Diagnosis of inherited metabolic disorders affecting the ... · The aminoacidurias include...
11
40ourmal of Neurology, Neurosurgery, and Psychiatry 1995;59:460-470 NEUROLOGICAL INVESTIGATIONS Diagnosis of inherited metabolic disorders affecting the nervous system Phillip D Swanson The number of metabolic disorders that can produce neurological symptoms is daunting. The clinician cannot simply send off to the laboratory a blood sample and ask for a meta- bolic "screen" that will detect a hypothetical metabolic abnormality. The range of possible conditions must be narrowed to the most likely before deciding which investigative approach should be taken. Most biochemical disorders encountered by neurologists are genetically determined. Thus one of the most important elements of the history is the family history. It is not sufficient to ask "has anyone in your family had a neurological problem?". The clinician must be aware of the different forms of inheritance patterns (autosomal dominant, autosomal recessive, X linked, mitochondrial) and must obtain enough information to construct a meaningful family tree. Directed questions must be asked about siblings as well as parents, grandparents, uncles, aunts, cousins, and children. Table 1 lists features that characterise single gene inheritance patterns. 1'3 Most of the clear cut genetic diseases are due to single gene abnormalities.There are several different mechanisms, however, that produce abnormal genes. A point mutation of a single DNA nucleotide can result in a different amino acid being coded for in the resulting polypeptide or protein. There can be deletion of a segment of a gene or insertion of one or more nucleotides. Duplication of a gene has been reported in Charcot-Marie- Tooth disease type IA. Unstable expansions of portions of a gene (trinucleotide repeats) are being increasingly found in autosomal Table 1 Some characteristics of single gene inheritance Type of inheritance Charactenrstics Autosomal dominant Multiple generations affected Father to son transmission (rules out X linked and mitochondrial inheritance patterns) Males and females equally affected Autosomal recessive Only siblings affected Parental consanguinity common Males and females equally affected X Linked Never father to son transmission Transmission through unaffected mothers Only males affected (rare exceptions) 50% risk to sons of carrier women All daughters of affected men are carriers Mitochondrial Maternally inherited Never father to child transmission Both sons and daughters can be affected Adapted from table 9-1.3 dominant neurodegenerative diseases. The pace of new discoveries in medical genetics is incredibly rapid. Many of the new discoveries have led to diagnostic methods that were unanticipated only a few years ago. Certain terms used by medical geneticists should be familiar to neurological practition- ers. Anticipation refers to a disease beginning earlier and often being more severe in succeeding generations. In some autosomal dominant disorders, such as myotonic dystrophy and spinocerebellar ataxia 1, this phenomenon seems to be related to the length of an expanded trinucleotide repeat in the abnormal gene.4 Penetrance refers to the proportion of subjects with the abnormal gene who will develop symptoms if they live long enough. The degree of expression of a genetic disease refers to the variation of sever- ity of the phenotype that is seen in a patient population. Mosaicism refers to variation among different cells and tissues in the chro- mosome complement. This occurs normally in women due to lyonisation, in which one of each cell's two X chromosomes is randomly inactivated. Mitochondrial disorders (see later) are associated with heteroplasmy, a term that refers to variation in the proportion of normal or genetically abnormal mitochondria in different tissues. In autosomal dominant disorders, multiple generations are usually affected, although this might not have occurred if the affected patient represents a new mutation. Male to male transmission only occurs with au'toso- mal dominant transmission. Each child of an affected parent will have a 50% chance of having or not having the abnormal gene. Autosomal recessive disorders occur when expression of the disease requires the abnor- mal gene to be inherited from both parents, so that the affected person's cells have two abnormal alleles. Many autosomal recessive disorders are associated with defective enzymes. The low level of enzyme activity often leads to accumulation of the enzyme substrate with resultant toxicity to susceptible cells. The carrier parents seldom manifest symptoms because the normal gene codes for normal enzyme that is active enough to prevent substrate accumulation. Consan- guineous marriages between cousins are more common in families with autosomal recessive diseases. Department of Neurology, Box 356427, University of Washington School of Medicine, Seattle, WA 98195, USA P D Swanson 460 on 2 October 2018 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.59.5.460 on 1 November 1995. Downloaded from
Transcript of Diagnosis of inherited metabolic disorders affecting the ... · The aminoacidurias include...

40ourmal ofNeurology, Neurosurgery, and Psychiatry 1995;59:460-470
NEUROLOGICAL INVESTIGATIONS
Diagnosis of inherited metabolicdisorders affecting the nervous system
Phillip D Swanson
The number of metabolic disorders that canproduce neurological symptoms is daunting.The clinician cannot simply send off to thelaboratory a blood sample and ask for a meta-bolic "screen" that will detect a hypotheticalmetabolic abnormality. The range of possibleconditions must be narrowed to the mostlikely before deciding which investigativeapproach should be taken. Most biochemicaldisorders encountered by neurologists aregenetically determined. Thus one of the mostimportant elements of the history is the familyhistory. It is not sufficient to ask "has anyonein your family had a neurological problem?".The clinician must be aware of the differentforms of inheritance patterns (autosomaldominant, autosomal recessive, X linked,mitochondrial) and must obtain enoughinformation to construct a meaningful familytree. Directed questions must be asked aboutsiblings as well as parents, grandparents,uncles, aunts, cousins, and children. Table 1lists features that characterise single geneinheritance patterns.1'3Most of the clear cut genetic diseases are
due to single gene abnormalities.There areseveral different mechanisms, however, thatproduce abnormal genes. A point mutation ofa single DNA nucleotide can result in adifferent amino acid being coded for in theresulting polypeptide or protein. There canbe deletion of a segment of a gene or insertionof one or more nucleotides. Duplication of agene has been reported in Charcot-Marie-Tooth disease type IA. Unstable expansionsof portions of a gene (trinucleotide repeats)are being increasingly found in autosomal
Table 1 Some characteristics of single gene inheritance
Type of inheritance CharactenrsticsAutosomal dominant Multiple generations affected
Father to son transmission (rules out X linked andmitochondrial inheritance patterns)Males and females equally affected
Autosomal recessive Only siblings affectedParental consanguinity commonMales and females equally affected
X Linked Never father to son transmissionTransmission through unaffected mothersOnly males affected (rare exceptions)50% risk to sons of carrier womenAll daughters of affected men are carriers
Mitochondrial Maternally inheritedNever father to child transmissionBoth sons and daughters can be affected
Adapted from table 9-1.3
dominant neurodegenerative diseases. Thepace of new discoveries in medical genetics isincredibly rapid. Many of the new discoverieshave led to diagnostic methods that wereunanticipated only a few years ago.
Certain terms used by medical geneticistsshould be familiar to neurological practition-ers. Anticipation refers to a disease beginningearlier and often being more severe insucceeding generations. In some autosomaldominant disorders, such as myotonicdystrophy and spinocerebellar ataxia 1, thisphenomenon seems to be related to thelength of an expanded trinucleotide repeat inthe abnormal gene.4 Penetrance refers to theproportion of subjects with the abnormalgene who will develop symptoms if they livelong enough. The degree of expression of agenetic disease refers to the variation of sever-ity of the phenotype that is seen in a patientpopulation. Mosaicism refers to variationamong different cells and tissues in the chro-mosome complement. This occurs normallyin women due to lyonisation, in which one ofeach cell's two X chromosomes is randomlyinactivated. Mitochondrial disorders (seelater) are associated with heteroplasmy, a termthat refers to variation in the proportion ofnormal or genetically abnormal mitochondriain different tissues.
In autosomal dominant disorders, multiplegenerations are usually affected, although thismight not have occurred if the affectedpatient represents a new mutation. Male tomale transmission only occurs with au'toso-mal dominant transmission. Each child of anaffected parent will have a 50% chance ofhaving or not having the abnormal gene.
Autosomal recessive disorders occur whenexpression of the disease requires the abnor-mal gene to be inherited from both parents,so that the affected person's cells have twoabnormal alleles. Many autosomal recessivedisorders are associated with defectiveenzymes. The low level of enzyme activityoften leads to accumulation of the enzymesubstrate with resultant toxicity to susceptiblecells. The carrier parents seldom manifestsymptoms because the normal gene codesfor normal enzyme that is active enough toprevent substrate accumulation. Consan-guineous marriages between cousins are morecommon in families with autosomal recessivediseases.
Department ofNeurology, Box356427, University ofWashington School ofMedicine, Seattle, WA98195, USAP D Swanson
460 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from
Diagnosis of inherited metabolic disorders affecting the nervous system
X Linked disorders are due to abnormalgenes located on the X chromosome. Clinicaldisease characteristically occurs in males whohave inherited the abnormal gene from a
carrier mother. Occasionally the mother or
daughter with one normal and one abnormalgene will manifest symptoms, which almostalways are milder than in the affected son or
father, who has only one X chromosome.Male to male transmission cannot occur
because a son receives the X chromosomefrom his mother.
Mitochondrial disorders are due to abnor-malities in genes (deletions, point mutations)located in mitochondrial DNA. Both maleand female mitochondria are derived from theovum rather than the sperm. Both males andfemales can be affected by mitochondrialdisorders, but father to child transmissiondoes not occur. Because tissues and cells varyin the proportion of normal and abnormalmitochondria they carry (heteroplasmy), theexpression of the disorder in different tissuesand in different subjects can be extremelyvariable.
