
Diagnosis and treatment of primary synovial cell sarcoma ...
9
Diagnosis and treatment of primary synovial cell sarcoma that occurred in the left mandible body: a case report and literature review Qian Tao, PhD, a Bin Qiao, MD, a,b Yi Wang, MD, a and Fengchun Hu, MD a Guangdong, China, and Queensland, Australia SUN YAT-SEN UNIVERSITY AND GRIFFITH UNIVERSITY Objective. The authors describe a case of synovial sarcoma in the left mandible body. Study design. The primary tumor was investigated morphologically and immunohistochemically. The patient was treated with madibulectomy and lymph node dissection, which was followed by an immediate reconstruction of the left mandible with a revascularized osteomyocutaneous fibula free flap. Results. The primary tumor was described as gingival sarcoma. The initial preoperative biopsy showed positive staining for cytokeratin, vimentin, smooth muscle actin, and desmin by immunohistochemistry. The definitive diagnosis of monophasic synovial sarcoma was established following postoperative excision biopsy. Antigens of S-100 and CD99 displayed positive staining but epithelial membrane antigen, Bcl-2, and CD34 were negative. Also, no metastasis or other bone swelling was observed by radionuclide survey suggesting the left mandible was the primary lesion of occurrence. Conclusions. Synovial sarcoma is an uncommon soft tissue malignant neoplasm. This is the sixth case of primary synovial sarcoma occurring in the jaw. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:e12-e20) A cancer diagnosis between 15 and 30 years of age is 2.7 times more common than a diagnosis during the first 15 years of life, and yet it is still relatively rare compared with malignant neoplasms occurring in older age groups. 1 The distribution of such malignant neo- plasms in persons 15 to 30 years of age is unique depending on the types that occur. Hodgkin lymphoma, for example, has the highest incidence within this age group. Soft tissue sarcoma is also reported frequently in adolescents; however, its international incidence rate is only between 1.8 and 5.0 cases per 100,000 per year. 2 Synovial cell sarcoma is a malignant mesenchymal neoplasm that has been reported frequently in 15- to 30-year-old patients without gender imbalance. 3 It ac- counts for up to 10% of all histologic types of soft tissue sarcoma. 4 The final incidence of synovial cell sarcoma, therefore, ranges only between 1.8 and 5.0 cases per 1 million per year. Most synovial cell sarcoma is reported in the extrem- ities, typically in a periarticular location or close to a bursa or tendon sheath. 5 The head and neck has been regarded as an extremely rare location of synovial cell sarcoma with the hypopharynx being the most com- monly affected site. The other reported sites are the masticator space, parapharyngeal space, sinonasal space, and infratemporal fossa. 6 In this study, we describe a rare case of synovial cell sarcoma occurring primarily in the left mandible body in a young Chinese woman. We also summarize the clinicopathological features of previously reported cases in the relative regions of synovial cell sarcoma. CASE PRESENTATION The patient, a 20-year-old woman, complained of a recurring swelling in the region of the left posterior teeth, without pain, but she felt alveodental suppu- ration. Three years prior she underwent a local ex- cision of tumor in the same intraoral region at an outside hospital. The tumor was diagnosed as benign epulis. For 4 months before enrolling in our hospital, she found a recurrence of the swelling, augmenting quickly, and accompanied by teeth motility. No his- tory of trauma was mentioned in her presentation. Facial asymmetry and left facial swelling were ob- served. Physical examination revealed a 6 4-cm, firm, tender, nonmobile mass in the left mental fo- ramen region. No restriction of mouth opening or lymph node enlargement was observed. X-ray indi- Q.T. and B.Q. contributed equally to this work. a Department of Oral and Maxillofacial Surgery, Guanghua School of Stomatology and Institue of Stomatological Research, Sun Yat-sen University, Guangzhou, Guangdong, China. b Centre for Medicine and Oral Health, School of Dentistry and Oral Health, Griffith University, Gold Coast, Queensland, Australia. Received for publication Jul 1, 2010; returned for revision Aug 3, 2010; accedpted for publication Aug 10, 2010. 1079-2104/$ - see front matter © 2011 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2010.08.025 e12
Transcript of Diagnosis and treatment of primary synovial cell sarcoma ...

