diagnosis and treatment planning for orthognathic surgery
110
© Ramaiah University of Applied Sciences 1 Faculty of Dental Sciences Diagnosis and treatment planning for orthognathic surgery Zeeshan Arif
-
Upload
zeeshan-arif -
Category
Health & Medicine
-
view
94 -
download
1
Transcript of diagnosis and treatment planning for orthognathic surgery

© Ramaiah University of Applied Sciences
1Faculty of Dental Sciences
Diagnosis and treatment planning for orthognathic surgery
Zeeshan Arif

© Ramaiah University of Applied Sciences
2Faculty of Dental Sciences
CONTENTS• History
• Etioligy
• Diagnosis and treatment planning
• Profile analysis
• Cephalometric evaluation
• -cogs
• -steiners
• -posteroanterior ceph analysis
• Panoramic radiographic assessment
• Tmj evaluation
• Errors in ceph analysis
• Limitations of ceph analysis
• Treatment plan
• Conclusion
• References

© Ramaiah University of Applied Sciences
3Faculty of Dental Sciences
INTRODUCTION
• When a jaw discrepancy accompanies a severe malocclusion, there are three broad
possibilities for correction:
• (1) growth modification
• (2) camouflage (orthodontic positioning of the teeth to compensate for the jaw
discrepancy)
• (3) orthognathic surgery in conjunction with orthodontics to reposition the jaws
and/or dentoalveolar segments.

© Ramaiah University of Applied Sciences
4Faculty of Dental Sciences
• Growth modification, generally referred to as dentofacial orthopedics, is the most
desirable approach to a severe skeletal problem when the potential for further
growth exists.
• Although the pattern of growth can be favorably modified for some patients, the
capacity for major increments in growth is rather limited.
• The variation in response of individual patients, however, suggests growth
modification should be attempted in preadolescent patients.

© Ramaiah University of Applied Sciences
5Faculty of Dental Sciences
• When a moderate skeletal discrepancy exists and there is no potential for further
growth (or if more change is required than can be accomplished through growth
modification alone), orthodontic camouflage should be considered.
• The teeth are repositioned to establish normal overjet and overbite in an effort to
compensate for the jaw discrepancy .

© Ramaiah University of Applied Sciences
6Faculty of Dental Sciences
• The final treatment option for a severe skeletal discrepancy is orthognathic surgery.
• Once growth has ceased, surgery becomes the only means of correcting a severe
jaw discrepancy.
• Although surgery may allow greater changes, there are still limitations to the
surgical options, depending on the type of problem and direction of desired jaw
movement, and certain problems are more receptive to surgical correction than
others.

© Ramaiah University of Applied Sciences
7Faculty of Dental Sciences
HISTORY
• First mandibular osteotomy : HULLIHEN (1849) done to correct a protrusive
malposition of a mandibular alveolar segment.
• In 1927, WASSMUND introduced total maxillary osteotomy and inverted “L” ramal
osteotomy, by external approach.
• In 1959, TRAUNER and OBWEGESER introduced sagittal split osteotomy as the
beginning of a new era of orthognathic surgery.
• The beginning of the early orthognathic surgery was in St.Louis where the
orthodontist Edward Angle and the surgeon Vilray Blair worked together

© Ramaiah University of Applied Sciences
8Faculty of Dental Sciences
• Epker, Bell and Wolford developed Lefort-1 maxillary downward fracture,so that we
can keep the maxilla stable in all 3 planes of spaces.
• By 1980 progress has reached to such an extent that, it is possible to reposition
either or both the jaws and to move the chin in all 3 planes of spaces & Rigid
internal fixation made it possible for comfort and better immobilization after
surgery.

© Ramaiah University of Applied Sciences
9Faculty of Dental Sciences
Etiology
• Known specific cause
syndromes
congenital defects
trauma
condylar hyperplaia
• Hereditary factors
• Environmental causes

© Ramaiah University of Applied Sciences
10Faculty of Dental Sciences
DIAGNOSIS AND TREATMENT PLANNING
• A. general patient evaluation
• 1.medical history
• 2. dental evaluation
• a) history
• b) general evaluation
• c) periodontal considerations
• d) occlusal-oral function evaluation

© Ramaiah University of Applied Sciences
11Faculty of Dental Sciences
• B. sociopsychological evaluation
• C. esthetic facial evaluation
• 1 frontal analysis
• 2 profile analysis
• D. radiographic evaluation
• 1 lateral cephalometric evaluation
• 2 posterior cephalometric evaluation
• 3 full mouth periapical evaluation
• 4 panoramic evaluation

© Ramaiah University of Applied Sciences
12Faculty of Dental Sciences
• E. occlusion and study cast evaluation
• 1 intra arch relationship
• 2 interarch relationship
• F. TMJ evaluation

© Ramaiah University of Applied Sciences
13Faculty of Dental Sciences
Medical analysis
• It can be obtained by means of a questionarre which is filled by the patient in his
first visit.
• The evaluation should be thorough.
• Existing problems should be discussed with the patients physician.
• The risk for general anaesthesia should be evaluated and discussed with the patient.
• Any congenital syndromes must be evaluated and any unusual growth pattern
should be recognised.