This contribution will not include muchdiscussion of diseases that primarily affectmuscle or nerve, as these have been thesubjects of previous articles in this series.Some metabolic conditions, however, includ-ing metachromatic leukodystrophy andcertain mitochondrial disorders that affectboth central and peripheral structures, will beincluded. Non-genetic metabolic conditionssuch as hypoglycaemia, hepatic encephalo-pathy, deficiency diseases, and electrolytedisorders will not be discussed. Emphasis willbe on conditions that are seen in adults byneurologists but many of these disorders willbe variants of diseases that usually have theirfirst manifestations in infancy or childhood.The first section contains brief discussions ofcategories of metabolic disease likely to be
encountered by neurologists. The secondsection contains a discussion of differentialdiagnoses of metabolic conditions that mightproduce particular complexes of neurologicalsymptoms, including mental retardation,dementia, ataxias, motor neuron disease,movement disorders, and stroke.
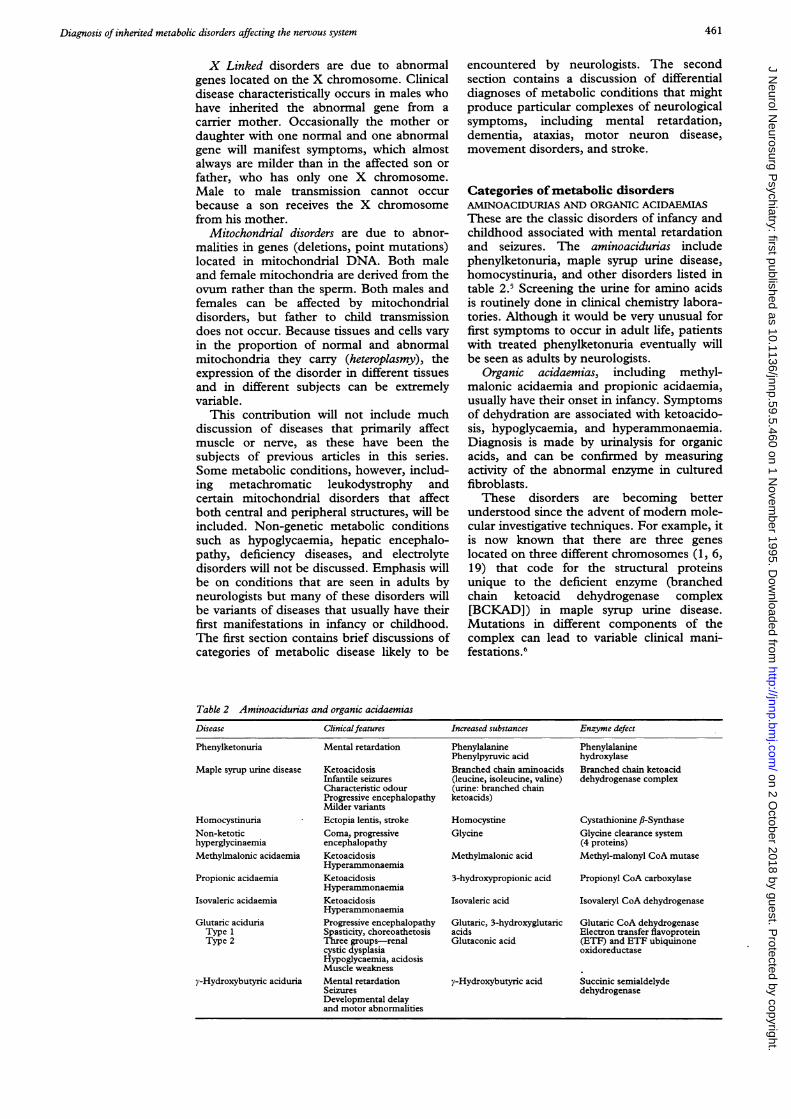
Categories of metabolic disordersAMINOACIDURIAS AND ORGANIC ACIDAEMIASThese are the classic disorders of infancy andchildhood associated with mental retardationand seizures. The aminoacidurias includephenylketonuria, maple syrup urine disease,homocystinuria, and other disorders listed intable 2.5 Screening the urine for amino acidsis routinely done in clinical chemistry labora-tories. Although it would be very unusual forfirst symptoms to occur in adult life, patientswith treated phenylketonuria eventually willbe seen as adults by neurologists.
Organic acidaemias, including methyl-malonic acidaemia and propionic acidaemia,usually have their onset in infancy. Symptomsof dehydration are associated with ketoacido-sis, hypoglycaemia, and hyperammonaemia.Diagnosis is made by urinalysis for organicacids, and can be confirmed by measuringactivity of the abnormal enzyme in culturedfibroblasts.
These disorders are becoming betterunderstood since the advent of modem mole-cular investigative techniques. For example, itis now known that there are three genes
located on three different chromosomes (1, 6,19) that code for the structural proteinsunique to the deficient enzyme (branchedchain ketoacid dehydrogenase complex[BCKAD]) in maple syrup urine disease.Mutations in different components of thecomplex can lead to variable clinical mani-festations.6
Table 2 Aminoacidurias and organic acidaemias
Disease Clinicalfeatures Increased substances Enzymne defect
Phenylketonuria Mental retardation Phenylalanine PhenylalaninePhenylpyruvic acid hydroxylase
Maple syrup urine disease Ketoacidosis Branched chain aminoacids Branched chain ketoacidInfantile seizures (leucine, isoleucine, valine) dehydrogenase complexCharacteristic odour (urine: branched chainProgressive encephalopathy ketoacids)Milder variants
Homocystinuria Ectopia lentis, stroke Homocystine Cystathionine,B-SynthaseNon-ketotic Coma, progressive Glycine Glycine clearance systemhyperglycinaemia encephalopathy (4 proteins)Methylmalonic acidaemia Ketoacidosis Methylmalonic acid Methyl-malonyl CoA mutase
HyperammonaemiaPropionic acidaemia Ketoacidosis 3-hydroxypropionic acid Propionyl CoA carboxylase
HyperammonaemiaIsovaleric acidaemia Ketoacidosis Isovaleric acid Isovaleryl CoA dehydrogenase
HyperammonaemiaGlutaric aciduria Progressive encephalopathy Glutaric, 3-hydroxyglutaric Glutaric CoA dehydrogenaseType 1 Spasticity, choreoathetosis acids Electron transfer flavoproteinType 2 Three groups-renal Glutaconic acid (ETF) and ETF ubiquinone
cystic dysplasia oxidoreductaseHypoglycaemia, acidosisMuscle weakness
y-Hydroxybutyric aciduria Mental retardation y-Hydroxybutyric acid Succinic semialdelydeSeizures dehydrogenaseDevelopmental delayand motor abnormalities
461 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

462
LYSOSOMAL DISORDERSThe term lysosome was proposed by DeDuveet al in 1955 for intracellular granules thatwere rich in hydrolytic enzymes.7 A lysosomaldisease is associated with an abnormalenzyme that results in defective breakdown ofthe enzyme substrate.8 The product accumu-
lates and eventually alters cell function.Because hydrolytic enzymes are present inmany tissues, the diagnosis of the accumu-lated product or of the enzyme deficiencyusually can be made with readily accessibletissues such as peripheral white blood cells or
skin fibroblasts.9-1" Although most of thesedisorders produce symptoms at a young age,some mutations, as in adult onset GM1gangliosidosis, lead to onset of symptomslater in life.'2
Lysosomal disorders can be subcategorisedaccording to the type of accumulated storageproduct. The two principal groups are lipidstorage diseases and mucopolysaccharidoses.As these conditions have been more fullycharacterised, it has become clear that a greatdeal of heterogeneity exists among them, inmany cases due to different point mutationsin the gene. Thus these disorders should beconsidered in the differential diagnosis ofatypical degenerative disorders.
Lipid storage diseasesTable 3 lists the lipid storage diseases thatcause neurological dysfunction. These disor-ders are diagnosed either by finding highconcentrations of substrate in tissues or byshowing pronounced reduction in concentra-tions of the lysosomal enzyme responsible fordegrading the accumulated storage substance.
