Diagnosis and management of the epilepsies in children · Prognosis is primarily determined by the...
6
Prescriber April 2018 ❚ 13 prescriber.co.uk PRESCRIBING IN CHILDREN ■ E pilepsy is a condition in which an individual is prone to recurrent seizures. An epileptic seizure is a change in movement or behaviour that is the direct result of a primary change in the electrical activity of the brain. Epilepsy is as common as diabetes, but continues to retain a stigma, which means many individuals with the condition remain ‘hidden’. Furthermore, there is no single diagnostic test, meaning there is a high rate of misdiagnosis. Correct diagnosis and management has major implications for long-term outlook. Consequently, guidelines specify that diagnosis in children should be made by a paediatrician with expertise in the con- dition, based on the description of events experienced, and review should continue in secondary care. Practical clinical definition of epilepsy Epilepsy is a family of disorders that is comprised of many different diseases and conditions. More accurately, it should therefore be referred to as the epilepsies. In the current prac- tical approach of the International League Against Epilepsy (ILAE), epilepsy is defined by any of the following conditions: 1 • At least two unprovoked (or reflex) seizures occurring >24 hours apart. • One unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years. • Diagnosis of an epilepsy syndrome. The term ‘unprovoked’ implies the absence of a temporary or reversible factor lowering the seizure threshold. A seizure after concussion, with fever, with alcohol withdrawal or in association with hypoglycaemia in the newborn would exemplify a provoked seizure that would not lead to a diagnosis of epilepsy. A provocative factor is ‘‘a transient and sporadic endoge- nous or exogenous element capable of augmenting seizure inci- Diagnosis and management of the epilepsies in children CHRISTINE PRAGER AND J HELEN CROSS There are many different types of epilepsy that can occur in childhood, therefore identification and management can be complex. Here, the authors discuss the diagnosis of epilepsy in children, choice of antiepileptic drug treatments and their adverse effects, and non-pharmacological treatment options. SPL
Transcript of Diagnosis and management of the epilepsies in children · Prognosis is primarily determined by the...

Prescriber April 2018 ❚ 13prescriber.co.uk
PRESCRIBING IN CHILDREN ■
Epilepsy is a condition in which an individual is prone to recurrent seizures. An epileptic seizure is a change in
movement or behaviour that is the direct result of a primary change in the electrical activity of the brain. Epilepsy is as common as diabetes, but continues to retain a stigma, which means many individuals with the condition remain ‘hidden’. Furthermore, there is no single diagnostic test, meaning there is a high rate of misdiagnosis. Correct diagnosis and management has major implications for long-term outlook. Consequently, guidelines specify that diagnosis in children should be made by a paediatrician with expertise in the con-dition, based on the description of events experienced, and review should continue in secondary care.
Practical clinical definition of epilepsyEpilepsy is a family of disorders that is comprised of many different diseases and conditions. More accurately, it should therefore be referred to as the epilepsies. In the current prac-tical approach of the International League Against Epilepsy (ILAE), epilepsy is defined by any of the following conditions:1
• At least two unprovoked (or reflex) seizures occurring >24 hours apart.• One unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years.• Diagnosis of an epilepsy syndrome.
The term ‘unprovoked’ implies the absence of a temporary or reversible factor lowering the seizure threshold. A seizure after concussion, with fever, with alcohol withdrawal or in association with hypoglycaemia in the newborn would exemplify a provoked seizure that would not lead to a diagnosis of epilepsy. A provocative factor is ‘‘a transient and sporadic endoge-nous or exogenous element capable of augmenting seizure inci-
Diagnosis and management of the epilepsies in childrenCHRISTINE PRAGER AND J HELEN CROSS
There are many different types of epilepsy that can occur in childhood, therefore identification and management can be complex. Here, the authors discuss the diagnosis of epilepsy in children, choice of antiepileptic drug treatments and their adverse effects, and non-pharmacological treatment options.