© Ramaiah University of Applied Sciences
14Faculty of Dental Sciences
Dental evaluation
HISTORY
• Previous restorative,orthodontic, periodontal, and facial pain treatment should be
reviewed.
• The patient compliance and future commitment to the treatment should be noted

© Ramaiah University of Applied Sciences
15Faculty of Dental Sciences
GENERAL EVALUATION
• Oral hygiene and previous dental treatment are good indications of patients dental
awareness and motivation for future treatment.
• Caries, periodontal and periapical pathology, and impacted third molars should be
noted.
• The need for implants should also be noted.
• Final prosthetic decisions are deferred , however, until completion of surgical
orthodontic treatment.

© Ramaiah University of Applied Sciences
16Faculty of Dental Sciences
PERIODONTAL CONSIDERATIONS
• The prognosis of any periodontically effected teeth is established and effect of
orthodontic and surgical treatment is considered.
• Periodontal disease and inadequately attached gingiva must be managed before
commencement of orthodontic treatment.
• Long term management and prognosis should be discussed with the periodontist
and the patient

© Ramaiah University of Applied Sciences
17Faculty of Dental Sciences
OCCLUSAL-ORAL FUNCTION EVALUATION
• Mastication, swallowing, mouth breathing, modified eating habits and maximum
mouth opening is documented.
• The effect of the dentofacial deformity on speech should be noted and patient
should be referred for speech evaluation.
• Tongue thrust, thumb sucking, and lip biting habits should be noted and their effect
on the deformity is evaluated

© Ramaiah University of Applied Sciences
18Faculty of Dental Sciences
SOCIOPSYCHOLOGIC EVALUATION
• The basic causes of patient dissatisfaction are
1. failure of the clinician to inform clearly to the patient of the realistic and probable treatment results especially the esthetic results
2.overoptimistic expectations of the patients.
• The clinician should refrain from overwhelming the patient with overt enthusiasm about the benefits of treatment, but rather should allow the patient to make his or her own decision.
• Some patients may need time to discuss future treatment from family and friends.
• Furthur counselling about realistic treatment expectations may be necessary, and treatment may even best be delayed until, through psychologic guidance, the patient can cope with treatment realities.

© Ramaiah University of Applied Sciences
19Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
20Faculty of Dental Sciences
Esthetic facial evaluation
• The clinical assessment of the face is probably the most valuable of all diagnostic procedures.
• The aesthetic facial evaluation should be performed in a systemic fashion with the patient standing or seated comfortably.
• Primary emphasis should be placed on frontal esthetics, since that is how ppl see themselves.
• The clinical examination of the face should always be done with two questions in mind:1. Would orthodontic-surgical treatment be able to correct the dental, skeletal, and soft
tissue structure diagnosed as abnormal?2. How would the orthodontic-surgical correction of the abnormal structures influence the
facial structures influence the facial structures considered to be normal• The patient should be examined in natural head posture, with the teeth in centric occlusion
and the lips relaxed

© Ramaiah University of Applied Sciences
21Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
22Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
23Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
24Faculty of Dental Sciences
Frontal analysis
• From the frontal view, it is particularly important to assess facial form; transverse
dimensions; facial symmetry; the vertical relationship in the upper, middle, and
lower thirds of the face and the lips.

© Ramaiah University of Applied Sciences
25Faculty of Dental Sciences
Facial form
• The relationship between the facial width and
vertical height has a strong influence on facial
harmony.
• The height-to-width proportion is 1.3:1 for females
and 1.35:1 for males.
• The bigonial width should be approximately 30%
less than the bizygomatic dimension

© Ramaiah University of Applied Sciences
26Faculty of Dental Sciences
Short, square facial types are often associated with
Class II deep bite malocclusion
vertical maxillary deficiency
masseteric hyperplasia
macro-genia
long, narrow facial types are often associated with
vertical maxillary excess
a narrow nose
mandibular anteroposterior deficiency
microgonia
a high palatal vault
an anterior open bite malocclusion