Diagnosis and treatment of primary synovial cell sarcoma thatoccurred in the left mandible body: a case report andliterature reviewQian Tao, PhD,a Bin Qiao, MD,a,b Yi Wang, MD,a and Fengchun Hu, MDaGuangdong, China,and Queensland, AustraliaSUN YAT-SEN UNIVERSITY AND GRIFFITH UNIVERSITY
Objective. The authors describe a case of synovial sarcoma in the left mandible body.Study design. The primary tumor was investigated morphologically and immunohistochemically. The patient wastreated with madibulectomy and lymph node dissection, which was followed by an immediate reconstruction of theleft mandible with a revascularized osteomyocutaneous fibula free flap.Results. The primary tumor was described as gingival sarcoma. The initial preoperative biopsy showed positivestaining for cytokeratin, vimentin, smooth muscle actin, and desmin by immunohistochemistry. The definitivediagnosis of monophasic synovial sarcoma was established following postoperative excision biopsy. Antigens of S-100and CD99 displayed positive staining but epithelial membrane antigen, Bcl-2, and CD34 were negative. Also, nometastasis or other bone swelling was observed by radionuclide survey suggesting the left mandible was the primarylesion of occurrence.Conclusions. Synovial sarcoma is an uncommon soft tissue malignant neoplasm. This is the sixth case of primary
synovial sarcoma occurring in the jaw. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:e12-e20)A cancer diagnosis between 15 and 30 years of age is2.7 times more common than a diagnosis during thefirst 15 years of life, and yet it is still relatively rarecompared with malignant neoplasms occurring in olderage groups.1 The distribution of such malignant neo-plasms in persons 15 to 30 years of age is uniquedepending on the types that occur. Hodgkin lymphoma,for example, has the highest incidence within this agegroup. Soft tissue sarcoma is also reported frequently inadolescents; however, its international incidence rate isonly between 1.8 and 5.0 cases per 100,000 per year.2
Synovial cell sarcoma is a malignant mesenchymalneoplasm that has been reported frequently in 15- to30-year-old patients without gender imbalance.3 It ac-counts for up to 10% of all histologic types of softtissue sarcoma.4 The final incidence of synovial cellsarcoma, therefore, ranges only between 1.8 and 5.0cases per 1 million per year.
Q.T. and B.Q. contributed equally to this work.aDepartment of Oral and Maxillofacial Surgery, Guanghua School ofStomatology and Institue of Stomatological Research, Sun Yat-senUniversity, Guangzhou, Guangdong, China.bCentre for Medicine and Oral Health, School of Dentistry and OralHealth, Griffith University, Gold Coast, Queensland, Australia.
Received for publication Jul 1, 2010; returned for revision Aug 3,2010; accedpted for publication Aug 10, 2010.1079-2104/$ - see front matter© 2011 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2010.08.025e12
Most synovial cell sarcoma is reported in the extrem-ities, typically in a periarticular location or close to abursa or tendon sheath.5 The head and neck has beenregarded as an extremely rare location of synovial cellsarcoma with the hypopharynx being the most com-monly affected site. The other reported sites are themasticator space, parapharyngeal space, sinonasalspace, and infratemporal fossa.6
In this study, we describe a rare case of synovial cellsarcoma occurring primarily in the left mandible bodyin a young Chinese woman. We also summarize theclinicopathological features of previously reportedcases in the relative regions of synovial cell sarcoma.
CASE PRESENTATIONThe patient, a 20-year-old woman, complained of
a recurring swelling in the region of the left posteriorteeth, without pain, but she felt alveodental suppu-ration. Three years prior she underwent a local ex-cision of tumor in the same intraoral region at anoutside hospital. The tumor was diagnosed as benignepulis. For 4 months before enrolling in our hospital,she found a recurrence of the swelling, augmentingquickly, and accompanied by teeth motility. No his-tory of trauma was mentioned in her presentation.Facial asymmetry and left facial swelling were ob-served. Physical examination revealed a 6 � 4-cm,firm, tender, nonmobile mass in the left mental fo-ramen region. No restriction of mouth opening or
lymph node enlargement was observed. X-ray indi-
OOOOEVolume 111, Number 2 Tao et al. e13
cated a large area of bone absorption (Fig. 1, A). Acomputed tomography (CT) scan revealed a continu-ity fragment of the normal structure of left mandiblebody (Fig. 1, B, C), whereas a 3-dimensional recon-structive CT disclosed a soft mass invading in thebone (Fig. 1, D). The patient underwent pathologicbiopsy before the operation, which showed positivestaining for the proteins cytokeratin (CK), vimentin(Vim), smooth muscle actin (SMA), and desmin(Des); a diagnosis of gingival sarcoma was given(Fig. 2).
Preliminary diagnosis and operative designationThe preliminary diagnosis of gingival sarcoma
was based on the following considerations. First, theclinical symptoms suggested that the tumor could bemalignant rather than benign because of the proper-ties of its speed of augmentation, alveodental suppu-ration, and the bone destruction. Although a fewbenign mandible neoplasms also possess the pheno-type of bone invasion, such as ameloblastoma andodontogenic keratocyst,7 their growth speed is lim-ited and the symptom of alveodental suppuration isunusual. Second, the pathologic biopsy diagnosisdemonstrated that the tumor originated from mesen-chymal tissues rather than epithelia because the spin-dle-shaped cells were observed predominantly withthe positive markers of mesenchyma (Vim, SMA,Des). Although fibroblastlike cells are also observedin some cases of gingival squamous cell carcinoma,8
epithelial cells are, however, the majority rather thanstromal cells, and the epithelial cells often constitute“cancer nests.” Third, abnormal aggregation of ra-dionuclide occurred in the left mandible (Fig. 3),suggesting that the enhanced metabolism of bonewas a result of the invading mass.9 In summary, wemade the preliminary diagnosis that this lesion oc-curring in the left mandible body was gingival sar-coma. This was consistent with the preoperative di-agnosis by pathologic biopsy.