SPL

■ PRESCRIBING IN CHILDREN l Epilepsies
14 ❚ Prescriber April 2018 prescriber.co.uk
dence in persons with chronic epilepsy and evoking seizures in susceptible individuals without epilepsy.’’2 A prominent example of a provocative factor is sleep deprivation, which might elicit a seizure in a healthy person as well as being a common factor for seizures in people with juvenile myoclonic epilepsy. Other common provocative factors are emotional stress, tiredness and excessive alcohol consumption. A reflex seizure is one that is precipitated by a sensory stimulus, the most common being a visual stimulus such as flickering light, striped black and white patterns, or a television in susceptible individuals. Other precipitating stimuli include noises or (rarely) music, tactile stimulation and reading. A reflex epilepsy syndrome is defined as: ‘‘a syndrome in which all epileptic seizures are precipitated by sensory stimuli”3 and although the seizures are provoked, they occur because there is an underlying susceptibility to have recurrent seizures. In such situations, seizures may be prevented by avoiding the stimulus. An epilepsy syndrome is characterised by a specific set of clinical and electrical characteristics: by age of onset, seizure types, EEG patterns, and co-morbidities such as intellectual impairment.4 Epilepsy syndromes are distinct clinical entities that carry treatment and prognostic implications. A detailed description of epilepsy syndromes is beyond the scope of this review, but can be found on the ILAE website (https://www.epilepsydiagnosis.org). A syndrome should be identified at diag-nosis if at all possible, but the epilepsy may be described in the context of the type of seizure (see Figure 1)5 or even in relation to the underlying cause (see Figure 2).6
Prevalence, incidence and prognosis Epilepsy is the most prevalent neurological condition in children and adults. The median lifetime prevalence in developed coun-tries has been estimated to be 5.8 per 1000 (range 2.7–12.4) with a median prevalence of active epilepsy of 4.9 per 1000 (range 2.3–10.3). Annual incidence rates in studies of all ages
range from 43−47 per 100,000 person-years;7 however, the incidence of the epilepsies is highest in infants. The long-term prognosis of epilepsy is favourable, with no seizures in five years before last follow-up occurring in ~70% of children, whereas epilepsy remains active (ie at least one seizure in five years) in ~30% of children.8 It is intractable (ie no remission exceeding three months during a one-year period of observation despite adequate treatment) in ~10%. Prognosis is primarily determined by the syndrome, and/or the underly-ing cause. Lennox-Gastaut syndrome, epilepsy with myoclonic absences and some brain malformations are among those with the highest risk of intractability.9
Diagnostic tools Diagnosis is made on the basis of description of events. The description, made by an eye witness to the events, should be as detailed and accurate as possible. Video documentation, for example using a mobile phone, can be of immense value. Clinical assessment of the events and examination of the patient by a paediatrician with expertise in epilepsy form the mainstay of the diagnosis. An EEG should be performed to support a diagnosis of epi-lepsy but it is unlikely to be diagnostic unless an event occurs during the recording. Sleep EEG and repeated standard EEGs may be helpful when the diagnosis of the epilepsy or the syn-drome is unclear. Long-term video or ambulatory EEG may be used in the assessment of children who present diagnostic difficulties after clinical assessment and standard EEG. Neuroimaging by MRI should be performed if there is any evidence to suggest the epilepsy is focal in onset (with the exception of what could be classed as ‘benign’ epilepsy syndromes such as childhood epilepsy with centrotemporal spikes), if there is an abnormal neurological examination, or in children younger than two years old (excluding those with simple febrile seizures). As a practical approach, neuroimag-ing is indicated in every child who does not have what may be considered a ‘benign’ epilepsy syndrome, namely childhood epi-lepsy with centrotemporal spikes, childhood absence epilepsy or juvenile myoclonic epilepsy. Assessment of educational level should be considered in all children who are diagnosed with epilepsy. It is important to eval-uate learning disabilities and cognitive dysfunction, particularly with regard to language and memory, especially when a child or young adult is having educational or occupational difficulties, or complains of memory problems and/or cognitive decline.