© Ramaiah University of Applied Sciences
27Faculty of Dental Sciences
Transverse dimensions
• The "rule of fifths"
• The face is divided into five equal parts--each the approximate width of the eye--from helix to helix of the outer ears
• The outer fifth is measured from the center helix of the ears to the outer canthus of the eyes.
• Prominent ears may have a profound effect on facial proportions and can be corrected by otoplasty.
• The medial two fifths of the face are measured from the outer to the inner canthus of the eyes.
• The outer border should coincide with the genial angles of the mandible

© Ramaiah University of Applied Sciences
28Faculty of Dental Sciences
• Width of the mouth should approximate the distance between the inner margins of the irides of the eyes
• The middle fifth is delineated by the inner canthus of the eyes.
• In patients with hyper-telorism, this fifth will be out of proportion with the other four fifths.
• The ala of the nose should coincide with these lines . • For patients in whom maxillary advancement and/or
superior repositioning is considered and the ala falls outside of the lines, control of alar width is indicated during surgery.

© Ramaiah University of Applied Sciences
29Faculty of Dental Sciences
Facial symmetry
• To assess facial symmetry, an imaginary line is drawn through the soft tissue glabella, pronasale, center of the filtrum of the upper lip and lower lip, and soft tissue pogonion
• The maxillary and mandibular dental mid-lines should be assessed in relation to the facial midline, as well as in relation to each other.
• It is also important to evaluate the mandibular dental midline in relation to the midline of the chin. This information will assist in treatment planning for correction of mandibular asymmetry by means of mandibular surgery, genioplasty, or both.
• Posteroanterior cephalometric radiography is indicated when a clinically significant asymmetry is present. This will allow the clinician to distinguish between bone, soft tissue, or a combination of the two as etiologic factors.

© Ramaiah University of Applied Sciences
30Faculty of Dental Sciences
Vertical relationship
• In the vertical dimension, the face can be divided into three equal parts :
• (1) upper third (hairline (trichion to the glabellar area)
• (2) middle third (glabellar area to subnasale)
• (3) lower third (subnasale to menton).

© Ramaiah University of Applied Sciences
31Faculty of Dental Sciences
Upper third of the face
• Fortunately, deformities that exist in the upper third of the face usually can be masked by an appropriate hairstyle. However, it is important to record deformities in this area, since they may indicate craniofacial deformities.
Middle third of the face
• The nose, center of the lips, and middle of the chin (in the lower third of the face) should fall along a true vertical line. Generally, no sclera is seen above or below the iris in a relaxed eyelid position with the patient looking straight ahead in natural head posture. Individuals with a mid-face deficiency tend to show sclera below the iris of the eye

© Ramaiah University of Applied Sciences
32Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
33Faculty of Dental Sciences
• The cheekbone-nasal base-lip contour is a convenient contour line to evaluate the harmony of the structures of the midface (zygoma, maxilla, and nasal base) with the paranasal area and upper lip.
• This line starts just anterior to the ear, extends forward through the cheekbone, and then runs anteroinferiorlyover the maxilla adjacent to the alar base of the nose, ending lateral to the commissure of the mouth.
• The line should form a smooth, continuing curve

© Ramaiah University of Applied Sciences
34Faculty of Dental Sciences
• Cc- cheekbone area
• A- zygomatic arch
• B-middle area
• C-subpupillary area
• D-commissure of the lip
• M*P- maxillary point- most medial point on the curve

© Ramaiah University of Applied Sciences
35Faculty of Dental Sciences
• Inturuption is lower in the curve indicative of mandibular prognathism

© Ramaiah University of Applied Sciences
36Faculty of Dental Sciences
Lower third of the face
• Vertical height – middle third to lower third = 5:6
• Upper lip makes up one third of the lower facial height
• If the upper lip is short there is a tendency of interlabial gap to be larger than normal
• The upper lip length should be related to lower anterior dental height
• Normal incisor show is around 1-4mm

© Ramaiah University of Applied Sciences
37Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
38Faculty of Dental Sciences
• Dental midline should coincide with the facial midline
• It can be corrected surgically or orthodontically
• The etiology can be dental or skeletal
• Causes- malpositioned teeth, crowding, tooth rotations, fixed partial dentures, tooth size descrepency
• In the mandible the chin is evaluated for symmetry, vertical relation and shape
• If the patient with facial asymmetry bites on a wooden spatula the cant is elevated

© Ramaiah University of Applied Sciences
39Faculty of Dental Sciences
• The amount of gingiva exposed during a smile is also noted
• The ideal gingival show is around 2mm , which is usually considered more in females than males
• The amount of tooth exposure is measured by :
The vertical length of the maxilla
Lip length
Maxillary incisors crown length
Amount of lip action with smile
Shape of cupids bow of the lip

