Diarrhea ER
24
UNIVERSIDAD DE MANILA (Formerly City College of Manila) Mehan Garden, Manila College of Nursing Case Study in a Patient with Diarrhea IN PARTIAL FULFILLMENTOF THE REQUIREMENTS IN NCM 105 (RELATED LEARNING EXPERIENCE) III Submitted by: Robles, Ceelin T. Nr-42/Group IV Submitted to: Mr.Ben O. De Paz, RN MAN Clinical Instructor Date Submitted:
-
Upload
ceelin-robles -
Category
Documents
-
view
222 -
download
0
Transcript of Diarrhea ER

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 1/24
UNIVERSIDAD DE MANILA(Formerly City College of Manila)
Mehan Garden, ManilaCollege of Nursing
Case Study in a Patient with Diarrhea
IN PARTIAL FULFILLMENTOF THE REQUIREMENTS IN
NCM 105
(RELATED LEARNING EXPERIENCE)
III
Submitted by:
Robles, Ceelin T.
Nr-42/Group IV
Submitted to:
Mr.Ben O. De Paz, RN MANClinical Instructor
Date Submitted:

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 2/24
Table of Contents
I. Introduction
II. Objectives
III. Patient's Health History
a. Demographic Data
b. Admission Data
c. Chief complaint
d. History of Present Illness
e. Past medical History
f. Family Medical History
IV. Gordon's Functional Health Pattern
V. Physical Examination
VI. Laboratory Examinations
VII. Drugs Study
VIII. Nursing Care Plan
IX. Anatomy and Physiology
X. Pathophysiology
I. Introduction

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 3/24
Diarrhea is the passage of loose and watery stools (more than 3
bowel movements per day) often associated with gassiness, bloating,
and abdominal pain. It may also be accompanied by nausea, vomiting,
and fever.
Diarrhea results to loss of body fluids and salts leading to
dehydration of varying severity. Severe dehydration may cause death
especially in children and the elderly.
Diarrhea can be brought by different etiologic causes such as
infection due to: virus (Rotavirus, Hepatitis B virus), bacteria (Cholera,
Shigella), and intestinal parasites (E. histolytical, ponworm), these
microorganisms are usually spread by contaminated hands, or through
food and water. Food intolerance (lactose deficiency, spicy food) and
use of laxative and antacid (magnesium hydroxide) can also be a
cause. In addition the use of antibiotics like tetracycline and
cephalosporins, an inflammatory bowel disease (ulcerative colitis) can
brought diarrhea. Moreover emotional stress
and a cancer of the colon (characterized by alternating diarrhea andconstipation) can also be included in the factors that causes diarrhea.
Diarrhea is classified as either acute or chronic. Acute diarrhea is
the sudden onset of abnormally frequent watery stools accompanied
by weakness, flatulence (farting), abdominal pain and sometimes fever
and vomiting. It may be caused by eating spoiled food. This lasts for 2
to 5 days.
Chronic diarrhea lasts for more than 2 weeks and is associated
with weight loss and anemia. This is usually caused by chronic use of
laxatives or amoebiasis.
A patient should consult a physician if he/she is less than 3 years
old; if the patient is a pregnant woman; if diarrhea is associated with
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 4/24
fever and dehydration; if diarrhea continues for more than 3 days; if
diarrhea is associated with bloody, mucoid stools (dysentery); and if
diarrhea is associated with abdominal tenderness and cramping.
Diarrhea can be managed through prevention of excessive los of and sodium that if severe can leads to dehydration and loss of salts. To
prevent these life threatening problems particularly in children and the
elderly, oral rehydration solution must be given as early as possible.
The cause of the diarrhea should be identified and treated especially if
the diarrhea was caused by bacteria (Shigella, Enterotoxigenic
Escherichia coli) should be treated with antibiotics like cotrimoxazole
and fluoroquinolones. Diarrhea caused by protozoa (Entamoeba
histolytica and Giardia lamblia) should be treated with metronidazole
in combination with other anti-amoebic drugs.
Provide symptomatic relief in adults, antidiarrheal agents like
loperamide and attapulgite may help in reducing the frequency of
bowel movement and in improving the consistency of stool of stools.
Consult your doctor if diarrhea is severe especially in children
and the elderly.
Always remember that one should to eat to prevent or minimize
nutritional damage, should also drink water during their illness,
especially if they have fever. Clients should be monitored closely,
particularly children who do not show a clear improvement within 2
days after beginning treatment with an effective antibiotic. Since most
of diarrhea-causing micro-organisms are spread by contaminated
hands, thorough hand washing with soap and water and careful
cleaning of all parts of the hand is an important measure to prevent
diarrhea.