Medical treatment A decision to treat with antiepileptic drugs (AED) does not nec-essarily equate to a diagnosis of epilepsy, but it can be taken as a marker for a predisposition to further seizures. For instance, AED treatment may be started following a seizure in a patient who presents with epilepsy in the context of an acute brain insult, eg herpes encephalitis. A decision to treat should be made by a paediatrician with expertise in epilepsy, together with the family and child where relevant. This should be followed by a discussion as to the best AED to trial in the context of the type
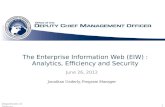
Figure 1. New classification of seizure types (International League Against Epilepsy 2017). From: Fisher RS, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017;58(4):522–30.5 © International League Against Epilepsy
Focal onset Generalised onset Unknown onset
Motor onsetNonmotor onset
Focal to bilateral tonic-clonic
Motor:- tonic-clonic- other motor
Nonmotor (absence)
Motor:- tonic-clonic- other motor
Nonmotor
Unclassified(due to inadequate
information or inability to place in other categories)
AwareImpaired
awareness

16 ❚ Prescriber April 2018 prescriber.co.uk
■ PRESCRIBING IN CHILDREN l Epilepsies
of epilepsy and the child. Conversely, a diagnosis of epilepsy does not necessarily require AED treatment. Children with epilepsy with centrotem-poral spikes, for instance, have a very good prognosis for remis-sion of seizures and cognitive outcome. There is an ongoing debate about offering AED treatment only to those children with a high seizure frequency or for the occurrence of prolonged seizures. Where possible, choice of AED should be based on the presenting epilepsy syndrome. If the epilepsy syndrome is not clear at presentation, the decision should be based on the presenting seizure type(s). The preference of the child or young adult and their family and/or carers needs to be taken into consideration, as well as co-medication and co-morbidity. Table 1 lists suitable AEDs for first-line treatment.10
Sodium valproate has been widely used as a first-line agent, particularly in early-onset generalised and mixed epilepsies, and remains a useful drug specifically in idiopathic general-ised epilepsies. However, there has been increasing concern about the effects of valproate medicines on the unborn child when taken by a mother during pregnancy. Babies exposed to valproate medicines in the womb are at high risk of congenital malformations, as well as developmental problems such as learning difficulty and or autism.11 Recognising these risks, the Coordination Group for Mutual Recognition and Decentralised Procedures-Human (CMDh) of the European Medicines Agency (EMA) consequently strengthened warnings on the use of val-proate in girls and women.12 The summary of product character-istics for sodium valproate states that it “should not be used in female children, in female adolescents, in women of childbear-ing potential and pregnant women unless other treatments are ineffective.” Recognising the issue in girls and women of childbearing age, specific guidance for the assessment of risk-benefit has been highlighted.13 Furthermore, a toolkit has been provided by the MHRA to aid discussions with girls of childbearing age prescribed or continuing sodium valproate.14 Further restric-tions on the use of valproate in women of childbearing potential were recently recommended by the EMA’s Pharmacovigilance Risk Assessment Committee (PRAC), and these have now been endorsed by the CMDh.15 Valproate medicines are now con-traindicated in girls and women able to have children unless no alternative treatments are suitable and the terms of a special pregnancy prevention programme are followed.