© Ramaiah University of Applied Sciences
40Faculty of Dental Sciences
Lips
• Asymmetry causes- cleft lip, facial nerve dysfunction, underlying dentoskeletal
asymmetry, scarring due to previous trauma, unilateral microsomia or macrosomia
• The lower lip generally exibits 25% more vermilion than the upper lip
• In repose the lips shoud be 0-3mm apart

© Ramaiah University of Applied Sciences
41Faculty of Dental Sciences
PROFILE ANALYSIS
UPPER THIRD OF THE FACE
• The supraorbital rims normally project 5 to 10 mm beyond the most anterior projection of the globe of the eye.
• Frontal bossing, supraorbital hypoplasia, exophthalmos, or enophthalmos should be distinguished.
MIDDLE THIRD OF THE FACE
• It is helpful to examine the middle and upper thirds of the face in isolation, and masking the lower third with a card eliminates any undue influence that this third may have on the perceptions of the face as a whole.
• The nose, cheeks, and paranasal areas are sequentially evaluated.

© Ramaiah University of Applied Sciences
42Faculty of Dental Sciences
Nose
• The shape of the dorsum is noted as normal, convex, or concave.
• The projection of the nasal bridge should be anterior to the globes (5 to 8 mm).
• It is important to distinguish between a dorsal hump and a turned-down tip, since the implications for treatment are entirely different.

© Ramaiah University of Applied Sciences
43Faculty of Dental Sciences
Nasal projection• The nasal projection measured horizontally from
subnasale to nasal tip is normally 16 to20mm
• Nasal projection is an indicator of maxillary antero posterior position.
• This length becomes particularly important when planning for anterior movement of maxilla.

© Ramaiah University of Applied Sciences
44Faculty of Dental Sciences
Orbital rim
• The orbital rim is an antero-posterior indicator of maxillary position.
• Deficient orbital rims may correlate positionally with a retruded maxillary position because the osseous structures are often deficient as groups ,rather than in isolation.
• The Eye globe normally is positioned 0-2mm anterior to the orbital rim.

© Ramaiah University of Applied Sciences
45Faculty of Dental Sciences
Cheeks• The cheeks should exhibit a general convexity
from cheek-bone apex to the commissure of the mouth.
• This line of convexity, called the cheekbone-nasal base-lip curve contour, requires simultaneous frontal and profile examination.
• This line starts just anterior to the ear, extending forward through the cheekbone, then anteroinferiorly over the maxilla adjacent to the alar base of the nose and ending lateral to the commissure of the mouth
• The line should form a smooth continuous curve with no breaks

© Ramaiah University of Applied Sciences
46Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
47Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
48Faculty of Dental Sciences
Paranasal sinus areas
• It is important because it plays an important role in distinguishing between middle third deficiency and mandibular anteroposteriorexcess

© Ramaiah University of Applied Sciences
49Faculty of Dental Sciences
Lower third of the face
Lips
• the protrusion, retrusion and soft tissue thickness of each lip is evaluated with the lips in repose
• The upper lip usually projects slightly anterior than the lower lip
• An individual with an excessive increase in lower lip vermillion and a deep labiomental fold aften has a class ii division 1 malocclusion
• The subnasale-pogonion line, also called the lower facial plane, is an important guide in assessing the lip position and planning orthodontic and surgical positioning of the chin

© Ramaiah University of Applied Sciences
50Faculty of Dental Sciences
• The upper lip should be 3+/- 1 mm ahead of this line and the lower lip 2+/- 1 mm ahead of this line.
• This assessment is influenced by the anteroposterior position of the chin and the soft tissue thickness of the lips

© Ramaiah University of Applied Sciences
51Faculty of Dental Sciences
Labiomental fold
• The lower lip- chin contour should have a gentle S-curve, with a lower lip- chin angle of at least 130 degrees.
• The angle is often acute in cases of class 11 mandibular anteroposteriordeficiency because of impingement of the maxillary incisor on the lower lip or macrogenia.

© Ramaiah University of Applied Sciences
52Faculty of Dental Sciences
Chin throat area
• Also termed cervicomental angle
• Varies between 105-120º.
• Absolute 110 o.
• Distance Between pogonian to neck chin angle is 50mm.