II. Objectives
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 5/24
General Objectives
At the end of our case study, the researchers will be able to
develop and enhance our nursing skills and responsibilities on how to
care for a patient with Diarrhea and be able to identify the nursing
interventions that will be appropriate with the client.
Specific Objectives
1) To be able to assess the client with Diarrhea and know the disease
process using the established assessment.
2) To be able to understand the pathophysiology of Diarrhea in relation
to client’s condition.
3) To be able to make a Nursing Care Plan based from the obtained
datas from the client.
4) To be able to determine the appropriate interventions for the
client’s specific condition.
5) To be able to determine complications associated with Diarrhea that
requires further assessment and treatment.
III. Patient History
A. Demographic Data
A case of a 8 months old, female, single, Roman Catholic and
currently residing at Paco, Manila.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 6/24
B. Admission Data
The client was admitted for the second time at Ospital ng
Maynila Medical Center, admitted last September 4, 2011, 1:00 am.When he arrived she was accompanied by her mother. During nurse-
client interaction with the help of her mother, the client was conscious.
C. Chief Complaint
The client was admitted with a chief complaint of fever of 38.5
and diarrhea.
D. History of Presnt Illness
5 days prior to admission, the client started to have watery stool
and consumed 12 diapers a day. According to the mother the client is
irritable, had difficulty in sleeping and had a on and off fever of 38.5 C.
They consulted at Valentina Health Center, and gave them Oresol, Zinc
Vitamins and Paracetamol drops for fever.
E. Past Medical History
According to the mother when the client was 5 months old she
had UTI and occasional fever. There was no injury nor accident and no
allergies to food and drugs as well. She had been vaccinated with BCG,
Hepa A and B, DPT and OPV at Valentina Health Center. Her current
mediactions are Ascorbic Acid (Ceelin) and Growee oral drops.
F. Family Medical History
The client’s mother is 30 years old and has asthma for 12 years
while her father is 30 years old and apparently well. Her older sister
who is now 2 years old has an allergy to chocolate and milk.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 7/24
Asthma
Allergy:
Chocolate &Milk
Legend:
Female
Male
Client
IV. Gordon’s Functional Health Pattern
HealthPattern
BeforeHospitalization
DuringHospitalization
Analysis
Health
Perception
Health
Management
Not Applicable Not Applicable Not Applicable
30 30
8 mos. 2
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 8/24
Pattern
Nutritional
metabolic
Pattern
The client’
mother stated
that client ate
three-five times
a day and ate
what her mother
prepared for her
like mashed
potato, banana,
and carrots. She
had increased in
appetite. She
consumes 8-10bottles of milk (6
oz) per day.
Now, the client
decreased
appetite. The
client has dry
lips, sunken
eyes and
depressed
fontanels. D5IMB
500 mL was
inserted on
clients left foot
for fluid and
electrolytereplacement.
The client’s
nutritional and
metabolic
pattern
changed
because of the
client’s current
condition.
Elimination
Pattern
According to the
mother of the
client, she had
regular bowel
habit. She
defecated once
to twice a day
and it is
characterized by
semi- solid,
yellowish brown
in color and soft.
She also had
good bladder
habit; she
usuallyconsumed 6-8
diaper a day it is
described as
light yellow in
color and
moderate
Now, the clients
consumed 12
diapers per day
with soft watery
stool.
Elimination
pattern was
affected
because of the
client’s current
condition.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 9/24
amount.
Activity
Exercise
The client was
able to do the
following with
the help of the
mother since her
physical ability is
limited due to
her is still a
baby: eating,
bathing,
dressing and
toileting. Her
mother regularlymassages her
lower
extremities.
Now, the client
has less energy,
and cannot
further more do
activities like
rolling, crawling.
Activity and
exercise is
being
influenced by
present health
condition of
patient itself.
Sleep Rest
Pattern
According to the
mother, client
had total of 8-12
hours of sleep
and seems to be
felt rested after
sleep.
Now, the client
usually has 6-8
hours of sleep,
experiencing
awakening at
night and
difficulty of
sleeping. The
method that the
mother used to
promote sleep is
positioning her
comfortably.
Sleep rest
pattern is being
altered due to
the client’s
present health
condition.
Cognitive
Perception
Pattern
Not Applicable Not Applicable Not Applicable
Self Perception Not Applicable Not Applicable Not Applicable

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 10/24
Self Concept
Pattern
Role
Relationship
Pattern
Not Applicable Not Applicable Not Applicable
Sexuality
Reproductive
Pattern
Not Applicable Not Applicable Not Applicable
Coping Stress
Tolerance
Pattern
Not Applicable Not Applicable Not Applicable
Value Belief
Pattern
Not Applicable Not Applicable Not Applicable
V. Physical assessment

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 11/24
General Survey
The client is an 8 months old female. Appears and behaves to be
as his apparent age. She has a light brown skin complexion; she is
clean and neat as well. The client is appeared irritable, has a good
posture and has coordinated body movement.