To consider the characteristics of malignancy andbone invasion of the tumor, we designed the operationin 3 parts: extensive neoplasm resection, extensive leftmandibulectomy and lymph node dissection, and thepreparation of a revascularized osteomyocutaneous fib-ula free flap for the reconstruction of the left mandible.
Definitive diagnosis and postoperative careDuring the process of the operation, we found that
the cortex of the bone was destroyed completely bytumor cells invading the medulla of bone down to thelevel of the mandibular canal. The tumor, the subtotalof the left mandible, and the regional lymph nodes were
excised successfully. The final size of the tumor was8 � 6 � 5 cm (Fig. 4), and it was soft and without acapsule. Frozen section microscopy showed no meta-static tumor cells in the lymph nodes. Following theassessment of the primary lesion by immunohistochem-istry, we found not only the proteins of CK, Vim, SMA,and Des, but also S-100 and CD99 showed positivestaining (Fig. 2). Epithelial membrane antigen, Bcl-2and CD34 were also studied but did not show positivestaining (Fig. 2), which was not consistent with theproperties of gingival sarcoma. Because gingival sar-comas, including angiosarcoma, malignant fibrous his-tiocytoma, and liposarcoma, are often associated withthe negative expression of CD99 but positive expres-sion of CD34,10-12 it was suggested that the hemato-poietic and vascular-associated tissues should not beinvolved in this lesion, but that immunocytes were.This diagnosis was adjusted from gingival sarcoma tosynovial cell sarcoma because of the pre- and postop-erative immunohistochemistry assays.
After tumor resection, the patient underwent adju-vant radiation treatment (4000 cGy), for 1 month.When the radiotherapy finished, the patient wasasked to return for several check-ups over 6 months.At present, the patient is free of recurrence withoutfunctional disturbances of mastication, swallowing,and speech (Fig. 5).
DISCUSSIONThe term synovial cell sarcoma was first proposed by
Knox in 1936. It was nominated because in histologythe cases reported in the early period showed someresemblance of the tumor to normal synovial tissues.This tumor, however, can be found anywhere in thehuman body without restriction to synovial cells. Theorigin of the tumor from synovial tissue therefore hasnot been fully elucidated.13
Most of these tumors are reported in the extremi-ties. It is suspected that because of misdiagnosis inthe oral and maxillofacial region only about 100cases have been published in head and neck sites todate.13 Notably, intraoral cases are extremely rare, infact, only 31 patients had been reported in Englishlanguage journals by the end of 2003.14 This numberincreased to 37 in 200913,15-19 with the tongue beingthe common site of the intraoral