© Ramaiah University of Applied Sciences
53Faculty of Dental Sciences
CEPHALOMETRIC EVALUATION

© Ramaiah University of Applied Sciences
54Faculty of Dental Sciences
• Glebella (G): The most anterior point of the frontal bone
• Nasion (N): The most anterior point on the frontal nasal suture in the midsagittal plane
• Orbitale (Or): The lowest point on the inferior orbital rim
• Sella (S): The center of the sells turcica, as on the lateral cephalogram, which is located by inspection

© Ramaiah University of Applied Sciences
55Faculty of Dental Sciences
• Pterygomaxillare (Ptm): The apex of the teardrop-shaped pterygomaxillaryfissure (lowest point of the opening)
• Basion (Ba): The point where the median sagittal plane of the skull intersects the lowest point in the anterior margin of the foramen magnum

© Ramaiah University of Applied Sciences
56Faculty of Dental Sciences
• Anterior nasal spine (ANS): Anterior tip of the nasal spine
• Posterior nasal spine (PNS): The most posterior aspect of the palatal bone
• A-point, or subspinale: The most posterior midline point in the concavity where the lower anterior edge of the anterior nasal spine meets the alve-olarbone overlying the maxillary incisors
• B-point, or supramentale: The most posterior midline point in the concavity of the mandible between the alveolar bone overlying the mandibular incisors (infradentale) and the pogonion

© Ramaiah University of Applied Sciences
57Faculty of Dental Sciences
• Pogonion (Pog): The most anterior point of the chin
• Gonion (Go): The point defined by using two lines, one tangent to the inferior border of the mandible and the other tangent to the posterior border of the ramus; found by bisecting the angle formed by the two lines and extending the bisector through the curvature of the mandible
• Gnathion (Gn): The lowest, most anterior mid-line point on the symphysis of the mandible (midway between the menton and the pogonion)

© Ramaiah University of Applied Sciences
58Faculty of Dental Sciences
• Menton (Me): The most inferior point on the symphysis of the mandible in the midline
• Porion (Po): The most superior point of the ex-ternal auditory meatus (anatomic point); the machine porionis the uppermost point on the outline of the rods of the cephalometer
• Condylion (Co): The most posterosuperior point on the head of the condyle

© Ramaiah University of Applied Sciences
59Faculty of Dental Sciences
Hard tissue planes
1. "True horizontal" plane (HP): A line perpendicu-lar to a plumb line on the radiograph will be the HP for a specific patient.
2. Constructed horizontal plane (cHP): A horizontal plane constructed by drawing a line through nasion at an angle of 7 degrees.Thisplane tends to be close to true horizontal.
3. Anterior cranial base (S-N): Formed by a line drawn from sella to nasion
4. Basion-nasion (Ba-N) plane: Extends between basion and nasion and divides the face and the cranium

© Ramaiah University of Applied Sciences
60Faculty of Dental Sciences
5.Frankfort horizontal (FH) plane: Extends from porion to orbitale
6.Pterygoid vertical (Ptv): A vertical line perpendicular to the Frankfort horizontal plane and drawn through the distal outline of the pterygomaxillary fissure
7.Functional occlusal plane: A line through the cusp contacts of the molars and premolars defines this plane
8.Occlusal plane: Formed by a line drawn through the mesial cusp contact of the molars and dividing the incisor overbite
9.Dental plane: Extends between A-point and pogonion
10.Mandibular plane: Extends from gonion to gnathion

© Ramaiah University of Applied Sciences
61Faculty of Dental Sciences
Analysis (COGS)
Burstone, Randal, Legan, Murphy & Norton
(1978)

© Ramaiah University of Applied Sciences
62Faculty of Dental Sciences
• The COGS appraisal describes
– Dental
– Skeletal
– Soft tissue variations.

© Ramaiah University of Applied Sciences
63Faculty of Dental Sciences
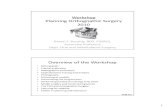
CRANIAL BASE
HORIZONTAL PLANE (HP), which is a surrogate Frankfort plane,constructed by drawing a line 7 o from the line S to N.
Most measurements will be made from projections either parallel or perpendicular to the Horizontal Plane
7

© Ramaiah University of Applied Sciences
64Faculty of Dental Sciences
• ARTICULARE (Ar): Intersection of basisphenoid and posterior border of the condyle.

© Ramaiah University of Applied Sciences
65Faculty of Dental Sciences
Articulare-Nasion : length of the cranial base
• Measured parallel to HP from Arto N
• Not an absolute value but a skeletal baseline to be correlated to other measurements
• Proportionate to mandibular and maxillary lengths

© Ramaiah University of Applied Sciences
66Faculty of Dental Sciences
• Ar- PTM :• It is a measurement of the
horizontal distance between the posterior aspects of the mandible and maxilla
• The greater the distance between Ar-PTM, the more the mandible will lie posterior to the maxilla, assuming that all other facial dimensions are normal.
• Therefore, one factor for prognathism or retrognathismcan be evaluated by this measurement of cranial base.