Interaction and answering of questions was done with the help of
his mother; the one who accompanied him in the hospital.
Vital signs
The client’s vital signs prior to the physical examination were
temperature of 38.4 oC, pulse rate of 123 bpm, and respiratory rate of
54 bpm.
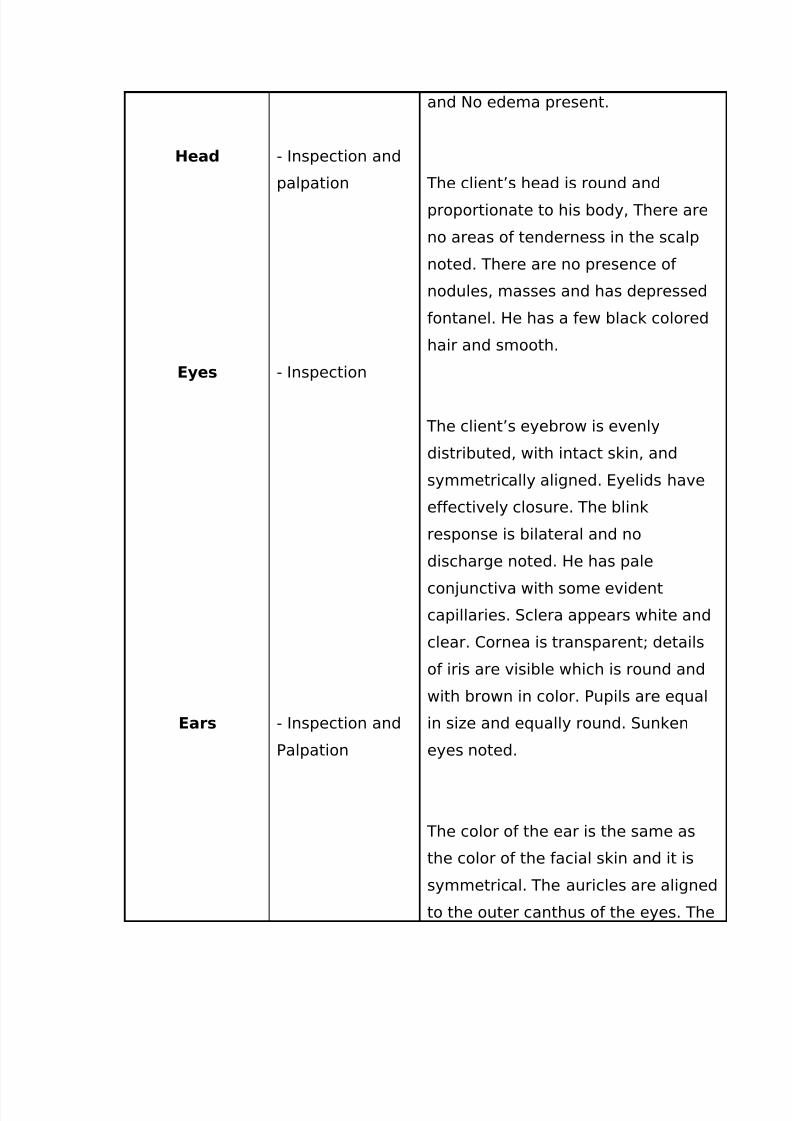
Head to toe Physical Examination
Area of Assessment
Type of Assessment
UsedFindings
Skin - Inspection and
Palpation
The client has light brown color of
the skin with dry poor skin turgor. It
is warm to touch which was noted to
be similar on the both sides of his
body. The client’s skin is free from
lesion, abrasion nor inflammation.
The body hair is evenly distributed
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 12/24
Head
Eyes
Ears
- Inspection and
palpation
- Inspection
- Inspection and
Palpation
and No edema present.
The client’s head is round and
proportionate to his body, There are
no areas of tenderness in the scalp
noted. There are no presence of
nodules, masses and has depressed
fontanel. He has a few black colored
hair and smooth.
The client’s eyebrow is evenly
distributed, with intact skin, and
symmetrically aligned. Eyelids have
effectively closure. The blink
response is bilateral and no
discharge noted. He has pale
conjunctiva with some evident
capillaries. Sclera appears white and
clear. Cornea is transparent; details
of iris are visible which is round and
with brown in color. Pupils are equal
in size and equally round. Sunken
eyes noted.