In each disorder, subtypes have been delin-eated. In Gaucher's disease, associated withaccumulation of glucocerebroside, and inNiemann-Pick disease, with sphingomyelinaccumulation, hepatosplenomegaly is promi-nent in all types; however, only types 2 and 3Gaucher's disease and types A and CNiemann-Pick disease are associated withneurological deterioration. Globoid leukodys-trophy (Krabbe'6 disease), metachromaticleukodystrophy (MLD) and Tay-Sachsdisease are inherited as autosomal recessivedisorders and can be diagnosed by measure-
ment of enzyme concentrations in peripheral
white blood cells or cultured skin fibroblasts.Clinical variants are found in each disorder.In MLD some mutations in the arylsul-phatase A gene on chromosome 22 have beencorrelated with different phenotypes.IISimilarly, in Tay-Sachs disease over 20 muta-tions including nucleotide insertions, dele-tions, and substitutions on the a subunit(chromosome 15) and the subunit (chro-mosome 5) of the hexosaminidase enzyme
have been described.'4 Late onset cases may
develop weakness, fasciculations, ataxia, andpsychiatric symptoms.'5GM, gangliosidosis, due to deficiency of the
lysosomal enzyme ,B-galactosidase, canproduce symptoms in infancy, childhood, or
adult life. At least 16 mutations have beenidentified in the ,B-galactosidase gene.'2 1617Severity of the diseases can be correlated withthe amount of residual enzyme activity, theinfantile form having no demonstrable activ-ity and the adult forms having 4-8% ofnormal activity. Leinekugel et al found that10-15% of,B-hexosaminidase A and arylsul-phatase A activities were sufficient to degradesubstrate. 18
The adult form of the disorder is slowlyprogressive and may produce gait disorders,involuntary choreoathetoid movements,bradykinesia, or dementia. Storage of GM,ganglioside can be much more pronounced inthe striatum than in other parts of the brainby contrast with younger onset patients, inwhom storage is more widespread.'2 19
Diagnosis is confirmed by finding muchreduced lysosomal acid,B-galactosidase activ-ity in leucocytes. Single base mutations can
be found on the ,B-galactosidase gene. The5'isoleucine (ATC) -+ threonine (ACC)
mutation in the gene is common in Japaneseadult onset GM, gangliosidosis.'2
MucopolysaccharidosesThese lysosomal disorders are associated withaccumulation of complex glycosoaminogly-cans (mucopolysaccharides), due to geneticdefects resulting in deficiencies of degradativeenzymes.20 21 The stored substances includedermatan sulphate, heparan sulphate, keratansulphate, and chondroitin 4/6 sulphates,which are detectable in the urine. Of the 12described disorders all are autosomal recessive
Table 3 Common lipid storage diseases
Major lipid EnzymeDisease Neurological symptom accumulated defect
Gaucher's Hepatosplenomegaly, Glucocerebroside Glucocerebroside-neurological deterioration in type 2 fl-glucosidaseDementia, seizures in type 3
Niemann-Pick Hepatosplenomegaly, psychomotor Sphingomyelin Sphingomyelinasedeterioration in types A and C Cholesterol (type C) (type A)
Globoid leukodystrophy Progressive encephalopathy, Galactocerebroside Galactocerebroside(Krabbe's) seizures, spasticity, blindness f,-Galactosidase
Metachromatic Progressive encephalopathy, Sulphatide Arylsulphatase Aleukodystrophy neuropathy, ataxia, spasticity
Fabry Pain, rare strokes, X linked, Ceramide trihexoside Ceramide trihexosiderenal insufficiency, skin lesions a-Galactosidase
Tay-Sachs Progressive encephalopathy GM2 ganglioside Hexosaminidase ATay-Sachs variant More rapid progression Globoside and GM2 Hexosaminidase A and B
GM, gangliosidosis Dementia, progressive ataxia, GM, ganglioside ,B-Galactosidasechoreoathetosis 16 point mutations
Swanson on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Diagnosis of inherited metabolic disorders affecting the nervous system
except for Hunter syndrome which is X linkedrecessive. Among these conditions are
Hurler's, Scheie's, Sanfilippo, Morquio's, andMaroteaux-Lamy diseases, and fl-glucuro-nidase deficiency. Clinical signs such as coarse
facial features, corneal clouding, hearing diffi-culties, hepatosplenomegaly, or joint abnor-malities are usually detected during the firstyear of life. Later, developmental delay or
mental regression may become apparent.
PEROXISOMAL DISORDERSThe peroxisome is an organelle that is foundin most tissues. It contains over 40 enzymes
including oxidases and catalase. Moser et allist 11 disorders attributable to defects inperoxisomal enzymes.222' These includedisorders of peroxisome biogenesis (Zellwegersyndrome, neonatal adrenoleukodystrophy,infantile Refsum's syndrome, and hyper-pipecolic acidaemia). The first two of thesedisorders can be associated with neonatalseizures, hypotonia, and developmental delay.Of the disorders associated with peroxiso-
mal enzyme abnormalities, X linked adreno-leukodystrophy is the most likely to be seen
by neurologists.Adrenoleukodystrophy and adrenomyelo-
neuropathy are X linked disorders and are
associated with raised blood concentrations ofvery long chain fatty acids (VLCFAs) due toimpaired peroxisomal fi oxidation. The
genetic defect seems to result from deletionsin the peroxisomal membrane protein gene.24
Some different phenotypes occur.22-26Neurologists are most likely to encounter an
adult patient with adrenomyeloneuropathy,with slowly progressive paraparesis as themain neurological manifestation and adreno-cortical failure as a common occurrence.
Adult onset cerebral adrenoleukodystrophy ismanifested by dementia, confusional states,and sometimes progressive ataxia or psychi-atric disturbances.27 Symptom progression isusually slower in patients with adult onset.
Assays for VLCFAs (C24:0, C26:0) are
carried out in specialised lipid laboratoriesusing gas liquid chromatography or mass
spectrometry. Although the vast majority ofpatients have raised plasma concentrations ofthese fatty acids, an occasional family will
Table 4 Disorders associated with unstable expanded trinucleotide repeats
Number of repeatsExtended
have VLCFA concentrations within the usual"normal" range.28 Molecular genetic analysisnow makes it possible to detect point muta-tions within the adrenoleukodystrophy gene.29
MITOCHONDRIAL ENCEPHALOPATHIESA high index of suspicion is aroused for thepresence of a disorder involving an abnormalmitochondrial gene if there are clinicalfeatures of Leigh's disease (subacute necro-
tising encephalomyelopathy), Kearns-Sayresyndrome (progressive external ophthalmo-plegia, retinal pigmentary degeneration, andother symptoms), MELAS (mitochondrialencephalomyelopathy with lactic acidosis andstroke-like episodes), MERRF (myoclonicepilepsy with ragged red flbres), Leber'shereditary optic neuroretinopathy, or NARP(neurogenic muscle weakness, ataxia, andretinitis pigmentosa).'>36 Various otherfeatures have been seen including shortstature, deafness, diabetes mellitus, pepticulceration, severe constipation, and migraine.
Mutations in mitochondrial DNA havebeen discovered in patients with several clini-cal presentations. Deletions of mitochondrialDNA are common in Kearns-Sayre syn-
drome.2 In MELAS, point mutations includean A -- G mutation at nt3243 in 80% of
cases, as well as T -+ C mutations at nt3271
and at nt9957, and an A -+ G mutation at
nt11084. An A-+G nt8344 mutation has
been found in MERRF, and a T -+ G or
T -+ C mutation at nt8993 in Leigh's
syndrome.3738Diagnostic laboratory tests include: (a)
serum pyruvate and lactate concentrations;(b) muscle biopsy to assess for the presence ofragged red fibres, and as a source of mito-chondria for DNA analysis; and (c) moleculargenetic studies on blood or muscle in a
specialised laboratory to assess for knownmutations.
DISORDERS ASSOCIATED WITH EXPANDED
TRINUCLEOTIDE REPEATS
One of the most exciting developments inneurology has been the discovery of neuro-
genetic diseases in which the abnormal gene
mutation results in expansion of a repeatedsequence of trinucleotides. Table 4 lists many
TranslationDisorder Chromosome trinucleotide Normal Disease of repeat
Fragile X syndrome X CGG 6-50 Premutation:52-200 No(FRXA) Disease: 200 to > 1000
Fragile X E (FRXE) X GCC 6-25 >200Myotonic dystrophy 19q CTG <30 Premutation: 42-180 No
Disease: 200->1000Bulbar spinomuscular Xql 1-12 CAG 17-26 40-52 Yes
atrophy(Kennedy's syndrome)
Huntington's disease 4p16.3 CAG 11-34 37-121 YesAutosomal dominant
spinocerebellar ataxiasSpinocerebellar ataxia 1 6p22-23 CAG 19-36 42-81 YesMachado-Joseph disease 14q32.1 CAG 13-36 68-79 YesDentatorubral- 12p 12-ter CAG 7-23 49-75 Yes
pallidoluysian atrophy(DRPLA)
463 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Swanson
of the presently known disorders of thistype.39-50 They are either X linked or auto-somal dominant disorders and include thedominant spinocerebellar ataxias SCAI andMachado-Joseph disease, Huntington'sdisease, fragile X syndrome, myotonic dystro-phy, and spinal bulbar muscular atrophy(Kennedy's syndrome). In many of thesedisorders, the length of the expanded trinu-cleotide repeat is unstable. Succeeding gener-ations have expansions of greater lengthwhich may be associated with earlier onsetand more severe disease manifestations. It islikely that additional neurodegenerative disor-ders will be added to this list.43
Genetics laboratories have the capability ofdefinitively diagnosing the presence orabsence of some of these disorders on a singlesample of blood, using molecular genetictechniques. Commercial availability is limitedat this time.
DISORDERS OF COPPER METABOLISMTwo diagnosable genetic disorders are associ-ated with defects in copper metabolism:Menkes' disease and Wilson's disease.
