Diagnosis of bacterial meningitis
21
ARE LUMBAR PUNCTURES THE BEST WAY TO DIAGNOSE BACTERIAL MENINGITIS? Group 13
-
Upload
anahita-sharma -
Category
Health & Medicine
-
view
106 -
download
0
Transcript of Diagnosis of bacterial meningitis

ARE LUMBAR PUNCTURES THE BEST WAY TO DIAGNOSE BACTERIAL MENINGITIS? Group 13
LUMBAR PUNCTURE
○ One diagnostic tool that may be used to confirm or exclude meningitis is lumbar puncture (LP)
○ What is lumbar puncture? ● According to the NHS, a lumbar puncture is “ a
medical procedure where a sample of fluid is taken from inside the lower back for testing”
● Cerebrospinal fluid (CSF) is the colorless fluid that surrounds and supports the brain and spinal cord. When analyzing a sample of CSF in lumbar puncture, the values of glucose, protein, WBCs, and cell differentials can help determine the presence and type of meningitis.

THE LUMBAR PUNCTURE PROCEDURE
○ Very Briefly: ● Place patient on left side with back exactly horizontal,
aligned with edge of bed, with spine fully flexed - knees up to chin.
● Mark intervertebral space L4/5 or L3/4 (at same height as iliac crest)
● Anaesthetise skin with 1% lidocaine. ● After 1 minute, insert 22G spinal needle with stylet in
place, horizontally through mark, aiming towards umbilicus with needle bevel facing upwards
● Withdraw stylet and wait for CSF to appear at needle cuff.
● Collect fluid

Copyright 2006 by the American Medical Association. All Rights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use. American Medical Association, 515 N. State St, Chicago, IL 60610. Published by American Medical Association.
2
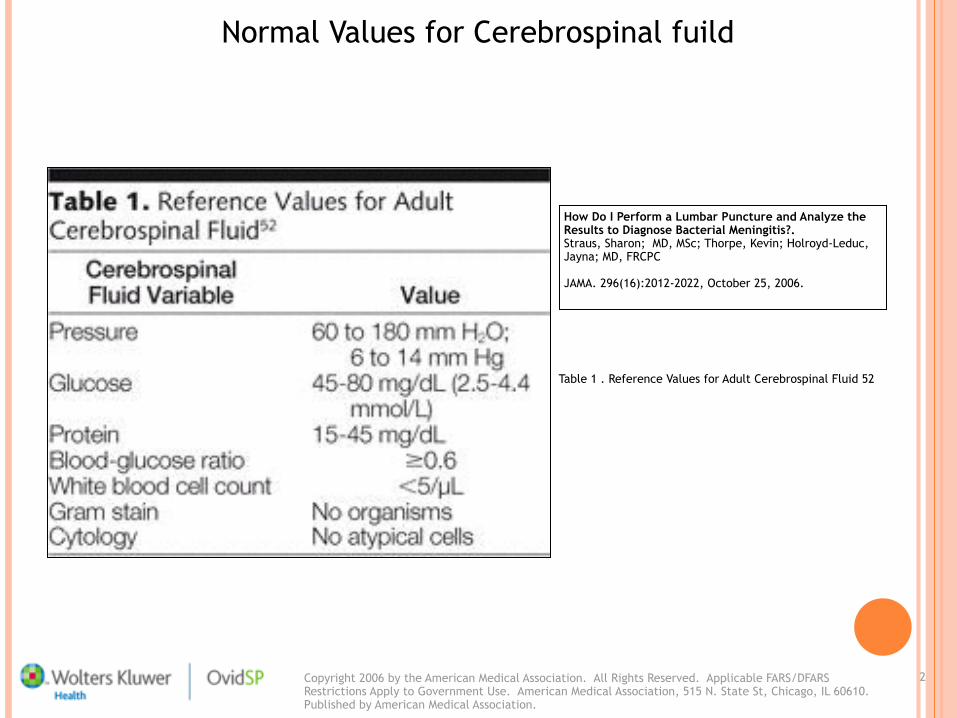
Normal Values for Cerebrospinal fuild
How Do I Perform a Lumbar Puncture and Analyze the Results to Diagnose Bacterial Meningitis?. Straus, Sharon; MD, MSc; Thorpe, Kevin; Holroyd-Leduc, Jayna; MD, FRCPC
JAMA. 296(16):2012-2022, October 25, 2006.
Table 1 . Reference Values for Adult Cerebrospinal Fluid 52
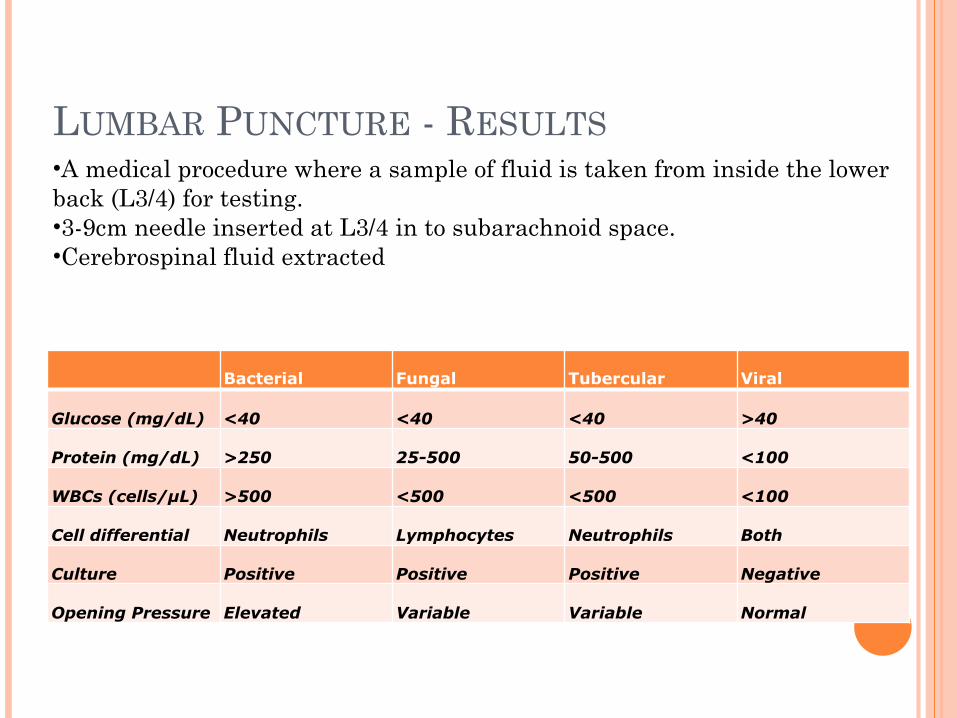
LUMBAR PUNCTURE - RESULTS
Bacterial Fungal Tubercular Viral
Glucose (mg/dL) <40 <40 <40 >40
Protein (mg/dL) >250 25-500 50-500 <100
WBCs (cells/µL) >500 <500 <500 <100
Cell differential Neutrophils Lymphocytes Neutrophils Both
Culture Positive Positive Positive Negative
Opening Pressure Elevated Variable Variable Normal
•A medical procedure where a sample of fluid is taken from inside the lower back (L3/4) for testing. •3-9cm needle inserted at L3/4 in to subarachnoid space. •Cerebrospinal fluid extracted