Adverse effectsAdverse drug effects are common in children treated with AEDs. They are significantly more frequent in children on polyther-apy compared with monotherapy. Approximately one in 10 chil-dren receiving an AED has to stop treatment due to toxicity.16 However, there is also a tendency to blame medication for all symptoms that manifest, some of which may be due to co-mor-bidities. The most common adverse reactions are a broad range of behavioural and mood problems (which can occur with sodium valproate, phenobarbital, clobazam, topiramate, zonisamide, or more specifically increased aggressiveness with

Prescriber April 2018 ❚ 17prescriber.co.uk
Epilepsies l PRESCRIBING IN CHILDREN ■
levetiracetam). Adverse cognitive effects have been reported for phenobarbital, phenytoin, topiramate and zonisamide, but there is a lack of systematic data. Somnolence is commonly reported for clobazam and carbamazepine/oxcarbazepine, but also for levetiracetam and phenobarbital. Other pharmacology-related (Type A) adverse effects include hyponatraemia and water intoxication with oxcarbazepine and carbamazepine, and metabolic acidosis and nephrolithiasis dur-ing treatment with topiramate and zonisamide. Gastrointestinal problems such as nausea, pain and weight gain are reported with ethosuximide and sodium valproate.16 Cutaneous manifestations of hypersensitivity are the most common idiosyncratic (Type B) adverse reactions to AEDs and range from mild urticaria/maculopapular eruptions to poten-tially life-threatening DRESS (drug rash with eosinophilia and systemic symptoms), Stevens-Johnson syndrome and toxic epi-dermal necrolysis. These most frequently occur with carbamaz-epine, phenytoin and lamotrigine. Other serious idiosyncratic reactions associated with AEDs include liver toxicity, pancrea-titis, aplastic anaemia and agranulocytosis. However, it is not uncommon to see mild elevation of transaminases in children on sodium valproate; these fluctuate and do not imply liver dysfunction or a requirement to reduce the dose. AED treatment (especially carbamazepine, phenytoin and sodium valproate) is associated with adverse effects on bone health including elevated bone turnover, reduced bone min-eral density and fractures. It is recommended that all patients obtain adequate amounts of calcium and vitamin D. Finally, there is a potential risk with any AED to cause seizure aggravation. This is best documented for the use of carbamaz-epine in generalised and myoclonic epilepsies. The pathophys-iology of seizure aggravation is not fully understood; it involves non-specific effects such as sedation, drug-induced encephalop-athy, and paradoxical or inverse pharmacodynamic effects.17
Management in case of failure of the first AED The diagnosis of epilepsy needs to be critically re-evaluated if seizures continue despite an optimal dose of a first-line AED. An alternative AED should be offered and treatment should be con-tinued as monotherapy whenever possible. However, because of the profound developmental, behavioural and psychological effects that may be associated with continuing seizures, chil-dren should be referred to tertiary services early, especially if:10
• The epilepsy is not controlled with medication within two years.• Management is unsuccessful after two drugs.• The child is aged under two years.• The child experiences unacceptable side-effects from med-ication. • There is a unilateral structural lesion. • There is psychological and/or psychiatric co-morbidity.• There is diagnostic doubt as to the nature of the seizures and/or seizure syndrome.
Non-pharmacological treatments Most children who develop epilepsy will respond to pharmaco-logical treatment; however, approximately 20–30% will develop
medically refractory epilepsy. For this population, non-pharma-cological treatments can be highly efficacious and should be seriously considered. Options are:• Epilepsy surgery is highly successful in achieving seizure freedom in carefully selected children with drug-resistant focal epilepsy. Children should be referred to and assessed within recognised epilepsy surgery programmes.18 • The ketogenic diet (KD) is an established, effective non-phar-macological treatment for intractable childhood epilepsy. It has been reported as particularly beneficial in glucose transporter protein 1 (GLUT1) deficiency, pyruvate dehydrogenase defi-ciency (PDHD), myoclonic-astatic epilepsy (Doose syndrome) and Dravet syndrome as well as several other childhood syn-dromes (see: www.matthewsfriends.org).• Vagus nerve stimulation (VNS) may be considered for drug refractory seizures in children; for Lennox-Gastaut syndrome- associated seizures, VNS is associated with a seizure reduc-tion of around 55% (95% CI 50–59%) for children with focal or generalised epilepsy.19