The color of the ear is the same as
the color of the facial skin and it is
symmetrical. The auricles are aligned
to the outer canthus of the eyes. The
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 13/24
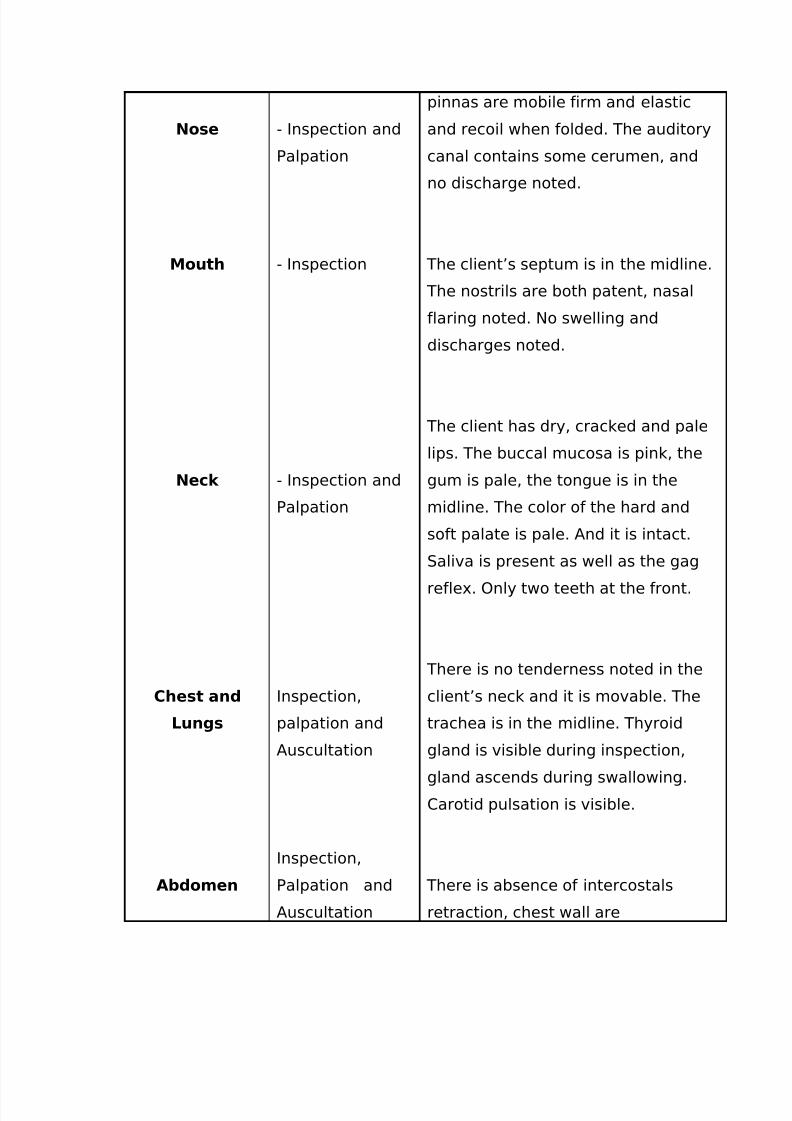
Nose
Mouth
Neck
Chest and
Lungs
Abdomen
- Inspection and
Palpation
- Inspection
- Inspection and
Palpation
Inspection,
palpation and
Auscultation
Inspection,
Palpation and
Auscultation
pinnas are mobile firm and elastic
and recoil when folded. The auditory
canal contains some cerumen, and
no discharge noted.
The client’s septum is in the midline.
The nostrils are both patent, nasal
flaring noted. No swelling and
discharges noted.
The client has dry, cracked and pale
lips. The buccal mucosa is pink, the
gum is pale, the tongue is in the
midline. The color of the hard and
soft palate is pale. And it is intact.
Saliva is present as well as the gag
reflex. Only two teeth at the front.
There is no tenderness noted in the
client’s neck and it is movable. The
trachea is in the midline. Thyroid
gland is visible during inspection,
gland ascends during swallowing.
Carotid pulsation is visible.