LIMITATIONS OF ANALYSIS OF CSF○ False positive reading due to contamination with
blood (i.e. due to the blood, not meningitis)
○ Neutrophil count can decrease by up to 50% in 2hr
WHAT ARE THE LIMITATIONS OF LUMBAR PUNCTURES? (1)
○ Taking a CT scan before a lumbar puncture may delay the administration of antibiotics
○ This is if raised intracranial pressure is suspected. ● Prospective study:
○ N = 142 cases of adult acute bacterial meningitis ○ Study provides compelling evidence that greater delays resulted in
higher case fatality rates ○ Such delays may be explained by inappropriate diagnostic-
treatment sequences: CT of the head followed by lumbar puncture followed by antibiotics
○ Suggests that some physicians prioritize accuracy of diagnosis over immediate administration of antibiotics
WHAT ARE THE LIMITATIONS OF LUMBAR PUNCTURES? (2) THERE ARE TIMES WHEN ONE SHOULD NOT PERFORM LUMBAR PUNCTURE:
○ Raised Intracranial pressure ○ Intracranial Lesion
Signs suggesting raised intracranial pressure: ! reduced or fluctuating level of consciousness (Glasgow Coma Scale Score less than 9 or a drop of 3 or more) ! relative bradycardia and hypertension ! focal neurological signs ! abnormal posture or posturing ! unequal, dilated or poorly responsive pupils ! papilloedema ! abnormal 'doll's eye' movements
WHAT ARE OTHER WAYS TO DIAGNOSE BACTERIAL MENINGITIS?

Kernig’s Sign Put the patient in the
supine position and the thigh flexed to a 90° right angle, attempts to straighten or extend the leg are met with resistance.
PHYSICAL EXAMINATIONS

PHYSICAL EXAMINATIONS
Brudzinski’s With the patient in
supine position. Flexion of the neck causes involuntary flexion of the knees and hips, or passive flexion of the leg on one side causes contralateral flexion of the opposite leg.