SummaryEpilepsy is common in children but there are many different types, and decisions about diagnosis and management can be complex. If epileptic seizures are suspected in a child, they should be referred urgently to a paediatrician with expertise in epilepsy, where appropriate investigation and decisions about management will be made. Most children will respond to med-ication, or go into long-term remission. However, in 30% of chil-dren, seizures continue and alternative management strategies may be considered. Furthermore, in such children there is a high rate of learning and behaviour difficulties, and seizures
Figure 2. New framework for the classification of the epilepsies (International League Against Epilepsy 2017). *Denotes onset of seizure. From: Scheffer IE, et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017;58(4):512–21.6 © International League Against Epilepsy

■ PRESCRIBING IN CHILDREN l Epilepsies
18 ❚ Prescriber April 2018 prescriber.co.uk
Seizure type / epilepsy syndrome
First-line AED Daily maintenance dose range (usually in two divided doses)
Remarks
Focal seizures lamotrigine oxcarbazepine carbamazepine levetiracetam
1–15mg/kg25–35mg/kg10–25mg/kg15–50mg/kg
If the first AED tried is ineffective, offer an alternative from these AEDs. Monotherapy should always be preferred
Newly-diagnosed generalised tonic-clonic seizures
sodium valproate*lamotrigineclobazam
10–30mg/kg1–15mg/kg0.2–1.0mg/kg
*Note the teratogenic and developmental risks of sodium valproate in pregnancy; consequently it should not be used in women/girls of childbearing age unless there is no suitable alternative.15 May require specialist discussion
Absence seizures ethosuximide sodium valproate*
20–30mg/kg10–30mg/kg
Offer ethosuximide or sodium valproate as first-line treatment. If there is a high risk of generalised tonic-clonic seizures, offer sodium valproate first, unless it is unsuitable eg girl of childbearing age
Myoclonic seizures sodium valproate* levetiracetamtopiramate
10–30mg/kg15–50mg/kg2–12mg/kg
Do not offer carbamazepine, gabapentin, oxcarbazepine, phenytoin, pregabalin, tiagabine or vigabatrin
Tonic / atonic seizures sodium valproate* lamotriginerufinamide
10–30mg/kg1–15mg/kg10–45mg/kg
Do not offer carbamazepine, gabapentin, oxcarbazepine, pregabalin, tiagabine or vigabatrin
Infantile spasms Steroid (prednisolone or tetracosactide) with vigabatrin
Offer vigabatrin as first-line treatment to infants with infantile spasms due to tuberous sclerosis
Myoclonic-astatic epilepsy (Doose syndrome)
sodium valproate* clobazam ethosuximidelamotrigine
10–30mg/kg0.2–1.0mg/kg20–30mg/kg1–15mg/kg
Children rarely respond to monotherapy; rational polytherapy needs to be considered early. Be aware that lamotrigine may exacerbate myoclonic seizures. Consider ketogenic diet
Lennox-Gastaut syndrome sodium valproate* lamotriginerufinamide
10–30mg/kg1–15mg /kg10–45mg/kg
Do not offer carbamazepine, gabapentin, oxcarbazepine, pregabalin, tiagabine or vigabatrin
Epilepsy with centrotemporal spikes and Panayiotopoulos syndrome, and late-onset childhood occipital epilepsy (Gastaut type)
oxcarbazepine carbamazepinelevetiracetamlamotriginesodium valproate*
25–35mg/kg10–25mg/kg15–50mg/kg1–15mg/kg10–30mg/kg
Be aware that carbamazepine and oxcarbazepine may exacerbate or unmask continuous spike and wave during slow sleep
Juvenile myoclonic epilepsy sodium valproate* levetiracetamlamotrigine
10–30mg/kg15–50mg/kg1–15mg/kg
Be aware that lamotrigine may exacerbate myoclonic seizures. Do not offer carbamazepine, gabapentin, oxcarbazepine, phenytoin, pregabalin, tiagabine or vigabatrin
Other epilepsy syndromes (continuous spike and wave during sleep (CSWS), suspected Dravet syndrome)
Under guidance of tertiary specialist
Table 1. First-line antiepileptic drug (AED) treatments. Adapted from: NICE. Epilepsies: Diagnosis and Management. CG137. January 2012 (updated February 2016)10

Prescriber April 2018 ❚ 19prescriber.co.uk
Epilepsies l PRESCRIBING IN CHILDREN ■
may not be the biggest concern in such families. For many, psy-chological support and educational assessment may contribute enormously to ongoing management.
