiency is the single greatest cause
of childhood blindness
o Prematurity is highly related to prenatal care
o All of these have direct and indirect relationships
to hearing

Diet: Pre-natal, Peri-natal, childhood o Obesity has been correlated with hearing loss in
childhood and increased risk for acquired hearing
loss as an adult
o Very limited data exist on the role of nutrition in
prevention of childhood hearing loss

Global Implications o Age related hearing loss is not caused
necessarily by age
o Healthy lifestyle is a fairly universal concept but regional issues are important
o Malnutrition can be an issue in developing countries and in the US
o Larger concern is influx of processed energy-dense foods (in lieu of nutrient dense foods) oCreates scenarios where a person is not only
malnourished or nutrient deficient but also obese

Take Away o Growing evidence to demonstrate that dietary health and
lifestyle can influence hearing and tinnitus oAnimal and human
oLikely direct and indirect effects
o Questions remain? oDoes source matter: diet vs. supplements?
o Will a supplement offer additional protection in a human that already eats healthy?
oIndividualized: nutrigenomics? o Interactions with medications?
oCan I just take a pill?
oDoes type of acquired loss matter? o Long term vs. short term
o Need longitudinal and case-control studies

Summary o An number of non-modifiable and modifiable
factors contribute to acquired hearing loss
o Determining modifiable factors and their potential
to mitigate or exacerbate risk of hearing loss is
critical for public health efforts for prevention
o Then doing something about it!
oBehavioral change is not easy
Hans Bernhard, 1981 from wikimedia