There is absence of intercostals
retraction, chest wall are
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 14/24
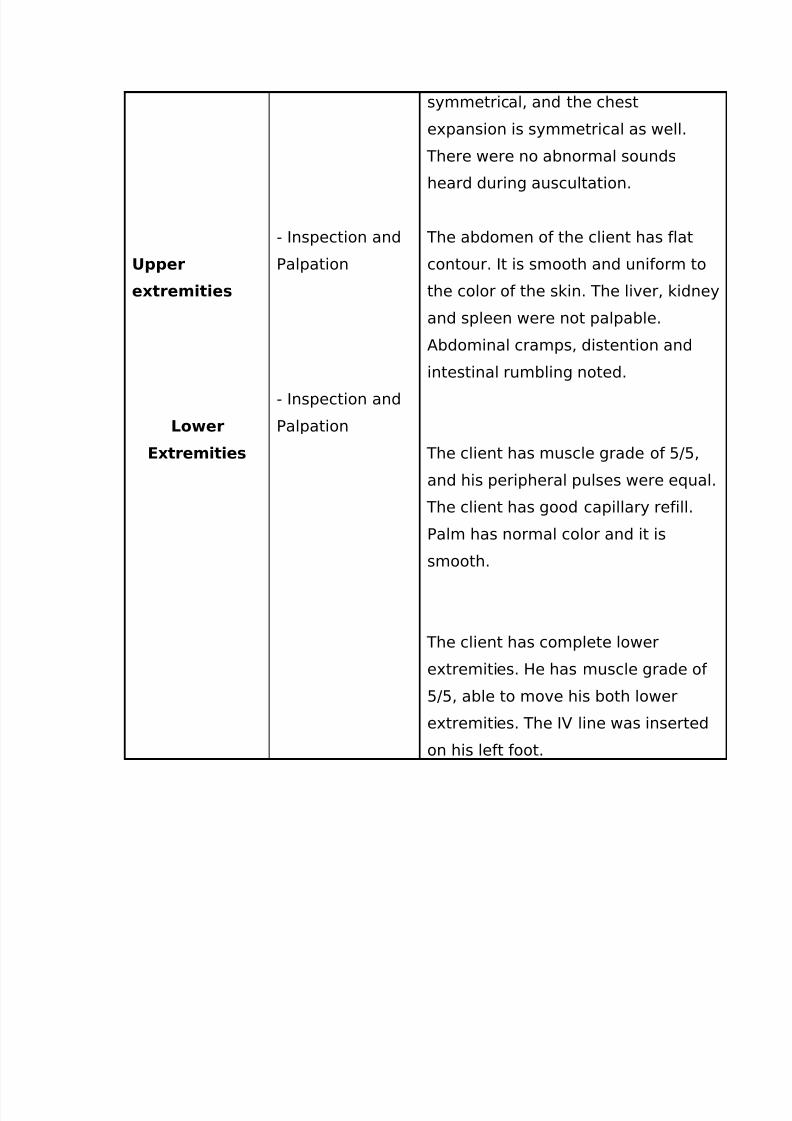
Upper
extremities
Lower
Extremities
- Inspection and
Palpation
- Inspection and
Palpation
symmetrical, and the chest
expansion is symmetrical as well.
There were no abnormal sounds
heard during auscultation.
The abdomen of the client has flat
contour. It is smooth and uniform to
the color of the skin. The liver, kidney
and spleen were not palpable.
Abdominal cramps, distention and
intestinal rumbling noted.
The client has muscle grade of 5/5,
and his peripheral pulses were equal.
The client has good capillary refill.
Palm has normal color and it is
smooth.
The client has complete lower
extremities. He has muscle grade of
5/5, able to move his both lower
extremities. The IV line was inserted
on his left foot.
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 15/24
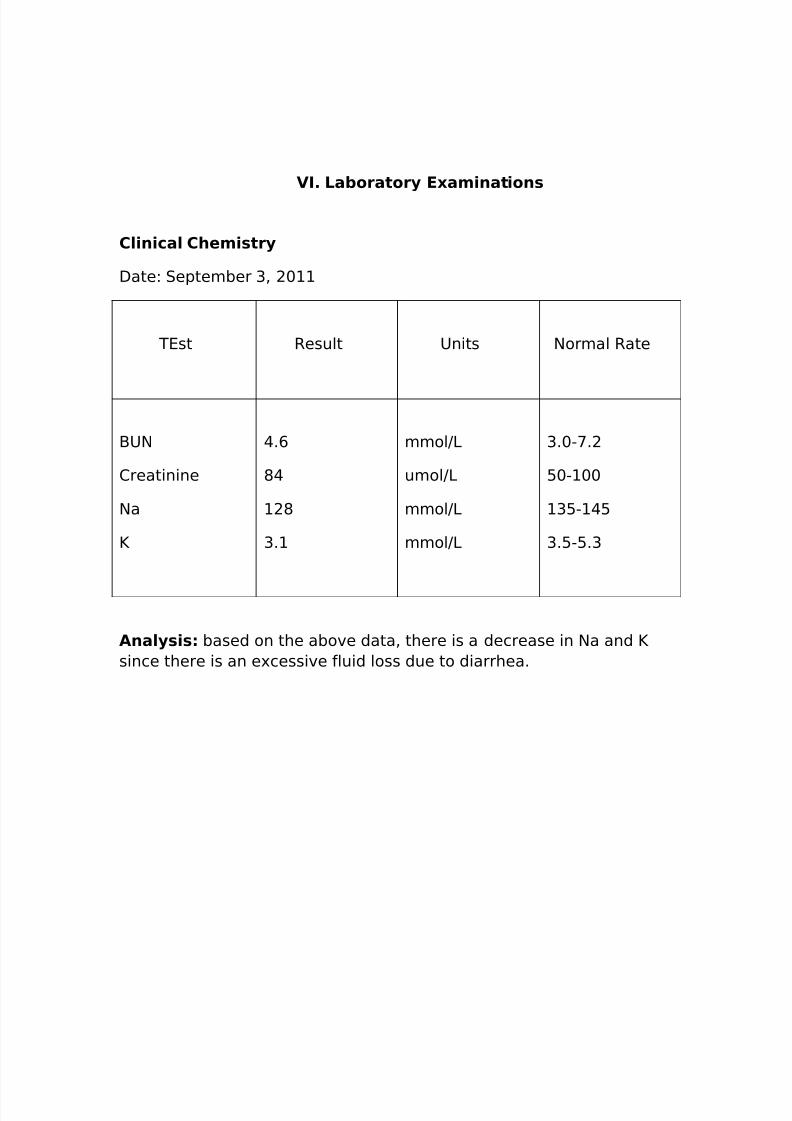
VI. Laboratory Examinations
Clinical Chemistry
Date: September 3, 2011
TEst Result Units Normal Rate
BUN
Creatinine
Na
K
4.6
84
128
3.1
mmol/L
umol/L
mmol/L
mmol/L
3.0-7.2
50-100
135-145
3.5-5.3
Analysis: based on the above data, there is a decrease in Na and K
since there is an excessive fluid loss due to diarrhea.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 16/24
Urinalysis
Date: June 28, 2008
Color: Yellow
Appearance: Clear
Specific gravity: 1.029
Protein (Albumin): Negative
Glucose: Negative
Bacteria: Negative
Analysis: Since the specific gravity is not in a normal range, it
indicates that the client has concentrated urine that maybe the result
of dehydration and fever.
Fecalysis
Date: September 2, 2011
Macroscopic appearance:
Color: yellow
Consistency: Soft
Microscopic appearance:
Pus cells: none seen /hpf
RBC: none seen /hpf