© Ramaiah University of Applied Sciences
67Faculty of Dental Sciences
Males Females
Ar-Ptm (
|| to HP)
37.1 +
2.8
32.8 +
1.9
Ptm-N ( ||
to HP)
52.8 +
4.1
50.9 +
3.0
Cranial Base

© Ramaiah University of Applied Sciences
68Faculty of Dental Sciences
HORIZONTAL SKELETAL PROFILE
• N-A –Pg (Angle): gives an indication of the overall facial convexity. A positive (+) angle of convexity denotes a convex face; a negative (-) angle denotes a concave face.
• Men = 3.9+- 0.4
• Females=2.6 +- 5.1

© Ramaiah University of Applied Sciences
69Faculty of Dental Sciences
• N-A : A perpendicular from HP is dropped through N.
• The horizontal position of A is measured to this perpendicular line ( N-A).
• This measurement describes the apical base of maxilla in relation to N and enables the clinician to determine if the anterior part of maxilla is protrusive or retrusive.
• Useful in planning treatment of anterior maxillary horizontal advancement or reduction, and of total maxillary horizontal advancement or reductions.
• Mean : males= 0.0 +/- 3.7mm ; females = -2.0 +/- 3.7

© Ramaiah University of Applied Sciences
70Faculty of Dental Sciences
• N-B : Also measured in a plane parallel to HP from the perpendicular line dropped from N.
• This measurement describes the horizontal position of the apical base of mandible in relation to N.
• Useful in planning the treatment of anterior mandibular horizontal advancement or reduction and the total mandibular horizontal advancement or reduction

© Ramaiah University of Applied Sciences
71Faculty of Dental Sciences
• N- POG
• Measured in the same manner as N- A and N-B and indicates the prominence of the chin.
• This measurement helps to determine if there is a horizontal genial hyperplasia or hypoplasia.
• Useful in the planning of augmentation or reduction genioplasty, of anterior mandibular horizontal advancement or reduction, and of total mandibular horizontal advancement or reduction

© Ramaiah University of Applied Sciences
72Faculty of Dental Sciences
VERTICAL SKELETAL ANALYSIS
• All measurements are made perpendicular to HP
• Determines the anterior posterior or complex dysplasia of the face
• Diagnosis of anterior, posterior, or total vertical hyperplasia or hypoplasia
• It also determines the clockwise or counterclockwise rotations of the mandible

© Ramaiah University of Applied Sciences
73Faculty of Dental Sciences
VERTICAL SKELETAL ANALYSIS
• Middle third facial height : Distance from N to ANS
• Posterior maxillary height : PNS-N
• Lower third facial height : ANS – GN
• Divergence of mandible posteriorly : M.P-H.P angle(clockwise or counter -clockwise rotations of the maxilla and mandible)

© Ramaiah University of Applied Sciences
74Faculty of Dental Sciences
MAX-MAND. RELATIONSHIP
• The total effective length of the maxilla is the distance from PNS-ANS that is projected on a line parallel to HP
• The ANS-PNS distance with the measurements of N-ANS and N-PNS, give a quantitative description of the maxilla in the skull complex

© Ramaiah University of Applied Sciences
75Faculty of Dental Sciences
• Ar - Go : Length of Mandibular ramus
• Go - Pg : Length of Mandibular body
• Ar - Go - Gn Angle : Gonialangle that represents the relationship between ramalplane and MP. Vertical /Horizontal growth
• B - Pg : Distance from B point to line perpendicular to MP through Pg describes chin prominence.

© Ramaiah University of Applied Sciences
76Faculty of Dental Sciences
VERTICAL DENTAL ANALYSIS
• Upper incisor to NF: Anterior maxillary dental height
• Lower incisor to MP: Anterior mandibular dental height
These two measurements define how far the incisors have erupted in relation to NF and MP respectively.

© Ramaiah University of Applied Sciences
77Faculty of Dental Sciences
• Max. molar to NF : Posterior maxillary dental height
• Mand. Molar to MP: Post mandibulardental height

© Ramaiah University of Applied Sciences
78Faculty of Dental Sciences
• Occlusal Plane- upper HP:increasedangle= skeletal open bite, lip incompetence, increased facial height, retrognatia.
• Decreased angle= deep bite, decreased facial height, lip redundancy
• Upper incisors to NF angle & Lower incisors to MP angle: These angulations determine the protrusion or rectrusion of the incisors.

© Ramaiah University of Applied Sciences
79Faculty of Dental Sciences
Soft Tissue Landmarks
• Glabella(G) The most prominent point of the forehead.
• Soft tissue nasion (N) The deepest point of the bridge of the nose.
• Pronasale (Pn)– the most anterior point of the nose
• Subnasale(Sn)- The point at which the base of the nose merges with the upper cutaneous lip.