Menkes' "kinky hair" (steely hair) disease isan X linked disorder with manifestations inearly infancy.5' 52 Infants feed poorly, becomehypothermic, gain weight slowly, developseizures, and show progressive neurologicaldeterioration. They have colourless, friablehair which has a characteristic microscopicappearance. Danks et al suggested that thedisease was due to a disorder of coppermetabolism.53 The gene has been isolated andis a copper transporting ATPase. Untilrecently, diagnosis if suspected clinically wasestablished by demonstrating low cerulo-plasmin and serum copper concentrationsand abnormalities in fibroblast copperuptake.5455 In the newborn, however, copperand ceruloplasmin are normally low, so reli-able detection of abnormally low concentra-tions cannot be made until the third or fourthweek of life. The diagnosis can be made byDNA analysis.56
Wilson's disease is an autosomal recessivedisorder due to an abnormal gene at q14.3 onchromosome 13. This gene codes for acopper transporting P-type ATPase that ispresumably important for hepatic incorpora-tion of copper into ceruloplasmin and forexcretion of copper into bile.57-59 The enzymeis also expressed in the kidney. Twenty fivemutations have been identified in theWilson's disease gene, accounting for thegreat variability in clinical symptomatology.60The pathogenetic role of reduced synthesis orimpaired function of the copper transportingprotein ceruloplasmin is not clear.6' In thecourse of Wilson's disease, increased storageof copper occurs in liver, brain, cornea(Kayser-Fleischer ring in Descemet'smembrane), and kidneys. Neurological andpsychiatric symptoms can occur secondary todeposition of copper in the brain or as aresult of hepatic encephalopathy due tocopper induced liver damage. The diagnosiscan and should be made before the onset of
symptoms in close relatives of affectedpatients.62 64 The diagnosis can be made withthe assistance of the following laboratoryfindings.63 (a) increased excretion of copperinto the urine (normal <30 ptg/24 h; Wilson'sdisease 100-1000 gg/24 h); (b) decreasedserum concentration of total copper (normal85-145 gg/dl); (c) decreased serum concen-tration of ceruloplasmin (normal range 25-45mg/dl); about 5% of cases will have normalceruloplasmin concentrations.65
Symptomatic approach to the diagnosisof inherited metabolic disordersMENTAL RETARDATION OR DETERIORATIONFragile X syndromeOver 100 X linked mental retardationsyndromes are known at the present time.66Of these, fragile X syndrome is the leadinggenetic cause of mental retardation.67 Thesyndrome is so named because of the instabil-ity of the X chromosome when incubated infolic acid deficient media.68 69 This was thefirst neurological disorder to be associatedwith an unstable trinucleotide repeatsequence.70 Clinically, patients may haveprominent ears, large testicles, high archedpalates, and behavioural deficits. Definitivediagnosis can be made by the demonstrationof an expanded trinucleotide CGG repeatsequence. Abnormality in the FMR gene resultsin lack of production of the FMR1 protein.
Diagnosis of mental deterioration orprogressive encephalopathy in infants mayrequire various metabolic tests if thesuspected diagnosis is not already obvious.72A metabolic screen of the urine carried out bya hospital laboratory usually includes a nitro-prusside-cyanide test, a ferric chloride test,tests for ketoacids and mucopolysaccharides,and two dimensional amino acid chromatog-raphy. Serum analyses for amino acids andorganic acids will usually be diagnostic foraminoacidurias and organic acidaemias.Studies to search for other disordersmentioned (Menkes' disease, lipid storagediseases) will require special testing by genet-ics laboratories.
JUVENILE OR ADULT PATIENTS PRESENTINGWITH DEMENTIALaboratory investigations are of limitedusefulness in dementia diagnosis. The mostcommon dementing illnesses such asAlzheimer's disease are not yet diagnosablebiochemically on a routine basis. In a fewfamilies with familial Alzheimer's disease,point mutations have been found in the geneon chromosome 21 that codes for theamyloid precursor protein (APP) gene.7374Most families, however, do not have thesemutations. In young onset families, linkageanalysis has located the gene defect to a locuson chromosome 14. Ultimately it may bepossible to diagnose the disorder by molecu-lar genetic techniques. At present, diagnosisof the rare APP mutation can be carried outonly by specialised research laboratoriesstudying this disorder.
464 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Diagnosis of inherited metabolic disorders affecting the nervous system
In some patients with progressive cognitiveimpairment, a high degree of suspicion basedon clinical or radiological clues may justifycarrying out further metabolic studies toconfirm a suspected diagnosis (table 5).Vitamin B- 12 deficiency rarely producesdementia alone but should be excluded.
Huntington's diseaseThe diagnosis of Huntington's disease cannow be confirmed by commercially availableDNA testing. The presence of an extendedCAG repeat in the Huntington's disease geneon chromosome 4 establishes the diagnosis. Anormal allele has less than 35 CAG repeats.The Huntington's disease gene has more than38 repeats in 98-99% of cases.76
LeukodystrophiesIn addition to multiple sclerosis and progres-sive multifocal leukoencephalopathy, cerebralwhite matter can be affected by several meta-bolic disorders, with dementia as a majorsymptom. These include adult onsetmetachromatic leukodystrophy (MLD),adrenoleukodystrophy, Pelizaeus-Merzbacherdisease, Krabbe's disease, and cerebrotendi-nous xanthomatosis (CTX). In each disorder,symptoms are progressive, usually overmonths to years. Inherited in an autosomalrecessive manner, MLD would likely be asso-ciated with clinical or EMG/nerve conductionvelocity evidence of a peripheral neuropathy.Adrenoleukodystrophy might be associatedwith adrenal insufficiency and, as it is an Xlinked disorder, would occur predominantlyin males. Patients with cerebrotendinousxanthomatosis usually develop prominentxanthomas in large tendons such as theAchilles tendon.
Adrenoleukodystrophy-This disorder ischaracterised by varying modes of onset atdifferent ages. Most affected people are male,
Table S Disorders associated with dementia
Disorder Diagnostic test
Alzheimer's disease In known families,genetics laboratory forDNA point mutationin the APP gene
B-12 deficiency Serum B-12 levelSchilling test
Huntington's disease Genetics laboratoryfor DNA screen(CAG > 37 repeats)
Adrenoleukodystrophy Lipid laboratory forplasma VLCFA
Pelizaeus-Merzbacher disease Genetics laboratoryfor PLP gene
Canavan's disease Urine forN-acetylaspartic acidFibroblasts foraspartoacyclase
Metachromatic leukodystrophy Arylsulphatase AGM, gangliosidosis fl-galactosidaseGloboid leukodystrophy (Krabbe's) GalactocerebrosidaseCerebrotendinous xanthomatosis Lipid laboratory for
cholestanolCeroid-lipofuscinosis EM of buffy coat for
curvilinear bodies
VLCFA = very long chain fatty acids; PLP = proteolipidprotein; APP = amyloid precursor protein; EM = electronmicroscopy.
as the disorder is X linked. Some heterozy-gous women may, however, develop spastic
22paraparesis.2 The phenotypes delineated byMoser et al are: childhood cerebral (48%),adolescent cerebral (5%), adult cerebral(3%), adrenomyeloneuropathy (25%), addis-onian only (10%), asymptomatic (8%).26The disorder is suspected in children withlearning disorders and dementia. Adreno-myeloneuropathy usually begins with progres-sive paraparesis.
Pelizaeus-Merzbacher disease-This disorderis X linked. Symptoms usually begin ininfancy or childhood, but onset in early adult-hood has been reported.77 Symptoms includepsychomotor delay and later, dementia,nystagmus, ataxia, spasticity, and involuntarymovements. Mutations in the gene coding forproteolipid protein result in defective myelin.Mutations in the proteolipid protein gene cannow be determined in genetics laborato-ries.7879 Prenatal diagnosis is also possible.80Canavan 's disease-Another rare leuko-
dystrophy is Canavan's disease, characterisedby infantile and juvenile forms with severeprogressive neurological deterioration. Raisedurinary N-acetylaspartic acid and deficiencyof the enzyme aspartoacyclase in skin fibro-blasts confirm the diagnosis.
Lipid storage diseasesMetachromatic leukodystrophy (MLD) andKrabbe's disease (globoid leukodystrophy), aswell as other lipid storage diseases such asGM, gangliosidosis and type 3 Gaucher'sdisease can produce dementia as part of moregeneralised neurological deterioration.Urinary sulphatides will be abnormallyincreased in MLD. In the other conditions,confirmation of clinical suspicion will requirewhite blood cell or fibroblast enzyme deter-minations carried out by a specialised labora-tory.
Neuronal ceroid lipofuscinosis (Batten'sdisease and variants)-This is a disorder asso-ciated with storage of a complex lipopigment.The disease has not yet been characterisedenzymatically, although linkage analysis haslocated the gene for the infantile form(CLN1) to chromosome lp32, and that forthe juvenile form (CLN3) to chromosome16p 12.8283 Patients usually develop retinaldegeneration, myoclonus, seizures, anddementia. Diagnosis is made by demonstrat-ing accumulated storage product in buffy coator in skin biopsies, which show curvilinearbodies or a "fingerprint" pattern on electronmicroscopy. The early onset forms are auto-somal recessive. Both autosomal dominantand autosomal recessive inheritance has beenreported in the adult form (Kufs' disease)which is not associated with pigmentaryretinal degeneration.84 85
ATAXIASProgressive ataxia can result from severalconditions that have metabolic causes. TheMRI will have assisted in diagnosing multiplesclerosis, cerebellar neoplasms, and the diag-noses of alcoholic cerebellar degeneration and
465 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Swanson
paraneoplastic syndromes will have beenconsidered.