cases.15,16 The oth-ers are cheek, soft palate, gingivobuccal sulcus, ret-romolar area, submental, floor of mouth, and jawbone. Interestingly, in these 37 cases only 7 subjectsare reported in jaws, including 2 cases occurring inthe mandible metastatic from calf and foot, respec-tively20 (Table I). So far it is known that only 5 caseshave existed that are the primary synovial cell sar-comas occurring in jaws (tumors found in temporo-
mandibular joint are excluded). Here, we report a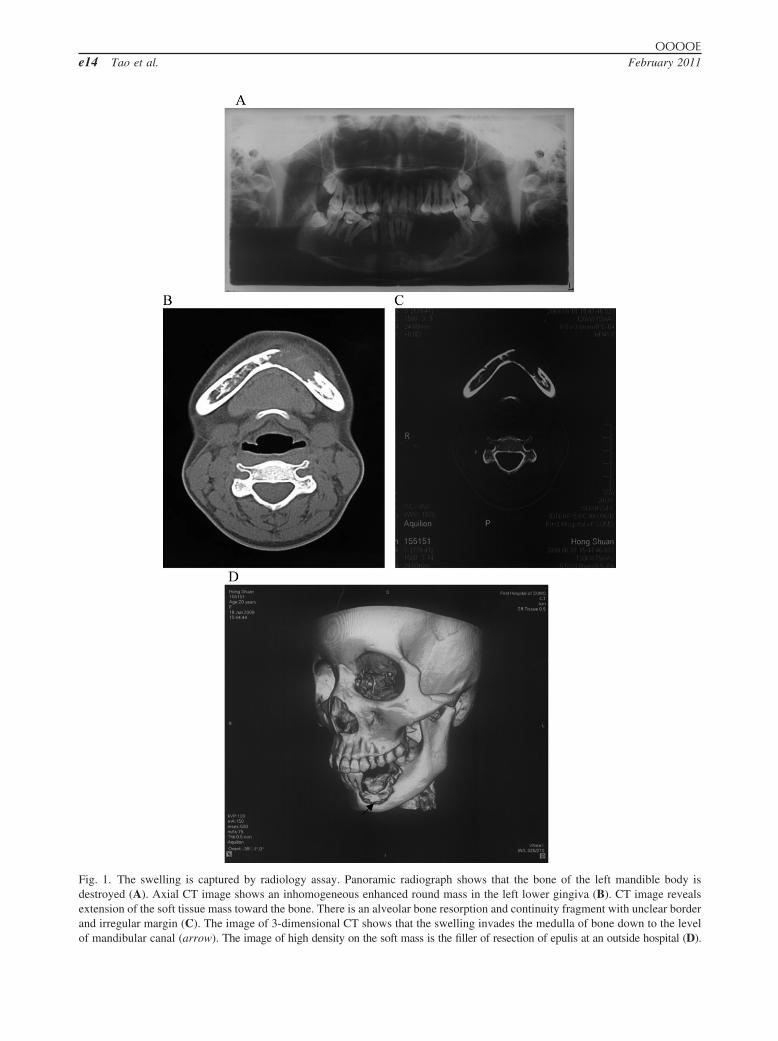
OOOOEe14 Tao et al. February 2011
Fig. 1. The swelling is captured by radiology assay. Panoramic radiograph shows that the bone of the left mandible body isdestroyed (A). Axial CT image shows an inhomogeneous enhanced round mass in the left lower gingiva (B). CT image revealsextension of the soft tissue mass toward the bone. There is an alveolar bone resorption and continuity fragment with unclear borderand irregular margin (C). The image of 3-dimensional CT shows that the swelling invades the medulla of bone down to the level
of mandibular canal (arrow). The image of high density on the soft mass is the filler of resection of epulis at an outside hospital (D).
OOOOEVolume 111, Number 2 Tao et al. e15
Fig. 2. The biopsy specimen of the tumor is illustrated by immunohistochemistry assay. All are at the magnification of �200. Thesubtype of this neoplasm is monophasic, with predominant spindle cell component by hematoxylin and eosin staining (A). Itshowed that antigens of cytokeratin (B), vimentin (C), smooth muscle actin (D), desmin (E), S-100, (F) and CD99 (G) are all positive,but epithelial membrane antigen (H), Bcl-2 (I), and CD34 (J) are negative. The arrows in J are positive endothelial cells but not tumor
cells.
OOOOEe16 Tao et al. February 2011
rare case of a local recurrence in the left mandiblebody, and then summarize the properties of synovialcell sarcoma in origin, diagnosis, and treatment.
As described previously, although the tendency isto arise near large joints,24 it seems that the origin ofsynovial cell sarcoma is not related to synovial tis-sues, and the name synovial sarcoma may be a mis-nomer. Recently, a novel nomenclature of “carcino-sarcoma” has been discussed based on frequentcoexpression of epithelial and mesenchymal mark-ers, such as CK and Vim. In fact, the feature of“uncertain differentiation” of this neoplasm is cur-rently regarded as part of the nature of this kind oftumor.25 It has been reported that myoblasts could betargeted as a potential source of synovial cell sarco-
Fig. 3. Metastasis is detected by radionuclide survey.99mTechnetium scintigraphic scans show increased uptake ofisotope in the left mandible. No other sites of abnormalaggregation of radionuclide are shown in this assay. A, ante-rior view. B, posterior view.