KERNIG’S SIGN AND BRUDZINSKI’S SIGN ○ A study in 2002 (N=287) has shown that this
diagnostic tool is too insensitive to identify the majority of patients with meningitis.
○ Sensitivity 5%
○ Specificity 95% ○These two physical examinations are not enough to make a definitive diagnosis of Bacterial Meningitis. Further diagnostic procedures are required.
BLOOD CULTURE / ANALYSIS: DIFFERENTIAL CELL COUNT (WBC)
○ Blood sample is taken and a white blood cell and CRP level is measured. A raised count of CRP and leukocytes (especially neutrophils) shows an increased risk of meningococcal disease
○ The blood glucose is also a reference of the CSF glucose level (which, if below 60% of blood, indicates presence of metabolising bacteria).
LIMITATIONS TO BLOOD CULTURES
○ A full blood culture may take 3-5 days
○ Whilst a normal C-reactive protein (CRP) and normal white blood cell count mean meningococcal disease is less likely, they do not rule it out. The CRP may be normal and the white blood cell count normal or low even in severe meningococcal disease.
○ CRP reaches peak level 48 hours after insult and degrades 18 hours after that. This is due to its short half-life.

POLYMERASE CHAIN REACTION (PCR)
○ PCR amplification of bacterial DNA from blood and CSF. It is more sensitive and specific than traditional microbiological techniques.
○ It is performed if the CSF culture is negative. ○ This is likely to become the new definitive test for
diagnosis. ○ May be helpful in diagnosing bacterial meningitis in
patients who have been pre-treated with antibiotics Early blood samples are more likely to be positive. A negative result does not rule out meningococcal disease.
CONCLUSION
○ Lumbar puncture is not the only way to aid diagnosis of suspected Bacterial Meningitis.
○ Other diagnostic procedures must be used in parallel with lumbar punctures.
○ BUT the speed of initiating antibiotics in bacterial meningitis is most important.
○ If Bacterial Meningitis is SUSPECTED, then antibiotics should be administered as soon as possible.
○ Negative readings on diagnostic tests do not necessarily rule out meningococcal disease.
HOW DO WE KNOW THAT SCIENTIFIC EVIDENCE IS RELIABLE?○ Using information from a reliable source
that was written by a reliable individual, group of individuals, or a reliable body/organisation.
○ Examples of sources that are less reliable: ● Yahoo answers
● Wikipedia
○ Examples of sources that are reliable: ● National Centre for Biotechnology Information
(NCBI) ● Journal articles/online Journal articles

BIBLIOGRAPHY
○ American College of Emergency Physicians, n.d. What to Know Before You Go. [online] Available at: http://www.emergencycareforyou.org/VitalCareMagazine/ER101/Default.aspx?id=500 [Accessed 20 November 2012]
○ Andrews PJ, 2004. Citerio G Intracranial pressure. Part one: historical overview
and basic concepts. Intensive Care Med. 30 pp.1730-3. ○ GlobalRph, n.d. Common Laboratory Values: Cerebrospinal Fluid Analysis.
[online] Available at: http://www.globalrph.com/cerebrospinal_fluid.htm [Accessed 19 November 2012]
○ Kumar, Prof. P. and Clark, Dr. M., 2009 Clinical Medicine. Spain: Elsevier
○ NHS, 2009. Electronic Prescribing: Briefing for Doctors. [pdf] Available at: http://www.connectingforhealth.nhs.uk/ [Accessed 25 November 2012]
○ Patient, n.d. Cerebrospinal fluid. [online] Available at: http://www.patient.co.uk/doctor/Cerebrospinal-Fluid.htm [Accessed 19 November 2012]
○ Patient, n.d. Lumbar Puncture. [online] Available at: http://www.patient.co.uk/doctor/Lumbar-Puncture-%28LP%29.htm [Accessed 19 November 2012]
BIBLIOGRAPHY
○ Smith, L. 2005. Management of Bacterial Meningitis: New Guidelines from IDSA. American Family Physician [online] 71(10) Available at: http://www.aafp.org/afp/2005/0515/p2003.html [Accessed 21 November 2012]
○ Steele RW, Marmer DJ, O'Brien MD, et al., 1986. Leukocyte survival in cerebrospinal fluid. J Clin Microbiol. 1986;23:965–966
○ Straus, S.E., MD, MSc, FRCPC, Thorpe, K.E., MMath and Holroyd-Leduc, J., MD, FRCPC. How Do I Perform a Lumbar Puncture and Analyze the Results to Diagnose Bacterial Meningitis? Journal of the American Medical Association. [pdf] 296(16) Available at: http://lrandic.instantglobe.com/mem-stick/JAMA_296_p2012.pdf [Accessed 22 November 2012]
○ World Health Organisation, 2012. Meningococcal Meningitis. [online] Available at: http://www.who.int/mediacentre/factsheets/fs141/en/index.html [Accessed 19 November 2012]
○ Scottish Intercollegiate Guidelines Network, 2008. Management of Invasive Meningococcal Disease in Children and Young People. (SIGN publication 102) [online] Edinburgh: SIGN. Available at: http://www.sign.ac.uk/guidelines/fulltext/102/index.html [Accessed 10 November 2012]