Genetic causes are of special importance inthis group of disorders. As yet the diagnosisof Friedreich's ataxia is based on clinical, notbiochemical findings. The genetics laboratorycan, however, assist in diagnosing several ofthese disorders, including spinocerebellarataxia type I (SCA-1) and Machado-Joseph'sdisease.44 86
Ataxia-telangiectasia, an autosomal reces-sive disorder, is the most common cause ofataxia in children under the age of 10.72Usually the diagnosis is evident clinically,with ataxia, nystagmus, choreoathetosis, andcharacteristic auricular and conjunctivaltelangiectases being evident. The abnormalgene on chromosome llq22-23, which isimportant for DNA repair, has recently beenidentified.87 The gene product is likely to be aphosphatidylinositol-3' kinase. Presumablymore definitive DNA diagnostic testing willbecome available. Symptoms of ataxia-telang-iectasia can begin in early adult life.88 Someserum abnormalities are found in patientswith this disorder, including raised a-fetopro-tein in 95% of cases, alterations in serumimmunoglobulins, and raised carcinoembry-onic antigen concentrations.89Autosomal dominant cerebellar ataxias are
being reclassified as their genetic defectsare discovered. Abnormal genes have beenfound on chromosomes 6, 11, 12, 14, and16.4246 8690-92 Dubourg et al sampled DNAfrom 88 families with inherited ataxias andfrom 16 patients with sporadic ataxia todetermine the frequency of the SCAl muta-tion on chromosome 6.4 Twelve of the fami-lies and none of the sporadic cases carried theSCAl mutation (unstable expanded CAGrepeat).
Clinical characteristics do not readilydistinguish the subtypes of cerebellar atax-ias.93 Many patients will have additional signssuch as extensor plantar responses, decreasedvibration sense, ophthalmoplegias, andincreased or decreased tendon reflexes. InSCAl, instability of the mutation is morecommon with male transmission and the ageof onset of symptoms is lower in patients witha higher number of CAG repeats (anticipa-tion).
Dentatorubral-pallidoluysian atrophy (DRPLA)is a rare autosomal dominant neurodegenera-tive disorder, usually classified under theataxias. The disorder can be associated withmyoclonus, chorea, dementia, and seizures.Juvenile and adult onsets are reported.94The disorder may be misdiagnosed asHuntington's disease.48 The molecular defectis an expanded CAG repeat on the genelocated on chromosome 12p and can be diag-nosed by molecular analysis.4950
Another disorder that may present withataxia is Cerebrotendinous xanthomatosis. Thiscondition is suspected in a patient who hastendon xanthomas, often in the Achillestendons.95 The diagnosis is confirmed byshowing raised concentrations of cholestanol(dihydrocholesterol) in blood or tissue.96 This
test will involve contacting a specialised lipidlaboratory, but it is important to do, as thedisease can be treated by giving chenode-oxycholic acid.97 Several mutations of thegene on chromosome 2 that codes for theenzyme sterol 27-hydroxylase have beenfound in families with this disorder.98 100
Presymptomatic cases and heterozygotes cannow be detected by molecular diagnostictechniques. 101
Ataxia with isolated vitamin E deficiency(AVED)-Patients have been described withprogressive ataxia and other features ofFriedreich's disease, in which vitamin Econcentrations were reduced in the absenceof malabsorption.'02 In the patient describedby Stumpf et al, serum vitamin E concentra-tions were below 1 0 (normal 5-20) psg/mland could be restored to normal with an oraldose of 800 mg/day of DL-a-tocopherol.'03This disorder is autosomal recessive. Thegene maps to chromosome 8q13.'°4105Affected patients have mutations in the a-tocopherol transfer protein resulting inimpaired ability to incorporate a-tocopherolinto lipoproteins.'06
A-/B-lipoproteinaemia-Patients with thisdisorder usually develop steatorrhea ininfancy followed in the second decade byprogressive ataxia and peripheralneuropathy.72 The patients have absence ofserum fl-lipoproteins and very low con-centrations of a-tocopherol. Dietary supple-mentation with high doses of vitamin E(100 mg/kg/day) may arrest the neurologicalmanifestations.'07 This condition is associatedwith defective genes coding for the largersubunit of the microsomal triglyceride trans-fer protein (MTP), resulting in abnormalVLDL secretion and impairing delivery ofvitamin E and other fat soluble substrates.'08The autosomal recessive disorder
Friedreich's ataxia is associated with an as yetunidentified genetic defect on chromosome 9.Because of clinical similarities to AVED, ithas been suggested that the Friedreich'sataxia gene may also be involved in a-toco-pherol metabolism.'09
Ataxia associated with mitochondrialdisorders-Ataxia can be a feature of several ofthe mitochondrial disorders, especially theMERRF and MELAS syndromes, and therare syndrome termed NARP.34 The presenceof retinitis pigmentosa should raise the indexof suspicion for NARP, which is sometimesdue to a point mutation at bp8993 resultingin substitution of arginine for leucine insubsequence 6 of the mitochondrialH+ATPase. Patients with this disorder mayhave seizures, muscle weakness, mental retar-dation and long tract signs with symptomsbeginning from infancy to late adulthood.
MOTOR NEURON DISEASEMost patients with suspected amyotrophiclateral sclerosis (ALS) have no knownbiochemical defect. Kennedy's syndrome(spinal bulbar muscular atrophy) may clini-cally resemble the bulbar form of ALS,though progression is usually slow. A genetics
466 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Diagnosis of inherited metabolic disorders affecting the nervous system
laboratory can confirm this diagnosis bydetermining the presence of an expandedCAG repeat on the X chromosome (table 4).About 20% of cases of familial ALS have
been discovered to have one of several muta-tions of the gene on chromosome 21 thatcodes for the Cu/Zn binding superoxidedysmutase enzyme (SOD). 101'12
In patients with mutations in this gene, theconcentration and specific activity of Cu/ZnSOD are reduced in erythrocytes by about50%"13; however, these changes do not corre-late with disease severity. Detection of theCu/Zn SOD mutation requires DNA analysisof a blood sample by a genetics laboratorystudying this disorder.
MOVEMENT DISORDERS (TABLE 6)Wilson's diseasePatients with Wilson's disease can developsymptoms of hepatic or neurological dysfunc-tion. Symptoms that may bring a patient to aneurologist include involuntary movements(tremor, dystonia, chorea, spasms), andbehavioural and personality changes.Psychiatric symptoms account for a highproportion of presenting complaints.64 AKayser-Fleischer ring may be seen on exami-nation of the cornea.
Wilson's disease is commonly but notinvariably associated with reduction in serumceruloplasmin concentrations (normal range25-45 mg/dl). Total serum copper concentra-tions may not be raised. "Free" serum coppercan be calculated by subtracting from thetotal copper (gg/dl), that amount bound toceruloplasmin (multiply by 3 the cerulo-plasmin concentration (in mg/dl) to obtainthe bound copper in ,ug/dl). The free copperconcentration should be <10-15 jg/dl.Laboratory standards are variable, however,so it is recommended that a 24 hour urinarycopper be obtained. In Wilson's diseasecopper excretion is >100 gg/24 h (normal<30 gg/24 h).
In an asymptomatic patient at risk forWilson's disease, liver biopsy may be neces-sary to detect increased copper content in theliver (patients with Wilson's disease have>200 gsg/g wet weight).
Table 6 Metabolic disorders associated with involuntary movements
Disease Type of movement Associatedfeatures Diagnostic test
Huntington's disease Chorea Dementia Molecular analysis forDystonia (juvenile) CAG repeat expansion
Wilson's disease Tremor, dystonia Hepatic insufficiency Ceruloplasmin, serumchorea Kayser-Fleischer ring and urine copper
Dentatorubral Chorea Ataxia, myoclonus, Molecular analysis forpallidoluysian atrophy dementia CAG repeat expansion(DRPLA)
GM, gangliosidosis Dystonia, Gait disturbance Leucocyte lysosomalChoreoathetosis acid fi-galactosidase
activityDopa responsive Dystonia Levodopa Research laboratory
dystonia responsiveness for GTP cyclohydrolasemutation
Ataxia-telangiectasia Choreoathetosis Ataxia, auricular, Decreased a-fetoprotein,and conjunctival immunoglobulintelangiectases abnormalities
Other metabolic causes of dystoniaAdult onset of dystonia can occur in GM,gangliosidosis."2 The disorder is autosomalrecessive and is diagnosed by showingpronounced reduction of activity of theenzyme f)-galactosidase which can bemeasured in leucocytes. Progressive doparesponsive dystonia has been recently reportedto be associated with mutations in a gene onchromosome 14q22.1-22.2 which codes forthe enzyme GTP cyclohydrolase 1.114
Other movement disordersChoreic movements are characteristic ofHuntington's disease, which is discussed inthe section on dementia. Another disorder inwhich chorea can occur is ataxia-telangiecta-sia, discussed in the section on ataxias.
STROKEMetabolic causes of stroke are rare, but mustbe considered in children and young adultspresenting with an acute ischaemic event.Disorders to consider include MELASsyndrome, homocystinuria, sulphite oxidasedeficiency, and Fabry's disease. MELASsyndrome can be associated with stroke-likeepisodes in young adults."5 Diagnosis may bedifficult (see section on mitochondrial disor-ders) and requires strong suspicion andcommunication with a genetics laboratoryspecialising in mitochondrial disorders.