ma.26 In one study, a conditional mouse model over-
expressing the oncoprotein of SYT-SSX2 in imma-ture myoblasts within the skeletal muscle lineage, ledto the induction of synovial cell sarcoma with 100%penetrance. However, when its expression was trans-fected into more differentiated myoblasts, the induc-tion of myopathy appeared without tumor forma-tion.26 This new discovery provided a novel insightthat undifferentiated cells of skeletal muscle lineagewere the origin of synovial cell sarcoma as well asillustrating a clinical phenomenon of frequent occur-rence within or in proximity to skeletal muscles ofthis neoplasm.27
The diagnosis of synovial cell sarcoma is a toughtask at present. It is the fourth most common type ofsarcoma following malignant fibrous histiocytoma, li-posarcoma, and rhabdomyosarcoma.28 Misdiagnosisoften occurs among these types of sarcoma, especiallyat the oral and maxillofacial region. The optimal diag-nosis of synovial cell sarcoma is composed of a mul-tispecialty approach. CT is the key indicator and initialstaging of a lesion, as it is helpful in identifying subtlesoft tissue calcifications and local bony changes, par-ticularly in regions of complex anatomy.29 Because CTimages of all types of sarcoma reveal similar extensionof the soft tissue mass, the definitive diagnosis of tumorcould not be made except for at the border and marginof the neoplasm. For example, on the image of gingivalangiosarsoma, bone window settings show a regularmargin and clear border of bone resorption, whichmight illustrate that angiosarsoma is less aggressivethan other malignant tumors.30 Compared with the im-ages of synovial cell sarcoma on which the margins ofbone invasion are often irregular and unclear,31 it issuggested that angiosarsoma and synovial cell sarcomacould be discerned only by CT scan. It has been shown,however, that a CT scan could not distinguish osteo-genic sarcoma, such as osteosarcoma from synovial cellsarcoma of primary bone origin. Osteoid tumor matrixmineralization is the typical feature of osteosarcoma onthe images of CT, while they show soft tissue extensioncomponent usually beyond the area of bone destruc-tion.32 Similarly, soft tissue synovial cell sarcoma maybe calcified in 15% to 20% of cases.33 Hence, if themass of synovial cell sarcoma primarily originates frombone, it is more difficult to make a correct diagnosis byCT scan alone, even if the osteoblastic changes arefound with a bone window.
Although histopathologic diagnosis is more persua-sive than radiology for a synovial cell sarcoma, thedifferential diagnosis of mesenchymal tumors and thosewith mesenchymal-like features, still can be difficult.34
Synovial cell sarcoma tumors are uniquely composedof 2 morphologically distinct cell types: spindle cells
and epithelioid cells. Three histologic subtypes, coming
ues co
OOOOEVolume 111, Number 2 Tao et al. e17
from the presence of the 2 cell types, exist along acontinuous spectrum: biphasic, monophasic (predomi-
Fig. 4. Operative findings of the resected tumor. It can be seewithout capsule, being excised with the connective bone tiss
Fig. 5. The reexamination of the patient in the convalescencfibula flap is well, without bone absorption and tumor recurrenpostsurgery. Physical examination reveals the color of skin ianterior view; E and F, lateral views.
nant fibrous or rare epithelial), and poorly differentiat-
ed.35 Monophasic epithelial synovial cell sarcoma orthe gland predominant biphasic synovial cell sarcoma is
the cortex of bone is totally destroyed. The neoplasm is soft,mpletely. A, anterior view. B, posterior view.
stsurgery. Panoramic radiograph shows that the retention of2 months postsurgery. B, 4 months postsurgery. C, 6 monthsal, without necrosis and darkness at the final return visit: D,
n that
e of poce. A,
s norm
similar to adenocarcinoma leading to potential misiden-

, chem
OOOOEe18 Tao et al. February 2011
tification as adenocarcinoma.36 The poorly differenti-ated type poses a diagnostic challenge and demon-strates structures that resemble high-grade small roundcell tumors: high cellularity, frequent mitosis, and ne-crosis. The common diagnosis of synovial cell sarcomais the biphasic pattern or monophasic fibrous type, butalso can be easily confused with spindle cell carcinoma,myofibromatosis, leiomyosarcoma, primitive neuroec-todermal tumors, malignant peripheral nerve sheathtumors, and malignant fibrous histiocytoma. It has beenadvised that a panel of antibodies in an immunohisto-chemistry assay must be assessed together with otherobservations. For example, unlike other spindle cellsarcomas, synovial cell sarcoma expresses CK7 and 19,which can help to distinguish it from neurogenic tu-mors.37,38 Also, CD34, the vascular-associated marker39
is often not expressed in synovial cell sarcoma, which canhelp to distinguish it from vascular tumors. More impor-tantly, synovial cell sarcoma demonstrates a specific t(X;18) (p11.2;q11.2) translocation,40 which is a more signif-icantly useful diagnostic tool, especially when histologicfeatures are equivocal.