© Ramaiah University of Applied Sciences
80Faculty of Dental Sciences
• Labiale superius(Ls) The median point of the upper margin of the upper membranous lip.
• Stomion superius(Sts)- the lowest point of the vermilion of the upper lip
• Stomion inferius(Sti)- the uppermost point of the lower lip vermilion
• Labiale inferius(Li) The median point of the lower margin of the lower membranous lip

© Ramaiah University of Applied Sciences
81Faculty of Dental Sciences
• Soft tissue pogonion(Pog) The foremost point on the soft tissue chin in the mid-sagittal plane.
• Soft tissue menton(Me) The lowermost point on the soft tissue chin in the sagittal plane.

© Ramaiah University of Applied Sciences
82Faculty of Dental Sciences
Soft tissue planes
1. Facial plane: Extends from nasion to pogonion (N'-Pog')
2. Upper facial plane: Extends from soft time glabella to subnasale (G'-Sn)
3. Lower facial plane: Extends from subnasale to soft tissue pogonion(Sn-Pog')
4. S-line: Formed by connecting soft tissue pogonion to a point midway between pronasale and subnasale
5. E-line (esthetic plane)- extends from the tip of the nose to the soft tissue pog

© Ramaiah University of Applied Sciences
83Faculty of Dental Sciences
Facial form
• Overall soft tissue profile, the angle of convexity or facial contour angle= angle between G-Sn-Pg
• As the angle of facial convexity becomes a smaller positive or a negative value, the profile is suggestive of a Class III skeletal and dental relationship.
• As the positive angle increases, the profile becomes more convex, suggesting a Class II skeletal and dental
relationship.

© Ramaiah University of Applied Sciences
84Faculty of Dental Sciences
• A line perpendicular to the horizontal plane (HP) is dropped from glabella and the relationship of the maxilla and mandible are related to it to determine if the problem is maxillary or mandibular.
• The distance to subnasale from this vertical line measured parallel to the horizontal plane describes the amount of maxillary excess or deficiency in the anteroposterior dimension
• A negative number suggests a maxillary retrusionand a positive number suggests a prognathism

© Ramaiah University of Applied Sciences
85Faculty of Dental Sciences
• The position of pogonion is also measured parallel to HP from the perpendicular line dropped from glabella
• This measurement gives an indication of mandibular prognathism or retrognathism
• As the magnitude of mandibular deficiency decomes more severe, the more negative is the measurement(G-Pg)

© Ramaiah University of Applied Sciences
86Faculty of Dental Sciences
• The lower facial throat angle(Sn-Gn-C)is formed by the intersection of Sn-Gnand Gn-C
• An appreciation of this angle is critical in planning the treatment to correct anteroposterior facial dysplasia
• An obtuse angle suggests that no chin augmentation procedures to be done

© Ramaiah University of Applied Sciences
87Faculty of Dental Sciences
• In vertical dimension, the anterior facial proportionality is assessed by taking the ratio of the middle third to lower third of the facial height
• G-Sn:Sn-Me= 1:1
• Ratio less than 1:1= large lower third of the face

© Ramaiah University of Applied Sciences
88Faculty of Dental Sciences
Lip position
• Nasolabial angle is an important tool for measuring anterosuperior dysplasias
• An acute nasolabial angle is helpful in surgical retraction of the maxilla
• An obtuse nasolabial angle suggests a degree of maxillary hypoplasia and calls for a maxillary advancement or orthodontic proclination of maxillary incisors.

© Ramaiah University of Applied Sciences
89Faculty of Dental Sciences
• Anteroposterior lip position is evaluated by drawing a line from subnasale to soft tissue pogonion, and the amount of lip protrusion or retrusion is measured as a perpendicular linear distance from this line to the most prominent point of both lips
• Retracting or protracting the incisors surgically ororthodontically or advancing or reducing the prominence ofthe chin, or both, can achieve concordant lip position.

© Ramaiah University of Applied Sciences
90Faculty of Dental Sciences
• The labiomental sulcus is measured from the depth of the sulcus perpendicular to the Li -Pg' line.
• A sulcus of about 4 mm is average
• Flared lower incisors, extruded upper incisors that roll out the lower lip, flaccid lower lip tone, and abnormal morphology of the lip itself are all factors that can effect the inclination of the lower lip and deepen the labiomental sulcus.

© Ramaiah University of Applied Sciences
91Faculty of Dental Sciences
• Uprighting the lower incisors, intruding maxillary incisors, and cheiloplasty to retract the lower lip all can help in reducing a deep sulcus.
• The prominence of the bony chin also affects the depth ofthe sulcus.
• Advancement genioplasty will help deepen the sulcus and reduction genioplasty will aid in reducing excessive sulcular depth.