Homocystinuria is much more commonthan sulphite oxidase deficiency. Both disordersmay be suspected by the presence of ectopialentis. Chronic homocysteine infusions inbaboons produce sustained endothelial cellloss and result in accelerated atherosclero-sis.116 It has been suggested that moderatehomocysteinaemia in otherwise normalsubjects may be a risk factor for athero-sclerotic stroke."17 The disorder is due to aninborn error of cystathionine synthase.Urinary amino acid screen will detect raisedconcentrations of homocystine. Sulphiteoxidase deficiency can be associated withstroke-like episodes in infancy and child-hood."8 Amino acid screening of the urinemust be done carefully and on fresh urine,and should show the presence ofS-sulphocysteine.ll9 S-sulphocysteine andsulphite are also detectable in plasma.'20 Basalganglia infarction in children, and adult onsetchorea and dementia have been reported inpropionic acidaemia."'2 122
Fabry's diseaseThis X linked lysosomal storage disease isassociated with accumulation of trihexoseceramide due to deficiency in the enzymeceramide trihexoside a-galactosidase (table3). At an early age, patients develop pinpointskin lesions, especially on the abdomen.Trihexose ceramide accumulates in bloodvessel walls, in kidney, and in myocardium.Death is usually due to renal or heart failure.Patients have been reported to developepisodic stroke-like symptoms and headaches.Small infarcts have been found in cerebralhemispheres, associated with proliferative
467 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Swanson
changes in vessel intima and media, presum-ably due to glycolipid deposition.123
SummaryKnowledge of the molecular causes forgenetic diseases that affect the nervous systemis rapidly expanding. Especially striking hasbeen the finding in several autosomal domi-nant neurodegenerative disorders that unsta-ble expansions of trinucleotide repeats areresponsible for the genetic disorder and thatthe length of the repeat can be correlated withthe age of onset and the severity of symp-toms. Phenotypic heterogeneity in manydisorders associated with enzyme deficienciescan often be linked to the amount of residualenzyme activity occurring with different genemutations.
Making a specific diagnosis of a neurologi-cal disorder associated with genetically deter-mined metabolic defects requires access to alaboratory that can assist in arranging forappropriate testing to be carried out. In somedisorders such as the aminoacidurias diagnos-tic metabolic studies can be performed inhospital clinical chemistry laboratories. Inothers, such as the lysosomal storage diseases,a laboratory that carries out special lipidanalyses and white blood cell enzyme assayswill be necessary. DNA mutational analysesare becoming commercially available for diag-nosing many disorders such as mitochondrialdiseases and those conditions associated withexpanded trinucleotide repeats. It may benecessary to contact individual research labo-ratories when confronted with a disorder thathas been newly discovered or that is very rare.A computerised directory of specialised labo-ratories that perform disease specific testingfor genetic disorders should be useful inchoosing the appropriate diagnostic orresearch laboratory.
1 Beaudet AL, Scriver CR, Sly WS, et al. Genetics andbiochemistry of variant human phenotypes. In: ScriverCR, Beaudet AL, Sly WS, Valle D, eds. The metabolicbasis of inherited disease. 6th ed. New York: McGraw-Hill, 1989:3-53.
2 Harding AE. The DNA laboratory and neurologicalpractice. J Neurol Neurosurg Psychiatry 1993;56:229-33.
3 Bird TD, Farrell DF. Genetics and neurology. In:Swanson PD, ed. Signs and symptoms in neurology,Philadelphia: JB Lippincott, 1984:345-77.
4 Dubourg 0, Durr A, Cancel G, et al. Analysis of theSCAl CAG repeat in a large number of families withdominant ataxia: clinical and molecular correlations.Ann Neurol 1995;37:176-80.
5 Nyhan WL, Haas R. Inborn errors of amino acid meta-bolism and transport. In: Rosenberg RN, Prusiner SB,DiMauro S, et al, eds. The molecular and genetic basis ofneurological disease, Boston; Butterworth-Heinemann,1993:145-65.
6 Cox RP, Chuang DT. Maple syrup urine disease: clinicaland molecular genetic considerations. In: RosenbergRN, Prusiner SB, DiMauro S et al, eds. The molecularand genetic basis of neurological disease. Boston:Butterworth-Heinemann, 1993:189-207.
7 de Duve C, Pressman BC, Gianetto R, et al. Tissue frac-tionation studies. 6. Intracellular distribution patternsof enzymes in rat-liver tissue. Biochem J 1955;60:604-17.
8 Hers HG. Inborn lysosomal diseases. Gastroenterology1965;48:625-33.
9 Brady RO. Biochemical genetics in neurology. ArchNeurol 1976;33:145-51.
10 Kolodny EH. Current concepts in genetics. Lysosomalstorage diseases. New EnglJ Med 1976;294: 1217-20.
11 Suzuki K. Enzymatic diagnosis of sphingolipidoses.Methods in enzymology 1987;138:727-62.
12 Yoshida K, Ikeda S, Kawaguchi K, Yanagisawa N. Adult
GM, gangliosidosis: immunohistochemical and ultra-structural findings in an autopsy case. Neurology 1994;44:2376-82.
13 Kolodny EH. Metachromatic leukodystrophy and multi-ple sulfatase deficiency: sulfatide lipidosis. In:Rosenberg RN, Prusiner SB, DiMauro S et al, eds. Themolecular and genetic basis of neurological disease. Boston:Butterworth-Heinemann, 1993:497-503.
14 Kolodny EH. The GM2 Gangliosidoses. In: RosenbergRN, Prusiner SB, DiMauro S et al, eds. The molecularand genetic basis of neurological disease. Boston:Butterworth-Heinemann, 1993:531-40.
15 Navon R, Argov Z, Frisch A. Hexosaminidase A defi-ciency in adults. AmJ Hum Genet 1986;24:179-96.
16 Yoshida IC, Oshima A, Sakuraba H, et al. GM,gangliosidosis in adults: clinical and molecular analysisof 16 Japanese patients. Ann Neurol 1992;31:328-32.
17 Nishimoto J, Nanba E, Inui K, et al. GMl-gangliosidosis(genetic ,B-galactosidase deficiency): identification offour mutations in different clinical phenotypes amongJapanese patients. Am J Hum Genet 1991 ;49:566-72.
18 Leinekugal P, Michel S, Conzelmann E, Sandhoff C.Quantitative correlation between the residual activityof ,B-hexosaminidase A and arylsulfatase A and theseverity of the resulting lysosomal storage disease. HumGenet 1992;88:513-23.
19 Goldman JE, Katz D, Rapin I, et al. Chronic G.\,-gangliosidosis presenting as dystonia: I. clinical andpathological features. Ann Neurol 1981;9:465-75.
20 Neufeld EF, Lim TW, Shapiro LJ. Inherited disorders oflysosomal metabolism. Ann Rev Biochem 1975;44:357-76.
21 Matalon R, Kaul R, Michals K. The mucopolysacchari-doses and the mucolipidoses. In: Rosenberg RN,Prusiner SB, DiMauro S et al, eds. The molecular andgenetic basis of neurological disease, Boston: Butterworth-Heinemann, 1993:401-9.
22 Moser HW, Moser AE, Singh I, O'Neill BP.Adrenoleukodystrophy: survey of 303 cases: biochem-istry, diagnosis and therapy. Ann Neurol 1984;16:628-41.
23 Moser HW. Peroxisomal disorders. In: Rosenberg RN,Prusiner SB, DiMauro S, et al, eds. The molecularand genetic basis of neurological disease. Boston:Butterworth-Heinemann, 1993:351-87.
24 Mosser J, Douar AM, Sarde CO, et al. Putative X-linkedadrenoleukodystrophy gene shows unexpected homol-ogy with ABC transporter. Nature 1993;361:726-30.
25 van Geel BM, Assies J, Weverling GJ, Barth PG.Predominance of the adrenomyeloneuropathy pheno-type of X-linked adrenoleukodystrophy in theNetherlands: A survey of 30 kindreds. Neurology 1994;44:2343-6.
26 Moser HW, Moser AB, Smith KD, et al. Adreno-leukodystrophy: phenotypic variability and implica-tions for therapy. J Inherit Metab Dis 1992;15:645-64.
27 Farrell DF, Hamilton SR, Knauss TA, et al. X-linkedadrenoleukodystrophy: adult cerebral variant.Neurology 1993;43:1518-22.
28 Kennedy CR, Allen JT, Fensom AH, Steinberg SJ,Wilson R. X-linked adrenoleukodystrophy with non-
diagnostic plasma very long chain fatty acids. J NeurolNeurosurg Psychiatry 1994;57:759-61.
29 Vorgerd M, Fuchs S, Tegenthoff M, Malin J-P. Amissense point mutation (Ser515Phe) in theadrenoleukodystrophy gene in a family with adreno-myeloneuropathy: a clinical, biochemical, and geneticstudy. J7 Neurol Neurosurg Psychiatry 1995;58:229-3 1.
30 Crimmins D, Morris JGL, Walker GL, et al. Mitochon-drial encephalomyopathy: variable clinical expressionwithin a single kindred. _7 Neurol Neurosurg Psychiatry1993;56:900-5.
31 DeVivo DC. The expanding clinical spectrum of mito-chondrial diseases. Brain Dev 1993;15:1-22.
32 Fryer A, Appleton R, Sweeney MG, et al. MitochondrialDNA 8993 (NARP) mutation presenting within a
heterogeneous phenotype including "cerebral palsy".Arch Dis Child 1994;71:419-22.
33 Lestienne P, Bataille N. Mitochondrial DNA alterationsand genetic diseases: a review. Biomed Pharmacother1994;48:199-214.
34 Holt IJ, Harding AE, Petty RKH, Morgan-Hughes JA. Anew mitochondrial disease associated with mitochon-drial DNA heteroplasmy. Am .7 Hum Genet 1990;46:428-33.
35 Lodi R, Montagna P, Iotti S, et al. Brain and muscleenergy metabolism studied in vivo by 31P magneticresonance imaging in NARP syndrome. _7 NeurolNeurosurg Psychiatry 1994;57: 1492-6.