Taking into consideration that synovial cell sarcomais a somatic genetic disease and tumorigenesis is de-pendent on a permissive microenvironment, preventionof local recurrence and distant metastasis of this tumorare the pivotal tasks of treatment. Depending on theextent of the lesion, the surgical intervention includescomplete resection together with affiliated organ dis-section and regional lymph node dissection. In the oraland maxillofacial region, however, the integrity of per-sonal appearance is a big challenge for surgeons afterablation of malignant and aggressive tumors.41 Today,ensuring good morphology and function are primarygoals in the reconstruction of oral cavity. Loss of man-
Table I. Clinicopathological features of reported and cCase Reference Site Age
1 Maxymiw (1990)21 Maxilla R 32
2 Karr (1991)20 Mandible L premolar areametastatic from L calf
41
3 Karr (1991)20 Mandible R metastaticfrom L foot
63
4 Torsiglieri (1991)22 Mandible 28
5 Captier (1999)23 Mandible in premolararea
10
6 Tilakaratne (2006)13 Ramus of the mandible R 297 Granowetter (2006)19 Mandible body L 118 Tao (2010) Mandible body L 20
A/W, alive and well; B, biphasic; L, left; M, monophasic; R, right;C
dible continuity results in alteration in speech, swal-
lowing, and mastication. A variety of free vascularizedflaps have been suggested as useful treatment of man-dibular discontinuity defects, including the iliac crest,radius, scapula, and fibula.42 Although vascularizedfibula transfer has become the preferred method ofmandible reconstruction after oncological surgical ab-lation,43 when it should be operated on is still a con-troversy. Primary reconstruction following tumor abla-tion seems to be mandatory in most of the cases withinthe oral cavity. This offers several advantages com-pared with the secondary reconstruction. It avoids fi-brosis in the surgical bed and minimizes significantfunctional disability.44 In the process of tumor ablation,however, the “safety boundary” of malignant and ag-gressive tumors is difficult to define, so an unexpectedseed of risk of recurrence would be buried in theimmediate reconstruction, which could finally result infailure of treatment.
In light of the disadvantages mentioned previously, ithas been advised that radiation therapy and chemother-apy must be added following primary reconstruction tohelp kill potentially migratory cells of synovial cellsarcoma.45 In a retrospective study, however, it wasshown that there was no significant difference in out-come between patients treated with or without chemo-therapy at this stage even though the use of radiationtherapy proved to be a significant factor in reducingmortality.46 In that research, the authors also confirmeda conventional viewpoint that tumor size was an im-portant prognostic factor for both overall survival andevent-free survival.47,48 Tumor size of 5 cm or greaterand the presence of bone and neurovascular invasionwere independent adverse predictors of distant recur-rence and mortality.47 It was documented that lesionsranging from 2 to 14 cm were observed; however, most
t cases of synovial cell sarcoma in jawser Size, cm Type Treatment Follow-Up
ale 10 B C/R/S Dead: multiplemetastases
ale 5 � 5 M Late R/C Dead: multiplemetastases
ale Unknown M R Dead: metastases tolung, liver, andbone
8 � 8 B S/R/C Dead: metastases tolung and bone
5 B C/S/R A/W: 1 y
ale 6 � 5 � 2 M S/R A/W: 2 yUnknown Unknown C/S/R A/W: 3 mo
ale 8 � 6 � 5 M S/R A/W: 1 y
otherapy; R, radiation; S, surgery.
urrenGend
Fem
Fem
Fem
Male
Male
FemMaleFem
tend to be large—more than 85% were larger than 5 cm

OOOOEVolume 111, Number 2 Tao et al. e19
in 1 series of deeper lesions.48 In this case report, thefinal size of the neoplasm was 8 � 6 � 5 cm. Althoughthe tumor was quite large, the prognosis of the patientwas good at 6 months postsurgery, and at present thepatient is free of recurrence.
CONCLUSIONSTo the best of our knowledge, this is the sixth case of
primary synovial cell sarcoma occurring in the jaw. Thedefinitive diagnosis was made by CT scan and immu-nohistochemistry. Given that jaws are circumvolutedby masseter muscle, temporalis, buccinator, medialpterygoid muscle, and lateral pterygoid muscle, wesuspect the true origin of the reported 6 cases of syno-vial cell sarcoma is undifferentiated myoblasts but isnot osteogenic. Exploring this hypothesis is the subjectof further work.
The treatment of this tumor was complete surgicalresection supplemented with radiation therapy, withoutchemotherapy. Although the patient currently is free ofrecurrence, long-term observation is advised, as it hasbeen calculated that tumor size larger than 5 cm asso-ciates with poor outcomes.
ConsentWritten informed consent was obtained from the
patient for publication of this case report and all ac-companying images.
We gratefully acknowledge Dr Emily M. Sullivanfrom Department of Pathology, Griffith UniversitySchool of Medicine for critical comments and Englishrevision on this manuscript.
REFERENCES1. Bleyer A, Viny A, Barr R. Cancer in 15 to 29-year-olds by
primary site. Oncologist 2006;11:590-601.2. Wibmer C, Leithner A, Zielonke N, Sperl M, Windhager R.
Increasing incidence rates of soft tissue sarcomas? A population-based epidemiologic study and literature review. Ann Oncol2010;21:1106-11.
3. Raney RB. Synovial sarcoma in young people: background,prognostic factors, and therapeutic questions. J Pediatr Hematol/Oncol 2005;27:207-11.
4. Cormier JN, Pollock RE. Sarcomas. CA Cancer J Clin2004;54:94-109.
5. Murray PM. Sarcoma of the upper extremity. Hand Clin2004;20:325-33.
6. Rangheard AS, Vanel D, Viala J, Schwaab G, Casiraghi O, Sigal R.Synovial sarcomas of the head and neck: CT and MR imaging findingsof eight patients. AJNR Am J Neuroradiol 2001;22:851-7.