References1. Fisher RS, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 2014;55(4):475–82. 2. Blume WT, et al Glossary of descriptive terminology for ictal semi-ology: report of the ILAE task force on classification and terminology. Epilepsia 2001;42:1212–8.3. Kasteleijn-Nolst Trenité DG. Provoked and reflex seizures: surprising or common? Epilepsia 2012;53(Suppl. 4):105–13.4. Berg AT, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 2010;51(4):676–85. 5. Fisher RS, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017;58(4):522–30.6. Scheffer IE, et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017;58(4):512–21.7. Forsgren L, et al. The epidemiology of epilepsy in Europe – a system-atic review. Eur J Neurol 2005;12(4):245–53. 8. Geerts A, et al. Course and outcome of childhood epilepsy: a 15-year follow-up of the Dutch Study of Epilepsy in Childhood. Epilepsia 2010;51(7):1189–97. 9. Geerts A, et al. Onset of intractability and its course over time: the Dutch study of epilepsy in childhood. Epilepsia 2012;53(4):741–51. 10. National Institute for Health and Care Excellence. Epilepsies: diag-nosis and management. CG137. January 2012 (updated February 2016). Available from: https://www.nice.org.uk/guidance/cg137. NICE guidance is prepared for the National Health Service in England, and is subject to regular review and may be updated or withdrawn. NICE has not checked the use of its content in this article to confirm that it accurately reflects the NICE publication from which it is taken.11. Veroniki AA, et al. Comparative safety of antiepileptic drugs for neurological development in children exposed during pregnancy and breast feeding: a systematic review and network meta-analysis. BMJ Open 2017;7(7):e017248. 12. European Medicines Agency. CMDh agrees to strengthen warnings
on the use of valproate medicines in women and girls. November 2014. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_document/Valproate_and_related_substances_31/Position_provided_by_CMDh/WC500177637.pdf13. Tomson T, et al. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia 2015;56:1006–19.14. Medicines and Healthcare products Regulatory Agency. Toolkit on the risks of valproate medicines in female patients. Available from: https://www.gov.uk/government/publications/toolkit-on-the-risks-of-valproate-medicines-in-female-patients 15. European Medicines Agency. PRAC recommends new measures to avoid valproate exposure in pregnancy. February 2018. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/referrals/Valproate_and_related_substances/human_referral_prac_000066.jsp&mid=WC0b01ac05805c516f 16. Anderson M, et al. A prospective study of adverse drug reactions to antiepileptic drugs in children. BMJ Open 2015;5(6):e008298. 17. Gayatri NA, Livingston JH. Aggravation of epilepsy by anti-epileptic drugs. Dev Med Child Neurol 2006;48(5):394–8.18. Epilepsy Action. Children’s Epilepsy Surgery Service (CESS) in England. Available at: https://www.epilepsy.org.uk/info/treatment/surgery/children19. Morris GL 3rd, et al. Evidence-based guideline update: Vagus nerve stimulation for the treatment of epilepsy. Neurology 2013;81(16):1453–9.
Declaration of interestsHelen Cross has been an investigator for clinical trials spon-sored by Vitaflo, GW Pharma and Zogenix, on advisory boards for Eisai, GW Pharma, Takeda and Zogenix, and a speaker for GW Pharma, Zogenix and Biomarin. All remuneration has been paid to her department. Christine Prager has received sponsor-ship as a main organiser for a workshop on epilepsy surgery in Berlin by Desitin, 2017.
Christine Prager is a consultant paediatric neurologist at Charité University Hospital, Berlin and J Helen Cross is the Prince of Wales’s Chair of Childhood Epilepsy and Head of the Developmental Neurosciences Programme, UCL-Great Ormond Street Institute of Child Health, London