36 Zeviani M, Taroni F. Mitochondrial diseases. Bailliere'sclinical neurology 1994;3:315-34.
37 Santorelli FM, Shanske S, Jain K, et al. A T -. C muta-tion at nt8993 of mitochondrial DNA in a child withLeigh syndrome. Neurology 1994;44:972-4.
38 Tatuch Y, Christodonlon J, Feigenbaum A, et al.Heteroplasmic mtDNA mutation (T -+ G) at 8993 cancause Leigh disease when the percentage of abnormalmtDNA is high. AmJHum Genet 1992;50:852-8.
39 La Spada AR, Paulson HL, Fishbeck KH. Trinucleotiderepeat expansion in neurological diseases. Ann Neurol1 994;36:8 14-22.
40 La Spada, Wilson EM, Lubahn DB, Harding AE,Fischbeck KH. Androgen receptor gene mutations inX-linked spinal and bulbar muscular atrophy. Nature199 1;352:77-9.
468 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

Diagnosis of inherited metabolic disorders affecting the nervous system
41 Plassart E, Fontaine B. Genes with triplet repeats: a newclass of mutations causing neurological diseases.Biomed Pharmacother 1994;48: 191-7.
42 Stevanin G, Le Guem E, Ravise N, et al. A third locusfor autosomal cerebellar ataxia (ADCA) type 1 mapsto chromosome 14q26.3qter: evidence for the exis-tence of a fourth locus. Am J Hum Genet 1994;521:11-20.
43 Willems PJ. Dynamic mutations hit double figures.Nature Genetics 1994;8:213-5.
44 Kawaguchi Y, Okamoto T, Taniwaki M, et al. CAGexpansions in a novel gene for Machado-Joseph diseaseat chromosome 14q32. 1. Nature Genetics 1994;8:221-7.
45 Ranum LPW, Chung M, Banfi S, et al. Molecular andclinical correlations in spinocerebellar ataxia 1 (SCA1):evidence for familial effects on the age of onset. Am JfHum Genet 1994;55:244-52.
46 Giunti P, Sweeney MG, Spadaro M, et al. The trinu-cleotide repeat expansion on chromosome 6p (SCA 1)in autosomal dominant cerebellar ataxias. Brain 1994;227:645-9.
47 Duryao M, Ambrose C, Myers R et al. Trinucleotiderepeat length instability and age of onset inHuntington's disease. Nature Genetics 1993;4:387-92.
48 Potter NT, Meyer MA, Zimmerman AW. Molecularand clinical findings in a family with denta-torubral-pallidoluysian atrophy. Ann Neurol 1995:37:273-7.
49 Nagafuchi S, Yanagisawa H, Sato K, et al. Dentatorubraland pallidoluysian atrophy expansion of an unstableCAG trinucleotide on chromosome 12p. NatureGenetics 1994;6: 14-8.
50 Nagafuchi S, Yanagisawa H, Ohsaki E, et al. Structureand expression of the gene responsible for the tripletrepeat disorder, dentatorubral and pallidoluysian atro-phy (DRPLA). Nature Genetics 1994;8:177-82.
51 Menkes JH, Alter M, Steigleder GK et al. A sex-linkedrecessive disorder with growth retardation, peculiarhair, and focal cerebral and cerebellar degeneration.Pediatrics 1962;29;764-79.
52 Menkes JH. Kinky hair disease: twenty-five years later.Brain Dev 1988;lO:77-9.
53 Danks DM, Campbell PE, Stevens BJ et al. Menkes'kinky hair syndrome: an inherited defect in copperabsorption with widespread effects. Pediatrics 1972;50:188-201.
54 Gunn TR, Macfarlane S, Phillips LI. Difficulties in theneonatal diagnosis of Menkes' kinky hair syndrome-trichopoliodystrophy. Clinical Pediatr 1984;23:514-6.
55 Tonnesen T, Horn N. Prenatal and postnatal diagnosisof Menkes disease, an inherited disorder of coppermetabolism. J7 Inherit Metab Dis 1989;12 (suppll):207-14.
56 Tumer Z, Tonnesen T, Bohmann J, et al. First trimesterprenatal diagnosis of Menkes disease by DNA analysis.JfMed Genet 1994;31:615-7.
57 Bull PC, Cox DW. Wilson disease and Menkes disease:new handles on heavy-metal transport. Trends Genet1994;10:246-52.
58 Tanzi RE, Petrukhin K, Chernov I et al. The Wilsondisease gene is a copper transporting ATPase withhomology to the Menkes disease gene. Nature Genetics1993;5:344-50.
59 Yamaguchi Y, Heiny ME, Gitlin JD. Isolation andcharacterization of a human liver cDNA as a candidategene for Wilson disease. Biochem Biophys Res Commun1993;197:271-7.
60 Thomas GR, Forbes JR, Roberts EA. The Wilsondisease gene: spectrum of mutations and their conse-quences. Nature Genetics 1995;9:210-7.
61 Czaja MJ, Weiner FR, Schwarzenberg FJ, et al.Molecular studies of ceruloplasmin deficiency inWilson's disease. J Clin Invest 1987;80: 1200-4.
62 Walshe JM. Diagnosis and treatment of presymptomaticWilson's disease. Lancet 1988;ii:435-7.
63 Walshe JM. Wilson's disease: yesterday, today, andtomorrow. Mov Dis 1988;3:10-29.
64 Walshe JM, Yealland M. Wilson's disease: the problemof delayed diagnosis. Jf Neurol Neurosurg Psychiatry1992;55:692-6.
65 Gibbs K, Walshe JM. A study of the coeruloplasminconcentrations found in 75 patients with Wilson'sdisease, their kinships and various control groups.QuartJ Med 1979;48:447-63.
66 Neri G, Chiurazzi P, Arena JF, Lubs HA. XLMR genes:update 1994.AmJ Med Genet 1994;51:542-9.
67 Jacobs PA, Glover TW, Mayer M, et al. X-linked mentalretardation: a study of 7 families. Am J Med Genet1980;7:471-89.
68 Turner G, Brookwell R, Daniel A, et al. Heterozygousexpression of X-linked mental retardation and X-chromosome marker fra(X) (q27). N EnglJ Med 1980;303:662-4.
69 Nielson KB. Diagnosis of the fragile X syndrome:clinical findings in 27 males with the fragile site atXq28. J'ournal of Mental Deficiency Research 1983:27:211-26.
70 Verkerk AJMH, Pieretti M, Sutcliffe JS, et al.Identification of a gene (FMR-1) containing CGGrepeat coincident with a breakpoint cluster regionexhibiting length variation in fragile X syndrome. Cell1991;65:905-14.
71 Fu Y-H, Kuhl DPA, Pizzuti A. Variation of the CGGrepeat at the fragile X site results in genetic instability:
resolution of the Sherman paradox. Cell 1992;67:1047-58.
72 Menkes JH. Textbook of child neurology, 5th ed.Baltimore: Williams and Wilkins, 1995.
73 Goate A, Chartier Harlin MC, Mullan M, et al.Segregation of missense mutations in amyloid precur-sor protein gene with familial Alzheimer's disease.Nature 1991;349:704-6.
74 Hardy J. Alzheimer's disease. Molecular genetics. J FlaMedAssoc 1994;91:759-61.
75 Schellenberg GD, Bird T, Wijsman E et al. Genetic link-age evidence for a familial Alzheimer's disease locus onchromosome 14. Science 1992;258:668-71.
76 Kremer B, Goldberg P, Andrew SE et al. A worldwidestudy of the Huntington's disease mutation. The sensi-tivity and specificity of measuring CAG repeats. N EnglJfMed 1994;330:1401-6.
77 Saito Y, Ando T, Doyu M, et al. An adult case of classi-cal Pelizaeus-Merzbacher disease-magnetic resonanceimages and neuropathological findings. RinshoShinkeigaku. Clinical Neurology 1993;33: 187-93.
78 Pham-Dinh D, Boespflug-Tanguy 0, Mimault C, et al.Pelizaeus-Merzbacher disease: a frameshift deletion/insertion event in the myelin proteolipid gene. HumanMolecular Genetics 1993;2:465-7.
79 Boespflug-Tanguy 0, Mimault C, Melki J, et al. Genetichomogeneity of Pelizaeus-Merzbacher disease: tightlinkage to the proteolipoprotein locus in 16 affectedfamilies. Am J Hum Genet 1994;55:461-7.
80 Strautnieks S, Rutland P, Winter RM, et al. Pelizaeus-Merzbacher disease: detection of mutations THR"'8 -
Pro and Leu223 -. Pro in the proteolipid protein gene,and prenatal diagnosis. Am J Hum Genet 1992;51:871-8.
81 Matalon R, Michals K, Sebasta D, et al. Aspartoacyclasedeficiency and N-acetylaspartic aciduria in patientswith Canavan disease. Am J Med Genet 1988;29:463-71.
82 Gardiner RM. Genetic analysis of Batten disease. _JInherit Metab Dis 1993;16:787-90.
83 Mitchison HM, Taschner PE, O'Rawe AM et al. Geneticmapping of the Batten disease locus (CLN3) to theinterval D16S288-D16S383 by analysis of haplotypesand allelic association. Genomics 1994;22:465-8.
84 Ferrer I, Arbizu T, Pena J, Serra JP. A Golgi and ultra-structural study of a dominant form of Kufs' disease. JNeurol 1980;222:183-90.