7. Oliveira Neto P, Sávio E, Bezerra TP, Avelar RL, Raimundo RdeC, Gomes AC, et al. Anterior mandibular swelling. J Oral Max-illofac Surg 2010;68:436-41.
8. Kudo Y, Ogawa I, Kitagawa M, Kitajima S, Samadarani Siri-wardena BS, Aobara N, et al. Establishment and characterizationof a spindle cell squamous carcinoma cell line. J Oral Pathol Med
2006;35:479-83.9. Imola MJ, Gapany M, Grund F, Djalilian H, Fehling S, AdamsG. Technetium 99m single positron emission computed tomog-raphy scanning for assessing mandible invasion in oral cavitycancer. Laryngoscope 2001;111:373-81.
10. Scholsem M, Raket D, Flandroy P, Sciot R, Deprez M. Primarytemporal bone angiosarcoma: a case report. J Neuro Oncol2005;75:121-5.
11. Hartel PH, Jackson J, Ducatman BS, Zhang P. CD99 immuno-reactivity in atypical fibroxanthoma and pleomorphic malignantfibrous histiocytoma: a useful diagnostic marker. J Cutan Pathol2006;33(Suppl 2):24-8.
12. Goto T, Motoi N, Motoi T, Okuma T, Kawano H, Yamamoto A, et al.Spindle cell lipoma of the knee: a case report. J Orthop Sci 2004;9:86-9.
13. Tilakaratne WM. Synovial sarcoma of the mandible. J OralPathol Med 2006;35:61-3.
14. Meer S, Coleman H, Altini M. Oral synovial sarcoma: a report of2 cases and a review of the literature. Oral Surg Oral Med OralPathol Oral Radiol Endod 2003;96:306-15.
15. de Almeida-Lawall M, Mosqueda-Taylor A, Bologna-MolinaRE, Domínguez-Malagón HR, Cano-Valdéz AM, Luna-Ortiz K,et al. Synovial sarcoma of the tongue: case report and review ofthe literature. J Oral Maxillofac Surg 2009;67:914-20.
16. Komis C, Lagogiannis GA, Faratzis G, Rapidis AD. Synovialsarcoma of the tongue: report of a case and review of theliterature. J Oral Maxillofac Surg 2008;66:154-60.
17. Sharif MA, Mushtaq S, Mamoon N, Khadim MT, Asghar Z.Biphasic synovial sarcoma of oral cavity. J Coll Physicians SurgPak 2008;18:713-5.
18. Wang H, Zhang J, He X, Niu Y. Synovial sarcoma in the oral andmaxillofacial region: report of 4 cases and review of the litera-ture. J Oral Maxillofac Surg 2008;66:161-7.
19. Granowetter L, Ladas E, Taromina K, Rooney D, Kelly KM.Integrative Tumor Board: pediatric synovial sarcoma. IntegrCancer Ther 2006;5:48-55.
20. Karr RA, Best CG, Salem PA, Toth BB. Synovial sarcomametastatic to the mandible: report of two cases. J Oral MaxillofacSurg 1991;49:1341-6.
21. Maxymiw WG, Wood RE. Synovial sarcoma of the maxillofacialregion with osseous involvement. Case report. Int J Oral Maxil-lofac Surg 1990;19:305-7.
22. Torsiglieri AJ Jr, Hendrix RA, Quinn PS. Synovial sarcoma ofthe jaw. Ear Nose Throat J 1991;70:396-8.
23. Captier G, Montoya P, Duché R, Le Barazer M, Bigorre M,Margueritte G. Synovial sarcoma of the mandible in children.Apropos of a case. Rev Stomatol Chir Maxillofac 1999;100:187-91.
24. Jones BC, Sundaram M, Kransdorf MJ. Synovial sarcoma: MRimaging findings in 34 patients. AJR Am J Roentgenol1993;161:827-30.
25. Haldar M, Randall RL, Capecchi MR. Synovial sarcoma: fromgenetics to genetic-based animal modeling. Clin Orthop RelatRes 2008;466:2156-67.
26. Haldar M, Hancock JD, Coffin CM, Lessnick SL, Capecchi MR.A conditional mouse model of synovial sarcoma: insights into amyogenic origin. Cancer Cell 2007;11:375-88.
27. Al-Daraji W, Lasota J, Foss R, Miettinen M. Synovial sarcomainvolving the head: analysis of 36 cases with predilection to theparotid and temporal regions. Am J Surg Pathol 2009;33:1494-503.
28. White RD, Makar J Jr, Steckler RM. Synovial sarcoma of thetemporomandibular joint. J Oral Maxillofac Surg 1992;50:1227-30.