Fat globules: none seen / hpf
Bacteria: Few

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 17/24
Analysis: Fecalysis indicates that there is few bacteria presented in
the fecal, this may indicate that it is positive in infection.
IX. Anatomy and Physiology
THE DIGESTIVE SYSTEM
Consists of (1) an alimentary canal- a long muscular tube beginning at
the lips and ending at the anus, including the mouth, pharynx (oral and
laryngeal portions), esophagus, stomach, and small and large
intestine, and (2) accessory glands that empty secretions into the
tube- salivary glands, pancreas, liver, and gallbladder.
1. Teeth
a. Crown projects above the gum, root below. Dentin (bulk of tooth)
surrounds pulp cavity. Enamel covers dentin of crown;
cementum covers dentin of root and anchors tooth to periodontal
ligament.
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 18/24
b. Each quadrant of mouth has eight teeth-two incisors, one canine,
two premolars, and three molars.
1. Esophagus
a. Mucous membrane lined with stratified squamous epitheliumrather than simple columnar epithelium, as in stomach and
intestine,
b. Muscular layer of upper third, striated; lower third, smooth;
middle, both striated and smooth.
c. Segment above stomach (indistinguishable anatomically from
remainder of esophagus) functions as sphincter, remaining
closed until reflexively relaxed as peristaltic wave approaches,
1. Stomacha. Consists of upper fundus, central body, and constricted lower
pyloric portion (antrum).
b. Musculature contains an oblique inner layer of smooth muscle in
addition to external longitudinal and underlying circular smooth
muscle layers found elsewhere in digestive tract.
c. Thick circular muscle in pyloric portion forms pyloric sphincter.
d. Openings: cardia, between esophagus and stomach; pylorus,
between stomach and duodenum.