© Ramaiah University of Applied Sciences
92Faculty of Dental Sciences
• The lower third of the face (Sn - Me') can be divided into thirds; the length of the upper lip, or the distance Sn - Stms, should be approximately one third the total
• When this ratio becomes smaller, often a vertical reduction genioplasty should be considered

© Ramaiah University of Applied Sciences
93Faculty of Dental Sciences
• The distance of the upper lip to the maxillary incisor (Stms - I) is a key factor in determining the vertical position of the maxilla.
• Two millimeters of maxillary incisor showing below the upper lip with the lip at rest has been shown to be desirable.
• This will also correspond in general with a pleasing smile.
• Patients with vertical maxillary excess tend to show a large amount of upper incisor with the lips in repose.

© Ramaiah University of Applied Sciences
94Faculty of Dental Sciences
• Patients with vertical maxillary deficiency tend not to show maxillary teeth with lips relaxed and may have incisors at a level superior to the upper lip, giving an edentulous look.
• Orthodontically extruding the maxillary teeth or surgically positioning the maxilla inferiorly may be the preferable treatment in these patients with a short face, provided a stable increase in vertical dimension is possible

© Ramaiah University of Applied Sciences
95Faculty of Dental Sciences
• Interlabial gap is fairly ideal at a range of from just lightly touching to approximately 3 mil apart.
• Patients with vertical maxillary excess tend to have large interlabial gaps and lip incompetency.
• Raising the level of the maxilla to shorten facial height will decrease a large interlabial gap and allow the patient to close the lips without muscle strain.
• Patients with vertical maxillary deficiency often have no interlabial gap and have lip redundancy with a rolling out of the upper and lower lips

© Ramaiah University of Applied Sciences
96Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
97Faculty of Dental Sciences
STEINER’S ANALYSIS

© Ramaiah University of Applied Sciences
98Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
99Faculty of Dental Sciences©M. S. Ramaiah University of Applied Sciences
99

© Ramaiah University of Applied Sciences
100Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
101Faculty of Dental Sciences
POSTEROANTERIOR CEPHALOMETRIC RADIOGRAPHIC EVALUATION

© Ramaiah University of Applied Sciences
102Faculty of Dental Sciences
Landmarks
• SF: where the smaller wing of sphenoid bone crosses the medial orbital ridge
• ANS: the centre point at the base of the nose
• Jugulare (J): The most superior and medal point on the zygomatic buttress
• Mastoid (M): The most inferior point on the mastoid bone
• A: The contact area between the maxillary incisors
• B: The contact area between the mandibular in-cisors

© Ramaiah University of Applied Sciences
103Faculty of Dental Sciences
• Y: The most lateral point on the buccalsurface area of the first maxillary molar
• Z: The most lateral point on the buccalsurface area of the first mandibular molar
• Gonion (Go): The most inferior posterior point at the angle of the mandible
• Menton (Me): The most inferior point at the an-terior mandibular area
• CH: The most inferior lateral point on the anterior inferior border of the mandible

© Ramaiah University of Applied Sciences
104Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
105Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
106Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
107Faculty of Dental Sciences
Errors in cephalometric measurements
• Radiographic cephalometry is a two dimensional representation of three dimensional object.
• Errors in cephalometric measurements- magnification or distortion
• Errors in landmark identification
- Quality of the radiographic image
- Precision of landmark definition
- Reproduceability of landmark location

© Ramaiah University of Applied Sciences
108Faculty of Dental Sciences
Limitations of ceph analysis
• 1)Growth pattern not taken into consideration
• 2)Mean values are based on different population
• 3)Two dimensional representation of three dimensional object
• 4)Form and functions not taken into consideration

© Ramaiah University of Applied Sciences
109Faculty of Dental Sciences©M. S. Ramaiah University of Applied Sciences
109
• A combination of various cephalometric norms and variables should be compiled to arrive at a proper diagnosis.
• Although innumerable controversies exist in the field of cephalometrics, it is still a very significant & effective diagnostic tool.
Conclusion

© Ramaiah University of Applied Sciences
110Faculty of Dental Sciences
REFERENCES
• Bell, William H, William R Proffit, and Raymond P White. Surgical Correction Of Dentofacial Deformities. 1st ed. Philadelphia, Pa.: Saunders, 1980.
• Burstone CJ, James RB, Legan H, Murphy GA, Norton LA.; Cephalometrics for orthognathic surgery.; J Oral Surg. 1978 Apr;36(4):269-77.
• Reyneke, Johan P. Essentials Of Orthognathic Surgery. 1st ed. Hanover Park, IL: Quintessence Pub.