29. O’Sullivan PJ, Harris AC, Munk PL. Radiological features ofsynovial cell sarcoma. Br J Radiol 2008;81:346-56.
30. Uchiyama Y, Murakami S, Kishino M, Furukawa S. A case

OOOOEe20 Tao et al. February 2011
report of primary gingival angiosarcoma. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2009;108:e17-21.
31. Marzano L, Failoni S, Gallazzi M, Garbagna P. The role ofdiagnostic imaging in synovial sarcoma. Our experience. RadiolMed 2004;107:533-40.
32. Shao Z, He Y, Wang L, Hu H, Shi H. Computed tomographyfindings in radiation-induced osteosarcoma of the jaws. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e88-94.
33. Milchgrub S, Ghandur-Mnaymneh L, Dorfman HD, Albores-Saavedra J. Synovial sarcoma with extensive osteoid and boneformation. Am J Surg Pathol 1993;17:357-63.
34. Cheng CY, Chang KM, Chang KW, Chang CH, Liu CJ, KushnerGM. Rapidly growing mass in mandibular gingiva. J Oral Max-illofac Surg 2004;62:214-7.
35. Weiss SW, Goldblum JR, editors. Enzinger and Weiss’s softtissue tumors. 4th ed. St Louis: Mosby; 2001.
36. Weinreb I, Perez-Ordoñez B, Guha A, Kiehl TR. Mucinous,gland predominant synovial sarcoma of a large peripheral nerve:a rare case closely mimicking metastatic mucinous carcinoma.J Clin Pathol 2008;61:672-6.
37. Folpe AL, Schmidt RA, Chapman D, Gown AM. Poorly differ-entiated synovial sarcoma: immunohistochemical distinctionfrom primitive neuroectodermal tumors and high-grade malig-nant peripheral nerve sheath tumors. Am J Surg Pathol1998;22:673-82.
38. Pelmus M, Guillou L, Hostein I, Sierankowski G, Lussan C,Coindre JM. Monophasic fibrous and poorly differentiated syno-vial sarcoma: immunohistochemical reassessment of 60 t(X;18)(SYT-SSX)-positive cases. Am J Surg Pathol 2002;26:1434-40.
39. Furness SG, McNagny K. Beyond mere markers: functions forCD34 family of sialomucins in hematopoiesis. Immunol Res2006;34:13-32.
40. Barco R, Garcia CB, Eid JE. The synovial sarcoma-associatedSYT-SSX2 oncogene antagonizes the polycomb complex proteinBmi1. PLoS ONE 2009;4:e5060.
41. Jeremic JV, Nikolic ZS, Boricic IV, Tacevic ZD, TomanovicNR, Drcic LJ, et al. Total mandibular reconstruction after
resection of rare “honeycomb-like” ameloblastic carcino-ma—A case report. J Craniomaxillofac Surg 2010;38:465-8[10.1016/j.jcms.2009.10.020].
42. Peled M, El-Naaj IA, Lipin Y, Ardekian L. The use of freefibular flap for functional mandibular reconstruction. J Oral Max-illofac Surg 2005;63:220-4.
43. González-García R, Naval-Gías L. Transport osteogenesis in themaxillofacial skeleton: outcomes of a versatile reconstructionmethod following tumor ablation. Arch Otolaryngol Head NeckSurg 2010;136:243-50.
44. González-García R, Naval-Gías L, Rodríguez-Campo FJ,Román-Romero L. Reconstruction of oromandibular defects byvascularized free flaps: the radial forearm free flap and fibularfree flap as major donor sites. J Oral Maxillofac Surg2009;67:1473-7.
45. Ferrari A, Gronchi A, Casanova M, Meazza C, Gandola L,Collini P, et al. Synovial sarcoma: a retrospective analysis of 271patients of all ages treated at a single institution. Cancer2004;101:627-34.
46. Brennan B, Stevens M, Kelsey A, Stiller CA. Synovial sarcomain childhood and adolescence: a retrospective series of 77 pa-tients registered by the Children’s Cancer and Leukaemia Groupbetween 1991 and 2006. Pediatr Blood Cancer 2010;55:85-90.
47. Lewis JJ, Antonescu CR, Leung DH, Blumberg D, Healey JH,Woodruff JM, et al. Synovial sarcoma: a multivariate analysis ofprognostic factors in 112 patients with primary localized tumorsof the extremity. J Clin Oncol 2000;18:2087-94.
48. Tateishi U, Hasegawa T, Beppu Y, Satake M, Moriyama N.Synovial sarcoma of the soft tissues: prognostic significance ofimaging features. J Comput Assist Tomogr 2004;28:140-8.
Reprint requests:Qian Tao, PhDDepartment of Oral and Maxillofacial SurgeryGuanghua School of StomatologySun Yat-sen University56 Ling Yuanxi RoadGuangzhou, Guangdong, 510055, China
[email protected]

