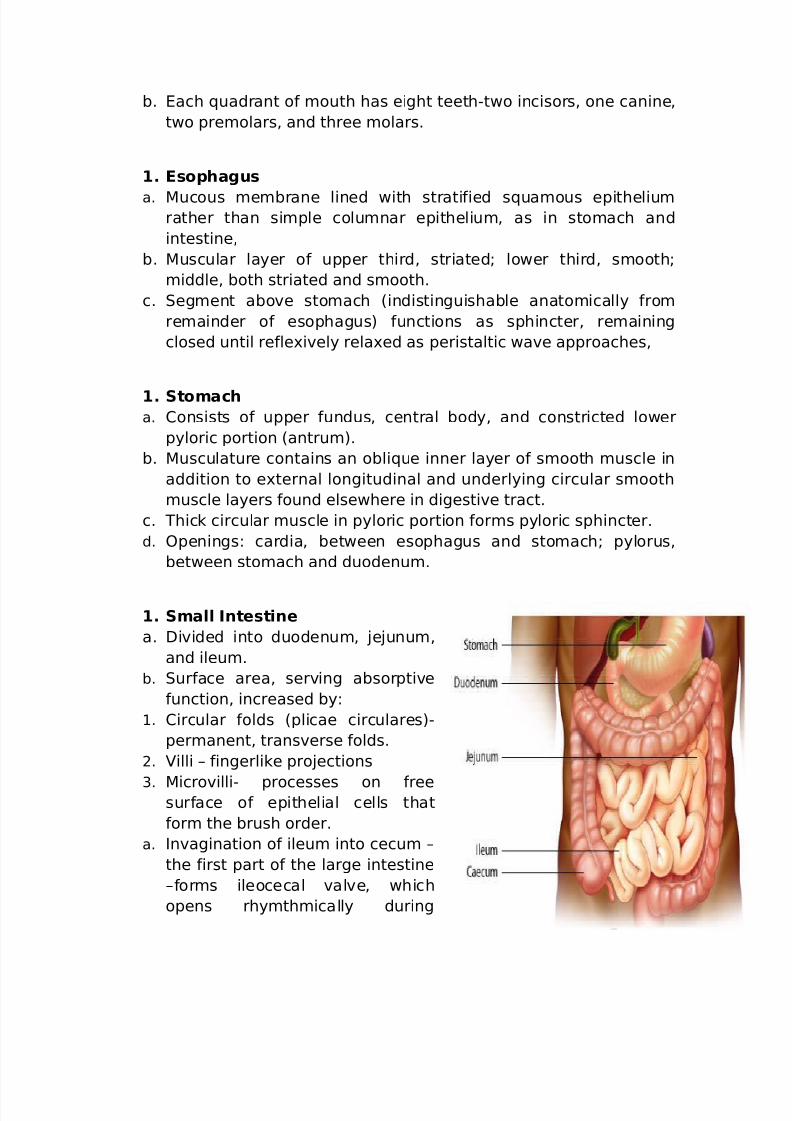
1. Small Intestine
a. Divided into duodenum, jejunum,
and ileum.
b. Surface area, serving absorptive
function, increased by:
1. Circular folds (plicae circulares)-
permanent, transverse folds.
2. Villi – fingerlike projections
3. Microvilli- processes on freesurface of epithelial cells that
form the brush order.
a. Invagination of ileum into cecum –
the first part of the large intestine
–forms ileocecal valve, which
opens rhymthmically during

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 19/24
digestion, permitting gradual emptying of ileum and preventing
regurgitation.
5. Large Intestine
a. Extends from the end of the ileum to the anus and is divisible
into the cecum, colon, rectum, and anal canal. The major part is the
colon, which consists of ascending, transverse, descending, and
sigmoid portions.
b. The longitudinal muscle of the cecum and colon forms three
conspicuous bands(taeniae coli).
c. Thickene circular smooth muscle of anal canal forms the internal
anal sphincter. Surrounding skeletal muscle forms the external
sphincter.
6.Salivary Glands
a. Three pairs (parotid, submaxillary, and sublingual), with ducts
opening into the mouth.
b. Two types of secretions:
1. Serous containing ptyalin –enzyme initiating digestion of the
starch.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 20/24
2. Mucous – viscous, containing mucus, which facilitates
mastication.
7. Pancreas
a. Two types of secretory cells in
exocrine pancreas:
1. Enzyme- secreting acinar cells.
2. Bicarbonate-and-water-secreting
–intralobular duct cells.
b. Pancreatic duct empties
pancreatic juice into duodenum.
8. Liver and Gallbladder
a. Bile secreted by liver is essential
for normal absorption of digested
lipids. Bile salts combine with
products of lipid digestion to formwater-soluble complexes (micelles)
which are absorbed by intestinal cells.
b. Gallbladder concentrates and stores bile.
c. Hepatic duct, formed from the bile duct system of liver, joins
cystic duct of gallbladder to form common bile duct, which empties
into duodenum.
Motility of Digestive Tract
1. Swallowing
a. In buccal stage (voluntary) bolus pushed toward pharynx.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 21/24
b. In pharyngeal and esophageal stages (involuntary) bolus
passes through pharynx into esophagus and through
esophagus into stomach.
c. Reflexes raise soft palate, raise larynx, adduct aryepiglottic
folds and true and false vocal cords, and inhibit respiration.
When food enters the pharynx, reflex contraction of the
superior constrictor muscle initiates peristalsis, propelling
the food, and relaxation of the upper and lower esophageal
sphincters allows food to pass first into the esophagus and
then into the stomach.
1. Peristalsis in Stomach
a. Mixes contents and forces chime through pylorus.
b. Three waves each beginning every 20 seconds near
midpoint of stomach, lasting about one minute, and ending
with contraction of pyloric sphincter travel down stomachat one time.
c. Rate of emptying determined largely by strength of
contractions.
d. Feedback from duodenum regulates gastric emptying. Two
control mechanisms, one neuronal (enterogastric reflex),
the other hormonal (mediated mainly by enterogastrone),
inhibit gastric motility.