85 Martin J-J. Adult type of neuronal ceroid-lipofuscinosis.Jl Inherit Metab Dis 1993;16:237-40.
86 Rosenberg RN. Autosomal dominant cerebellar pheno-types: the genotype has settled the issue. Neurology1995;45: 1-5.
87 Savitsky K, Bar-Shira A, Gilad S, et al. A single ataxiatelangiectasia gene with a product similar to PI-3kinase. Science 1995;268:1749-53.
88 Serizawa M, Sakamoto M, Hirabayashi K, et al.Histological and radiobiological study of adult caseswith ataxia telangiectasia. Rinsho Shinkeigaku. ClinNeurol 1994;34:38-42.
89 Boder E. Ataxia-telangiectasia. In: Gomez MR, ed.Neurocutaneous diseases. A practical approach, Boston:Butterworths, 1987:95-117.
90 Gardner K, Alderson K, Galster B, et al. Autosomaldominant spinocerebellar ataxia: clinical description ofa distinct hereditary ataxia and genetic localization tochromosome 16 (SCA4) in a Utah kindred. Neurology1994;921S.
91 Benomar A, Le Guern E, Dure A. Autosomal dominantcerebellar ataxia with retinal degeneration (ADCA typeII) is genetically different from ADCA type 1. AnnNeurol 1994;35:439-44.
92 Ranum LPW, Schut LJ, Lundgren JK, et al.Spinocerebellar ataxia type 5 in a family descendedfrom the grandparents of President Lincoln maps tochromosome 11. Nature Genetics 1994;8:280-4.
93 Harding AE. The clinical features and classification ofthe late onset autosomal dominant cerebellar ataxias.Brain 1982;105:1-28.
94 Smith JK, Gonda VE, Malamud N. Unusual form ofcerebellar ataxia. Combined dentato-rubral andpallido-luysian degeneration. Neurology 1958;8:205-9.
95 Schimschock JR, Alvord EC, Swanson PD. Cerebro-tendinous xanthomatosis: clinical and pathologicalstudies. Arch Neurol 1968;18:688-98.
96 Menkes JH, Schimschock JR, Swanson PD. Cerebro-tendinous xanthomatosis: the storage of cholestanolwithin the nervous system. Arch Neurol 1968;19:47-53.
97 Bferginer VM, Salen G, Shefer S. Long-term treatment ofcerebrotendinous xanthomatosis with chenodeoxy-cholic acid. New EnglJMed 1984;311:1649-52.
98 Leitersdorf E, Reshef A, Meiner V, et al. Frameshift andsplice-junction mutations in the sterol 27-hydroxylasegene cause cerebrotendinous xanthomatosis in Jews ofMoroccan origin. J Clin Invest 1993;91:2488-96.
99 Kim K-S, Kubota S, Kuriyama M, et al. Identificationof new mutations in sterol 27-hydroxylase genein Japanese patients with cerebrotendinousxanthomatosis (CTX). J7 Lipid Research 1994;35:1031-9.
100 Nakashima N, Sakai Y, Sakai H, etal. A point mutationin the bile acid biosynthetic enzyme sterol 27-hydroxy-lase in a family with cerebrotendinous xanthomatosis. J'Lipid Research 1994;35:663-8.
101 Meiner V, Meiner Z, Reshef A, et al. Cerebrotendinousxanthomatosis: molecular diagnosis enables presymp-
469 on 2 O
ctober 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.5.460 on 1 Novem
ber 1995. Dow
nloaded from

470 Swanson
tomatic detection of a treatable disease. Neurology1994;44:288-90.
102 Harding AE, Matthews S, Jones S, et al. Spinocerebellardegeneration associated with a selective defect of vita-min E absorption. NEnglJMed 1985;313:32-5.
103 Stumpf DA, Sokol R, Bettis D, et al. Friedreich'sdisease: V. Variant form with vitamin E deficiency andnormal fat absorption. Neurology 1987;37:68-74.
104 Ben Hamida M, Belal S, Sirugo G, et al. Friedreich'sataxia phenotype not linked to chromosome 9 andassociated with selective autosomal recessive vitamin Edeficiency in two inbred Tunisian families. Neurology1993;43:2179-83.
105 Ben Hamida C, Doerflinger N, Belal S, et al.Localization of Friedreich ataxia phenotype with selec-tive vitamin E deficiency to chromosome 8q byhomozygosity mapping. Nature Genetics 1993;5:195-200.
106 Ouahchi K, Arita M, Kayden H, et al. Ataxia withisolated vitamin E deficiency is caused by mutations inthe a-tocopherol transfer protein. Nature Genetics 1995;9:141-5.
107 Kayden HJ. The neurologic syndrome of vitamin E defi-ciency: a significant cause of ataxia. Neurology 1993;43:2167-9.
108 Sharp D, Blinderman L, Combs KA et al. Cloning andgene defects in microsomal triglyceride transfer proteinassociated with abetalipoproteinemia. Nature 1993;365:65-9.
109 DiDonato S. Can we avoid AVED? Nature Genetics1995;9: 106-7.
110 Rosen DR, Siddique T, Patterson D, et al. Mutations inCu/Zn superoxide dismutase gene are associated withfamilial amyotrophic lateral sclerosis. Nature 1993;362:59-62.
111 Deng H-X, Hentati A, Tainer JA. Amyotrophic lateralsclerosis and structural defects in Cu,Zn superoxidedismutase. Science 1993;261: 1047-51.
112 Aoki M, Ogasawara M, Matsubara Y, et al. Familialamyotrophic lateral sclerosis (ALS) in Japan associatedwith H46R mutation in Cu/Zn superoxide dismutase
gene: a possible new subtype of familial ALS.Neurological Sciences 1994;126:77-83.
113 Bowling AC, Barkowski EE, McKenna YD, et al.Superoxide dismutase concentration and activity infamilial amyotrophic lateral sclerosis. .7 Neurochem1995;64:2366-9.
114 Ichinose H, Ohye T, Takahashi E, et al. Hereditaryprogressive dystonia with marked diurnal fluctuationcaused by mutations in the GTP cyclohydrolase 1gene. Nature Genetics 1994;8:236-41.
115 Lertrit P, Noer AS, Jean-Francis MJB, et al. A newdisease related mutation for mitochondrial encephalo-myopathy, lactic acidosis and stroke-like episodessyndrome affecting the ND4 subunit of complex I. AmHum Genet 1992;52:457-68.
116 Harker LA, Ross R, Slichter SJ, Scott CR. Homocystine-induced arteriosclerosis. The role of endothelial cellinjury and platelet response in its genesis. Y Clin Invest1976;58:731-41.
117 Brattstrom LE, Hardebo JE, Hultberg BC. Moderatehomocysteinemia-a possible risk factor for arterioscle-rotic cerebrovascular disease. Stroke 1984;15:1012-6.118 Riela AR, Roach S. Etiology of stroke in children. T ChildNeurol 1993;8:201-20.
119 Mudd SH, Irreverre F, Laster L. Sulfite oxidase defi-ciency in man: demonstration of the enzymatic defect.Science 1967;156: 1599-602.
120 Shih VE, Abroms IF, Johnson JL, et al. Sulfite oxidasedeficiency. Biochemical and clinical investigations of ahereditary metabolic disorder in sulfur metabolism.New EnglJ Med 1977;297:1022-8.
121 Haas RH, Marsden DL, Capistrano-Estrada S,Hamilton R et al. Acute basal ganglia infarction inpropionic acidemia. _7 Child Neurol 1995;10: 18-22.
122 Sesthi KD, Ray R, Roesel RA. Adult-onset chorea anddementia with propionic acidemia. Neurology 1989;39:1343-5.
123 Christensen Lou HO, Reske-Nielson E. The centralnervous system in Fabry's disease. Arch Neurol 1971;25:351-9.
Rosa canina (dog rose)
The Roman naturalist Pliny attributed the name dog roseto a belief that the plant's root could cure the bite of amad dog. It is not clear if the dogs were rabid. The use ofthe dog rose in prescriptions dates back to Hippocratesbut precisely what for is unclear. As a medicinal plant itcame into full bloom in the second world war. WhenBritain was unable to import fresh citrus fruits thegovernment organised the gathering of dog rose fruits, orhips, which were known to be a rich rource of vitamin C.Processed into syrup the rose hips helped to preventscurvy and, today, the plant is valued as a rich source ofvitamin C.The dog rose is illustrated as part of a commemorative
set issued for the International Congress ofPharmacology held in Prague in 1971 (Stanley Gibbons1980, Scott 1773).
L F HAAS
w-@e3igw-m W '?t %j >-97 ' w -'= §'~~~ U Ai0 'V J...'g;@ .t ..0LX
w INv.
'V~~~~~~~~~~~~~~~~1.
-7&t-i1. .hSipod. ji fM>f i.
A'#4W'~~~~~~~~~~~~~~~~~~~~~~5~~~~~~a*~ ~ ~~f
NEUROLOGICAL STAMP
on 2 October 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.5.460 on 1 N
ovember 1995. D
ownloaded from




![Three Main Causes of Homocystinuria: of Metabolism ... · most frequent causes are classical homocystinuria [deficiency of cystathionine beta-synthase (CBS)], methylmalonic aciduria](https://static.fdocuments.us/doc/165x107/5e951dcb19bd325819567b57/three-main-causes-of-homocystinuria-of-metabolism-most-frequent-causes-are.jpg)