1. Contractions of the Small Intestine
a. Segmenting: rhythmic contractions along a section
dividing it into segments: primarily mixing action.
b. Peristaltic waves superimposed upon segmenting
contractions.
c. Ingestion of food increases ileal peristalsis and frequency
of opening of ileocecal valve (gastroileal reflex).
1. Contractions of Large Intestine
a. Simultaneous contraction of circular and longitudinal
muscle, forming haustra,
b. Infrequent usually two or three times daily of most mass
movements transferring contents from proximal to distalcolon and into rectum. Most commonly occur shortly after
a meal (gastrocolic reflex).
1. Defecation reflex
a. Distention of rectum triggers intense peristaltic
contractions of colon and rectum and relaxation of internal
anal sphincter.

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 22/24
b. Reflex preceded by voluntary relaxation of external
sphincter and compression of abdominal contents.
Digestion
1. Mouth
a. Enzymatic action: initiation of the digestion of carbohydrate by
ptyalin, which splits starch into the disaccharide maltose. Action
in mouth slight, but continues in stomach until acid medium
inactivates ptyalin.
b. Regulation: exclusively nervous- impulses transmitted from
center in medulla activated principally by taste, smell, or sight of
food to salivary glands by parasymphatetic nerve fibers.
1. Stomach
a. Enzymatic action: initiation of protein digestion by pepsin,
producing proteoses, peptones, and polypeptides. Pepsinogensecreted by chief cells converted to pepsin by autoactivation
process in presence of acid secreted by parietal cells.
b. Regulation
1. Cephalic phase- initiated by taste, sight, or smell of food;
secretion stimulated directly or indirectly by the hormone
gastrin. Gastrin, released from so called G cells in the pyloric
region of the stomach, stimulates the secretion of an acid-rich
gastric juice.
2. Gastric phase- initiated by food in stomach; secretion triggered
directly or indirectly, as in cephalic phase.
3. Intestinal phase- initiated by digestive products in upper small
intestine; mediated by hormone released by duodenum acting on
stomach.
4. Inhibition- strong acid in antrum inhibits gastrin release. Fat,
acid, or hypertonic salt solutions in duodenum stimulate release
of hormones which inhibit gastric secretion.
8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 23/24
1. Intestine
a. Enzymatic action- fat digestion and continuation of carbohydrate
and protein digestion.
1. Pancreatic lipase splits fat into monoglycerides, fatty acids, andglycerol.
2. Pancreatic amylase converts starch and glycogen into maltose.
Intestinal disaccharidases split maltose, sucrose, and lactose into
their constituent monosaccharides,
3. Pancreatic enzymes trypsin and chymotrypsin both
endopeptidases split proteins and the products of pepsin
digestion into peptides. Peptidases split peptides into amino
acids.
b.. Regulation of pancreatic secretion: by vagus nerve during
cephalic and gastric phase of gastric secretion and by two duodenal
hormones-cholecystokinin-pancreozymin and sectetin. Vagus
stimulation and cholecystokinin-pancreaozymin stimulate enzyme
secretion; secretin stimulates bicarbonate secretion.
Absorption
1. Occurs almost exclusively in the small intestine.
2. Simple sugars, amino acids, short-chain fatty acids, and glycerol
are absorbed into blood stream via capillary network of villi.
Products of lipid digestion are absorbed as chylomicrons into
intestinal lymphatics via central lacteal of villi.
Digestion process- the digestive system prepares food for
consumption by the cells through five basic activities:
1. Ingestion- is an active, voluntary process of taking in food. Food
must be placed in the mouth before it can be acted on.
2. Propulsion is movement of food along the digestive tract.
Swallowing is one example of food movement that depends
largely on the propulsive process called peristalsis. Peristalsis is

8/3/2019 Diarrhea ER
http://slidepdf.com/reader/full/diarrhea-er 24/24
involuntary and involves alternating waves of contraction and
relaxation of the muscles in the organ wall to squeeze food along
the tract.
3. Digestion- the breakdown of food by both chemical and
mechanical processes.
4. Absorption- the passage of digested food from the digestive tract
into the cardiovascular and lymphatic systems for distribution to
cells. For absorption to occur, the digested foods must first enter
the mucosal cells by active or passive transport processes. The
small intestine is the major absorptive site.
5. Defecation- the elimination of indigestible substances from the
body.
X. Pathophysiology
(+)Staphylococcus aureus
toxin binds to mucosal cells
secretory diarrhea mediated by cyclic AMP
Increased production of fluids and electrolytes by the intestinal mucos
Increased secretion of fluids and electrolytes by the intestinal mucos